Founder, MIT Sloan, coach, fmr Chief Med Officer & Medicaid med dir, Top Voice 4x, data nerd, digital health, MedEd, humanist, Tweets personal, RT🚫endorsement
- Tweets 113,607
- Following 7,574
- Followers 6,874
- Likes 202,403






















ALT Twenty years ago, longevity medicine didn't have a name. No standards, no curricula, no consensus on evidence. Today, ARPA-H has committed $144M through its PROSPR program for therapeutics targeting aging biology directly. XPRIZE Healthspan is mobilizing global talent. Governments from the U.S. to Saudi Arabia are funding aging research at unprecedented scale. The people building this field are gathering in Cambridge on May 26 and 27 for the Aging Code Summit, part of the inaugural Boston Tech Week. I'm speaking on Day 2 on evidence-based best practices in longevity medicine. The question I keep returning to: which interventions actually deliver outcomes, and how do we tell. Also on the agenda: Manolis Kellis on the computational biology of aging, Li-Huei Tsai on neurodegeneration, Kristen Fortney on translation, plus a pitch competition for a one-year residency at MIT's The Engine. If you work where this field is being built, you should be in the room. More at linkedin.com/in/agingdoc















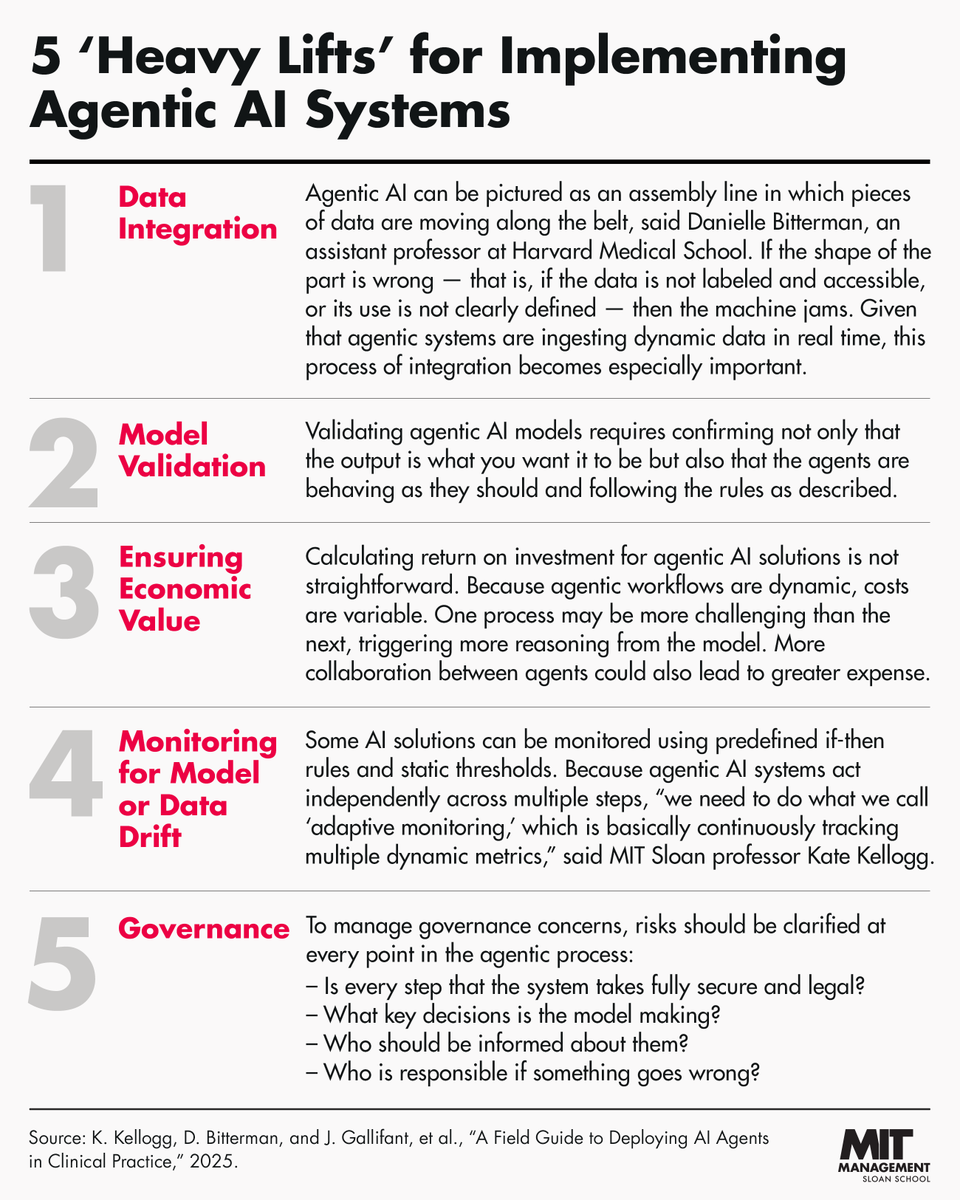
ALT Graphic titled '5 "Heavy Lifts" for Implementing Agentic AI Systems'. The five "lifts" are: 1. Data integration. 2. Model validation. 3. Ensuring economic value. 4. Monitoring for model or data drift. 5. Governance. Each category has a brief description.