
Stanford MD. Longevity medicine without miracle language: labs, meds, supplements, risk, and what the science actually proves. Founder @goCareCore.
Joined July 2009
- Tweets 812
- Following 802
- Followers 1,248
- Likes 421
310 Photos and videos














Pinned Tweet

Apr 22
The most promising longevity drug isn't a peptide or metformin. It's the Shingles vaccine.
New data shows it slows biological aging and lowers systemic inflammation for 4 years post-shot. We are seeing a 20% reduction in new dementia diagnoses and a 25% lower risk of stroke.
Stop waiting for a magic pill. One is already on the shelf.

221
913
4,116
305,404
Frontier LLMs are now beating specialized clinical AI tools like OpenEvidence and UpToDate Expert AI on medical benchmarks.
Not shocking, but it matters.
The study compared OE UpToDate Expert AI against GPT-5.2, Gemini 3.1 Pro, and Claude Opus 4.6, models that already feel “old” by frontier lab standards.
That’s the problem for clinical AI wrappers:
If your main promise is “better answers to medical questions,” you are competing with the fastest model labs in the world at exactly what they do best.
The defensible wedge probably isn’t answer quality alone.
It’s workflow:
- privacy / BAA posture
- source UX
- CME
- auditability
- institutional trust
- EHR/context integration
- habit
But even that moat is narrowing. ChatGPT for Clinicians now offers privacy protections and CME support too.
So I’m curious:
Clinicians: are you still using OpenEvidence / UpToDate AI as your default?
Or are you skipping straight to frontier LLMs and bringing your own clinical judgment?
85
Jun 8
"It's just lifestyle." "Just eat clean and exercise."
I keep seeing messaging like this in longevity.
But this misses the more important point:
Most people don’t fail health habits because they’re weak.
They fail because the path of least resistance was crafted through nefarious design.
When social media and the news brings your fear and anxiety,
Or when you're overwhelmed with demands from your boss, kids, spouse, parents,
Obviously it'll be hard to stay on track through the day. Individual responsibility is just one tiny piece of the puzzle.
It's our general responsibility as innovators, leaders, and operators to design a better ecosystem.
The fix is not more self-shaming.
It is making the useful choice slightly easier than the default tired choice.
And that isn't all on the individual.
1
2
212
Jun 4
Bolting AI onto broken workflows produces faster broken workflows.
The question is not whether AI changes medicine. It already is.
The question is whether we use it to automate broken medicine, or rebuild care around what patients actually need.
medstorystudio.com/the-machi…
1
1
1
120
Jun 4
Also quoted in the MedStory piece: @ShikhaJainMD and @THEanxietyMD.
The whole thing is a useful snapshot of where physicians are excited — and worried — about AI in care.
70
Jun 2
Speaking today at NY Tech Week: Sick care is dead. What comes next?
Consumer health is already the new front door: AI, labs, GLP-1s, wearables, telehealth longevity clinics.
The question is how we make it clinically useful, not just noisier.
RSVP: partiful.com/e/FY3KclQ7SZQRA…
3
161
Jun 1
“Non-toxic” is not a material.
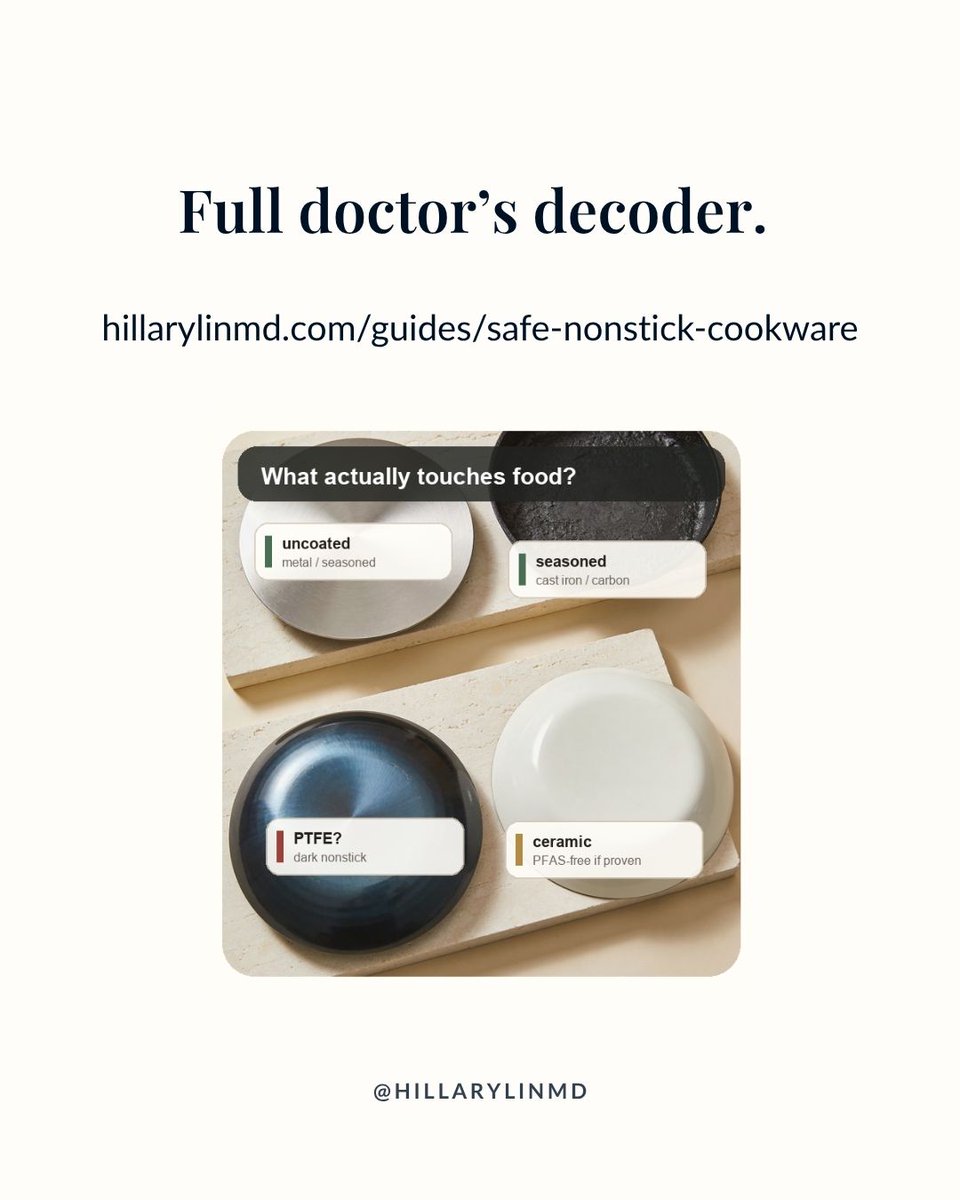
If you’re buying nonstick, the better question is: what surface is touching your food?

1
90
Jun 1
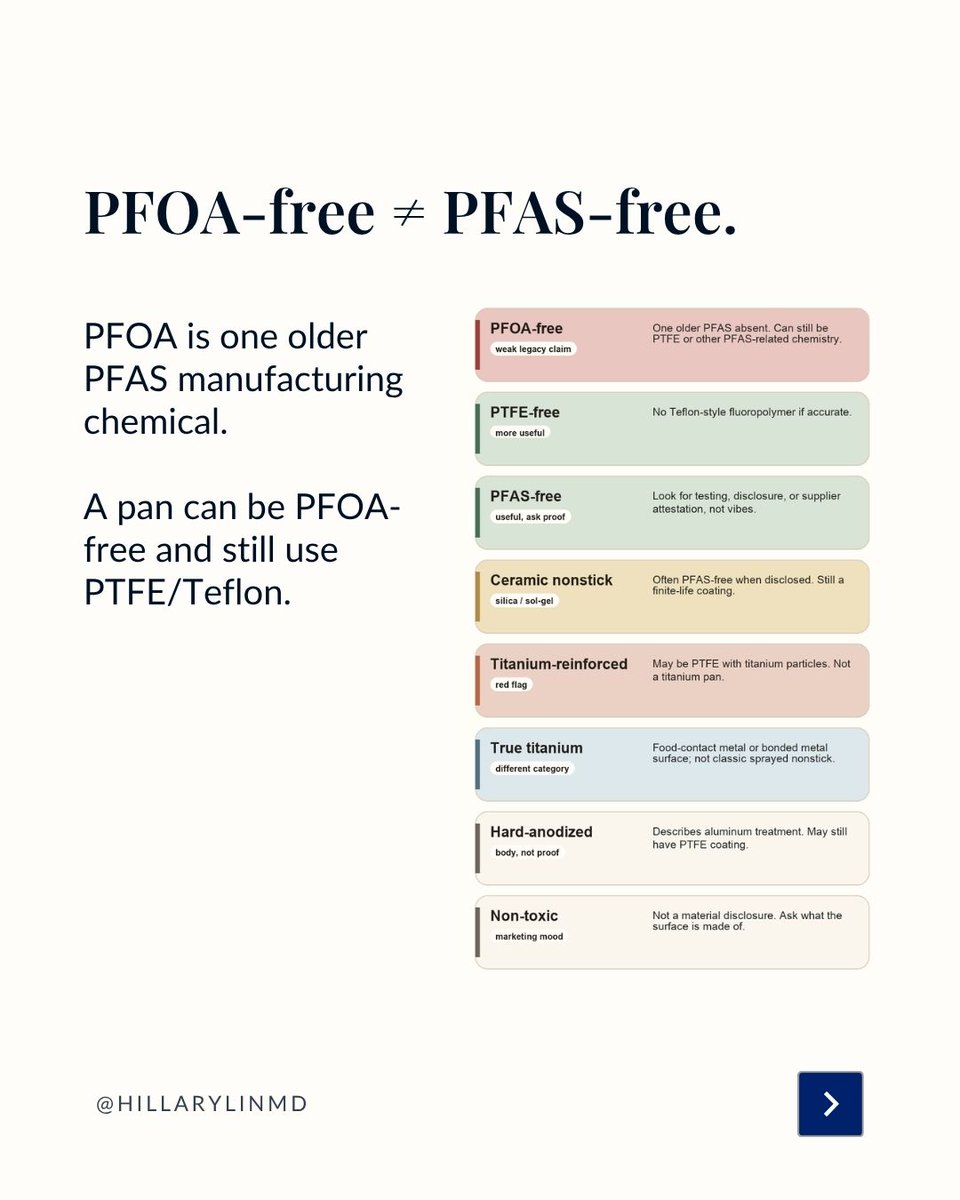
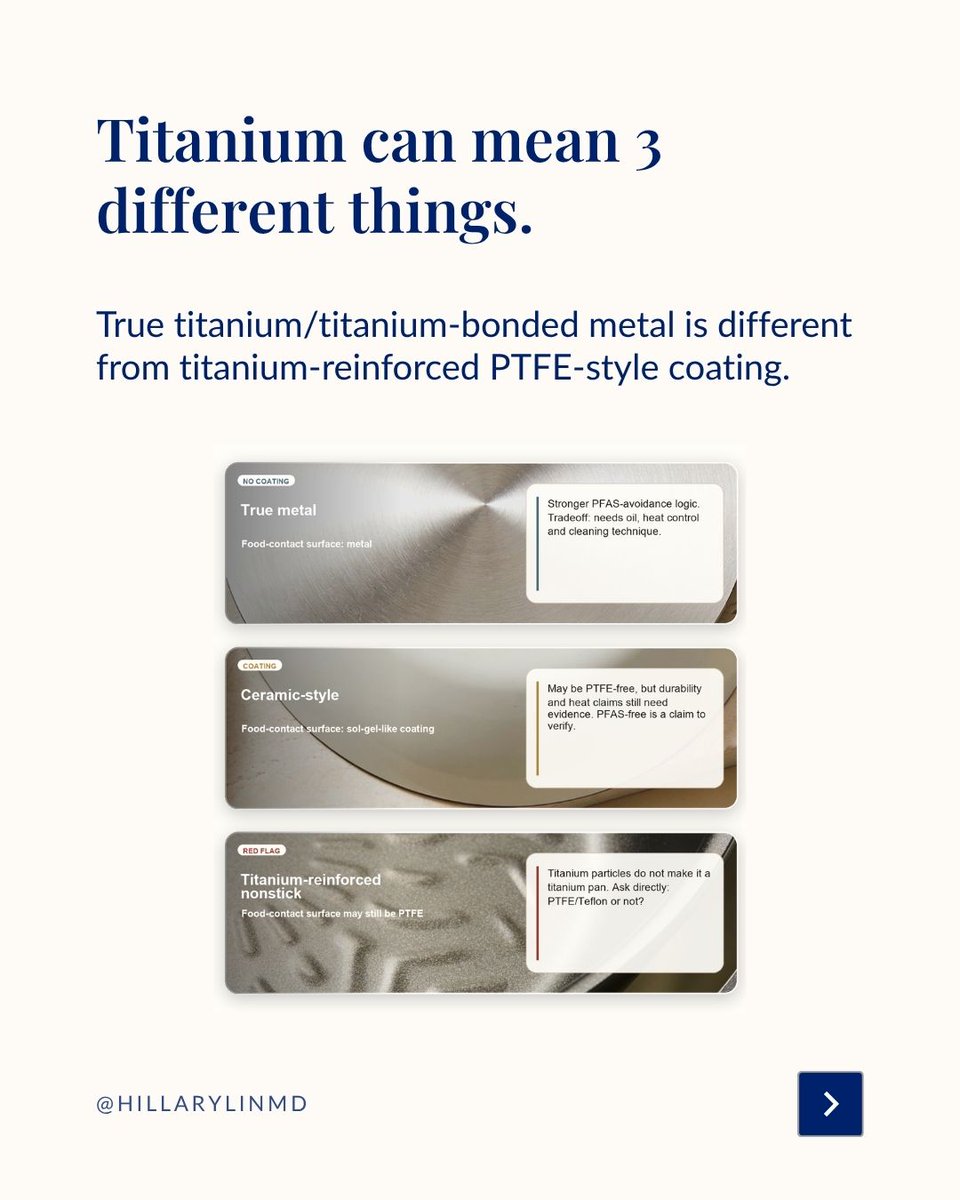
PFOA-free ≠ PFAS-free.
PTFE-free is a stronger clue.
Ceramic can be useful but finite-life.
“Titanium” can mean very different things depending on the actual coating/surface.

1
123

May 29
1/4 Speaking at NYC AI x Longevity Summit during NYC Tech Week on Jun 4–5.
I’m on the AI in Clinical Practice panel Thu 3:30–4:30p ET w/ @mishalreja, @NeilpDo Jim Donnelly, hosted by @LongevityGL.
2
2
6
537
May 29
3/4 Speakers I’m excited to hear from: @NirBarzilaiMD @M_S_Ringel @rv_sehgal @DrGlorioso @DanielSodickson @MiriamMerad @ISBLeeHood @JamesPeyer @celinehalioua @lucascamillomd
1
3
132
May 29
4/4 Also: @Danbelsky @VarunDw @tomzuber @mayafromtunisia @JFutoma teams from @lifebiosciences @AFARorg @BioLabsNY.
Agenda/register: longevitygl.org/ai-x-longevi…
2
48
May 29
Longevity doctor to her Hermes agent - "Track this very weird breakfast" 😆
78
May 28
Longevity medicine has a major bottleneck.
And it's not even the science.
It's care delivery.
Because most health decisions don’t happen in a doctor’s office.
Spent the last two days at the Aging Code Summit in Cambridge with scientists, founders, investors, and clinicians working across biomarkers, therapeutics, AI, neurodegeneration, inflammation, regenerative medicine, and clinical trials.
The discovery engine is real.
But as a practicing longevity clinician, I kept thinking about the layer after discovery:
How does any of this actually reach people?
Not just the patient with time, money, and medical literacy.
Not just the person who can find the right concierge doctor.
And not just once a year, during a visit.
People make health decisions every day: in grocery stores, gyms, group chats, supplement aisles, lab portals, algorithm feeds, and anxious 11pm searches.
Most of those moments do not involve a physician.
So if the future of longevity is “clone more doctors,” we’re going to fail.
There will never be enough of us. And that’s not how people live.
The real opportunity is to build better surfaces for healthcare:
- tools that translate evidence into action
- systems that support follow-through
- guardrails against overtesting, overtreatment, and false certainty
- care models that meet patients where they already are
That’s the part I care most about building.
Longevity needs great science.
It also needs delivery models that make the science usable. @gocarecore
Thanks so much to @LongevityGL for another amazing meeting, and fellow speakers, organizers, and attendees: @Mindvyne @3cubedAi @DrGlorioso @justinqtaylor @NeuroAgeTX @agingdoc1 @usnehal @CoreViva @agelessrx_ @kpfortney @bioagelabs @lifebiosciences @JamieHeywood @microbeminded2 @polybioRF @mahdi_moqri @agingbiomarkers @manoliskellis @MIT_Picower @DrDorisDay @VincereBio @InSilicoMeds @hevolution_f @CellinoBio @MariZazzer
1
3
7
797
May 28
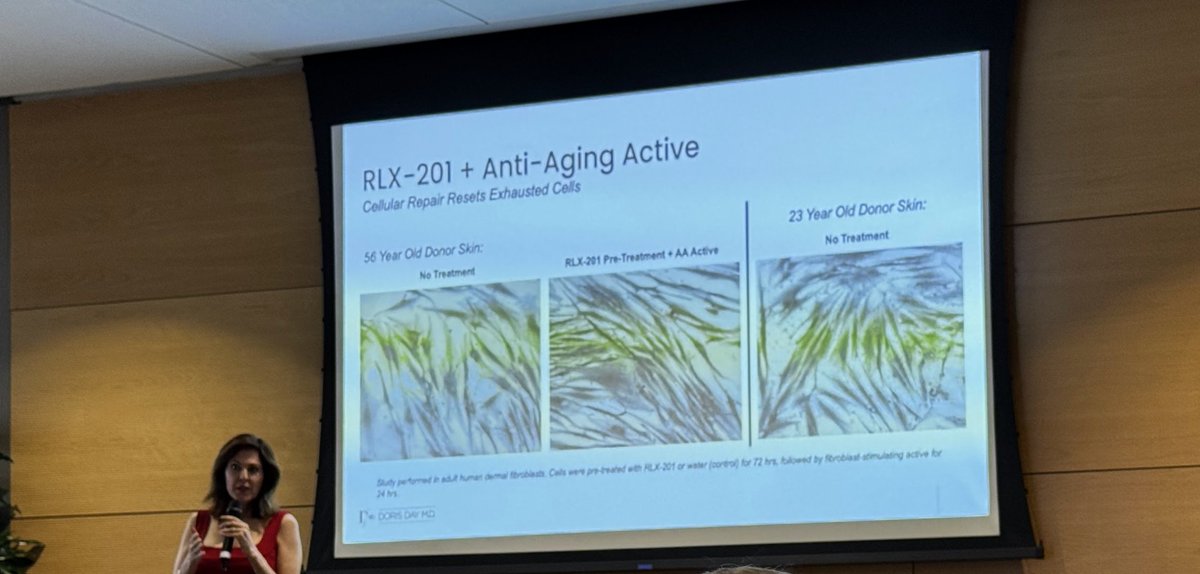
Delighted to meet the brilliant @DrDorisDay - skin is the absolute most visible aspect of longevity, for science and clinical application alike - fascinating work with blocking mTORC1!
1
148
May 28
Much fun to reunite with fellow longevity physicians and brilliant speakers @agingdoc1, Dr. Jay Luthar, @MariZazzer @LongevityGL - can't wait till our next panel together 💪
1
2
237
May 26
The longevity field has gotten better at measuring aging.
Epigenetic clocks. Proteomics. VO2 max. DEXA. CGMs. ApoB. Inflammatory markers. Microbiome readouts. A growing menu of things we can track, score, compare, and optimize.
But a biomarker is not a treatment plan.
The harder question is clinical: when should any of that data actually change care?
That’s the lens I’m bringing to Aging Code Summit this week in Cambridge. I’ll be on the Wed May 27, 9:50am panel, “Longevity in Practice: Concierge Medicine and Frontline Learnings,” with Jay Luthar, @agingdoc1, and Marianna Zaslavsky.
What I’m most interested in:
- Which biomarkers are mature enough to act on
- Which interventions change outcomes, not just dashboards
- How to give high-agency patients better tools without handing them expensive noise
- Where concierge/longevity medicine can be more accountable, not just more personalized
If you’re in Boston/Cambridge for Boston Tech Week and thinking about how aging science makes the jump into real clinical care, come say hi.
Hosted by @LongevityGlobal with @Mindvyne and @3cubedAi, during Boston Tech Week.
Details and registration:
longevitygl.org/boston
#BostonTechWeek #LongevityMedicine
1
4
682
May 24
The @enhanced_games are not just a doping story.
They’re an opportunity to test the limits of human potential in public.
Not longevity itself. But before we can bioengineer healthspan, we need to know what healthy physiology can do, tolerate, recover from, and fail at.
1/5 🧵
1
3
137
May 24
The risk is that all @enhanced_games becomes is marketing.
May 24 in Las Vegas: PED-permitted sport, a sponsor-run registered study (NCT07568574), elite athletes, longevity-world names, media distribution, and a consumer performance/longevity business behind it.
4/5
1
2
239
May 24
If we were to make the most of @enhanced_games - we would go beyond the argument of pro-PED vs. anti-doping.
It is pro-data pro-governance:
disclose protocols, measure downside, monitor long term, publish results, separate endpoints, and don’t oversell.
5/5
2
82