
Joined June 2011
- Tweets 5,190
- Following 762
- Followers 698
- Likes 6,084
174 Photos and videos




Sofia Gambetta retweeted

Jun 4
A very impressive study for how we could prevent lung cancer more than 5 years before it is diagnosed. Using machine learning, discovery of a 14-plasma protein signature of risk that predicts responsiveness to an antibody therapy to interleukin, IL-1β
Validated across 8 cohorts
@CellCellPress @CharlesSwanton
cell.com/cell/fulltext/S0092…

31
322
1,016
173,075
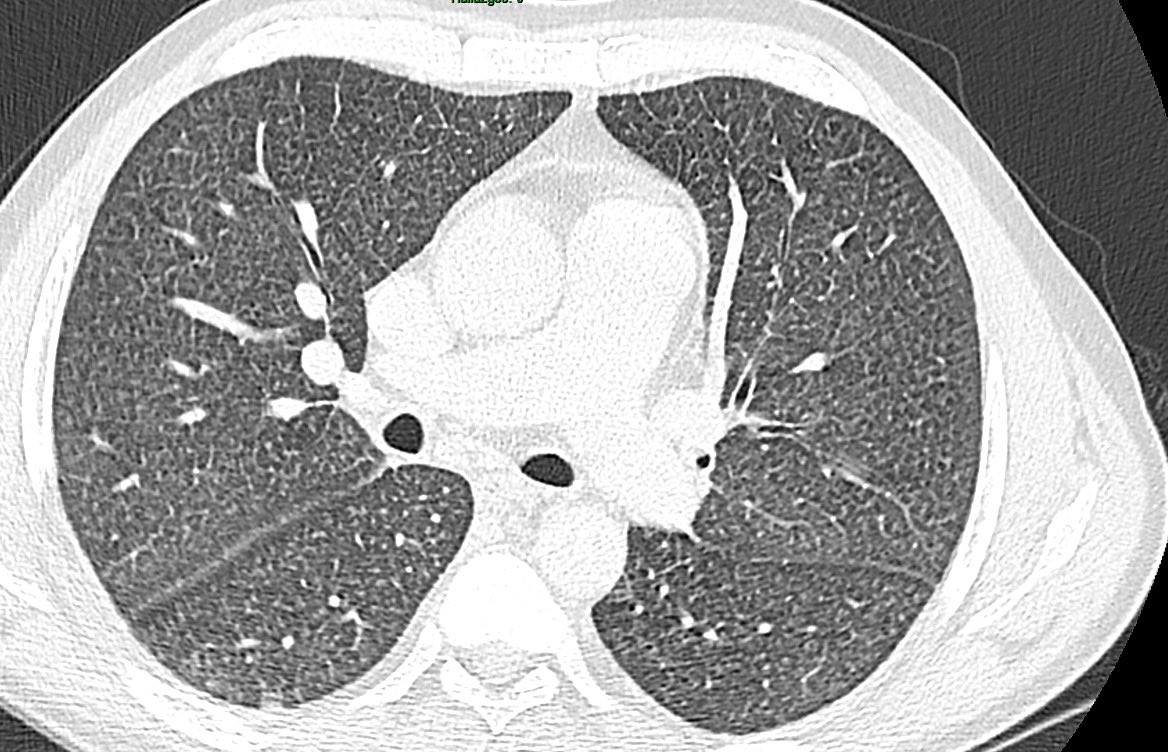
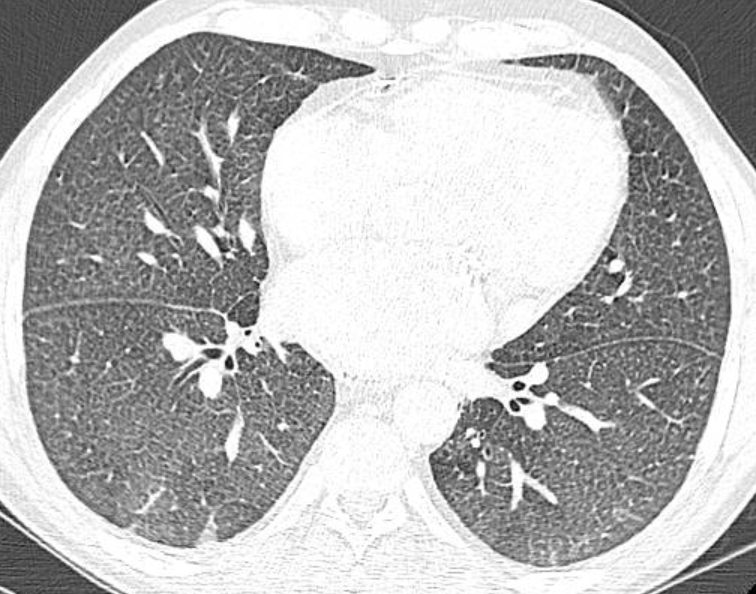
🧵 Seems like chronic pulmonary edema cases are following me lately 👀
I haven't found a pathognomonic CT sign described in the literature for this entity, but after seeing a few of these, I started calling it "nutmeg lung" 🫁
Has anyone else noticed this pattern? Is there a better name for it in your practice? 🤔
#Radres #FOAMed #RadTwitter
Jan 27

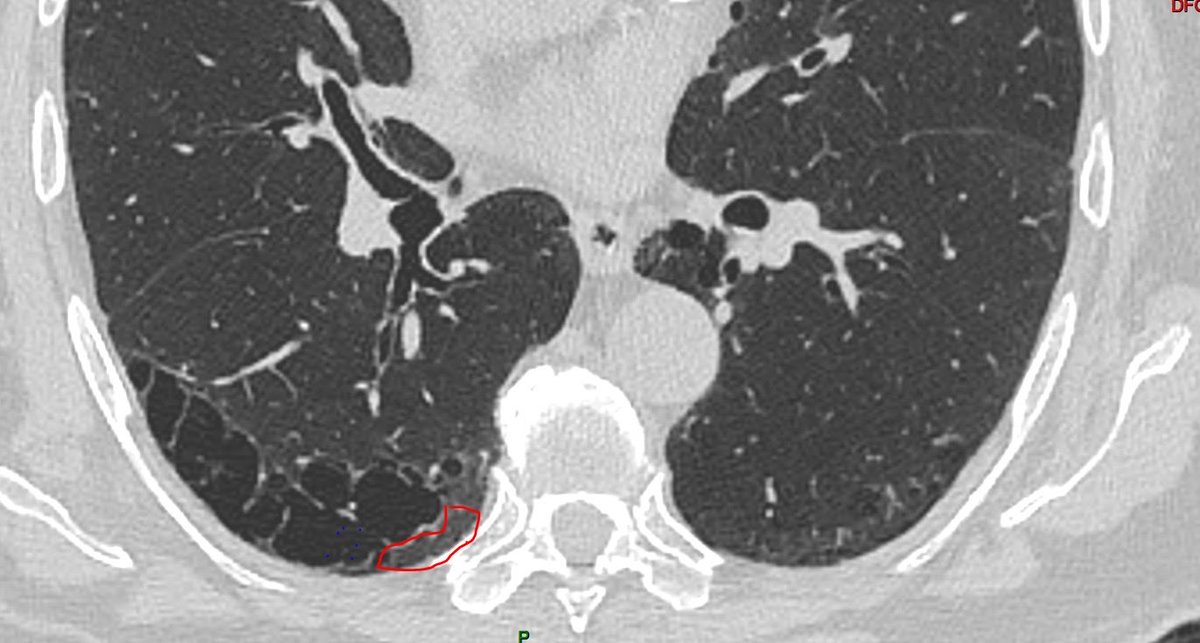
🫁 Challenging chest CT pattern
41-year-old male. Chronic kidney disease secondary to polycystic kidney disease
CT findings:
▫️ Innumerable miliary nodules
▫️ Bronchial interlobular septal thickening
▫️ Isolated mediastinal lymphadenopathy
▫️ No pulmonary edema
📌 With no additional clinical information, applying a pattern-based approach, the main differentials are:
1️⃣ Miliary tuberculosis
2️⃣ Hypersensitivity pneumonitis
3️⃣ Sarcoidosis
#RadTwitter #RadRes #ChestImaging #MedEd
1
1
11
1,392

May 16
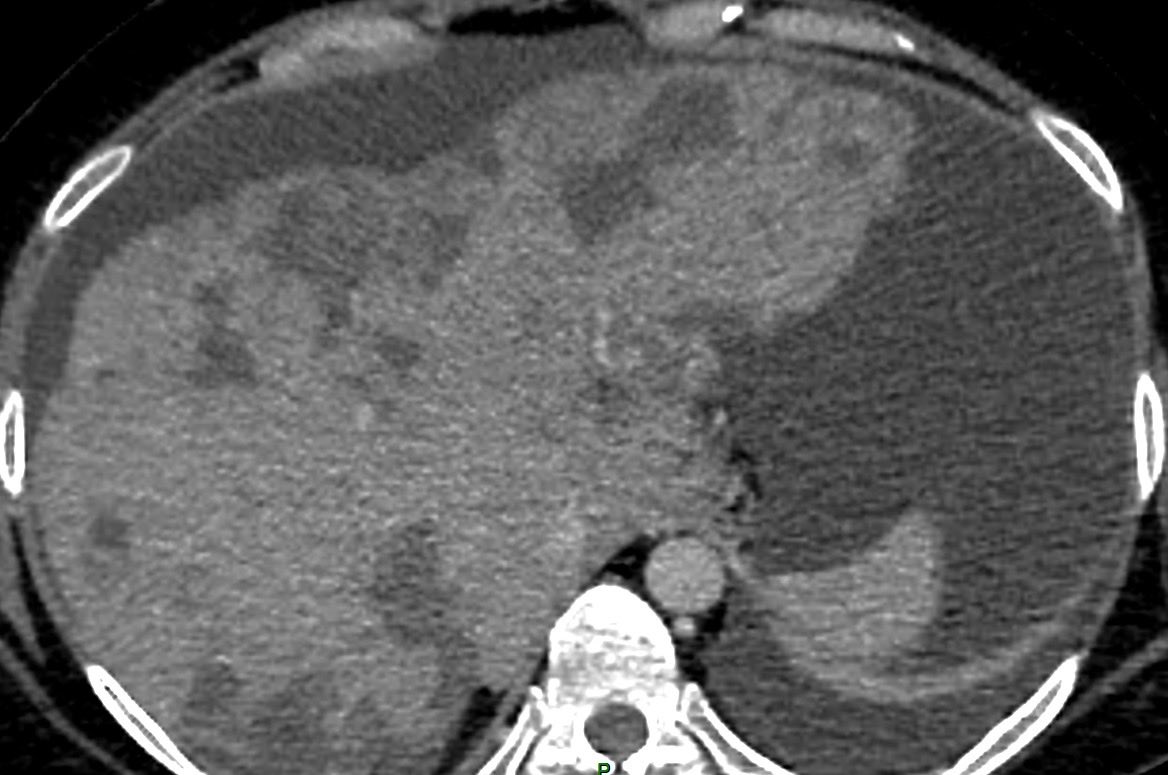
Yesterday a colleague shared this fascinating case 🫀
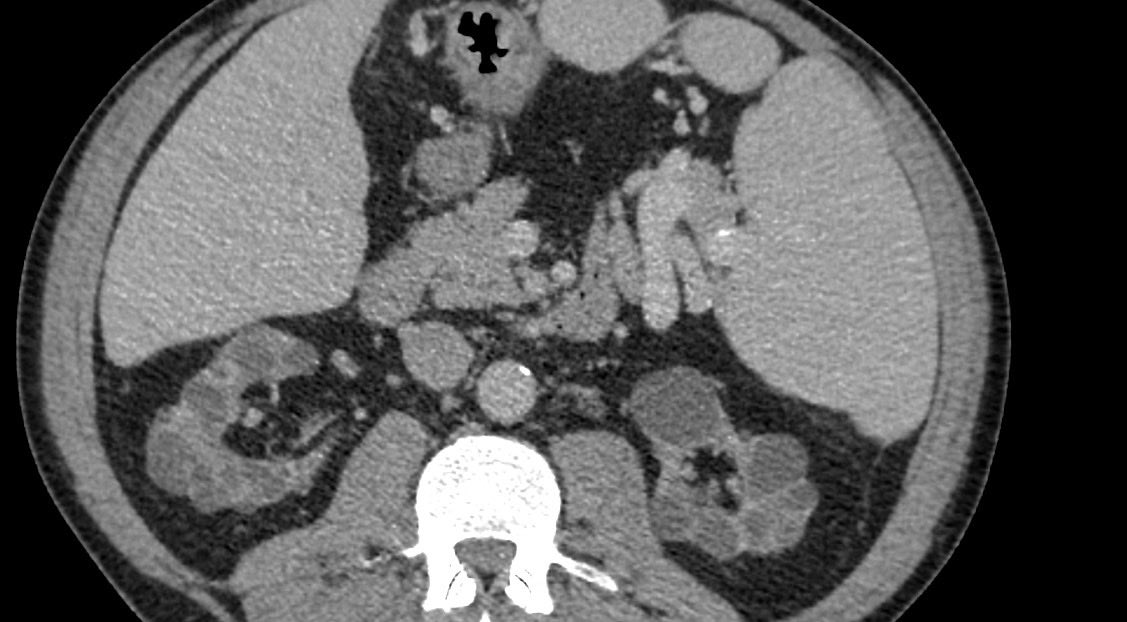
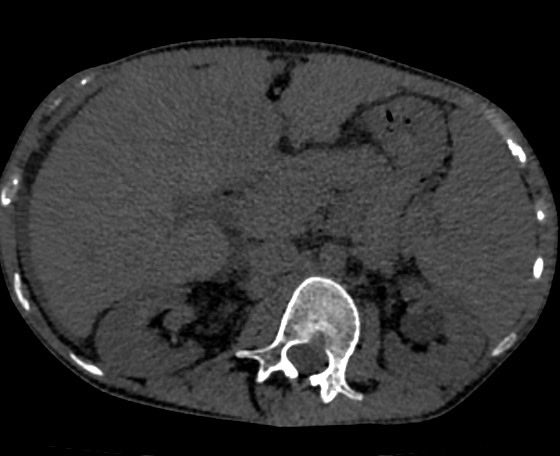
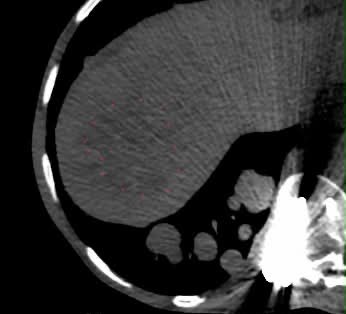
20F with history of Fontan surgery (TGA) Chest CT showing diffuse bilateral solid nodules.
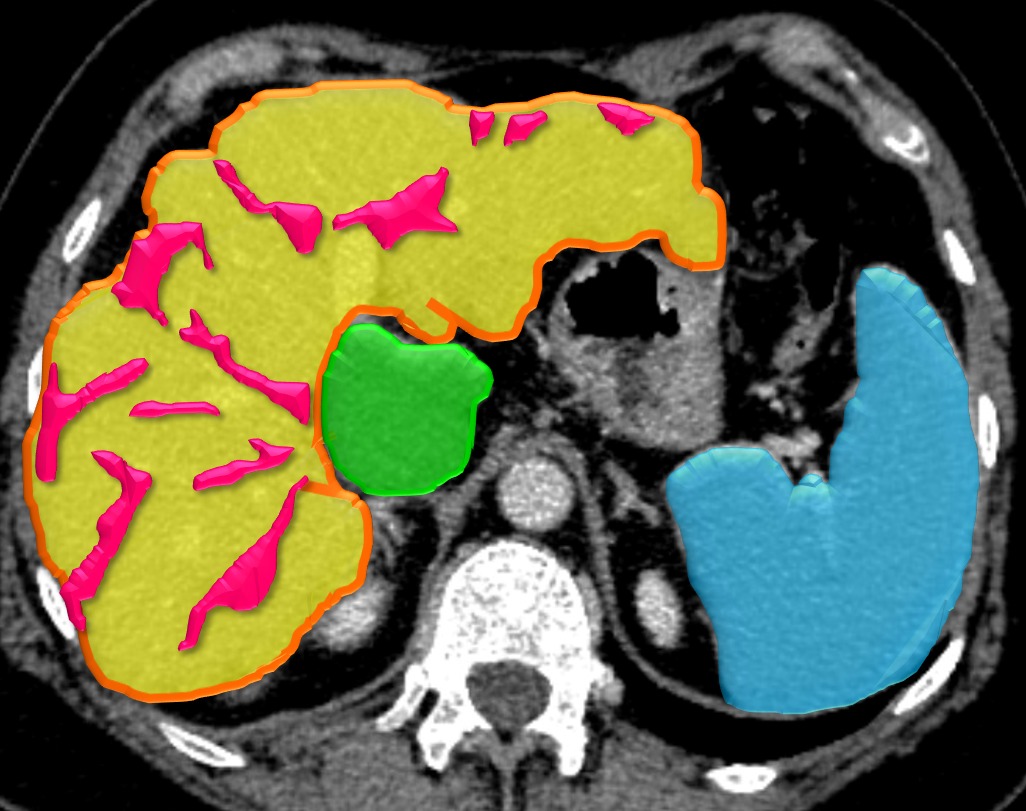
Now take a look at the CT slices of the abdomen 🚨 Heterogeneous liver appearance suspicious focal hepatic lesion
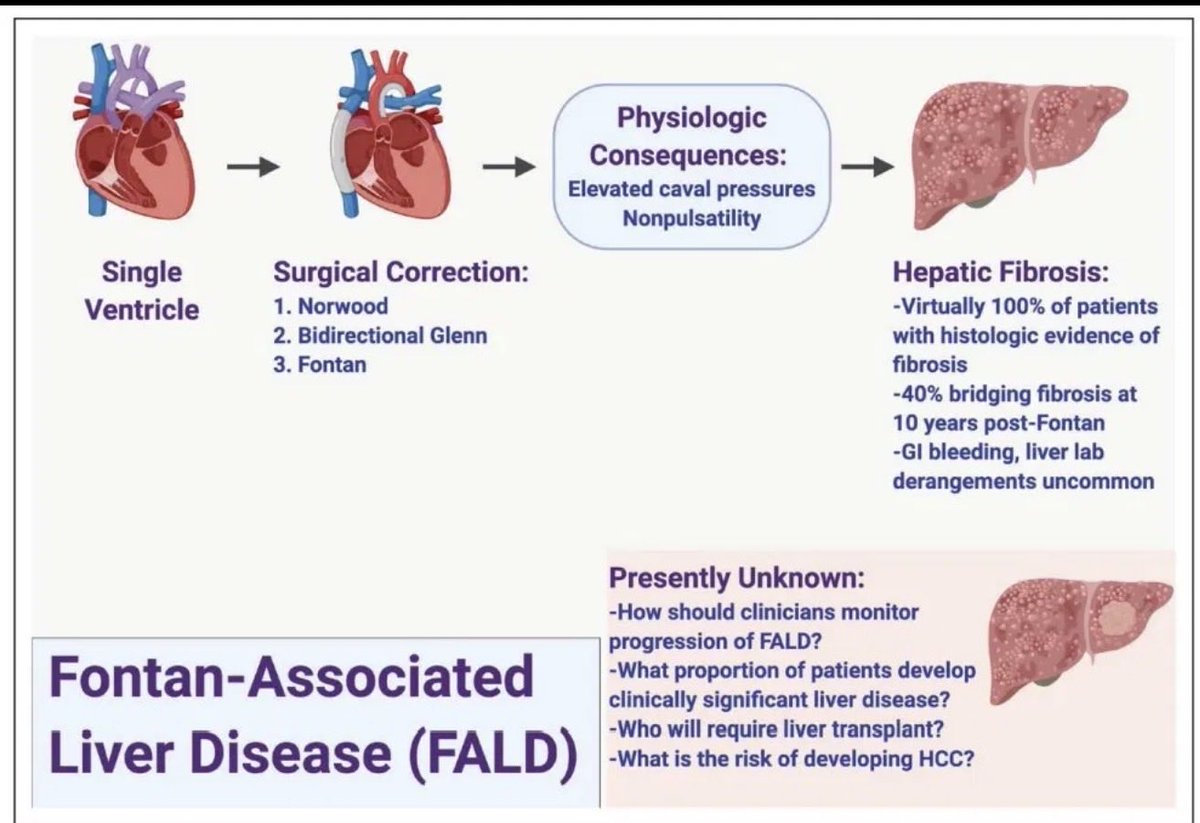
We’re probably looking at FALD-associated HCC with pulmonary metastases!
A reminder that Fontan patients need long-term hepatic surveillance 👁️
#Radiology #FOAMed #RadTwitter #RadRes
4
14
64
4,724
May 16
In addition, the other day I came across a compelling case from the folks @AbdominalCase : HALT-D (Heart-After-Liver Transplasnt with Domino).
Mindblowing surgical choreography 🤯😅
Thanks for sharing such educational and interesting cases for all! @YashantAswani
youtube.com/watch?v=2lwMxuGP…
1
5
766
Mar 28
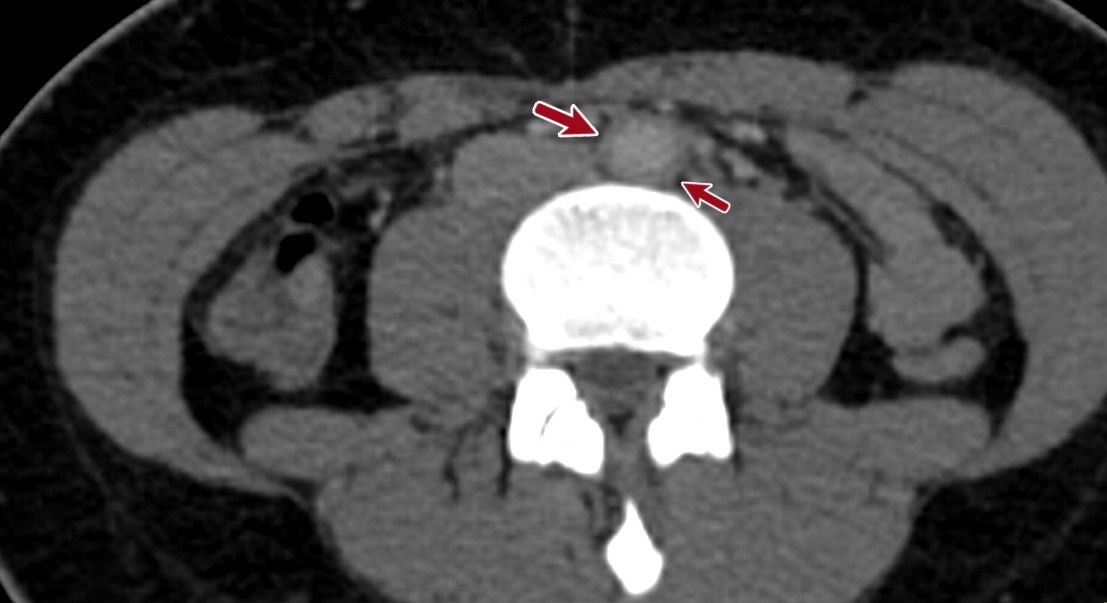
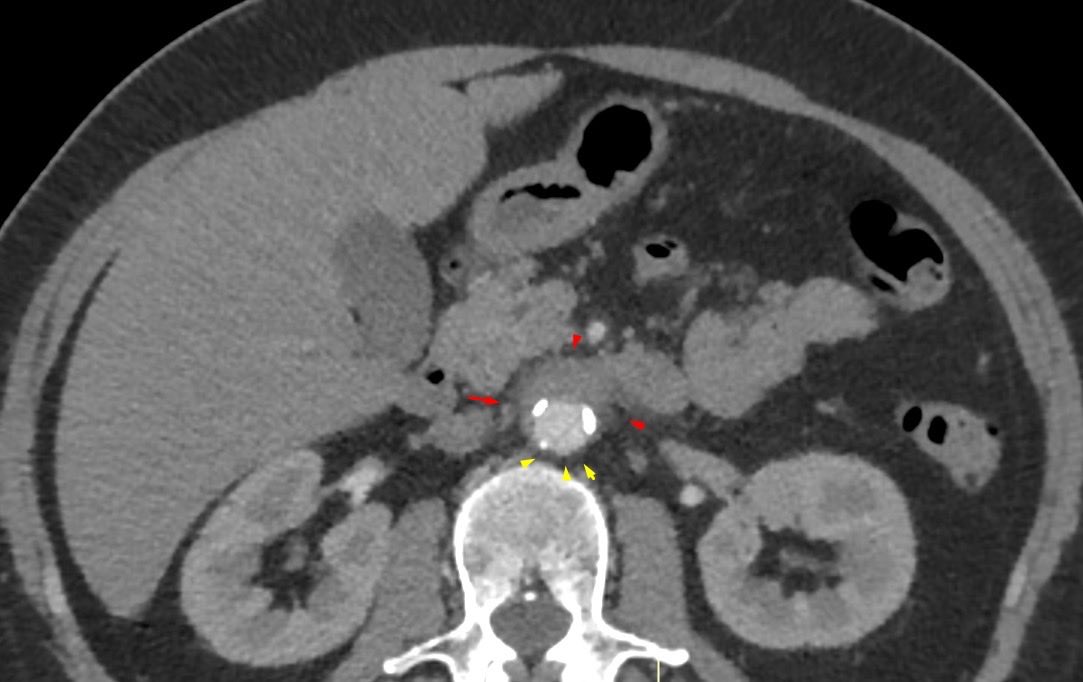
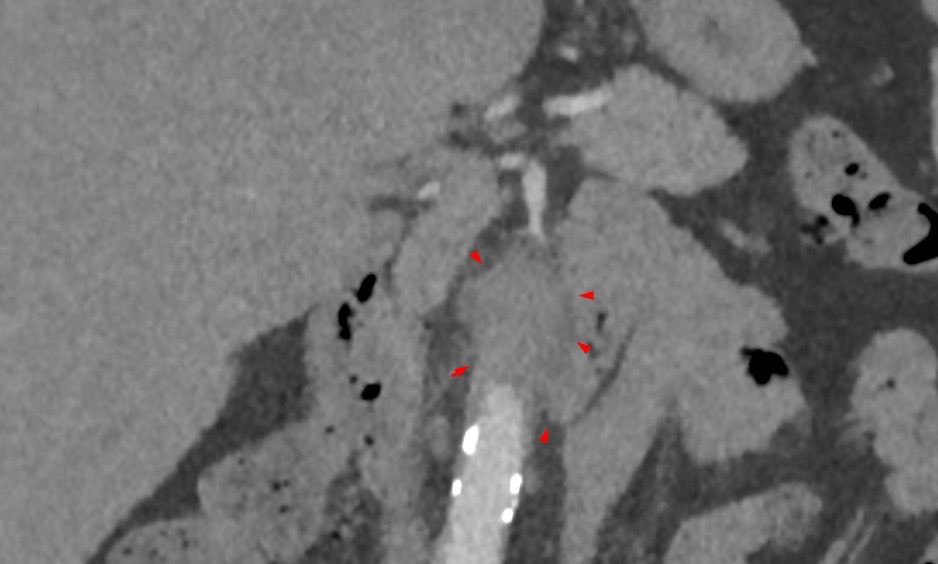
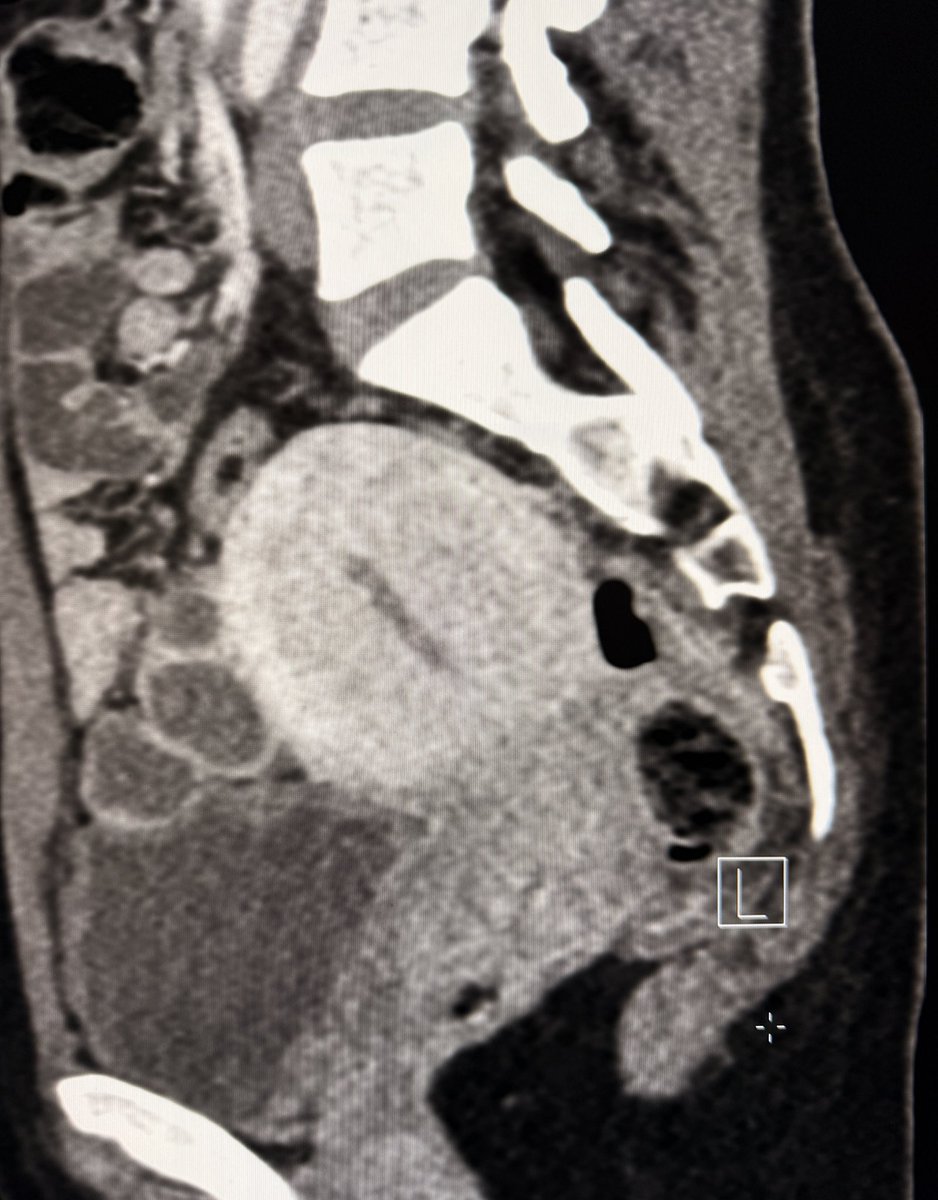
50F with abdominal pain. What’s surrounding the aorta? 👀
(Periaortic soft tissue thickening, non-circumferential, with posterior sparing and no aortic dilatation)
👉 Inflammatory periaortitis? IgG4-related disease high on the list.
IgG4 pending… 🥶
#Radiology #FOAMed #RadTwitter
2
1
21
1,514
May 11
Another case to add! 📚
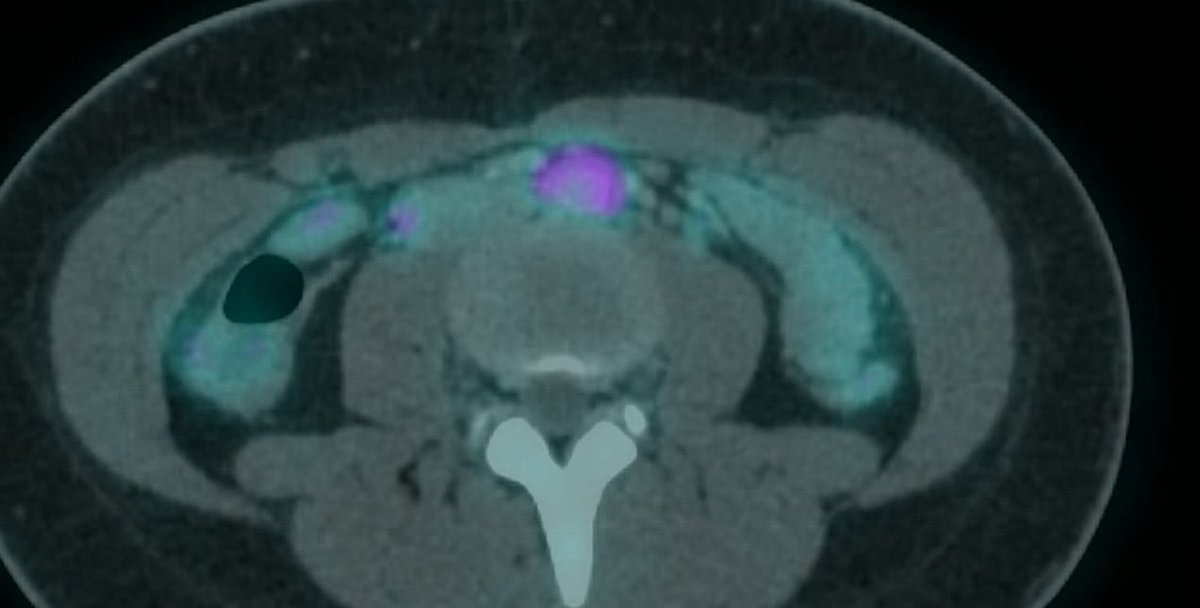
16F with Myasthenia Gravis — whole-body 18F-FDG PET/CT showing periaortic soft tissue thickening with increased metabolic activity surrounding the abdominal aorta.
No aortic dilatation. Posterior sparing. Same pattern 👀 👀
Extra findings: FDG-avid lymphadenopathies.
IgG4 also pending on this one 😅
I wonder if there's any association between aortitis and MG 🤔
#Radres #FOAMed #PETCT #vascular
1
118
Apr 28
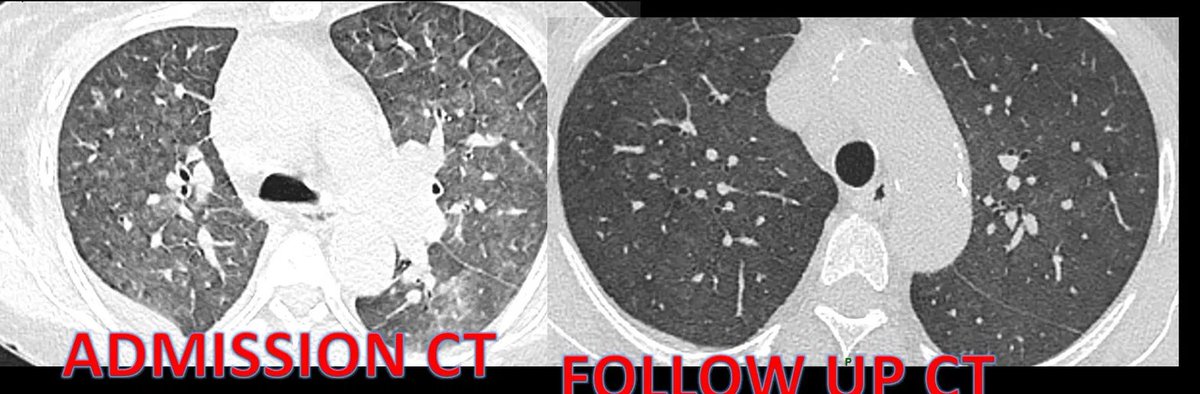
No conflict of interest — just a radiologist amazed by science!
BRAF MEK inhibition in metastatic melanoma.
Only 3 months between these CTs. The difference speaks for itself. 🎯
#Radres #Oncology #TargetedTherapy #Melanoma #Radiology
1
27
1,491
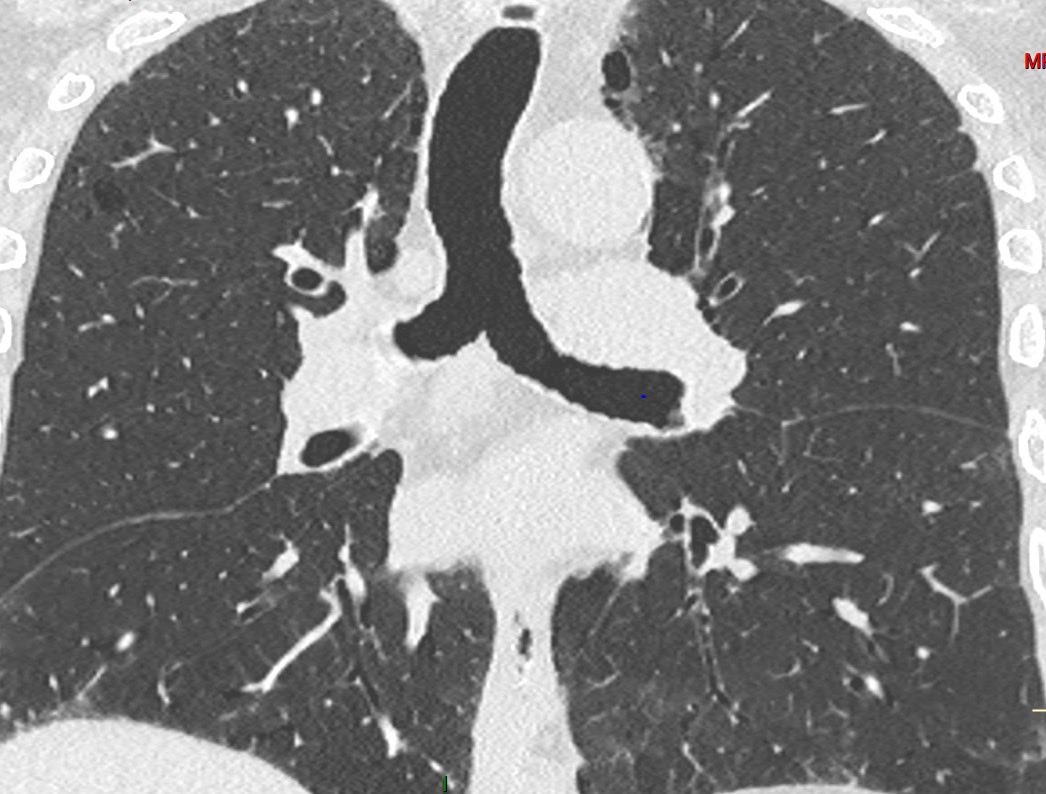
Apr 16
Digging into 2024 radiology gold ⛏️✨
These key points on SRIF are worth revisiting.
Applying them to this 78-year-old smoker:
– Mild emphysema
– Cysts within reticulation & large irregular cysts
– No subpleural predominance
– No honeycombing or traction bronchiectasis
Pattern favors SRIF ✅
30 Jun 2024

To answer the question in this post, HRCT readers should be aware of two things.
First, they need to understand the features of smoking-related interstitial fibrosis (SRIF). SRIF manifests in three main appearances:
1.Involvement of existing centrilobular and paraseptal emphysema by developing dense, definable walls and causing irregular, heterogeneous shapes and sizes, thereby disfiguring their usual appearance.
2.Cysts within reticulation.
3.Large irregular cysts.
It’s important to note that the second and third appearances do not abut the pleura. SRIF typically occurs without other fibrotic features such as traction bronchiectasis, bronchiolectasis, irregular reticulation, or honeycombing.
The second question to address is whether SRIF contributes to combined pulmonary fibrosis and emphysema (CPFE). The answer depends on the presence of fibrotic features such as traction bronchiectasis, bronchiolectasis, irregular reticulation, or honeycombing. If these features are present, SRIF is not the contributor to CPFE.
Based on these guidelines, you can determine which of the four cases are CPFE due to SRIF.
1
4
33
3,995
Sofia Gambetta retweeted

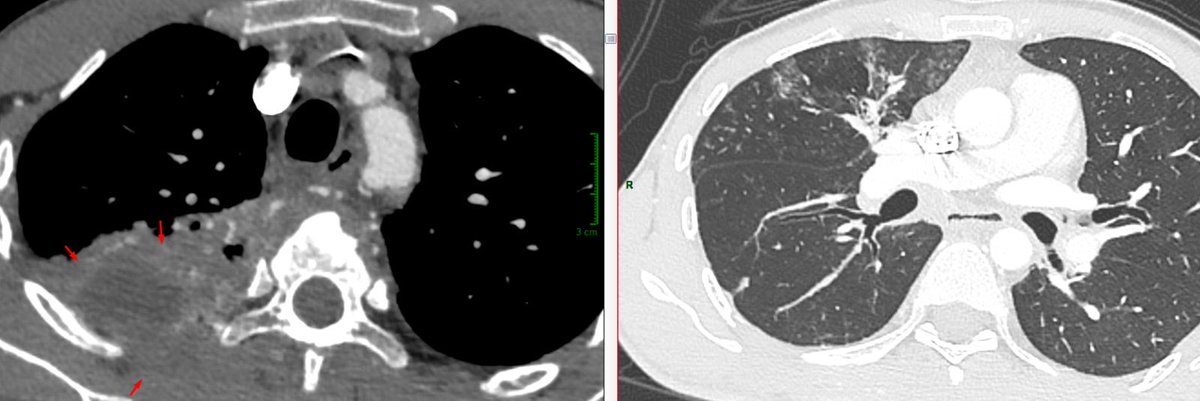
🫁 When heart failure mimics interstitial lung disease
A patient with congestive heart failure showed an indeterminate reticular lung pattern on chest CT.
Was this interstitial lung disease… or something else? 👇
#Radiology #ChestRadiology #MedTwitter
9
18
112
7,525
Sofia Gambetta retweeted

Mar 12
On portal venous phase CT, the uterus enhances more than the cervix. This differential enhancement is common and physiological. Yet it is often mistaken for cervical pathology.
The relatively lower attenuation of the cervix is often overcalled a cervicitis or a cervical mass.
Understanding normal enhancement patterns helps avoid these errors and keeps us from creating pathology where none exists.
—Pearls, Pitfalls, and Wisdom from my reporting list

5
26
176
8,793
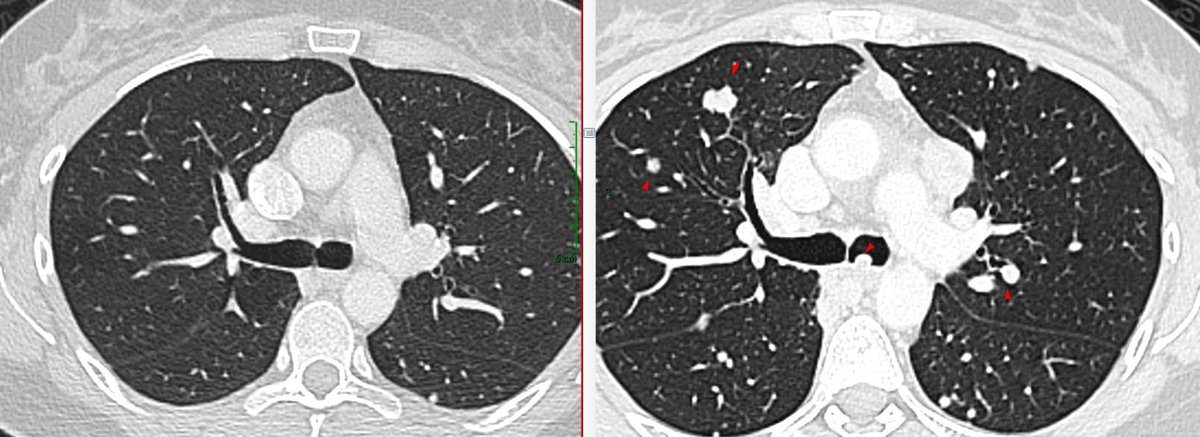
Feb 28
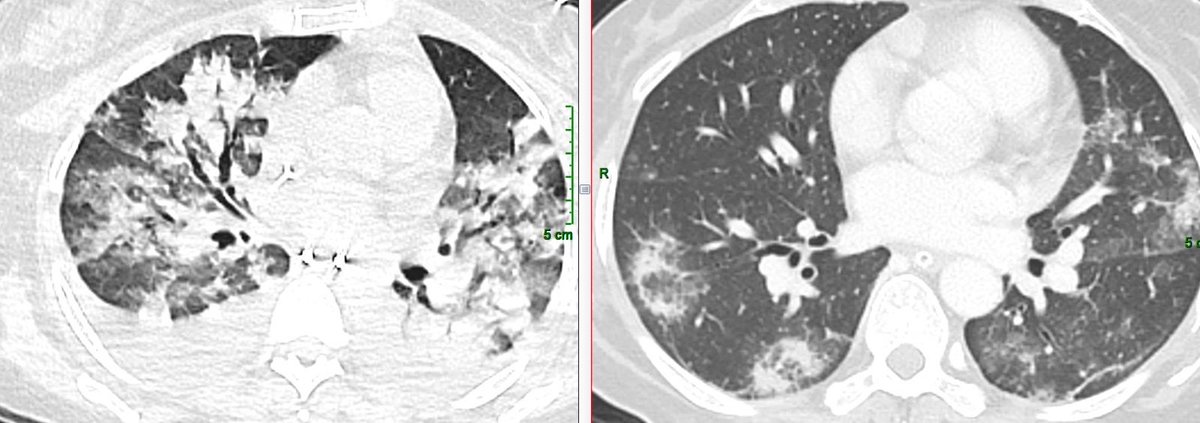
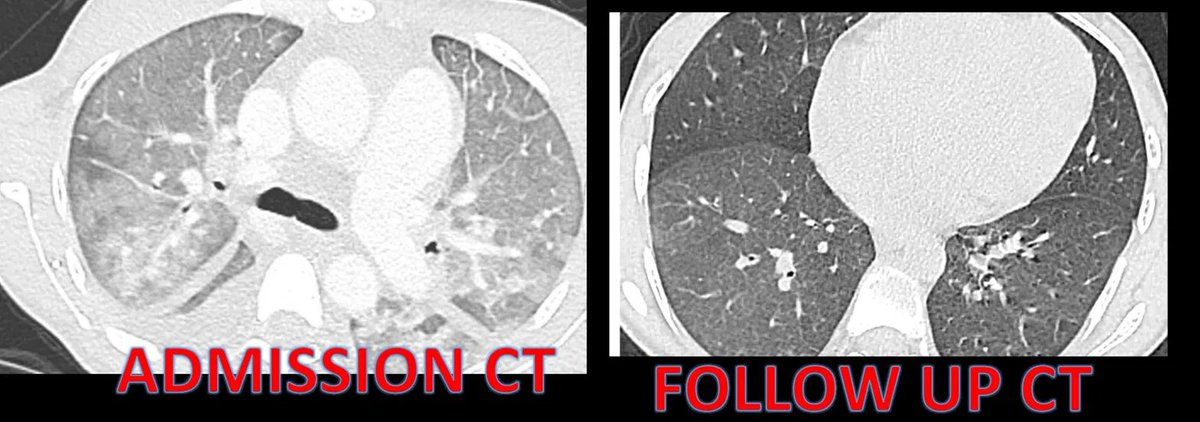
Saturday on call case 🩻 🏥
Young woman with AML
Only 1 month interval CT
From diffuse alveolar damage ➝ organizing pneumonia; A classic radiologic pattern ⬇️⬇️
#radcase #FOAMed #organizingpneumonia #radres
1
2
25
1,097
Sofia Gambetta retweeted

When anatomy tells the story. 🧬 A massive retroperitoneal mystery traced back to an undescended testis, with hyperrealistic CT revealing vascular supply, a scrotal connection, and surgical road‑mapping in 3D. Imaging guides the save. 🩻#ImagesInRadiology
pubs.rsna.org/doi/10.1148/ra…
2
9
1,255
Feb 25
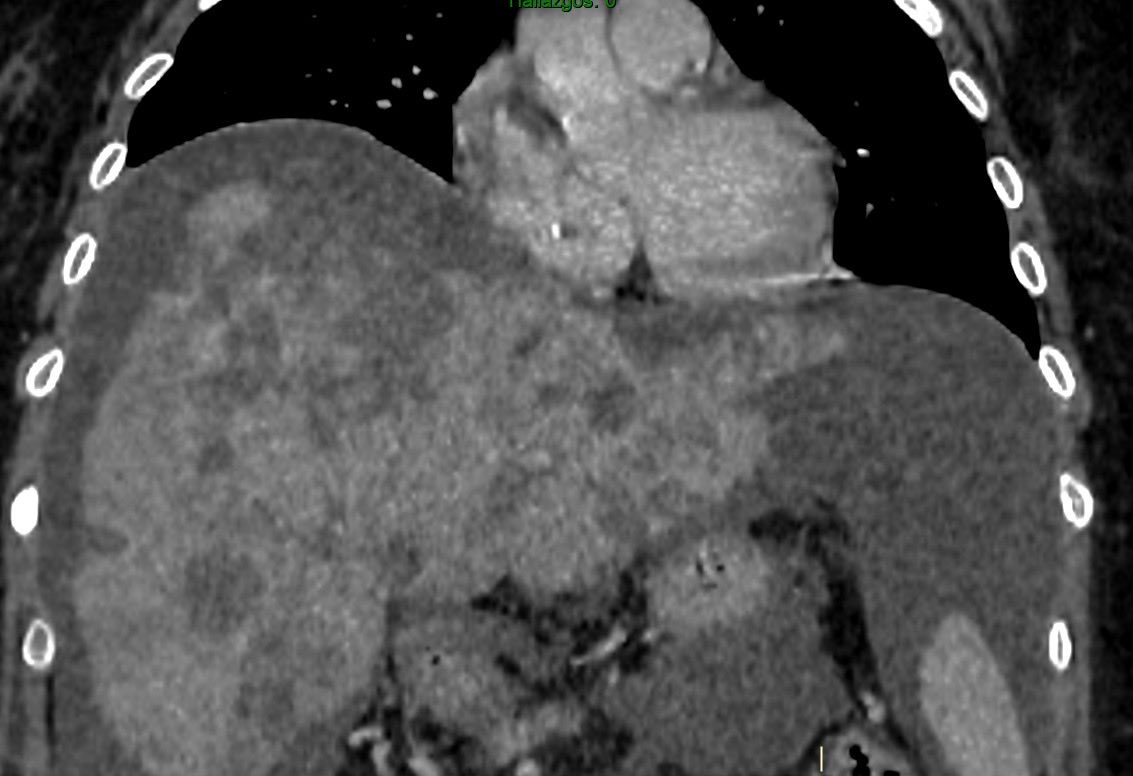
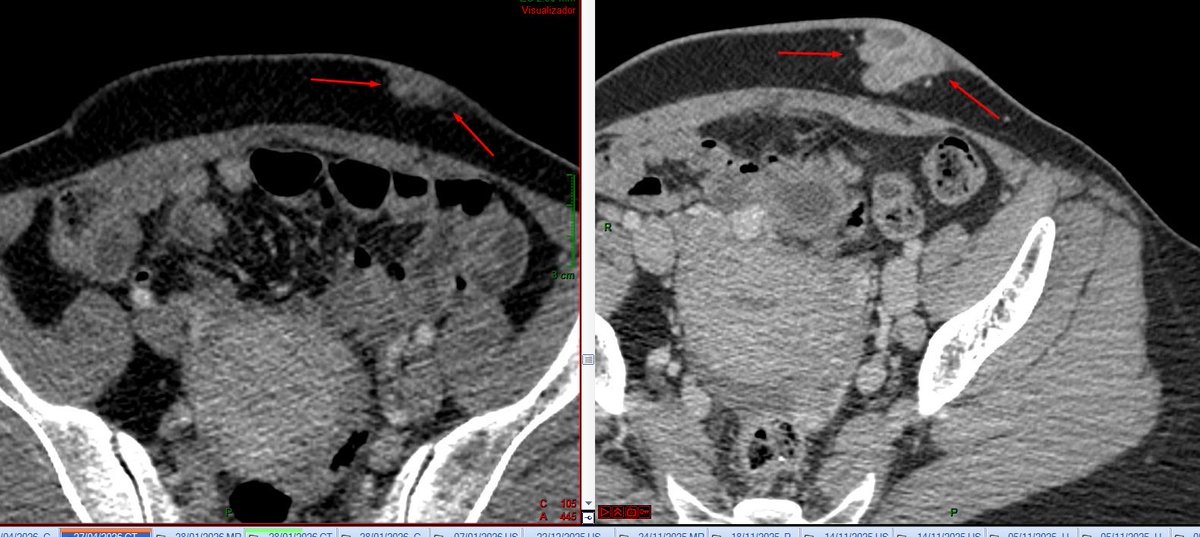
36-year-old female with advanced breast cancer.
CT findings:
🔸 Liver volume loss
🔸 Nodular contour
🔸 Ascites
In patients with hepatic metastases (especially post-chemotherapy), this pattern- Pseudocirrhosis 🚨
Recognizing it changes management.
#RadTwitter #OncoImaging
14 May 2023

Pseudocirrhosis!
Findings of liver cirrhosis, but in the setting of hepatic mets. Most common after chemo treatment of breast cancer
🟡Volume loss
🟢Caudate lobe enlargement
🟠Nodular contour
🟣Confluent fibrosis
🔵Splenomegaly
#radiology #radtwitter #MedTwitter #FOAMrad

7
565
Sofia Gambetta retweeted

Feb 17
5 exámenes que podrían salvar vidas: colonoscopia desde 45 años; APE desde 50, o desde 40 si hay antecedentes familiares de cáncer de próstata; TAC de tórax de baja dosis si fumó por años; autoexamen testicular mensual; vacuna VPH. Vea el video. @USC_Urology
3
166
512
79,783
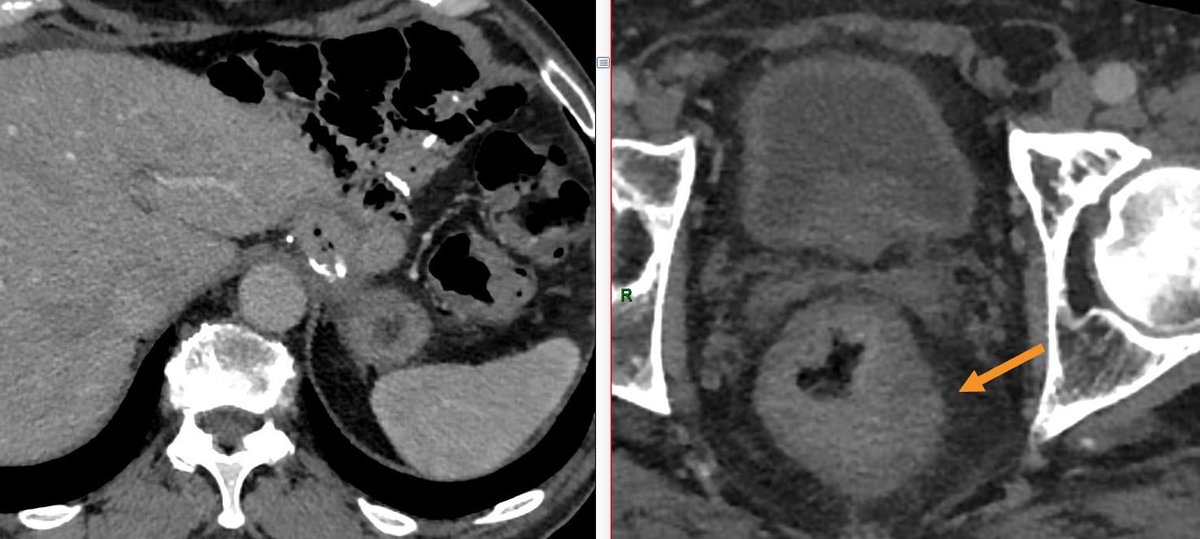
70-y/o male with prior gastric signet-ring cell carcinoma. No distant metastases on CT; EXCEPT focal distal rectal wall thickening.
I suggested rectal biopsy and pelvic MRI for further evaluation.
Pathologists, I want your thoughts, could this represent secondary involvement from signet-ring gastric carcinoma dissemination?
#RadPath #radres #GIpath
1
1
4
408
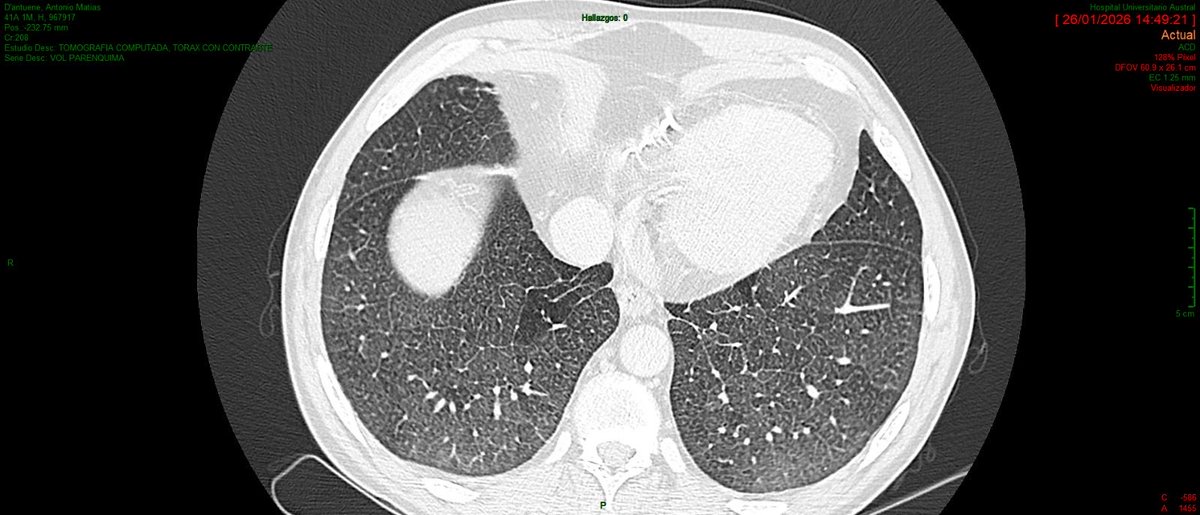
Jan 27
🫁 Challenging chest CT pattern
41-year-old male. Chronic kidney disease secondary to polycystic kidney disease
CT findings:
▫️ Innumerable miliary nodules
▫️ Bronchial interlobular septal thickening
▫️ Isolated mediastinal lymphadenopathy
▫️ No pulmonary edema
📌 With no additional clinical information, applying a pattern-based approach, the main differentials are:
1️⃣ Miliary tuberculosis
2️⃣ Hypersensitivity pneumonitis
3️⃣ Sarcoidosis
#RadTwitter #RadRes #ChestImaging #MedEd
1
8
1,641
Jan 28
After reviewing the case and literature, the most likely diagnosis was pulmonary edema secondary to CKD/CHF, with pulmonary hemosiderosis due to venous congestion.
Interestingly, this appears to be the first description of a nodular CT pattern of hemosiderosis related to congestion
1
3
130
Jan 29
84