
Physician, Nutritionist, US Army Veteran, World Traveler (75 countries), T1 Diabetic. #BernsteinBrigade
Joined November 2008
- Tweets 8,068
- Following 983
- Followers 4,597
- Likes 14,131
1,845 Photos and videos









Dr. Ryan Attar retweeted

This is the funniest, most rewatchable five minutes in the history of recorded comedy
It is perfection and never gets old
175
516
7,297
370,080
Dr. Ryan Attar retweeted

18 Apr 2024
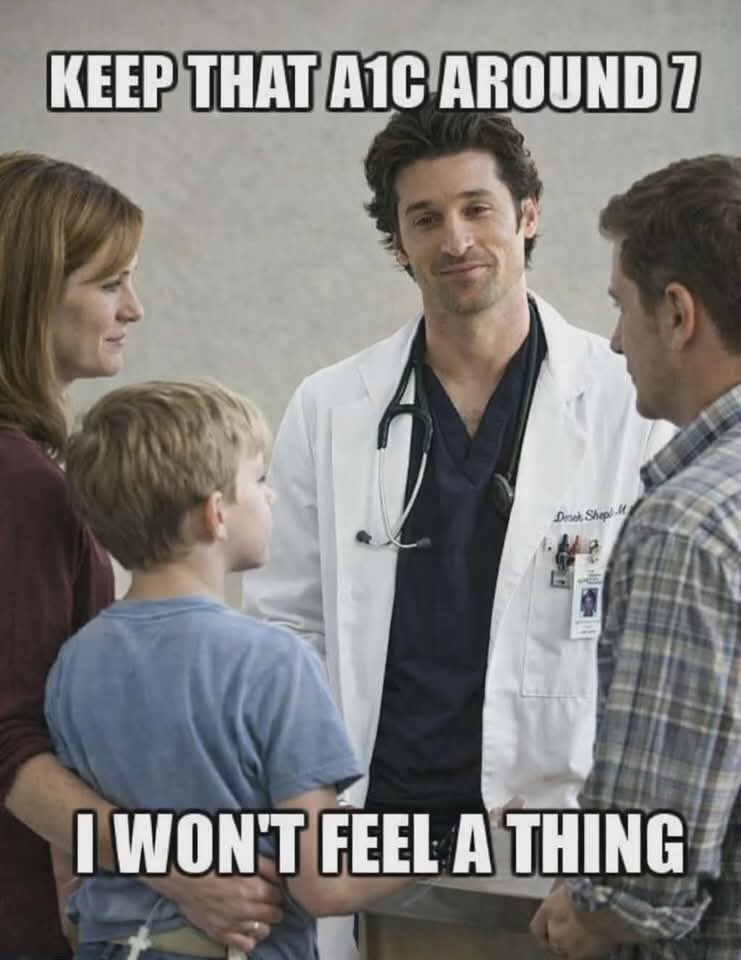
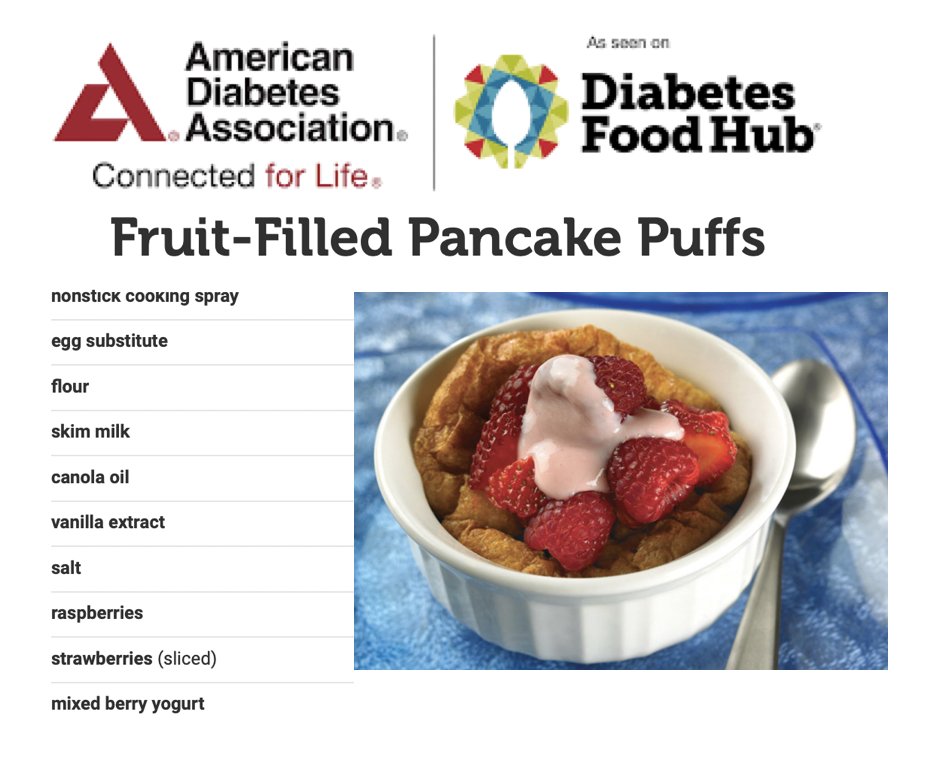
A recipe from the @AmDiabetesAssn @ADA_DiabetesPro for diabetics.
To my diabetic followers, what would this do to your blood sugar?
@ChuckatADA
87
16
128
18,122
May 5
Every wrestler knows and loves this movie. The peg board scene is legendary.
Wrestling shaped me more than anything else growing up. The hard work, brutal practices, and… the weight cutting. Sitting in the cafeteria watching your friends eat while you’ve got a match coming up and you’re still a pound or two over. I didn’t understand at the time this sport was building character in me that would carry me through my life after.
When I got diagnosed with T1 diabetes at age 26 and had to completely change how I ate to achieve normal blood sugars. It was hard… but I already knew how to do hard. I had grit. Wrestling taught me that years earlier.
Thank you, @MatthewModine!
May 4

I’m often asked about the pegboard scene in VISION QUEST. That was all me. No stunt doubles or safety measures. I trained for a long time and had to climb it several times to get all the angles. The “trick” is not to over extend, so you’d be pulling up your entire body weight. You have to keep it compact. Arms and elbows tight. 💪🏽
You can support the @FMJDiary project by bidding on a signed VQ poster here: ebay.com/itm/206252131912
2
17
736
Dr. Ryan Attar retweeted

You forgot to remove the quote from your ChatGPT generated AI response
2
2
15
536
Dr. Ryan Attar retweeted
24 Jun 2024
10 years ago, I had the honor of shadowing Dr. Bernstein at his office. It was an incredible experience that still impacts the management of my own T1 diabetes and that of my patients today. Read about my time with Dr. B in this article I wrote back then diabetesdaily.com/blog/2014/…
9
17
127
5,156
Dr. Ryan Attar retweeted

Apr 17
Doctor: "I am truly feeling that our days are numbered because of AI."
407
347
2,389
151,851
Dr. Ryan Attar retweeted

Unfortunately, @drterrysimpson blocked me, but his other account @terrysimpson can hopefully see my reply🤗
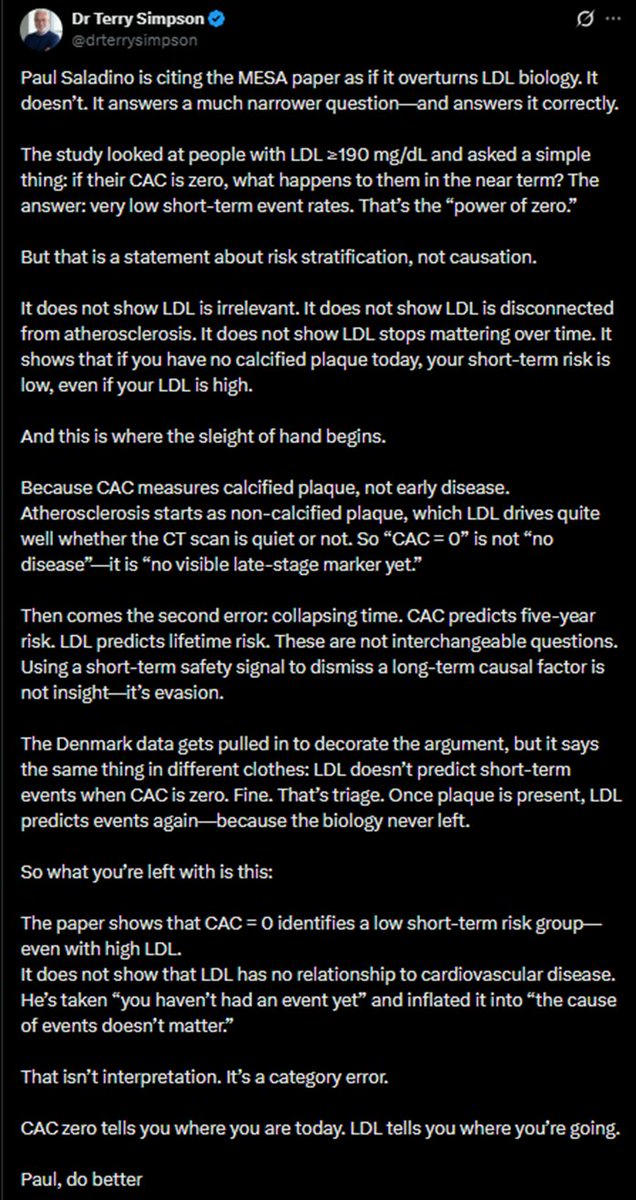
@paulsaladinomd's claim was that the association between LDLc and heart disease is “massively attenuated or not even present” in those who are “metabolically healthy.”
Then the video proceeds to cite data with respect to the “Power of Zero” for those with LDLc >190 mg/dl in an analysis of a MESA cohort here: pubmed.ncbi.nlm.nih.gov/3160…
While it is probably a reasonable inference that those with a CAC of 0 are more likely to be “metabolically healthy”, CAC 0 is not the same as "metabolically healthy" nor is "metabolically healthy" super well defined.
Likewise, technically, I wouldn’t say this paper specifically supports Paul’s claim given this paper does not really evaluate an association between LDLc as a continuous variable and CV events in CAC 0; however, it does denote a low incidence of CV events in CAC 0 w/ LDLc >190mg/dl – “incidence rate per 1000 person-years = 4.7; 10-year risk = 3.7%; risk/year = 0.4%”.
Of note, this was a median follow-up of 13.2 years - @terrysimpson indicates this is "short-term". This is well within a rescan window, and I guess I wouldn’t consider 13.2 years “short-term”.
The paper Paul would likely cite to support the lack of meaningful association with LDLc and CV events in CAC of zero is the Western Denmark Heart Registry Study, replicated in MESA from Circulation in 2023: pubmed.ncbi.nlm.nih.gov/3662…
“…a very high LDL-C level (>193 mg/dL) versus LDL-C <116 mg/dL was…not [associated] in those without CAC (aHR, 0.92 [0.48–1.79])”
👉🏻median follow-up is 4.3 years for WDHR, replicated over 16.6 years of follow-up in MESA…
“In the 3,340 individuals with CAC>0, the multivariable adjusted HR per 38.7 mg/dL higher LDL-C was 1.15 (p=0.004) compared to 0.91 (p=0.26) for the 3,361 individuals with CAC=0 (pinteraction =0.02 in fully adjusted model).”
I do think it is true that many providers don’t assess fasting insulin (I personally prefer c-peptide > fasting insulin) which would be a proxy for how “metabolically healthy” someone is to a degree, but I would argue the vast majority of providers look at fasting glucose so this claim from Paul is silly/hyperbole IMO; if fasting glucose is >100mg/dl, most providers are almost always running an A1c in response.
I do think many providers put excessive emphasis on total cholesterol and/or LDLc on a lipid panel as a risk stratification tool – neither of which are generally very helpful for this purpose in light of imaging.
Paul then indicates “In metabolically healthy individuals, a slight rise in your cholesterol because you’re eating more saturated fat and less seed oils, I don’t think there is a shred of evidence in the medical literature to suggest that is going to increase your rate of cardiovascular disease.”
I don’t really think this wording is super precise, but I don’t think most would argue that if LDLc increases but ApoB does not from an incorporated food, there is unlikely a significant increased incidence of CV events.
A subgroup from PESA with optimal CV risk factors demonstrated an association with LDLc and subclinical atherosclerosis, not events (though 94% had CAC 0 - pubmed.ncbi.nlm.nih.gov/2924…); a subgroup of MiHeart with optimal CV risk factors failed to find a significant association between ApoB and subclinical atherosclerosis [perhaps underpowered] (pubmed.ncbi.nlm.nih.gov/3912…) and likewise, ApoB >120 appears to have no significant association with events in CAC 0 vs ApoB <120 mg/dl over median follow-up of 13.9 years. (x.com/ApoDudz/status/2037746…).
I think if consuming any specific food that helps to improve/maintain optimal body composition via aiding in satiety and supports energy levels to improve/maintain excellent cardiorespiratory fitness and you have CAC 0, I am not certain that food’s effect on LDLc and/or ApoB is likely meaningfully changing the incidence of CVD over the lifespan of a human with possible rare exception.
Soft plaque is unlikely clinically meaningful in CAC 0 over 6.6 years within the window of rescan: x.com/ApoDudz/status/1969043…
I would argue minimal CAC is not end-stage or late-stage marker in any pragmatic sense, its subclinical disease that can be treated aggressively depending on age. Minimal CAC offers plenty of time to intervene with excellent prognosis to avoid unnecessary pharmacotherapy for years to decades.
I don’t think Paul technically claimed he was overturning LDL biology or LDL causality in atherosclerosis; I think he was referring to risk stratification.
CAC of 0 generally predicts very low risk within a reasonable scan window within 3-7 years.
x.com/ApoDudz/status/1936266…
“CAC zero tells you where you are today. LDL tells you where you’re going.”
I would say CAC 0 tells you that you likely to have a low incidence of CV events over at least 3-5 years, at which you can rescan and treat minimal CAC aggressively if needed and LDLc doesn't appear to tell you much of anything within this time frame.
21 Jun 2025

🧘🏼Baseline CAC 0, CHD events:
⚪️ 0.7% over initial 5 years…
🤸🏼Rescan at 5 years, CHD events:
🔵 1.8% in those who remained CAC=0 (28%) over following 5 years
🔴 5.7% in those who developed CAC (72%) over following 5 years

15
6
17
2,899
Dr. Ryan Attar retweeted

Apr 15
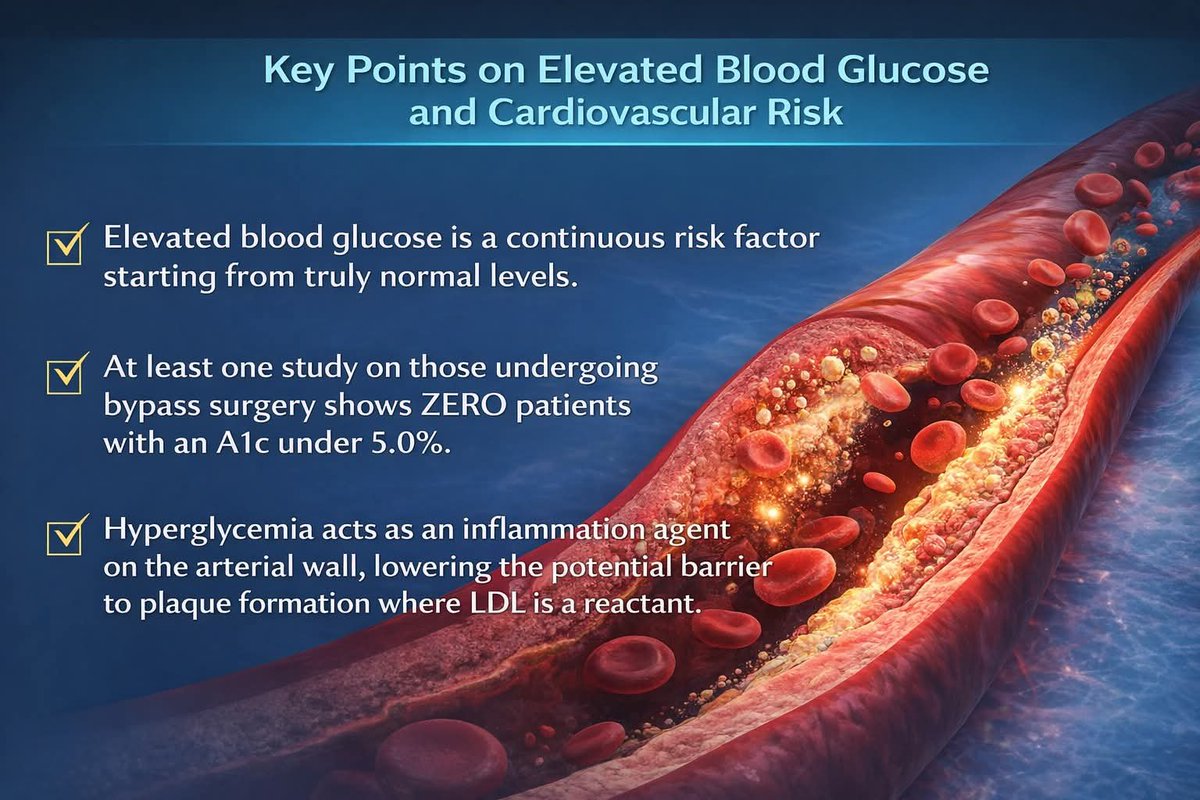
Great find. Loved this one "In the atherogenic reaction picture, LDL provides one substrate, but hyperglycemia lowers the potential barrier at the vessel wall; and as any physicist knows from catalysis and activated processes, the kinetics are often governed far more by barrier height than by modest changes in reactant concentration."
1
1
7
436
Dr. Ryan Attar retweeted
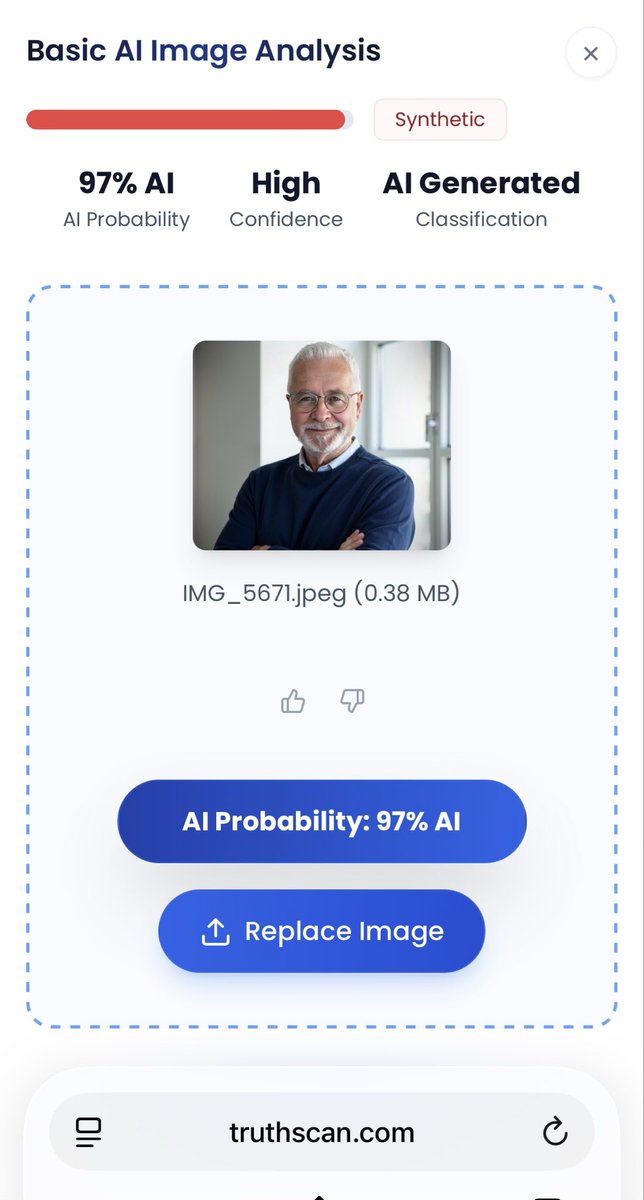
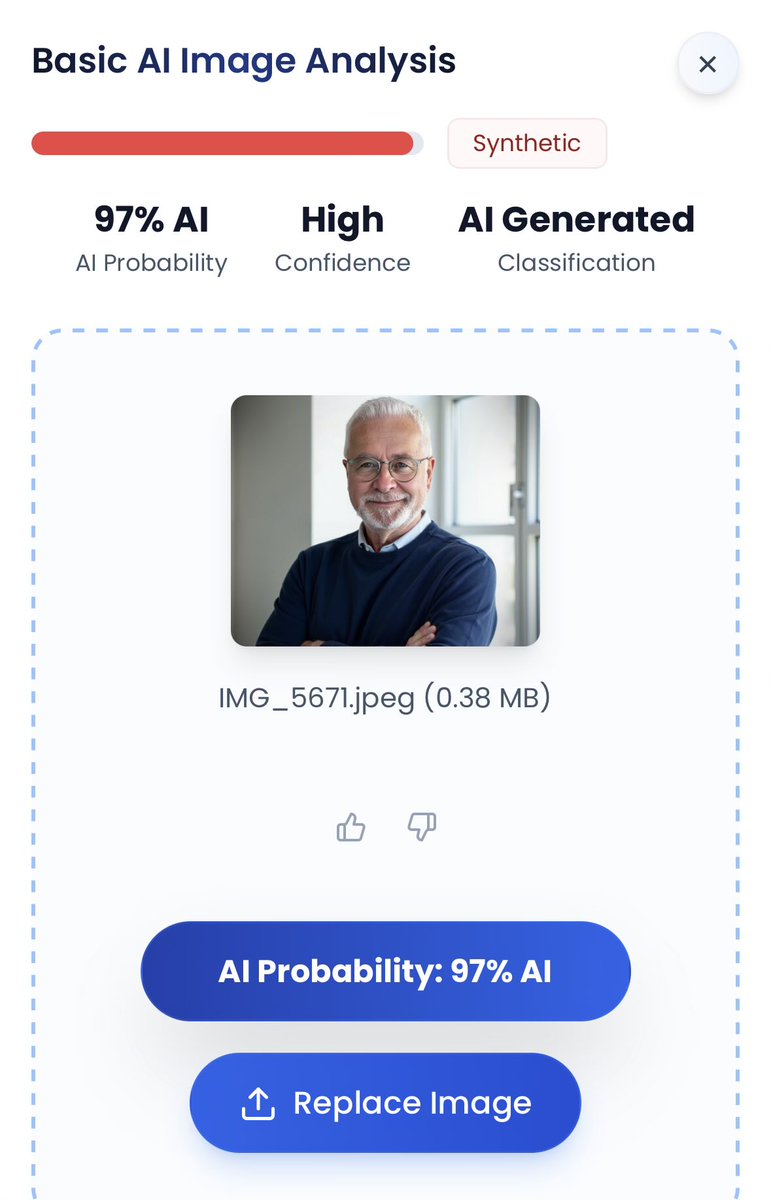
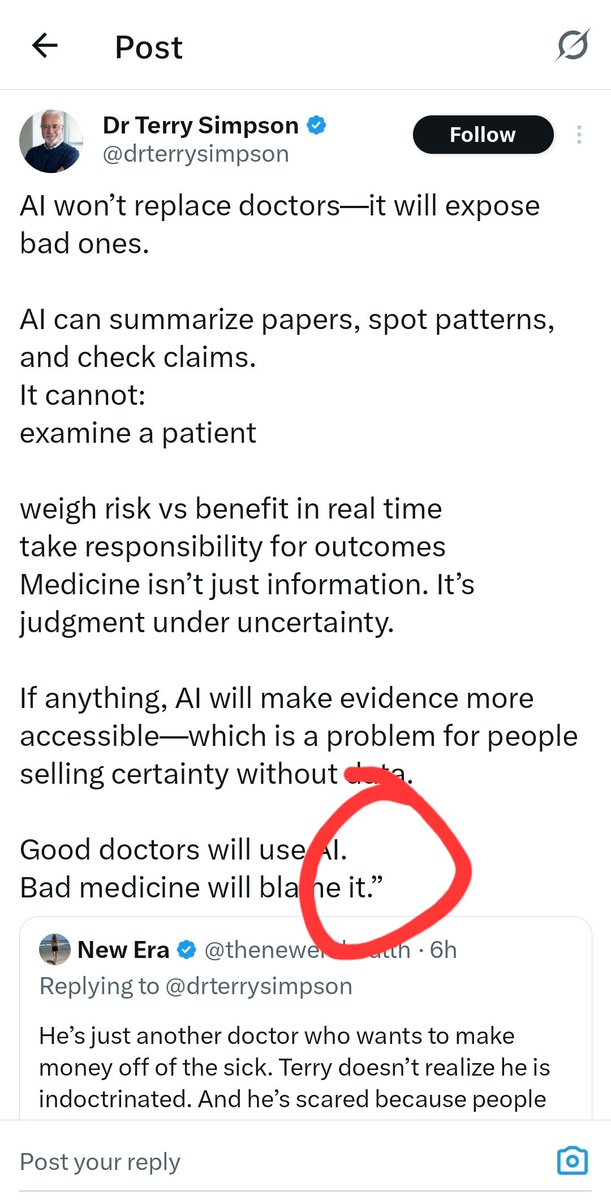
If you don’t outsource your writing, your social media manager almost certainly does based on a credible AI writing checker, @pangram.
There is no contraindication here, Terry.
Let me be clear: I have ZERO issue with the use of AI to generate content, fact check, or otherwise.
You have made claims that you don’t use AI to generate content.
A credible AI writing checker has indicated that the original post is 100% AI-generated with high confidence.
Pointing this out is not childish behavior – it is one of integrity and transparency.
If you would just admit that you (or your social media manager) generate this content using AI, I will be happy to go back to the playground with my childish friends.
You can ironically ad hominem me all you want.
I am happy to craft a post to directly address your claims in your original post (one that I will actually write myself) - truthfully, I didn't think your post was inaccurate albeit I didn't read it closely because that is tangential to my point and your claim that you do not use AI to generate content.
Anyone with more than 2 brain cells and 10 minutes with ChatGPT can spot the hallmarks of AI writing. Your inconsistent use of hyphens, style, and tone are a dead give-away. You can even see where your reply here was generated by AI (red boxes - elegant writing) and then where you begin to write (blue box). And then sprinkle AI and your (or your social media manager’s) writing throughout.
1
5
224

Dr. Ryan Attar retweeted
Apr 7
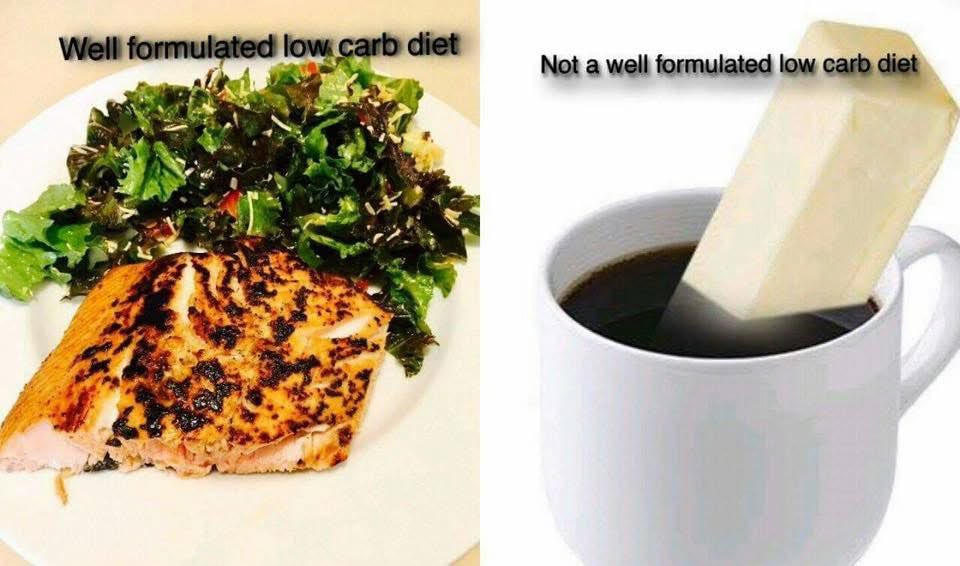
Low carb is great for diabetics, but for T2s especially those with fat to burn, I’d do leaner ground beef and a salad instead of this fat bomb.
1
7
823
Dr. Ryan Attar retweeted
The Europoor mind cannot fathom this much freedom

86
169
4,057
256,082
Dr. Ryan Attar retweeted
I just had a very disturbing Good Friday encounter with an ICE agent at the airport
As I was going through security, an ICE agent asked me for my ID. I told him this isn’t Soviet Russia and that the only citizenship papers I planned to show him were the Declaration of Independence
“Sir, I’m just asking for ID, not proof of citizenship,” he said.
“Today is the anniversary of Jesus’s resurrection,” I replied. “He was an American. Would you have asked to see his papers too? Would the scars on his hands not have been enough for you?”
He was stunned silent. I strode past him without showing my ID and went through the metal detector
I received a standing ovation
4,809
366
6,921
1,346,273
Dr. Ryan Attar retweeted
Mar 27
Pass the whole grain dinner rolls!
1
1
4
340
Dr. Ryan Attar retweeted
Mar 25
You are anti low carb. And you keep ignoring what I’m writing and moving goal posts.
3
1
11
1,117
Dr. Ryan Attar retweeted
Mar 25
@drterrysimpson, can you read?
Head to head, Mediterranean diets vs Mediterranean diet with reduced carbs, who wins?
Mar 25

Always so anti low carb, Terry!
Why not a Mediterranean diet while reducing the bread and pasta?
Mediterranean diets perform better on A1c and cardiovascular risk markers when carbohydrates are reduced.
pubmed.ncbi.nlm.nih.gov/2015…
1
1
4
318
Dr. Ryan Attar retweeted
Mar 25
Always so anti low carb, Terry!
Why not a Mediterranean diet while reducing the bread and pasta?
Mediterranean diets perform better on A1c and cardiovascular risk markers when carbohydrates are reduced.
pubmed.ncbi.nlm.nih.gov/2015…
4
4
24
1,477