
Joined October 2011
- Tweets 2,540
- Following 581
- Followers 73
- Likes 3,270
285 Photos and videos



Pinned Tweet

7 May 2024
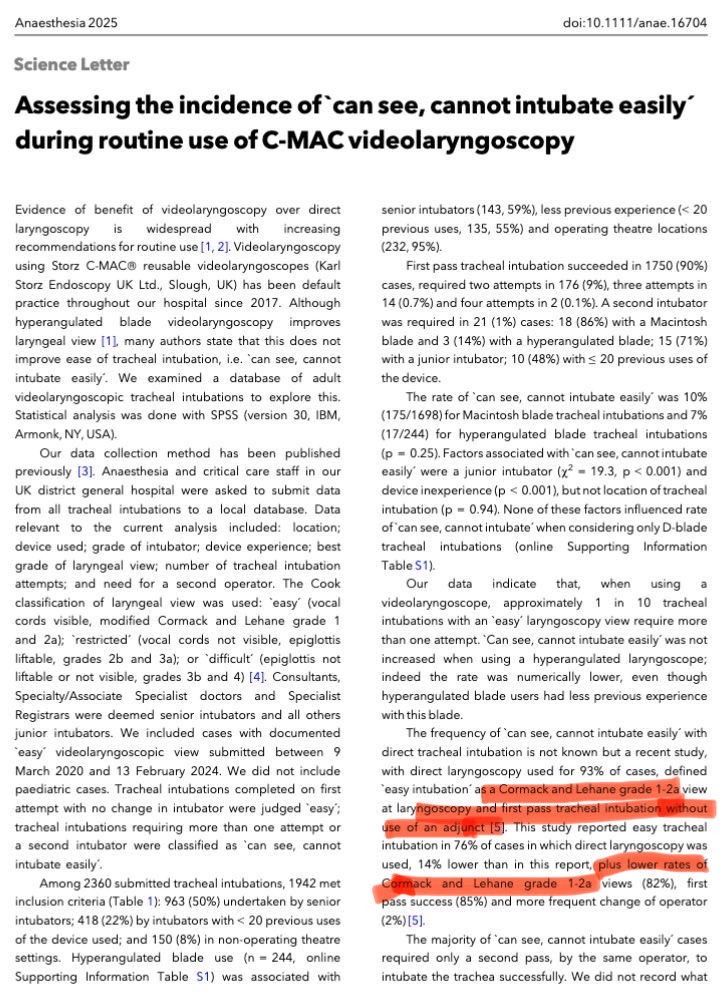
4/Point being made : MAC VL gives you superior laryngeal views than DL and superior training can get the ETT into the trachea without an introducer / Stylet.
1
772
Selvan Ramsamy retweeted

👏👏👏👏👇👇👇👇👇

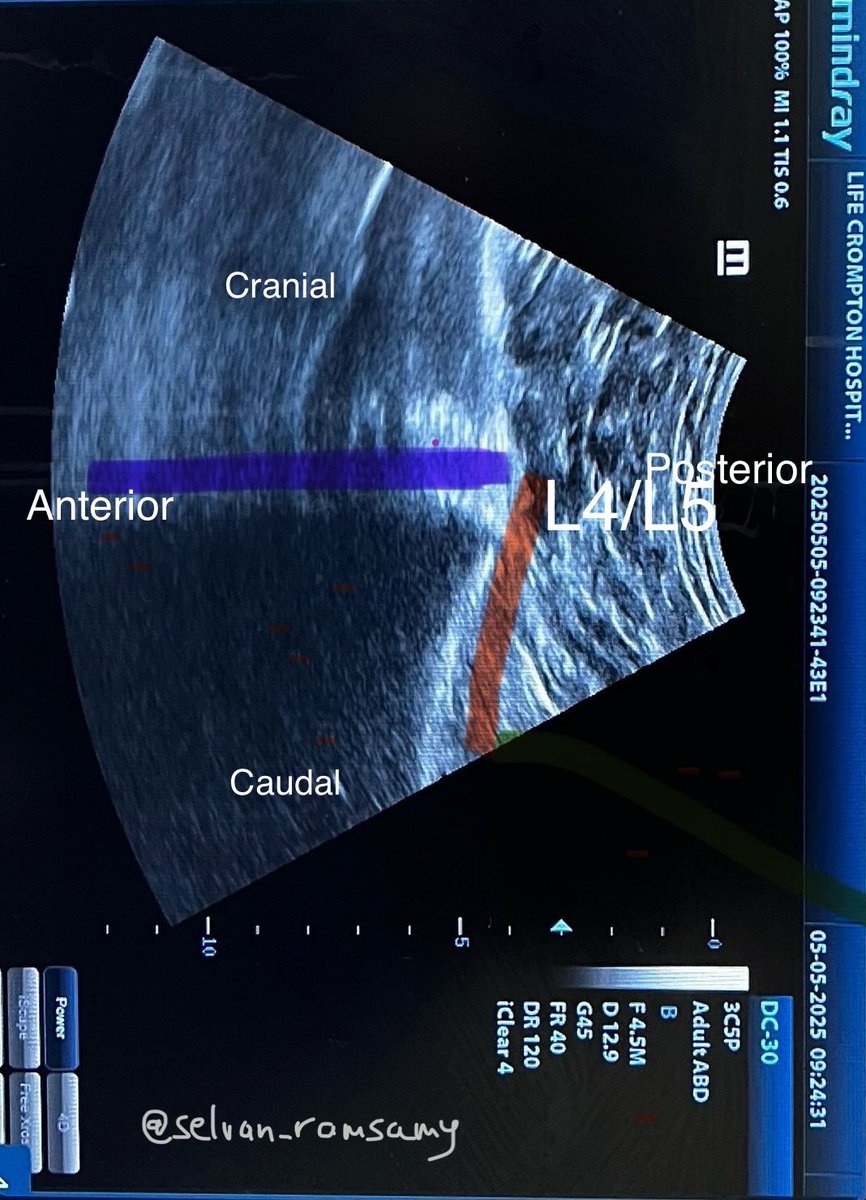
New video: Navigating the Difficult Spinal Anesthesia.
youtube.com/watch?v=ig_6uusG…
#CASAM2026 #Regional #Anesthesia #Spinal
1
5
11
1,412
Selvan Ramsamy retweeted

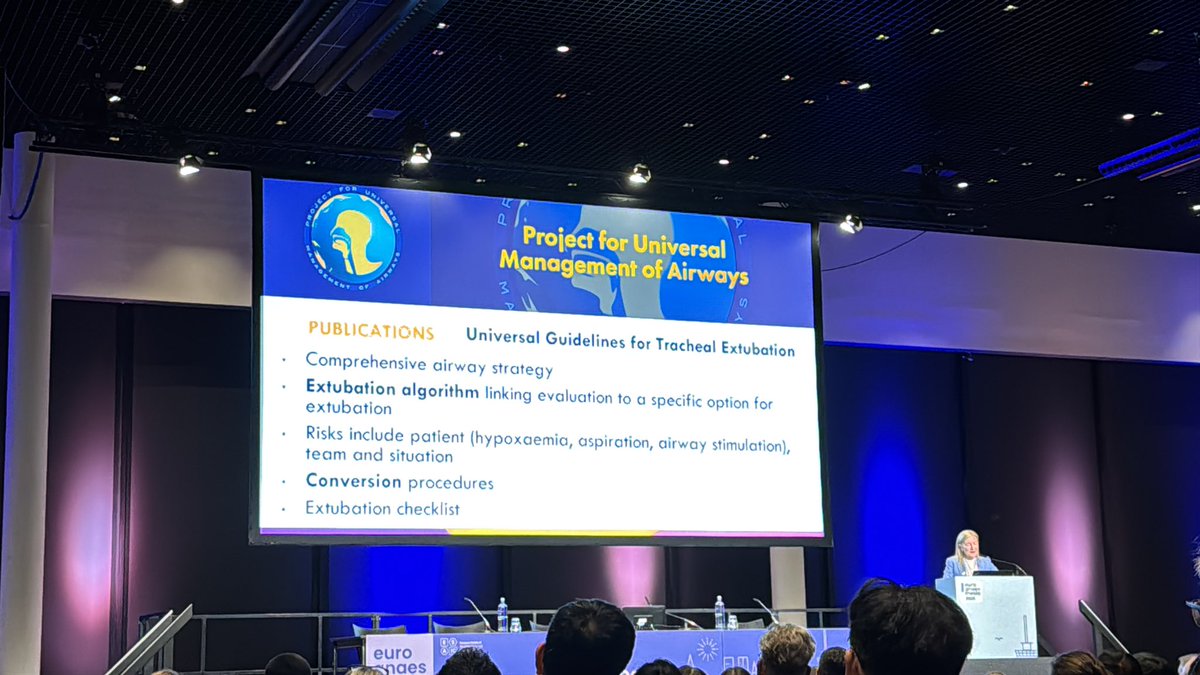
Ellen O’Sullivan teases the content of the upcoming PUMA Extubation guidelines being launched at the Airway SIG Meeting 27th Aug. Followed by launch of the Foundation guideline at #SAS2026 on Aug 28th. Both in Noosa, QLD, Aust
anzca.edu.au/events-and-cour…
sas-sas2026-annual-meeting.e…

@ProfEllenO @doctimcook @GongGasGirl
Extubation : dark side of airway management
« Extubation is a planned loss of the airway »
#ea26 #esaic
7
9
1,056
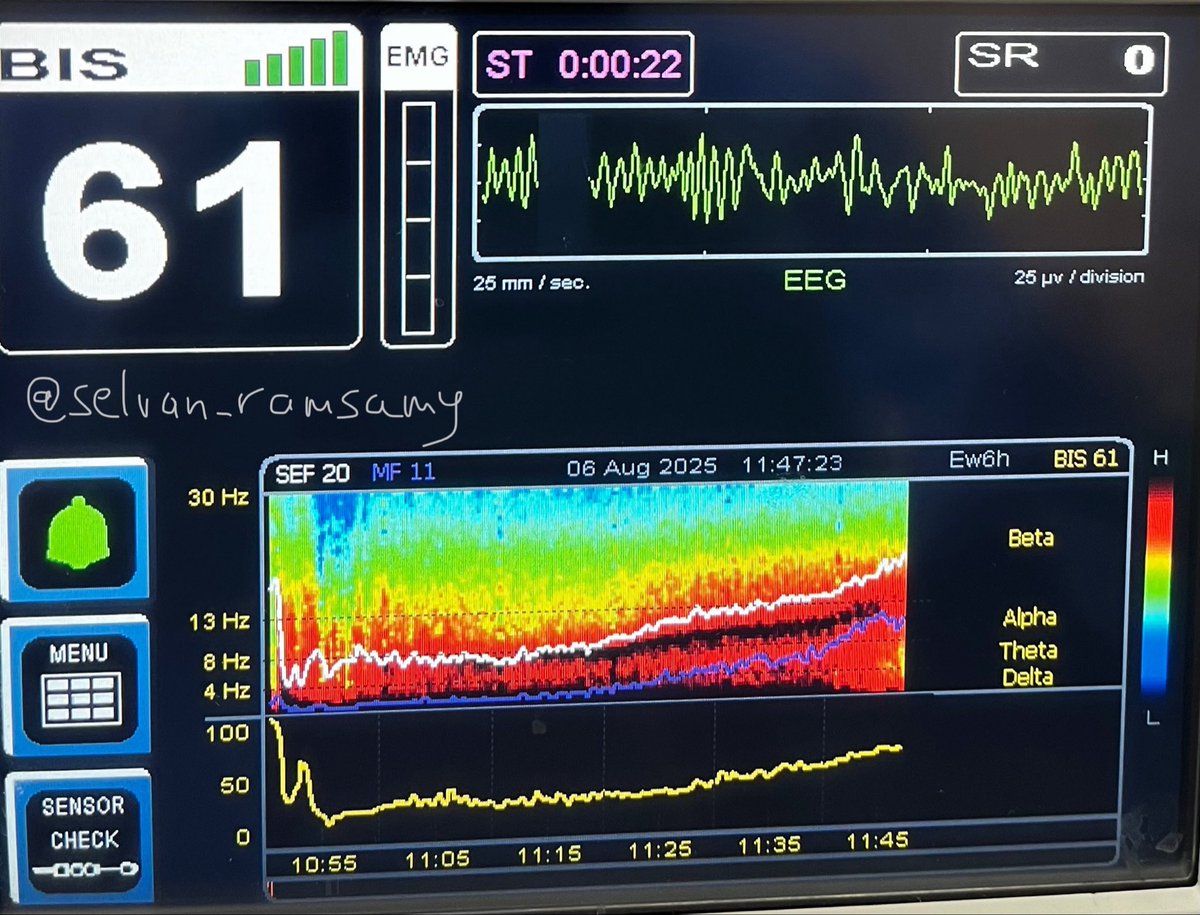
The old ( C&L Grade 1-4) works just fine . VL will not change the grading but does improve the accuracy of the grading because of the better laryngeal view .

How to document the view on #videolaryngoscopy to help communicate #airway management to colleagues - do we need to combine old and new systems? New editorial by Craig Lyons.

22
Selvan Ramsamy retweeted

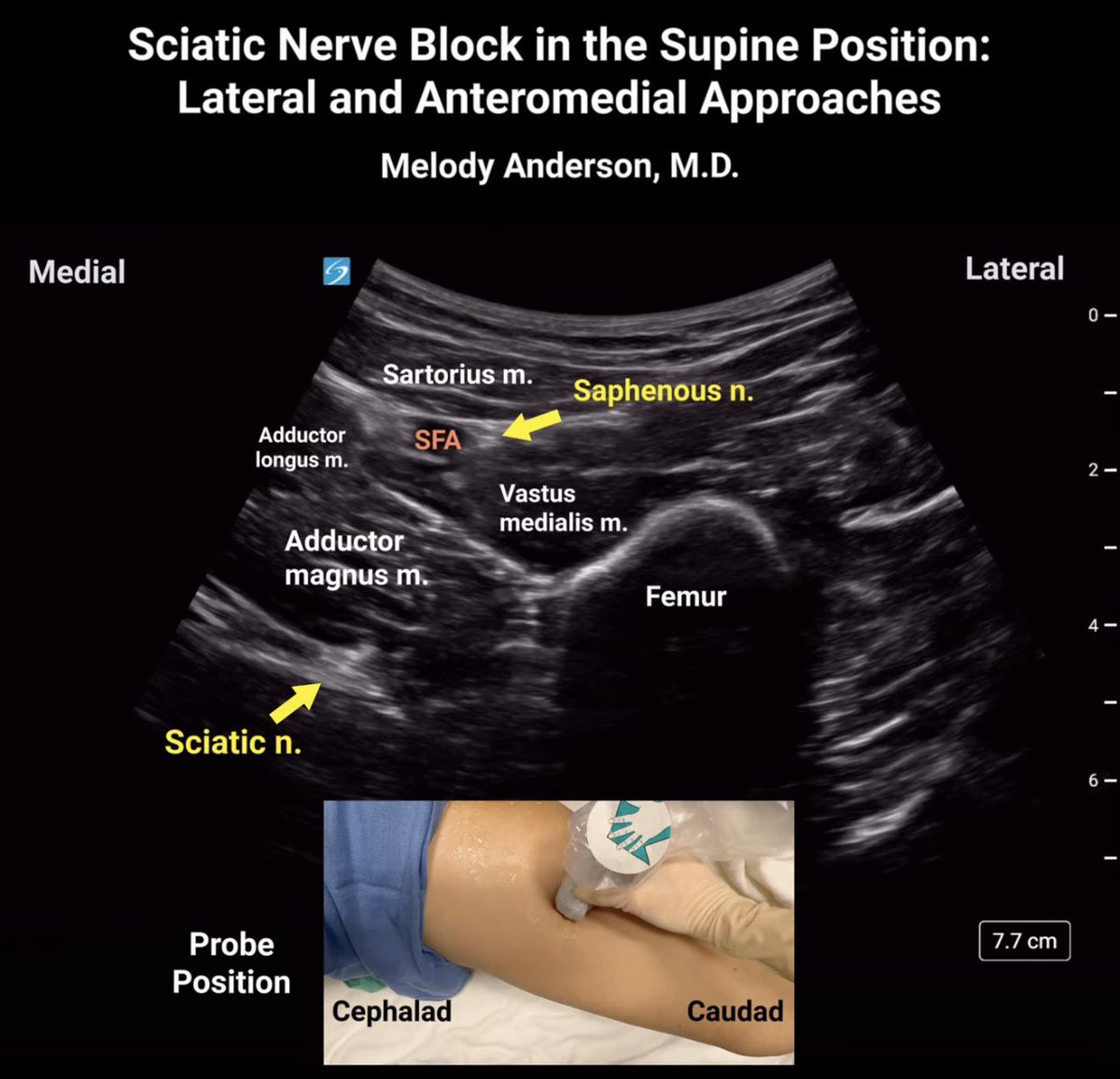
Sciatic nerve blockade in the supine position is highly effective for trauma patients and others unable to tolerate leg repositioning.
This video reviews lateral and anteromedial approaches to expand your regional anesthesia toolbox 💉🛠️
youtu.be/3pKka0aQKKo?si=T53h…
3
17
60
2,668
Selvan Ramsamy retweeted

May 12
✔️If a tracheal tube is accidentally placed in the oesophagus, a capnogram is the gold standard to detect this and prevent hypoxia.
⛔️ The big universal 🌎 problem: on most medical monitors the ventilator pressure curves can look very similar to capnogram curves!! (See images 1 and 2)
⚠️This is a call to action for all capnograph device companies in the world to set shaded capnograph curve as default (Image 3). Open curves look like other measurements.
People have died because of this (Image 4)
Currently, on most monitors the default cannot be changed manually.
We need a universal shaded curve for capnography to increase patient safety.
If you care about patient safety: please #retweet and #share.
@doctimcook @NaveenEipe @dasairway @wei_huafeng @cliffreid @altgm @ProfEllenO @SheilaMyatra @jducanto @NicholasChrimes @NightShiftMD @ProtectedAirway @EM_RESUS @emcrit @maffygirl @AnRocad @DaveOlvera1 @Philips @Masimo @Verathon @HamiltonMedical @storz_karl @MassGenBrigham @Siemens @Sony @Olympus_Corp @fisherpaykelAU @RUHAnaesthesia @oldandbaffled @PentaxMedical @SafeAirway @SaferSurgery @psmn999 #shadedcapnocurve #anaesthesia #patientsafety #criticalcare #ambulance




1
15
27
5,967
Selvan Ramsamy retweeted
Wow!
I am not sure I agree with the paranormal comparison here in this opinion piece by some very respected authors.
As we are learning, there is some nuance to performing this block correctly, and it still fulfils many criteria that make it a plan A block. Interesting 🤔
May 4

It was once thought that N-rays could explain paranormal phenomena such as telepathy or mind reading.
Are there parallels between the popularity and enthusiasm of erector spinae blocks plane today and that of N-rays in the past?
#anaesthesia #MedTwitter
doi.org/10.1111/anae.70226

6
6
18
6,950
Wordle 1,773 6/6*
Almost lost my streak on hard mode
⬜⬜🟨🟨⬜
🟩🟨⬜⬜⬜
🟩⬜🟨⬜⬜
🟩⬜🟨⬜🟩
🟩⬜🟩🟩🟩
🟩🟩🟩🟩🟩
18
Selvan Ramsamy retweeted

If can be intubated using VL, it is not a can’t intubate scenario.
1
1
1
711
Selvan Ramsamy retweeted

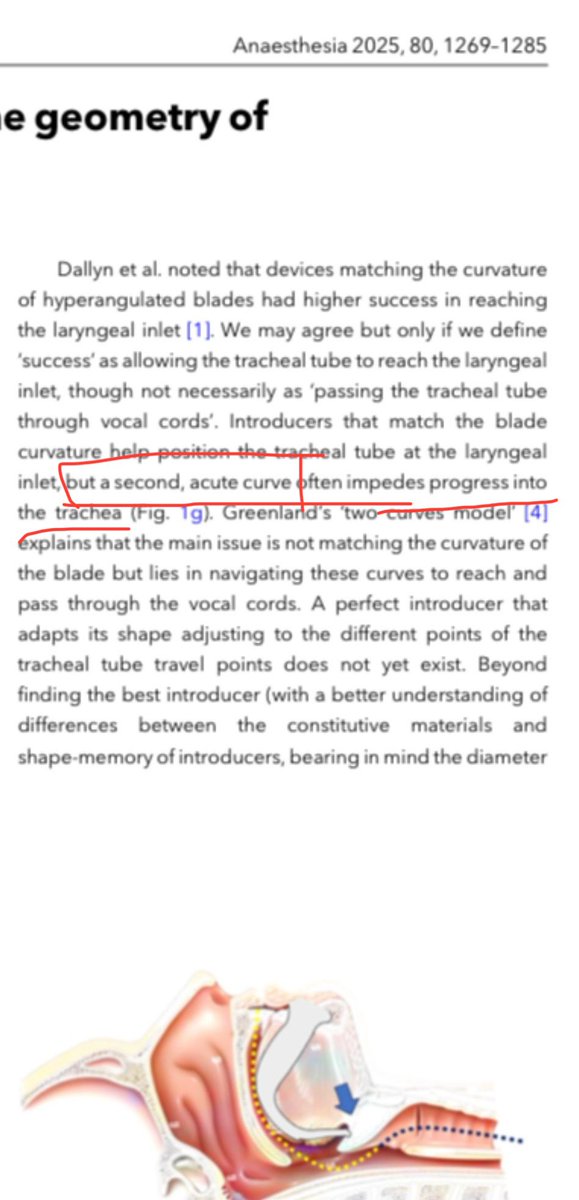
It's not really a myth else there wouldn't be an industry centered around bougies, stylets and introducers that get round the corner.
1
1
69
Selvan Ramsamy retweeted

Feb 5
Yes but what do we then do for airway management….?
We know the incidence of a non-empty stomach in all elective patients is around 5-6% (much higher in some series)
But the incidence of aspiration is around 1 in 10,000
That’s 600-fold lower
If we start doing RSIs or even intubating all these patients then there is a significant risk we’ll cause more harm.
So I think identifying who has a full stomach is the easy bit. Working out who is actually at high risk or deciding what to do about it is the complex one!
@kariem
11
15
81
13,921
Selvan Ramsamy retweeted
Feb 7
Why no? For all the reasons I’ve reasons I’ve explained, imo,
1
1
264
Selvan Ramsamy retweeted

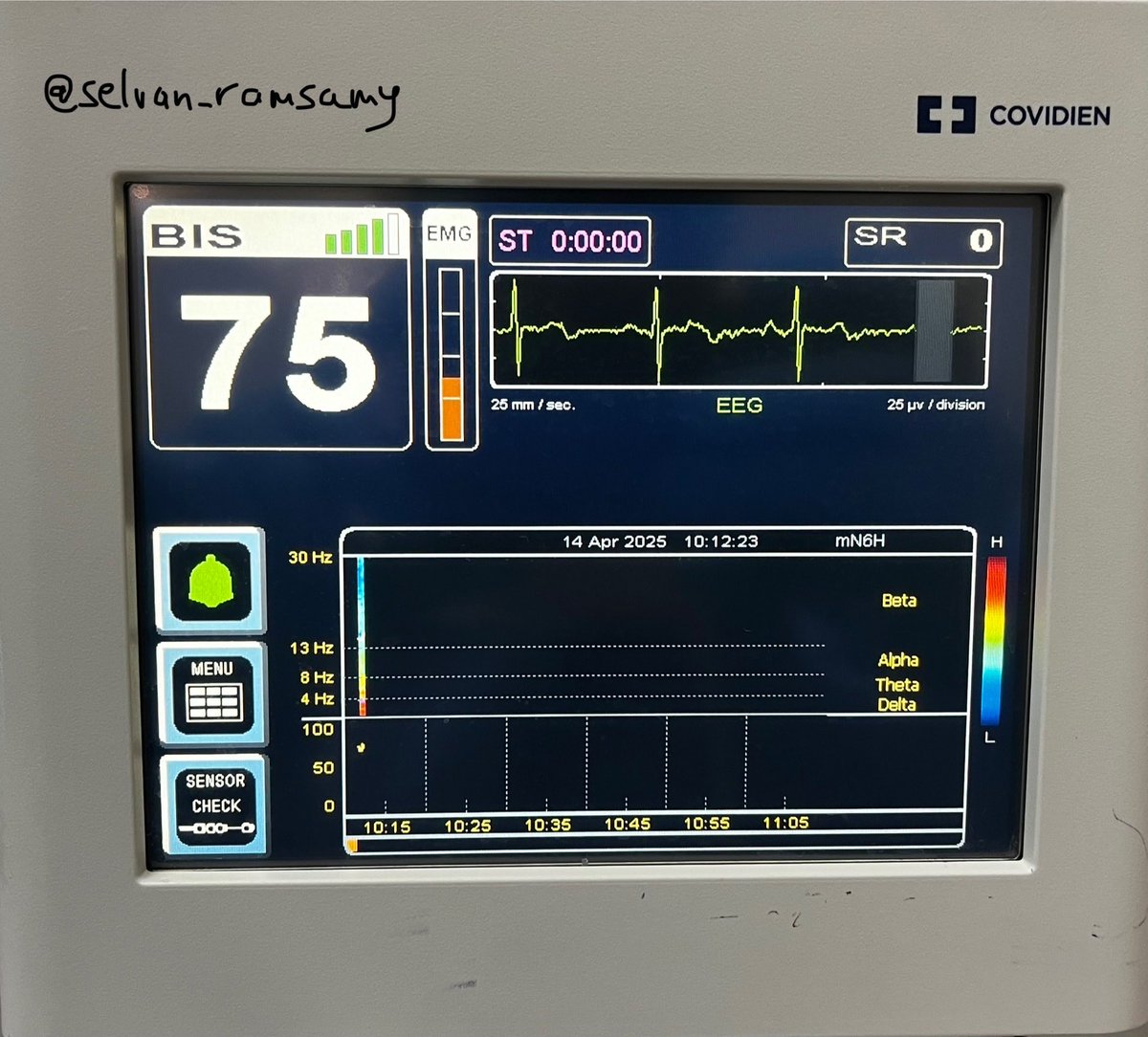
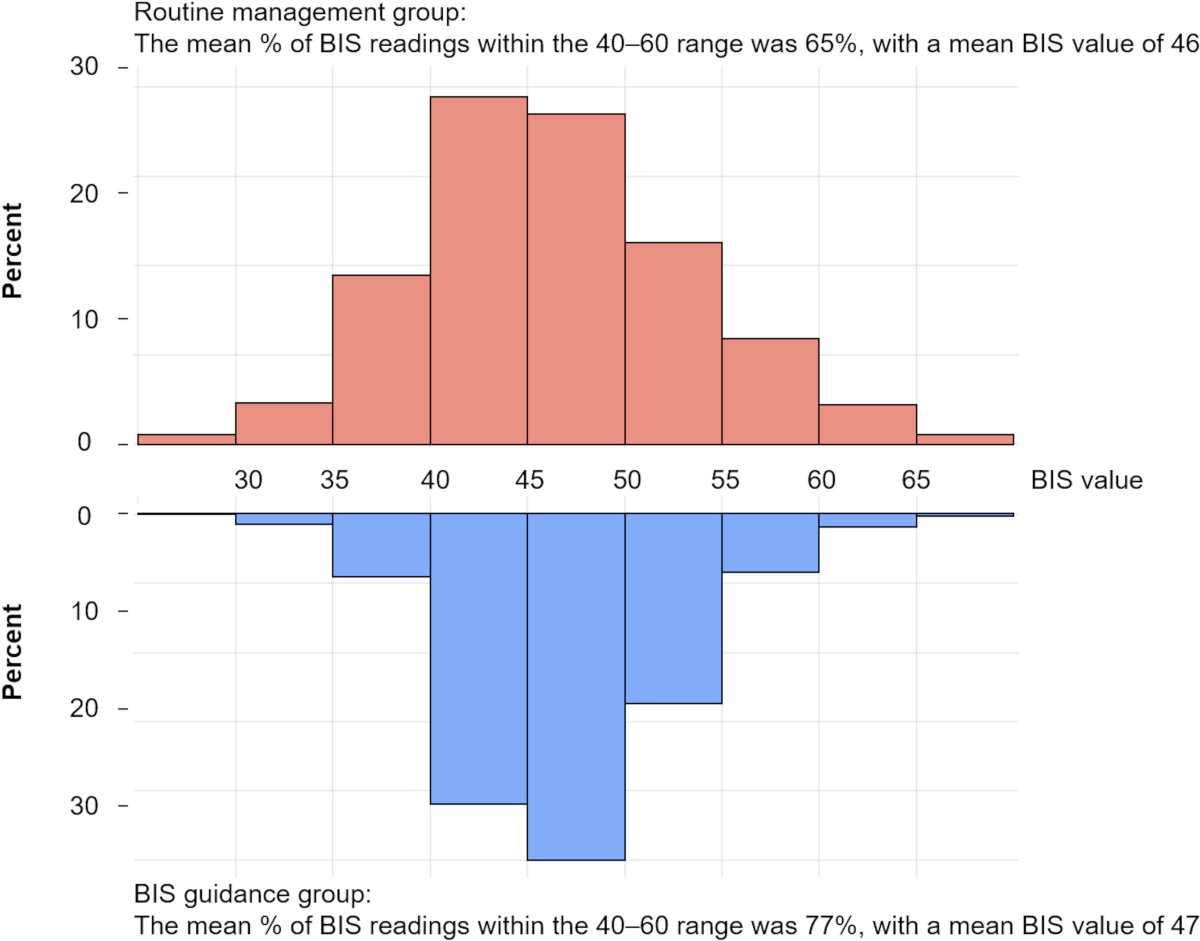
Older surgical patients are at risk because of age-related physiologic decline and comorbidities. In a new article, Zhou et al. analyze the effectiveness of a widely used monitoring device in improving outcomes.
Read the article: ow.ly/MsSn50Y5642
7
21
1,766
Selvan Ramsamy retweeted
Jan 7
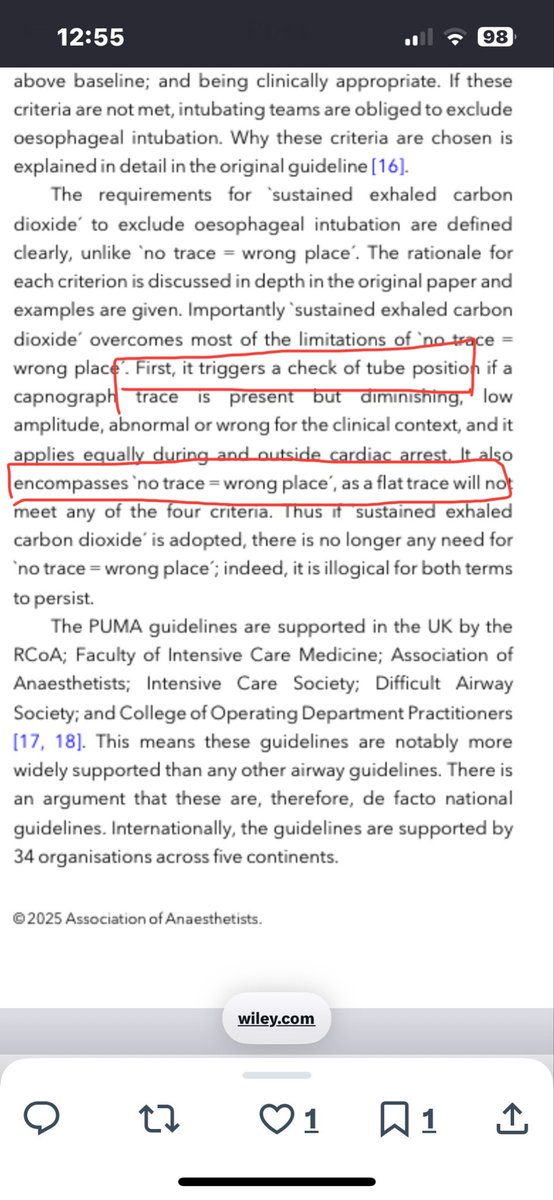
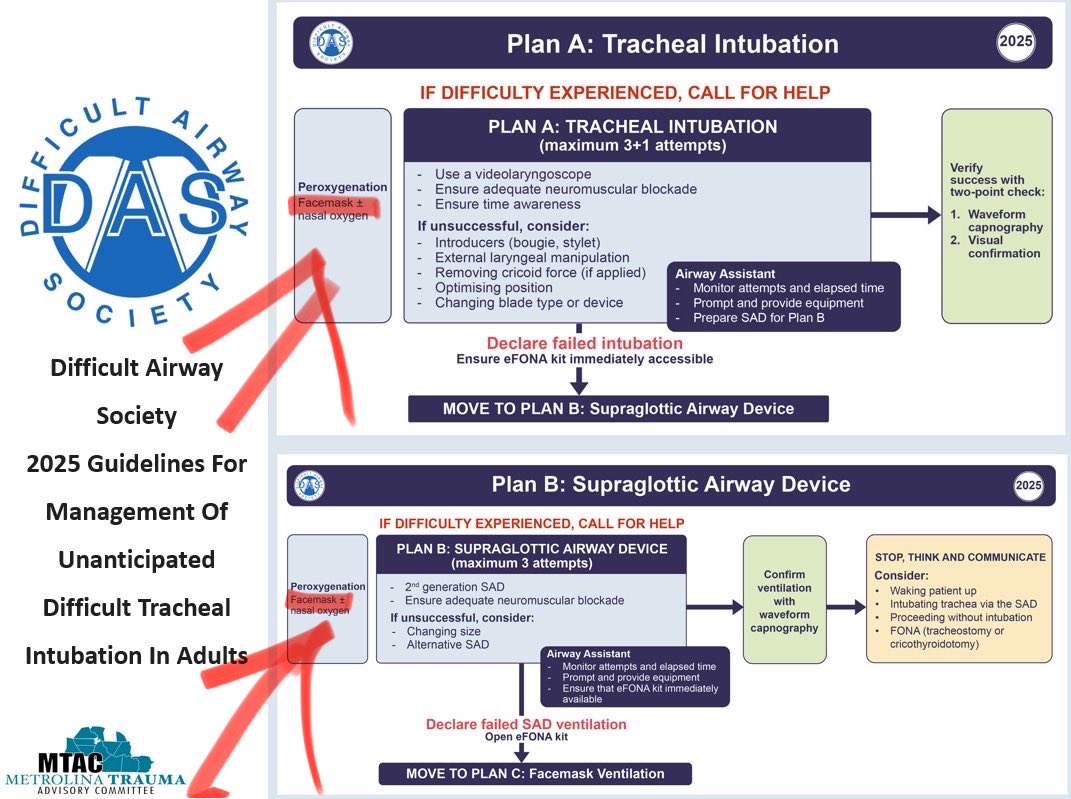
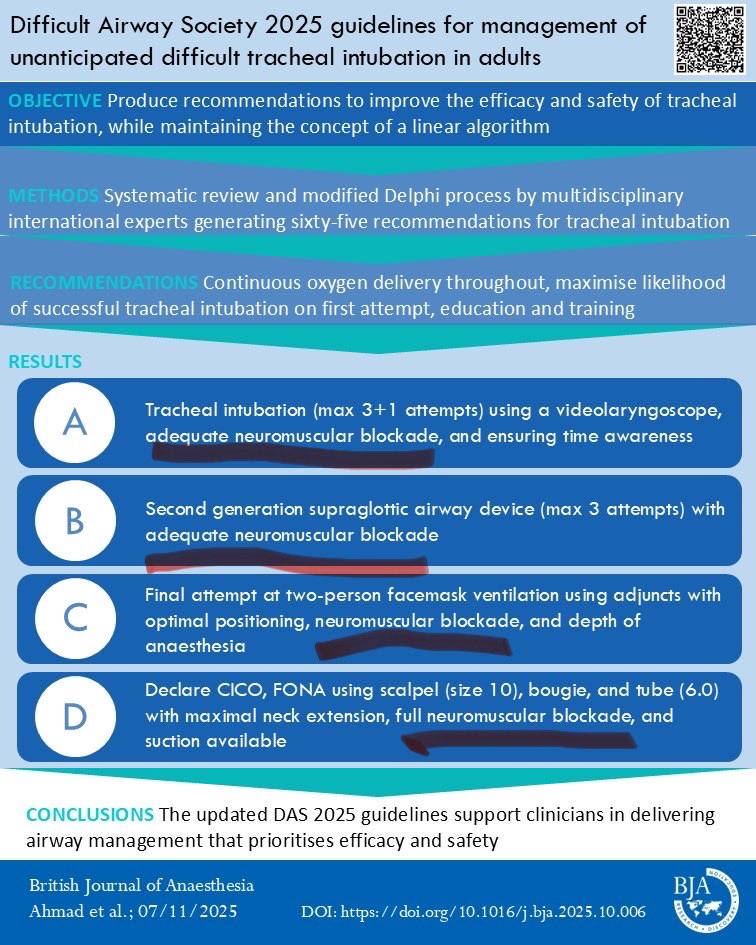
My comments regarding the new DAS2025 guidelines for management of the unanticipated difficult tracheal intubation.
📖 kwnsfk27.r.eu-west-1.awstrac…
@BJAJournals @NicholasChrimes @NaveenEipe @dasairway @navarroguillej @dr_imranahmad @maffygirl @DaveOlvera1 @PedsAnesNet @NightShiftMD
2
11
28
3,027
Selvan Ramsamy retweeted
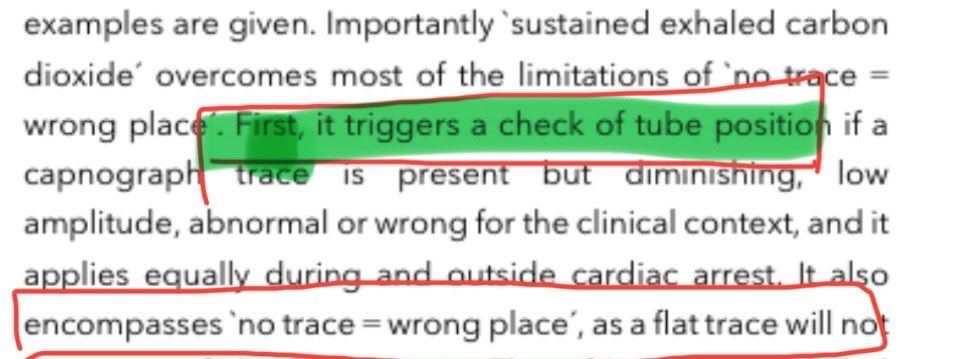
6 Dec 2025
No
NTWP is…..
Retired
Defunct
Gone
Exited
Done with
Deleted
Absent
Obsolete
…..It is no more.
(Please read the editorial if that’s not clear)
1
1
1
59
Selvan Ramsamy retweeted
4 Dec 2025
Let me ask a question and offer some observations…..
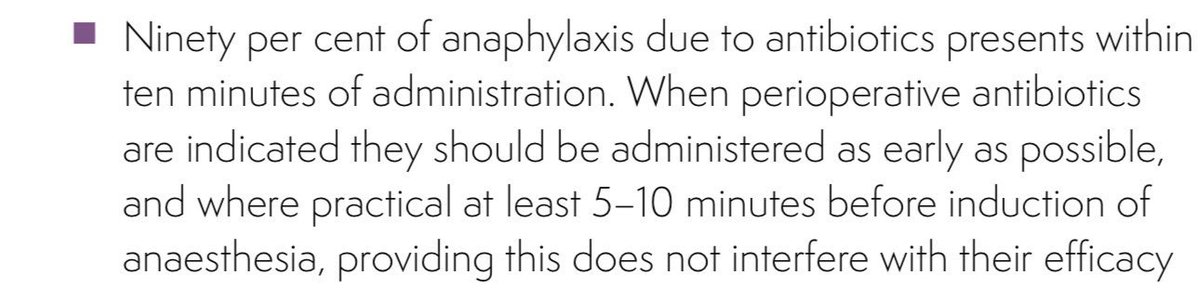
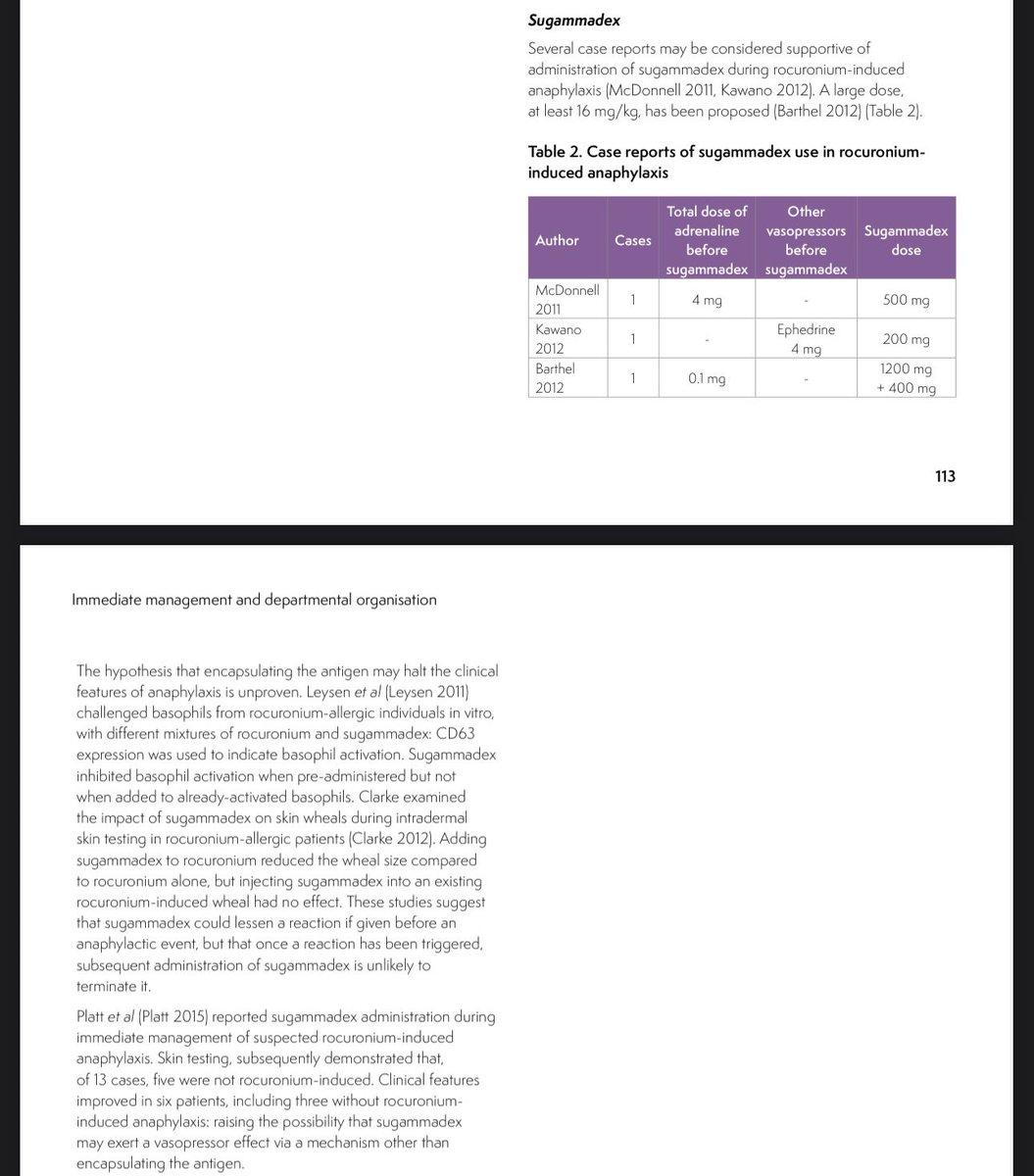
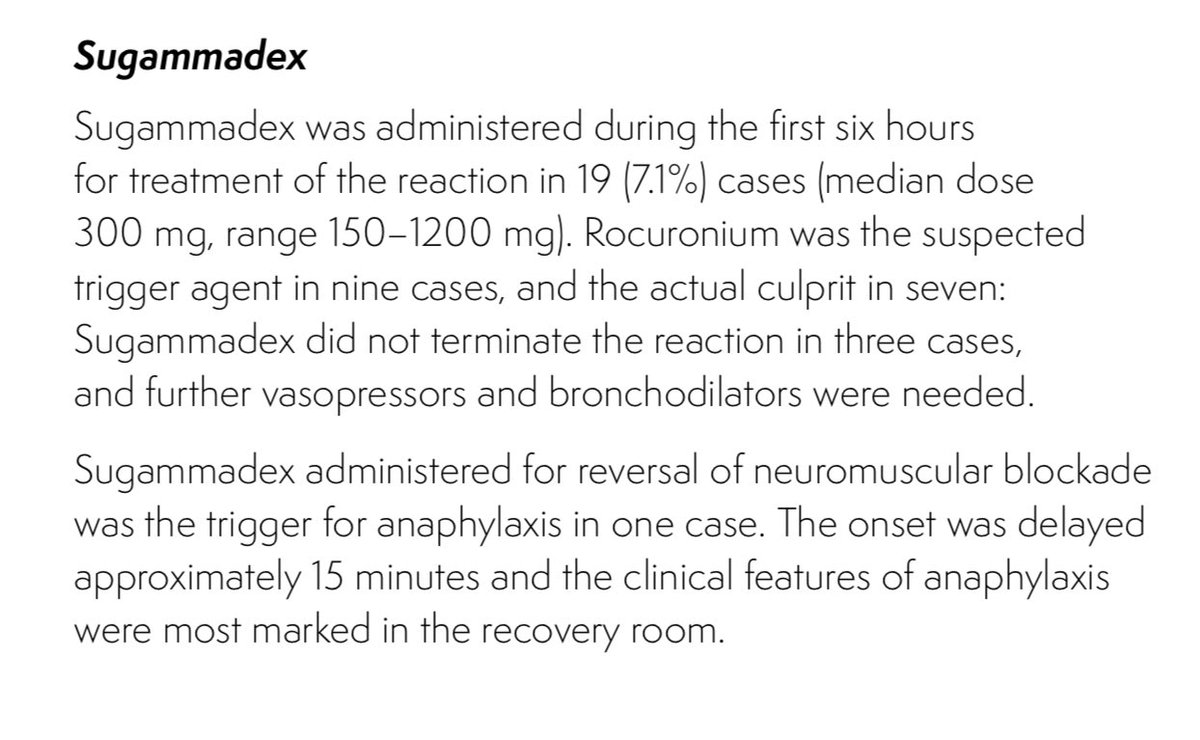
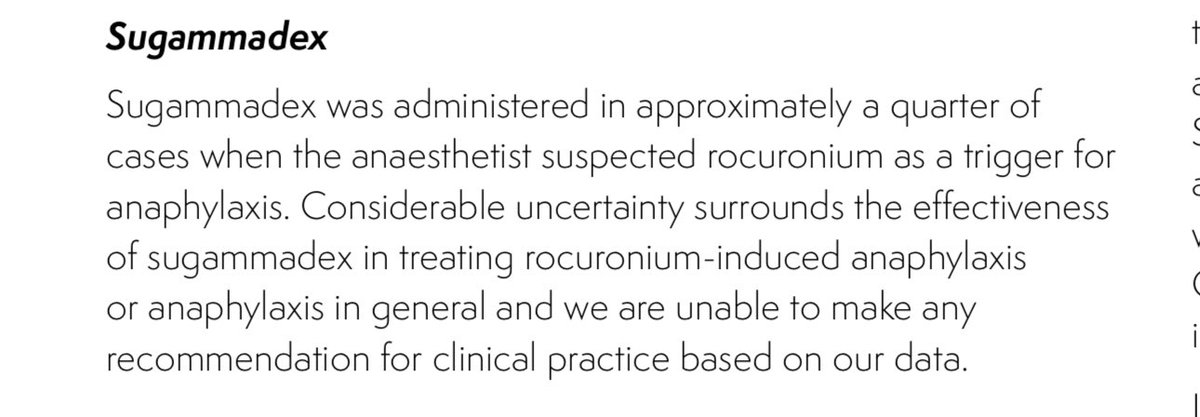
When we wrote NAP6 the evidence base for treating anaphylaxis to roc (or indeed to any drug) was pretty poor.
See rcoa.ac.uk/sites/default/fil… Has that changed?
The first drug to give in anaphylaxis is adrenaline (or you could use epinephrine if you’re in the USA😊😊)
The other interesting and relevant finding was that anaesthetists over-estimate the proportion of cases of anaphylaxis by NMBs by about 40%. Ie that they identify NMB as the culprit 40% more often than it is found to be the culprit on testing (chlorhexidine is one culprit easily forgotten)
Anaesthetists also over diagnose anaphylaxis as a cause of severe hypotension/ventilation difficulty…classically in cases of oesophageal intubation) #NAP7
See rcoa.ac.uk/sites/default/fil…
2
2
7
1,038
Selvan Ramsamy retweeted

27 Nov 2025
You cannot FMV during laryngoscopy attempts; so FMV in plan A refers to between laryngoscopy attempts
1
1
39
Selvan Ramsamy retweeted

23 Nov 2025
Medicolegal issues with AI:
If you include AI in your care of the patient, then you are obliged to let them know when seeking consent.
This includes if their data goes to a third party for data processing.

3
5
18
1,055
Selvan Ramsamy retweeted
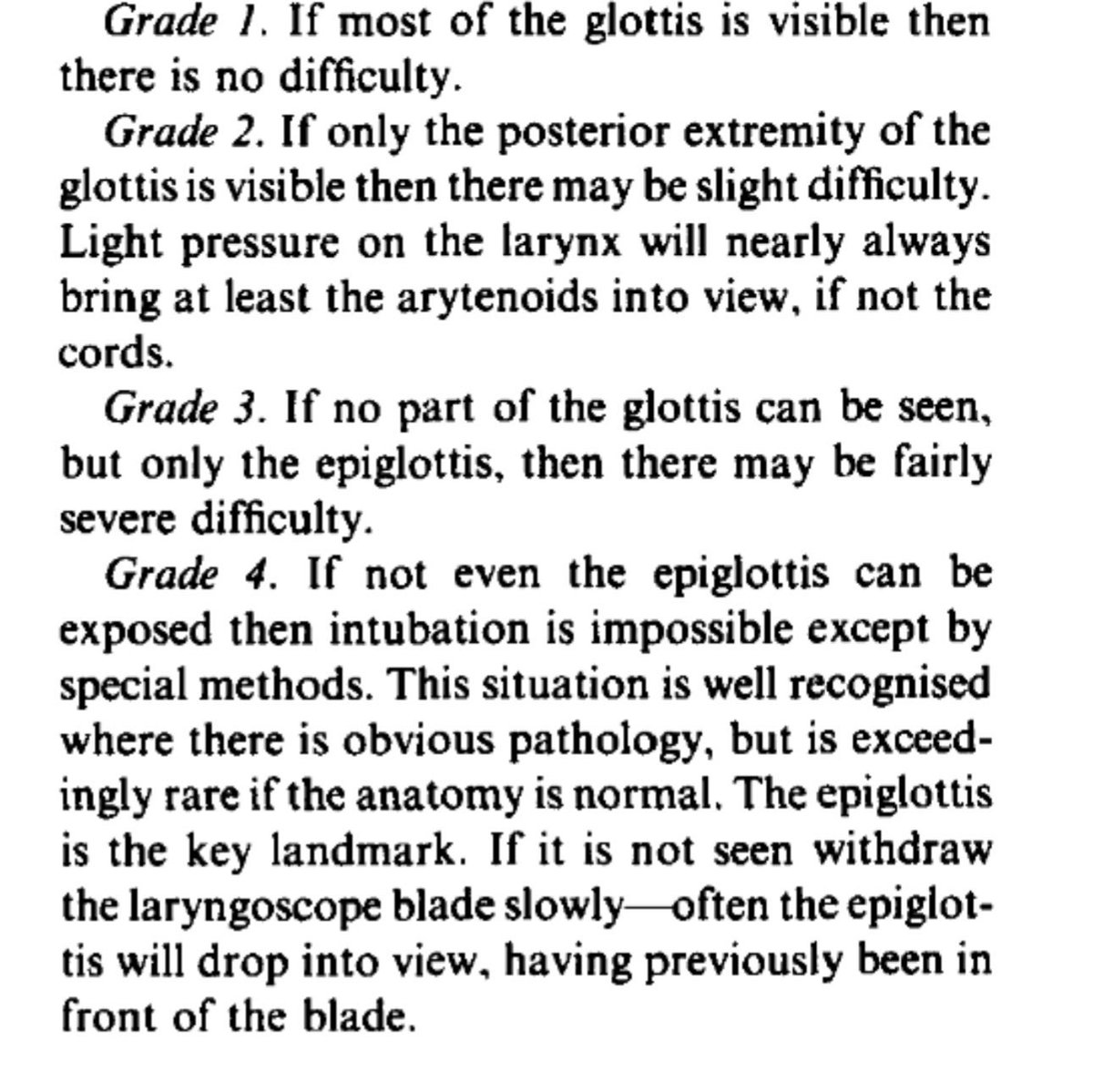
20 Nov 2025
I guess the trouble with a definition like that is that it it’s entirely open to interpretation
So let’s break it down….
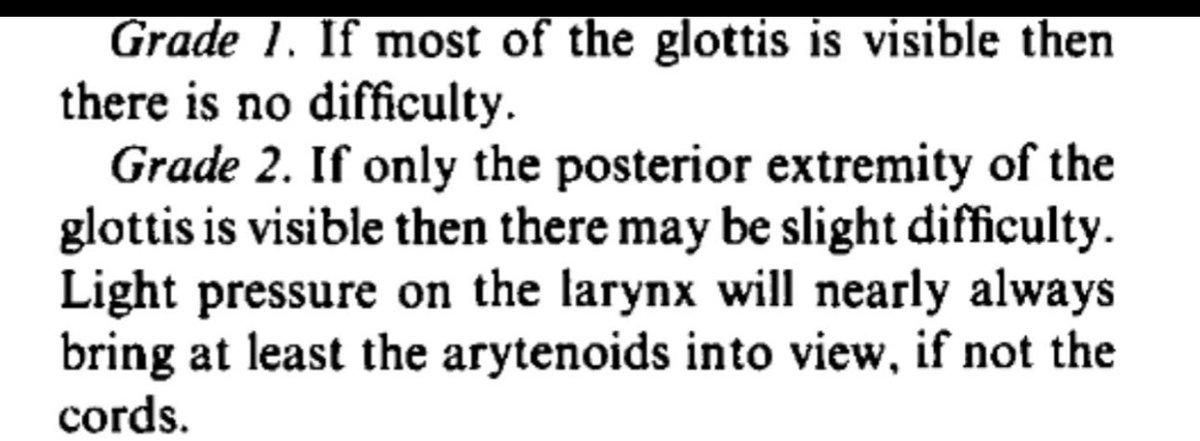
Is 95% most of the glottis? YES
Is 80% most of the glottis? YES
Is 63% most of the glottis? YES
etc etc until
Is 50% most….NO!
So we end up having to agree anything >50% = most of the glotts
That’s the logical definition, and what they’ve written
If asked ‘what % defines most of? I doubt you’ll get agreement on
95%, 80%, 63% etc
So I think technically it has to fall at 50%
However the kicker is that when C&L describe grade 2 they start with talk of the posterior larynx.
Grade 1 vs 2 has to have a cut off….one side grade 1 vs other side grade 2
Logically and technically this has to be 50% (unless the logic is that everything from 100% to at 10% is grade 1 with grade 2 only kicking in at POGO 20%….. which makes no sense because 20% most certainly isn’t most)
Even I don’t say that
The only attentive is POGO say 808 to 20% is a C&L wilderness, an ungraded no man’s land!
So logically and technically
>50% grade 1
<50% grade 2
@VirtueOfNothing
3
3
6
2,250
Selvan Ramsamy retweeted
21 Nov 2025
No
See my other tweets…
At the moment I think your proposal seems to be
Grade 1 = all re cords
Grade 2 = none of the cords
That leaves an ungraded vacuum in the middle……
And C&L grade is always the BEST view you can get so whether you’re moving the head or applying pressure is not relevant
1
1
1
171