
Organic chemist |• Nerd l • Together, we can make beautiful molecules.
Joined December 2011
- Tweets 13,482
- Following 4,025
- Followers 4,707
- Likes 14,412
261 Photos and videos










Pinned Tweet

4 Jan 2024
Let me, a young man in my desperation, go and hunt. Maybe I will kill an elephant, or the elephant will kill me, but either way, my poverty ends. Birth and death are inevitable elemental aspects of human nature.
1
9
61
13,079
Raphael retweeted

Jun 14
A lot of women are desperate for the wedding and not the marriage..
33
39
273
12,413
Raphael retweeted

Jun 10
📢 CALL FOR APPLICATIONS – ACS-RI WORKING TEAM
Are you passionate about research, innovation, and empowering the next generation of African scholars?
The African Center for Student-Led Research and Innovation (ACS-RI), invites qualified and motivated individuals to apply for the listed available positions.
This role offers an opportunity to contribute to the design of a continental research bootcamp aimed at equipping university students with practical research skills, mentorship opportunities, and innovative problem-solving competencies.
Responsibilities include:
✅ Designing training modules and learning activities
✅ Developing the bootcamp curriculum and program structure
✅ Identifying relevant research themes and practical exercises
✅ Supporting the implementation of high-impact research capacity-building initiatives
If you have experience or interest in research, education, curriculum development, public health, biomedical sciences, or innovation, we encourage you to apply.
⏰ Application Deadline: 15th June 2026
📌 Click the application link attached to apply.
Join us in building a stronger culture of student-led research and innovation across Africa.
#ACSRI #ResearchBootcamp #StudentLedResearch #AfricanInnovation #ResearchCapacityBuilding #FAMSA #IPSF #AFMLSSA
docs.google.com/forms/d/1twu…

1
4
35
3,132


Raphael retweeted

👋 IEA's R&D (Research and Development) sixth call is now open 👋
🧪 IEA invites research proposals aimed at improving and advancing the science and methodology of IEA studies, ensuring that they remain at the forefront of international large-scale assessments in education.
🔎 The level of funding is generally based on the proposed project’s needs and will fall into either:
• tier 1: projects up to 55,000 Euros
• tier 2: projects between 55,000 and 110,000 Euros.
🔗 The sixth R&D call is thematically open, and the deadline for submissions is Monday, 14 September 2026, at 13:00 CEST. Read more: ow.ly/TVK650Z9icM

7
19
1,132
Raphael retweeted

💰 Funding opportunity alert: Applications are now open for grants up to EUR 10,000!
🧩 Youth-led organizations and groups can now apply for the Youth Voices Third-Party Funding Mechanism under the AU-EU Youth Voices Lab - Power of the Collective.
This funding opportunity supports youth-led initiatives working to amplify the voices of hard-to-reach young people, strengthen advocacy, and contribute to more inclusive decision-making across Africa and Europe.
ℹ️ Eligibility criteria and terms apply. Before applying, we suggest that you read the Funding Manual.
If your organization is working with young people and communities whose voices need to be heard, this is your opportunity to take action!
📅 Deadline: 29 June 2026, 23:59 EAT
🔗 Read more and apply in English, French, or Arabic: lnkd.in/dKvtgNem
📢 Share this post to spread the word!

1
35
79
5,122
Raphael retweeted

There’s a €50,000 grant for African founders building innovative technology solutions.
No equity. No repayment.
Funding per project not per company.
Open to tech innovators and researchers across Africa.
Projects in digital innovation, health, agriculture and financial inclusion prioritised.
It’s called FCI4Africa Open Call 1.
Most African tech founders have never heard of it.
Deadline June 30. Apply at fundsforngos.org
24
133
550
54,364
Jun 6
The absence of evidence is not evidence of absence. 😅
You hiking on Nyangani and not encountering Mapostori is not proof that they are not there.
It only proves that your path and their prayer sites did not intersect.
If two groups occupy different regions of the same mountain, one group’s observations cannot be generalized to the entire mountain.
Basic sampling bias.
Tasiyana side chete tiri pa rectangle.
Jun 5

Hanzi naSauro.. “Mmm.. Kana uchida kuona kuti gomo iri rinoera, chingotarisa uone kuti hapana kana one mupostori arikukwira kuenda kunonamata ari mariri..”
😂😂😂
To his credit, as much as Mapostori do prayers in mountains, muNyangani manga musina kana one.
78
Raphael retweeted

Jun 4
She giving the ladies a masterclass on how to keep their household together…Ladies do you agree with her?
1,182
3,691
29,521
1,569,429
Raphael retweeted

This Child Protection Month: Know the law. Protect a child.
Every child deserves safety, dignity, protection, & a future full of possibility.
Protecting kids means stronger systems & empowered youth.
#ChildProtectionMonth #GirlsRights #YouthLeadership #Education #SRHR #STEM

11
11
266
Raphael retweeted

May 26
I remember dating someone who would often share her feelings and expectations with me. She was essentially telling me how to love and treat her. Although I listened, I didn't truly apply what she said because I was still figuring myself out and assumed she'd always be around. To my surprise, she eventually left and ceased all communication. At first, I felt betrayed and harbored resentment towards her. However, I soon realized that she had been communicating her needs all along, while I had chosen to act according to my own whims. The lesson here is: if someone consistently communicates with you and your actions don't align with their messages, don't be taken aback when they choose to distance themselves. This holds true for all types of relationships, including friendships.
36
1,099
5,384
151,841
May 12
Outcome: uncertain
Effort: non-negotiable
Consistency: routine 🤝
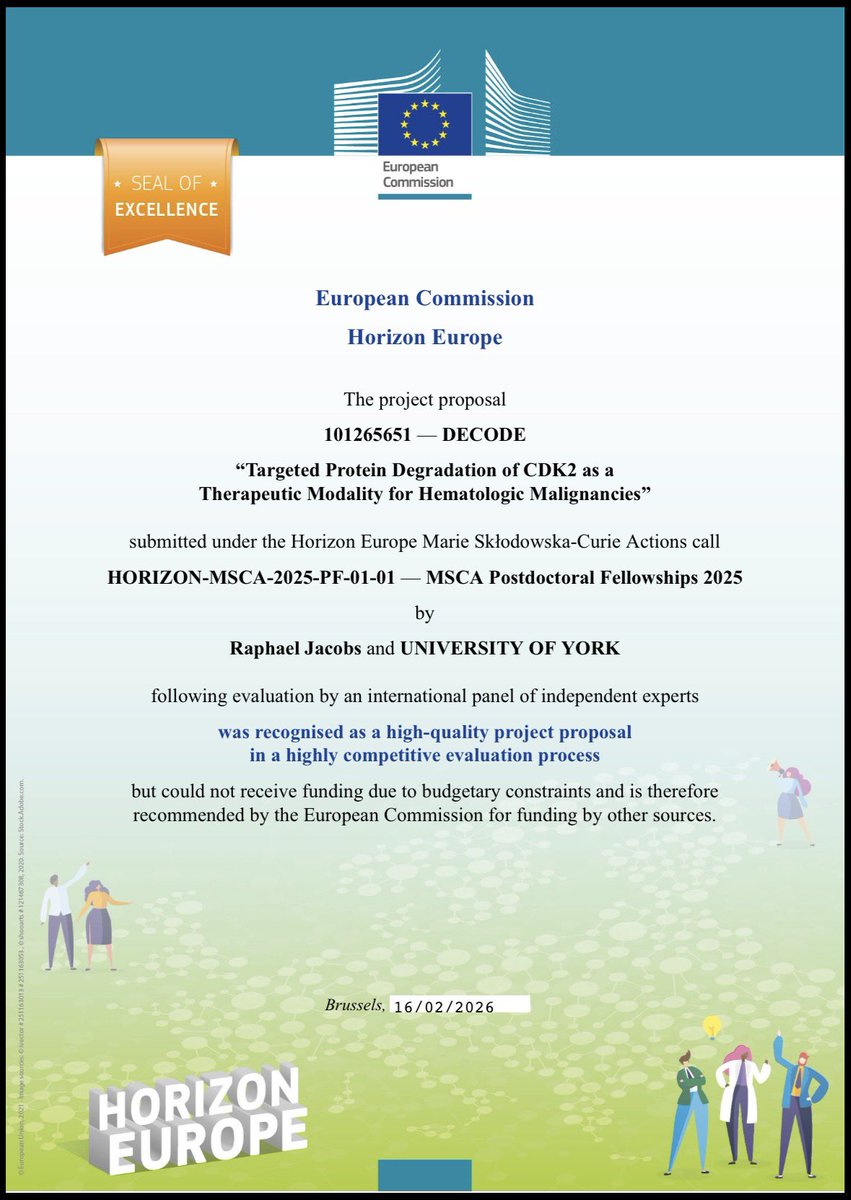
So it has been almost four months since this happened, and if I am honest, it has been one of the hardest pills to swallow in my career.
My first Marie Skłodowska-Curie Postdoctoral Fellowship application, submitted with University of York, was evaluated at ~92% and awarded the MSCA Seal of Excellence. ✨
In other words: objectively excellent… but apparently not quite elite enough this time around. The academic equivalent of receiving a very prestigious loser’s medal. 😂
Jokes aside, the MSCA Seal of Excellence is granted to proposals that meet the high-quality threshold under Horizon Europe but cannot be funded due to budget limitations. It reflects recognition by an international panel of independent experts and confirms that the proposal met the programme’s rigorous standards for scientific excellence, impact, and implementation.
As frustrating as the outcome was, receiving this recognition on a first submission gave me confidence in the originality, competitiveness, and ambition of the project. More importantly, the process reinforced that excellence is not only about strong science, but also about precision, clarity, timing, and execution at every level.
There is still work to do, and I take that seriously. I leave this experience sharper, more reflective, and motivated to come back stronger.
So we learn, refine, and keep moving. 🔁🎯
#MSCA #SealOfExcellence #HorizonEurope #UniversityOfYork #ResearchExcellence #AcademicJourney #Persistence
128
Raphael retweeted

Container loading. 🚛📦
Your trusted partner for sourcing, purchasing, and shipping from China to your destination.
Contact: 8618520184476/ 263771353542
@redmarketsunday
@iMisred @te_hub @Raphael17189292 @raphaelkylej #redmarketsunday #Shipping #ChinaSourcing #Logistics


4
4
184
Raphael retweeted
Different stories. Shared purpose.
Diversity is not a checkbox. Inclusion is not a slogan. Equity is not optional.
When every voice is heard, innovation deepens. When barriers fall, talent rises. When opportunity is shared, communities transform.

3
5
83
Raphael retweeted

Was on my way to Town from Chinhoyi ndikati rega nditakurewo 2o3 passengers muVezel yangu. then on our way ndanga ndichiridza zvangu Winky D, song iye yekuti drink up zvikanzi nemumwe song iyoyo Winky akanyorerwa neAI ndangoti achipedza kutaura ndikamisa mota yangu ndikati sarai
33
40
385
18,338
Raphael retweeted

May 3
📢 CALLING AFRICAN FOUNDERS
The Accelerate Africa Startup Programme 2026 is now accepting applications from early-stage founders building global businesses that solve Africa’s biggest challenges.
FOCUS AREAS
The programme supports bold, early-stage ventures working on:
▪ Scalable solutions addressing Africa’s biggest challenges
▪ Technology-driven and innovation-led businesses
▪ High-growth startups with global ambition
ELIGIBILITY HIGHLIGHTS
✅ Startups based and operating in Africa
👥 At least two co-founders required
🌍 Strong vision to build a global brand from Africa
📊 Early-stage ventures solving meaningful problems
👩💼 Teams with a female co-founder are strongly encouraged
⏱️ Availability to fully engage in programme sessions and coaching
WHAT’S AVAILABLE
✔ One-on-one support from experienced founders and operators
✔ Expert-led workshops (tech, legal, financial)
✔ Access to a strong founder peer network
✔ No application fee or upfront equity required
✔ Potential investment of USD 250,000 – 500,000
✔ Direct access to the Future Africa fund
📅 Application deadline: July 25, 2026
🔗 Apply here: acceler8.africa/
NOTE: This funding opportunity is not administered by GrowthAfrica. Please direct all application-related inquiries to the programme organisers.
Photo credit: Dennis Bett, Deed Technologies #africa

4
41
138
13,478
May 3
When clinical trial design erases $600 million in market value overnight, it is a reminder that in oncology, biology is only part of the equation. Study design can be just as consequential.
The pursuit of anti-angiogenic therapies has long been defined by bold ideas, repeated setbacks, and relentless reinvention. More than four decades ago, Judah Folkman introduced a transformative concept: rather than attacking tumors directly, deprive them of their blood supply and starve them of the oxygen and nutrients required for growth. Elegant in theory, difficult in practice.
Translating that idea into effective medicines proved far more challenging than many expected. Early anti-angiogenic approaches, ranging from endogenous inhibitors such as endostatin to nucleic acid based therapies targeting abnormal vessel formation, produced inconsistent outcomes. Monoclonal antibody programs also faced repeated disappointments before VEGF inhibition finally delivered a clinical breakthrough with Avastin in metastatic colorectal cancer, validating angiogenesis as a therapeutic target.
Interestingly, where oncology struggled, ophthalmology flourished. VEGF directed therapies transformed treatment for wet age related macular degeneration, with agents such as Lucentis, Eylea, Beovu, and Vabysmo collectively building a market worth roughly $10 billion.
Cancer biology, however, rarely stays still. Tumors adapt. As VEGF blockade became established, researchers uncovered compensatory vascular escape mechanisms that could sustain angiogenesis despite VEGF inhibition. One of the most compelling was the DLL4/Notch signaling pathway, which rapidly became a major focus for drug development, including programs pursued by Regeneron. Preclinical data looked promising and expectations were high, but clinical translation again proved unforgiving. Toxicity concerns, narrow therapeutic windows, and inconsistent efficacy ultimately limited the success of anti-DLL4 strategies, whether used alone or in combination with anti-VEGF therapies.
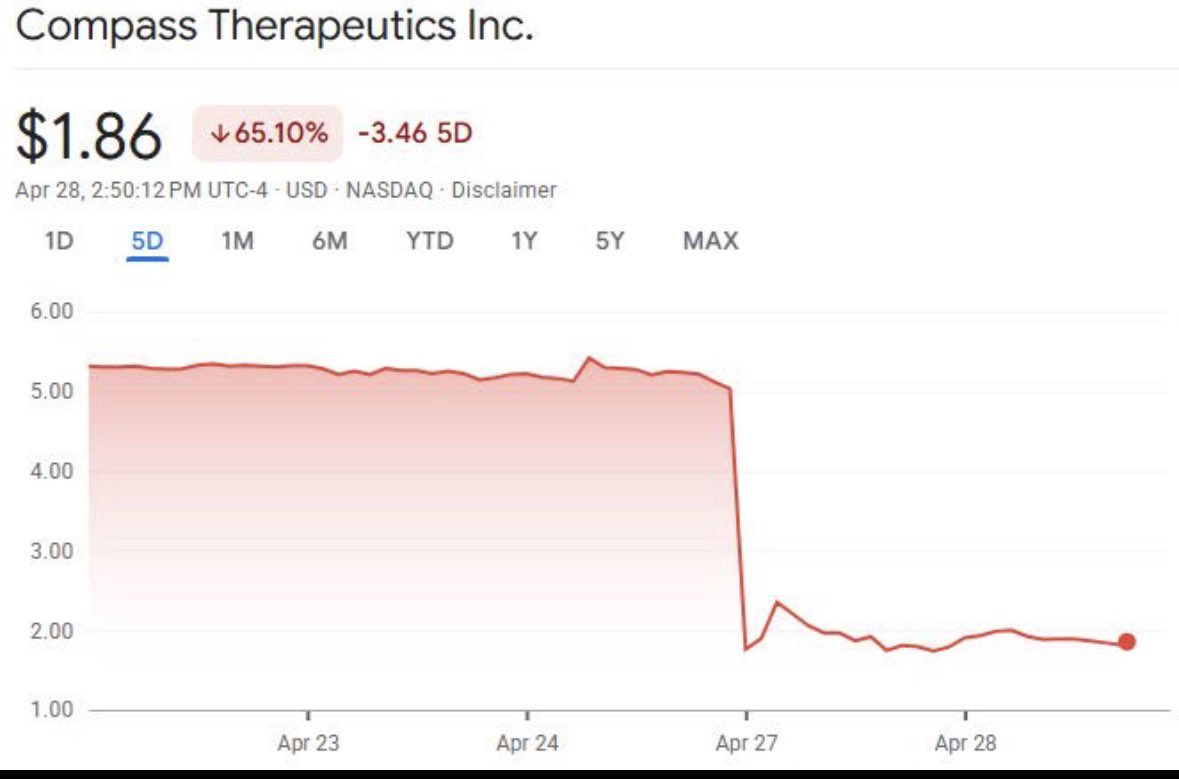
Fast forward to 2026, and Compass Therapeutics appeared poised to reignite optimism in angiogenesis drug development, until pivotal trial data brought a familiar challenge back into focus: the complexity of crossover trial design.
As reported by BioSpace, CEO Thomas Schuetz explained the issue directly during the company’s investor call:
“54% of patients crossed over from the paclitaxel alone control group, meaning 85% of patients ultimately received tovecimig. This group of crossover patients lived an incredibly long time. The overall survival for this group was 12.8 months… Patients who did not cross over had an overall survival of 6.1 months.”
That observation cuts to the heart of the paradox. Patients who received treatment later through crossover appeared to survive substantially longer than many who received therapy earlier, challenging one of oncology’s core assumptions that earlier intervention should generally translate into greater survival benefit. Yet crossover provisions are often required on ethical grounds, ensuring patients in control arms can access promising therapies. Scientifically, however, that ethical safeguard can blur efficacy signals. By counting crossover patients within the original control population under intention to treat analysis, survival in the control arm was effectively elevated, narrowing the apparent treatment gap and pushing overall survival below statistical significance.
Compass will likely work closely with the FDA to further dissect the data and clarify treatment effect. But financial markets rarely reward nuance. Investors tend to react to black and white endpoints, not datasets that require careful interpretation.
In drug development, science may write the story, but trial design often determines how that story is read.
Source: BioSpace
lnkd.in/euyfT-X8
65
Raphael retweeted

Anybody want to come work with me? We're hiring for a cool policy job in my smol research team in DC to work on global education and health. It's a combo of technical academic work and translation work, on a variety of frontier and cool projects. Link below!!
8
31
190
15,281