
Psychiatric epidemiologist policy analyst Critic of dodgy claims/bandwagons/propaganda/conflicts of interest. JSBachtragic Klavierschülerin Ambulophile Aviphile
Joined September 2011
- Tweets 39,281
- Following 5,018
- Followers 2,409
- Likes 91
203 Photos and videos


Pinned Tweet

28 Jan 2021
#Untreated mental illness: #ideology trumps evidence, fuelling #overdiagnosis ebm.bmj.com/content/24/Suppl… #evidenceunbased #psychiatricideology #magicalthinking
5
23
34
Melissa Raven retweeted

I think that in a recent paper McCutcheon and colleagues have obscured the finding that slower tapering of antipsychotics produces clearly lower relapse rates than faster tapering by treating patients maintained on depot antipsychotics as the same as those maintained on oral antipsychotics when the latter are much more likely to stop their drugs.
This unwarranted equivalency obscures the fact found in similar data by other researchers that slower tapering (stopping depots) produces less relapse than faster tapering (stopping orals). This suggests that slower tapering (ideally hyperbolically) can reduce relapse rates in clinical practice and in research studies. Link below.
1
11
36
1,257
Melissa Raven retweeted
“When in doubt or there are uncertainties, blame patients”
I am glad Awais wrote this piece because it is a very useful summary of where I think most psychiatrists are and it is useful to see it laid out in his mostly careful and thorough style. Given how much Awais is a bellwether for mainstream opinion from psychiatry (the irony of his blog being named ‘from the margins’!) it is important to respond to it which I will do in the next few days but just wanted to comment quickly.
It is riddled with errors and misunderstandings of the theory and evidence for withdrawal and hyperbolic tapering (the section on receptor occupancy is particularly full of howlers – this is the double edged sword of blogs. They allow people to put out work quickly but there is no peer review which would normally catch basic errors before they are put out to thousands of people) but it also raises some useful points about holes in the field and points for research, many of which I agree with (e.g. where is the line between an injury due to exposure and an injury due to withdrawal).
What I find most concerning about it is the overall tone of it is written as a ‘gotcha’ piece to expose what he believes to be inconsistencies and illogic in the experience of large numbers of patients (and the researchers and intellectuals that work in this area). Some of his ‘gotchas’ are based on misunderstandings of the science or erroneous conclusions, which can be clarified.
But what can’t be altered is his desire (and I am not pointing the finger at Awais specifically, he is just the most outspoken and articulate of his cohort) to reveal that patients are wrong. Transparently, this is because it is couched as an ‘us against them’. If patients and the research that ‘supports’ their experience is valid then it puts psychiatrists in a difficult position of having to grapple with prescribing treatments that cause devastating consequences for a portion (and not an insignificant portion) of patients. Easier to blame the patients.
And this is what he does at every point of uncertainty. Instead of saying ‘hmm, this is pretty concerning: there are people experiencing debilitating symptoms years after stopping antidepressants (like for many classes of psychiatric drugs and matching the neurobiological evidence of similar long-lasting brain alterations) I wonder what the hell is going on here?’ he jumps to saying ‘this makes no sense (based on a few throw away assumptions and no careful reading of the literature)’ and these patients must be hysterical or ill in some way.
The same thing was said in response to tardive dyskinesia from antipsychotics (said for years to be due to the illness), to withdrawal effects from benzodiazepines, to PSSD for antidepressants, metabolic effects from newer antipsychotics, etc, etc. It is a common response from a discipline that often feels itself on fragile ground and finds it more convenient to blame patients for the issues caused by its treatments.
I agree with Awais that there are unexplained phenomenon in withdrawal but I wish that Awais (and other psychiatrists) came at this in the spirit of open-minded inquiry and concern rather than a desire to dismiss, minimise and belittle. This really does prompt me to have to update my blog on ‘why doctors don’t see withdrawal’ in which I was trying to be as sympathetic as possible to doctors, acknowledging that at some point I also had no idea about withdrawal. But I need to add an important factor that doctors don’t want to see this because of all the implications for them.

17
26
107
7,154
Melissa Raven retweeted

Jun 13
The experience of all the kids put into therapy or psychiatry to be controlled and broken down is constantly being erased by clinical authority. Mental health professionals get to define the narrative there because of all the power our society gives them. If they say it’s “humanistic” and sincerely about helping them, then that’s the story that prevails, even if it couldn’t be further from the truth (which is often, if not most of the time). The scariest part is the victims of this often believe it too.
Jun 11

That's not true at all. It's a very antipsychiatric thought (psychiatry is about moral or social control) that is not borne out in what a psychiatrists goals are, which is to help an individual suffer less and overcome impediments. Even with kids.
2
5
25
802
Melissa Raven retweeted

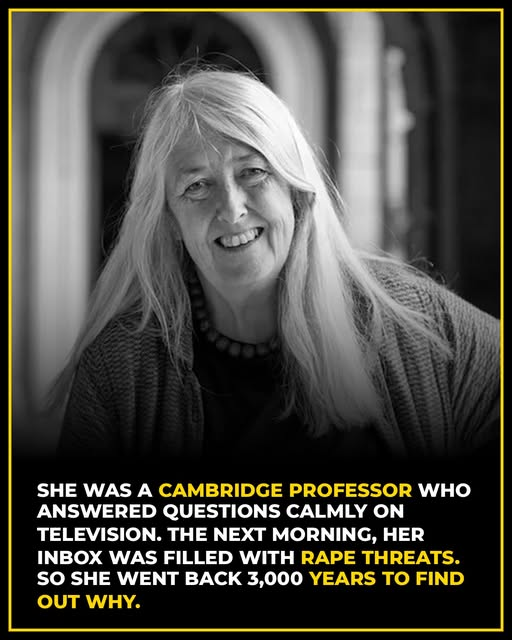
She was 57 years old.
White hair. No carefully managed image. No media training designed to make her more palatable. Just thirty years of accumulated knowledge and the calm, unhurried authority of a woman who had spent her life mastering her subject.
She sat on a BBC panel, answered questions about immigration and politics, cited evidence, made arguments — and then went home.
The next morning, her inbox looked like a crime scene.
Her name is Mary Beard — Cambridge professor, classicist, one of the most respected scholars of ancient Rome and Western civilisation alive. And the internet had decided that a woman speaking with quiet authority on television needed to be punished for it.
The messages were not criticism. They were not debate. They were rape threats. Death threats. Coordinated campaigns of personal destruction targeting her appearance, her age, her voice — anything that could be used to remind her that spaces like the one she had just occupied were not meant for her.
Most people would have gone quiet.
Mary Beard went further in.
She did what scholars do when they find a pattern that disturbs them: she followed it backward. Through decades. Through centuries. Through millennia. All the way back to some of the oldest texts in Western civilisation.
And she found it had always been there.
In Homer's Odyssey — one of the foundational works of Western literature, nearly three thousand years old — there is a scene that most readers pass over without registering its quiet violence. Penelope comes downstairs and asks the poet to sing a different song. Her own son, Telemachus, cuts her off. He orders her back to her room and tells her plainly: speech is the business of men.
She goes.
Mary Beard read that scene and recognized it immediately.
Not as ancient history. As a pattern.
In ancient Rome, women who dared to speak in public were not described as orators or thinkers. They were described as noise — disorderly sound, something that did not deserve to be called language or argument. Their voices were not speech. Their thoughts were not thoughts.
In the medieval world, women who claimed public authority were labeled as witches.
Elizabeth I — Queen of England, ruler of a nation — had to rhetorically reshape herself into something masculine just to be taken seriously as the leader of her own country.
The silencing of women who speak with authority was not invented by social media. It was not a modern pathology or a cultural accident. It was built deliberately, over centuries, into the very foundations of how Western civilisation defined who gets to speak, what authority sounds like, and who is allowed to take up space in public life.
Mary Beard had found something important.
In 2017, she published Women & Power: A Manifesto — short enough to read in an afternoon, substantial enough to reframe everything you thought you understood about why this keeps happening.
Her argument was precise and devastating.
The problem is not that women lack the ability to lead. The problem is that the model of leadership itself — the template for what public authority looks, sounds, and feels like — was built by men over centuries and has never been redesigned. When a woman enters public life and doesn't fit that template, she is not failing. The template was never built for her. It was built specifically to exclude her, and it has been doing exactly that, efficiently and continuously, for three thousand years.
The solution, Beard argued, is not to teach women to perform power the way men have always performed it. The solution is to dismantle and rebuild the very concept of what power is allowed to look like.
She kept teaching. She kept writing. She kept appearing on television — white-haired, unhurried, carrying her decades of authority without performing it, without packaging it for comfort, without apologizing for it.
The threats continued.
But other messages began arriving too. Letters from women and girls who had spent their entire lives feeling that every door was slightly too narrow, every table slightly too high, every room slightly reluctant to make space for them. Women who had spent years wondering what was wrong with them — why they couldn't quite fit, couldn't quite belong, couldn't quite be taken seriously no matter how much they knew or how hard they worked.
They read the book and understood, perhaps for the first time, that nothing had ever been wrong with them.
The room had been designed without them in mind.
That is not a personal failing.
That is a three-thousand-year-old architectural decision.
And one Cambridge professor with white hair and a calm voice — who refused to go quiet when the internet told her to — spent her career documenting it, naming it, and handing that knowledge to everyone who needed to hear it.
Telemachus told Penelope that speech was the business of men.
He was wrong then.
He is still wrong now.
And Mary Beard has three thousand years of evidence to prove it.
via The Inspireist
#FeministFriday #HERstory
138
2,693
7,839
178,321
Melissa Raven retweeted

"Moncrieff said that the risks and side effects of SSRIs are often underestimated.
'They are a drug that interferes with our brain chemistry and other biological systems,' said Moncrieff.
Moncrieff said side-effects can include sexual dysfunction, dependence, osteoporosis, weight gain, bleeding and pregnancy complications. 'We really should be minimizing their use as much as possible,' she said."
#MentalHealth #antidepressants
LINK: dw.com/en/ssri-antidepressan…
3
27
57
1,634
Melissa Raven retweeted
It’s good to see wider discussion of withdrawal and hyperbolic tapering, including critiques. My observation is that whenever a clinician who is minimising the existence of withdrawal or the need for hyperbolic tapering is asked about their deprescribing experience they give vague answers like ‘I stop drugs all the time’ but when pressed for details trail off. Of course reading the literature is a part of being informed but actual first hand experience of large volumes of deprescribing teaches you a lot more. Everyone is entitled to an opinion but I think it is worth probing how informed such opinions are. Most friends of mine in psychiatry who are not invested in this debate either way rarely if ever stop long term drugs without switching to another or are seeing people on large numbers of drugs which buffer withdrawal effects. In other words they rarely have the chance to see withdrawal effects. I don’t want to make generalisations but I wonder where some people derive the confidence in their opinions? For example I have overseen about 4000 people coming off their drugs and I have very little idea what these drugs are doing in long term to the brain but there are some let’s say concerning signals - I would like to learn from people with much greater confidence than me what the source of their insights are.
6
19
79
2,668
Melissa Raven retweeted
Jun 12
The progressive, holistic, "biopsychosocial" language the mental health field uses in public, I believe is not their actual practice, in most cases. It is a public relations shield.
Jun 11

Shrödinger’s psychiatry:
When you actually go in to see a psychiatrist it’s 15 minutes, you get gaslit, told you have a chemical imbalance or faulty brain circuitry, can feel an underlying air of authoritarianism.
When you point out that this is how it actually operates, suddenly psychiatry becomes “biopsychosocial”, “humanistic”, all about helping you achieve your goals and making you feel better, etc.
3
4
24
947
Melissa Raven retweeted

Jun 12
Is a drug class that causes sexual dysfunction in 70% patients "toxic"? Some might say yes.
Is a drug class that barely reduces short-term symptoms vs placebo "useless"? Again, reasonable people might agree.
......
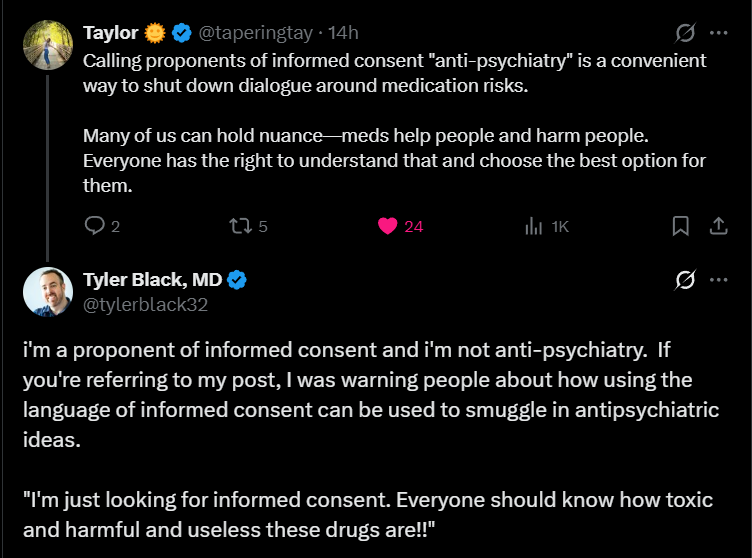
Are factual, empirically supported statements "antipsychiatry"?
4
10
24
692
Melissa Raven retweeted

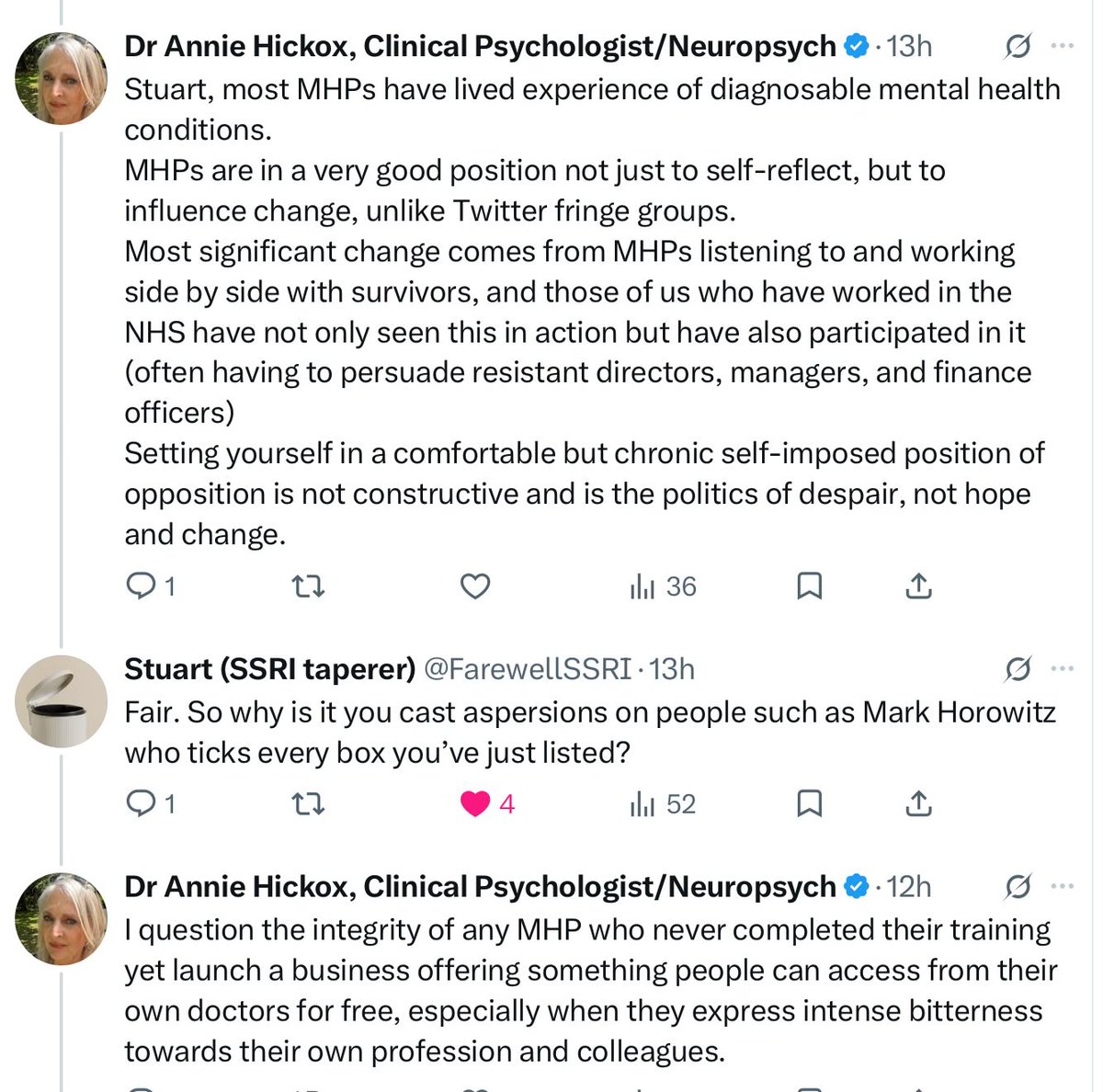
I don't think any of us doubt the integrity of @markhoro because he has worked so hard to try to make a difference by attempting to ensure safer deprescribing practices. He provides a free NHS service in the UK. The US has a different system where paying for services is common.

2
8
16
661
Melissa Raven retweeted

Jun 12
Anyone who tries to shut you down with statements like ‘the science says’ or ‘the data says’ ask them to look at this.
If it takes this much to retract junk science like Study 329 how confident can we be about the accuracy and integrity of what is published?
And remember this is just one of the ones where they got caught….

🚨Study 329 lawsuit collapses
A legal attempt to force a retraction of Study 329 has failed and the journal has gone silent. What happens when science cannot—or will not—correct itself?
LINK 👇👇
@LauraDelano @MikhailaFuller @SecKennedy @AaronSiriSG @newstart_2024 @jchilders98
3
30
66
3,226
Melissa Raven retweeted

Jun 11
The reason why fraudulent antidepressant studies are not retracted by the Psychiatric medical establishment & remain part of the training curriculum (see STAR*D) is simple. If the general public & trained professionals became aware it would end Psychiatry as a viable healthcare specialty and wipe out the antidepressant market. The product liability lawsuits themselves would be astronomical. The public trust in western medicine would be further destroyed.
14
83
305
16,530
Melissa Raven retweeted

Jun 12
Involuntary commitment is more likely if you're Indigenous, immigrant, lower-income... seeing any trends here? robwipond.substack.com/p/who… My latest at PsychForce.Report
3
13
23
635
Melissa Raven retweeted

New Research Challenges the Logic of Coercion in Psychiatry
By Richard Sears
Recent studies examine long-term harms of psychiatric detention, ward environments as a major driver of coercive interventions, and why some staff support coercive practices.
buff.ly/BenbLBR

2
24
43
1,419
Melissa Raven retweeted

Stigma from mental health professionals arises from a pathologising ideology that casts people in distress as dysfunctional, maladapted, disordered & ill, rather than as individuals in pain, in need, in burgeoning awareness, or in protest against conditions holding them back.
21
37
144
4,959
Melissa Raven retweeted
Not only is Nicolas a wonderfully polite man to call his interlocutors ‘advocates’ but Cochrane reviews find nnts of more than 9. But more importantly these measures are made after 8 weeks of drug or placebo. Lots of drugs look effective at 8 weeks - benzos for anxiety and opioids for pain - but wear off over time because of tolerance. Not to mention all the methodological issues such as unblinding that exaggerate the difference between placebo and antidepressants.
Jun 11

@sanilrege “incorrect” -> Grok “No”
@tylerblack32 “misinterpreted” -> Gemini “No”
@vitorborin_ “inaccurate” -> Claude “No”
Look, I appreciate those advocates doing their thing, but I am not an advocate. I don’t try to interpret things in a positive light but an accurate one.
Psychiatry deals with very fraught issues. We should be honest about our limitations and not spin things positively.
I would have been fine with them saying the NNT could be interpreted in other ways, or that placebos don’t exist in the real world, but instead they used precise words which IMO ended up being more inaccurate. I don’t think that 11% helped is that bad; it just is what it is.


1
7
27
1,994
Melissa Raven retweeted
Very useful article in @TheBJPsych evaluating different off-lablel techniques for making small doses to make hyperbolic tapering feasible: reassuring that all were found to be within 90-110% of target values (the same standard used for manufactured tablets).

Hyperbolic tapering is increasingly recommended for the gradual reduction of psychiatric drugs to minimise withdrawal symptoms, yet available formulations rarely accommodate the small dose regimens required. cambridge.org/core/journals/…
5
16
32
3,788
Melissa Raven retweeted

Jun 12
80% of people on psychiatric drugs take them for months or years at a time.
Yet most of these drugs only went through short term trials before doctors prescribed them for long term use.
Psychiatric drugs can also produce adverse effects and withdrawal symptoms that closely resemble the very diagnoses they are supposed to treat.
Once we start viewing every emotional or psychological change through a medicalized lens, it becomes incredibly difficult to recognize when the treatment itself may be causing harm.
That was certainly true in my own life: 🧵
@bretweinstein @thedarkhorsepod
6
42
146
4,707
Melissa Raven retweeted

“Suicide risk assessment should include questions about current medications, recent changes, & new or unusual symptoms. Asking the right questions can make a life-or-death difference. Failure to recognize #akathisia has & may continue to hinder intervention & risk reduction ..”
Indeed.
Important rapid reponse by @MISSDFoundation
"Medication-induced #Akathisia: An overlooked contributor to #suiciderisk..."👇
bmj.com/content/393/bmj-2025…
1
5
9
385
Melissa Raven retweeted
Jun 11
Shrödinger’s psychiatry:
When you actually go in to see a psychiatrist it’s 15 minutes, you get gaslit, told you have a chemical imbalance or faulty brain circuitry, can feel an underlying air of authoritarianism.
When you point out that this is how it actually operates, suddenly psychiatry becomes “biopsychosocial”, “humanistic”, all about helping you achieve your goals and making you feel better, etc.
Jun 11

I'm blocked by Dr. Black, so I can't respond directly to him, but typical psychiatry sessions are only 15 minutes long! Does he believe psychiatrists can do anything other than what he's calling "mcmental health" in that short amount of time?
1
17
65
4,412
Melissa Raven retweeted

While certain psychiatrists on X, argue definitions, time frames and each other's word salads, there's real people suffering through real long-term withdrawal as a necessity to prevent the seizures and other destabilizing WD from irresponsible Rx rapid tapers. I've been tapering for 66 months in total. I'm off 11 psych meds (yes, my ex GP was Big Pharma's best sales woman). I'm down to 6.25mg Seroquel with another year or so to go and then I've still got to taper another 2 psych meds.
Not rare! Just rarely acknowledged by those profiting off the harm.

There are hundreds of thousands of members in withdrawal-related support groups and that figure does not include the countless individuals who never formally joined these communities or those who suffered in isolation, never finding them at all.
It is a profound failure that drug manufacturers and regulators did not adequately warn patients, people who simply trusted their doctors, about the possibility of severe, life-altering withdrawal and the need for careful, often years-long tapering. For many long-term users, tapering is not a passive process. It requires measuring tiny amounts of medication (crumbs, beads, or drops) with extraordinary precision to avoid debilitating symptoms.
In the absence of meaningful medical guidance, patients have become the experts, creating makeshift laboratories in their kitchens and developing tapering methods through necessity and lived experience. Attempts to dismiss these experiences as mere anecdote, or to discredit patients’ accounts of their own bodies and minds because they have a mental health diagnosis, are fundamentally anti-patient.
9
19
69
2,989