
Joined May 2020
- Tweets 2,408
- Following 717
- Followers 142
- Likes 1,617
156 Photos and videos




Pinned Tweet

14 Apr 2025
when the destroyer of the worlds can’t even survive one mood swing
Caption for the pic
#ghilbistudio
#ghiblistyle
#ghibli

2
2,312
#CardioComics
#Cardiotwitter
#CardioUpdate
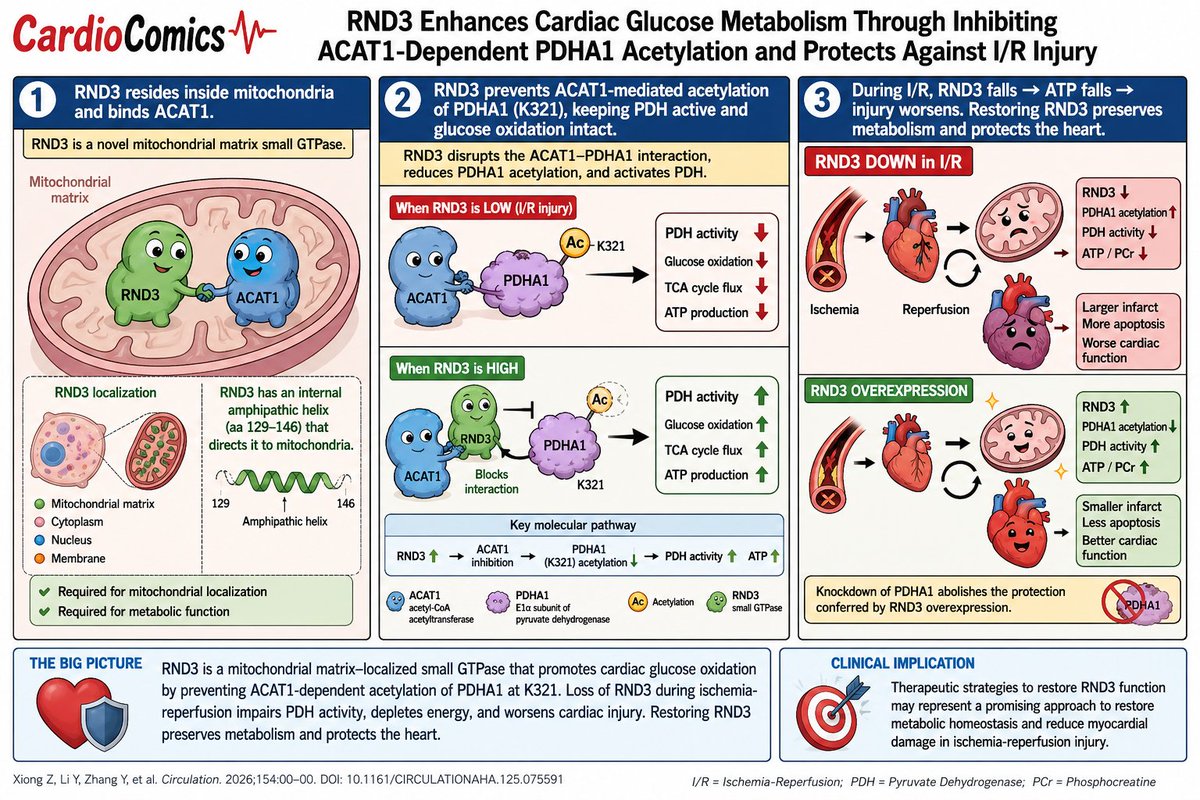
🫀 RND3 is a newly discovered mitochondrial protector of the heart.
By blocking ACAT1-dependent PDHA1 acetylation, RND3 enhances glucose oxidation, preserves ATP, and reduces ischemia-reperfusion injury..
1
12
Veeresh Hubballi retweeted

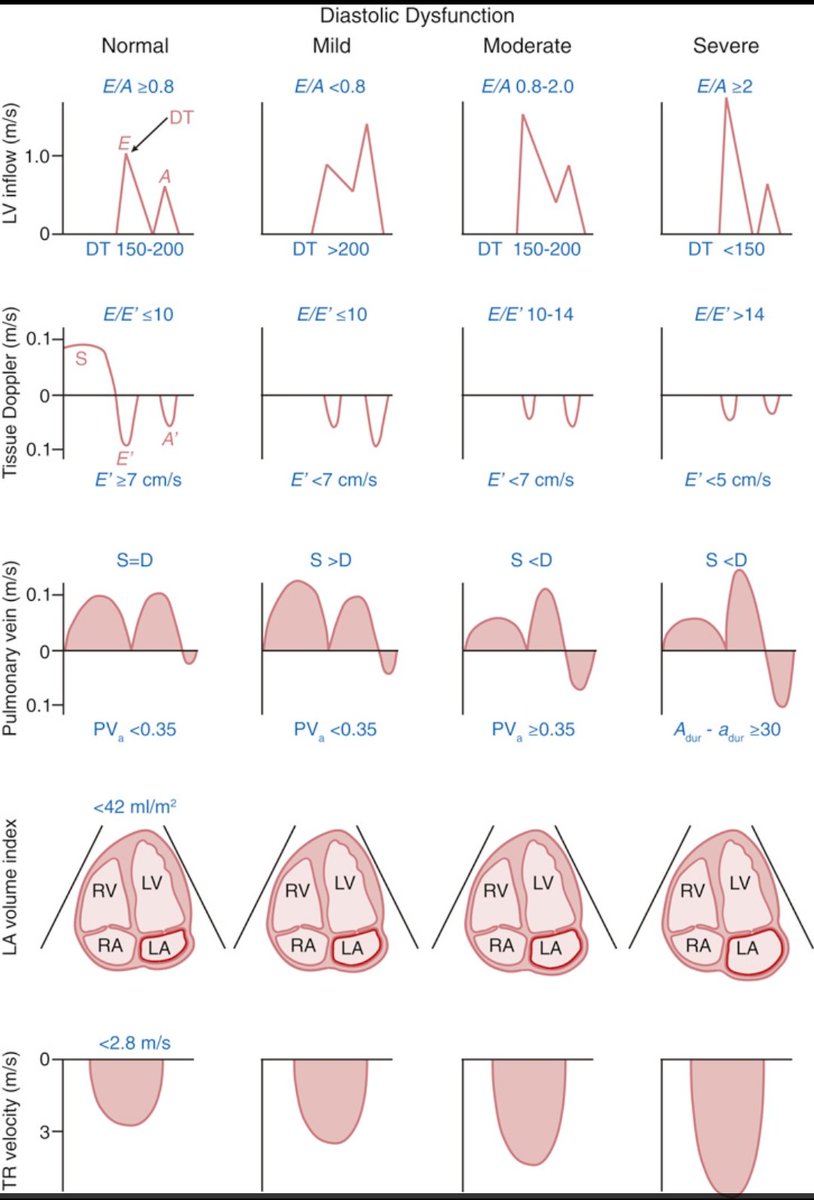
Understanding Diastolic Dysfunction with Doppler Echocardiography
This chart beautifully compares Doppler findings in normal vs. varying grades of LV diastolic dysfunction from inflow (E/A, DT) to tissue Doppler (E′/A′), pulmonary vein flow, LA volume, and TR velocity.
Source: Catherine M. Otto, Textbook of Clinical Echocardiography
1
52
155
11,541
Veeresh Hubballi retweeted

Jun 10
ADA 2026 Day 3 — CME INDIA Style Top Clinical Pearls
Source: ADA 2026 Day 3
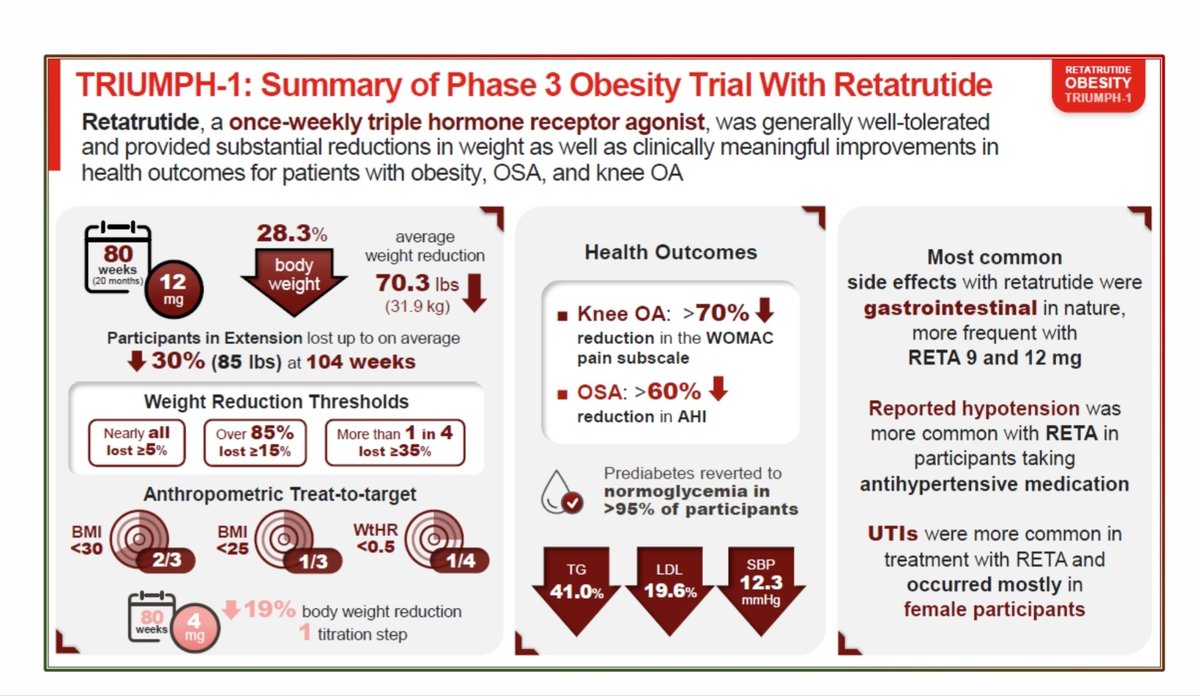
1️⃣ Retatrutide looks like the next “triple-action” metabolic molecule.
Triple agonism at GIP GLP-1 glucagon receptors produced nearly 2% HbA1c reduction in recent-onset T2D and weight loss up to 16.8% in TRANSCEND-T2D-1.
2️⃣ In obesity, retatrutide is entering bariatric-range territory.
In TRIUMPH-1, weight loss reached 28.3% at 80 weeks and up to 30% at 104 weeks; more than 85% achieved ≥15% weight loss.
3️⃣ Retatrutide is not just a glucose drug; it is a cardiometabolic-remodelling drug.
Beyond glycemia and weight, benefits were seen in obesity-related complications including OSA severity and knee osteoarthritis pain.
4️⃣ Inflammation is the hidden CV-risk amplifier in CKD T2D.
In 12,864 participants, 53% had hsCRP ≥2 mg/L, and every doubling of hsCRP increased composite CV event risk: aHR 1.11.
5️⃣ Obesity plus inflammation is a dangerous cardio-renal phenotype.
The hsCRP–CV risk signal was strongest in those with elevated BMI, reinforcing the need to phenotype T2D patients beyond HbA1c alone.
6️⃣ Finerenone benefit remains robust despite inflammation or obesity.
Finerenone’s CV benefit was consistent irrespective of baseline hsCRP or BMI — useful reassurance for CKD T2D patients with inflammatory or obese phenotype.
7️⃣ SGLT2 inhibitors may protect kidneys before classical albuminuria appears.
In T2D with preserved eGFR and UACR <30 mg/gCr, SGLT2 inhibitor use markedly slowed eGFR decline: non-users −1.33 vs users 0.06 mL/min/1.73 m²/year.
8️⃣ UACR 10–30 mg/gCr may be the “early-warning kidney window.”
Renoprotection was more evident in patients with UACR 10–30 mg/gCr, suggesting this “high-normal albuminuria” range should not be ignored.
9️⃣ Ramadan fasting with CGM appears safer and more stable.
Real-world Dexcom CGM data showed stable glycemic control before, during, and after Ramadan, with reduced level 1 hypoglycemia during Ramadan.
🔟 MDI insulin users during Ramadan need special attention.
Among insulin users, those on multiple daily injections had higher glycemic variability and rebound hyperglycemia — CGM alerts and structured dose planning are crucial.
1️⃣1️⃣ CKD screening in T2D remains embarrassingly inadequate.
Even among patients with CKD, UACR was available in only 42.1%; among those without coded CKD, UACR was available in only 26.6%.
1️⃣2️⃣ GDMT gap is the biggest preventable kidney-care failure.
Among T2D patients with CKD, use of recommended therapy classes remained below 60%, including RAS inhibitors, SGLT2 inhibitors, GLP-1 RA, and nsMRA.
1️⃣3️⃣ Prediabetes is not benign for kidneys.
In nondiabetic adults, both prediabetes and higher FIB-4 independently predicted faster eGFR decline, supporting a liver–kidney metabolic risk axis.
1️⃣4️⃣ FIB-4 may become a simple metabolic renal-risk marker.
Higher FIB-4 identified adults with faster renal decline even without established liver or kidney disease — a cheap tool with possible cardio-renal value.
1️⃣5️⃣ Newly diagnosed T2D often means late-diagnosed metabolic disease.
In 55,464 newly diagnosed Mexican T2D patients, obesity, dyslipidemia, hypertension, CKD, and complications were already frequent at diagnosis.
1️⃣6️⃣ HbA1c at diagnosis mirrors complication burden.
Complications rose with higher HbA1c and were most prevalent when HbA1c was >12%, reminding us that diagnosis often happens years after metabolic injury begins.
1️⃣7️⃣ CGM-derived GMI behaves like HbA1c for CV prediction.
In the GRADE-CGM substudy, GMI and HbA1c similarly predicted serious CVD and mortality, with overlapping rather than additive prognostic value.
1️⃣8️⃣ Time-in-range is clinically meaningful, but not independent of HbA1c yet.
Higher TIR was associated with lower CVD risk, but the signal attenuated after adjustment, suggesting TIR complements rather than replaces HbA1c.
Next..
2
7
10
915
Veeresh Hubballi retweeted

Jun 9
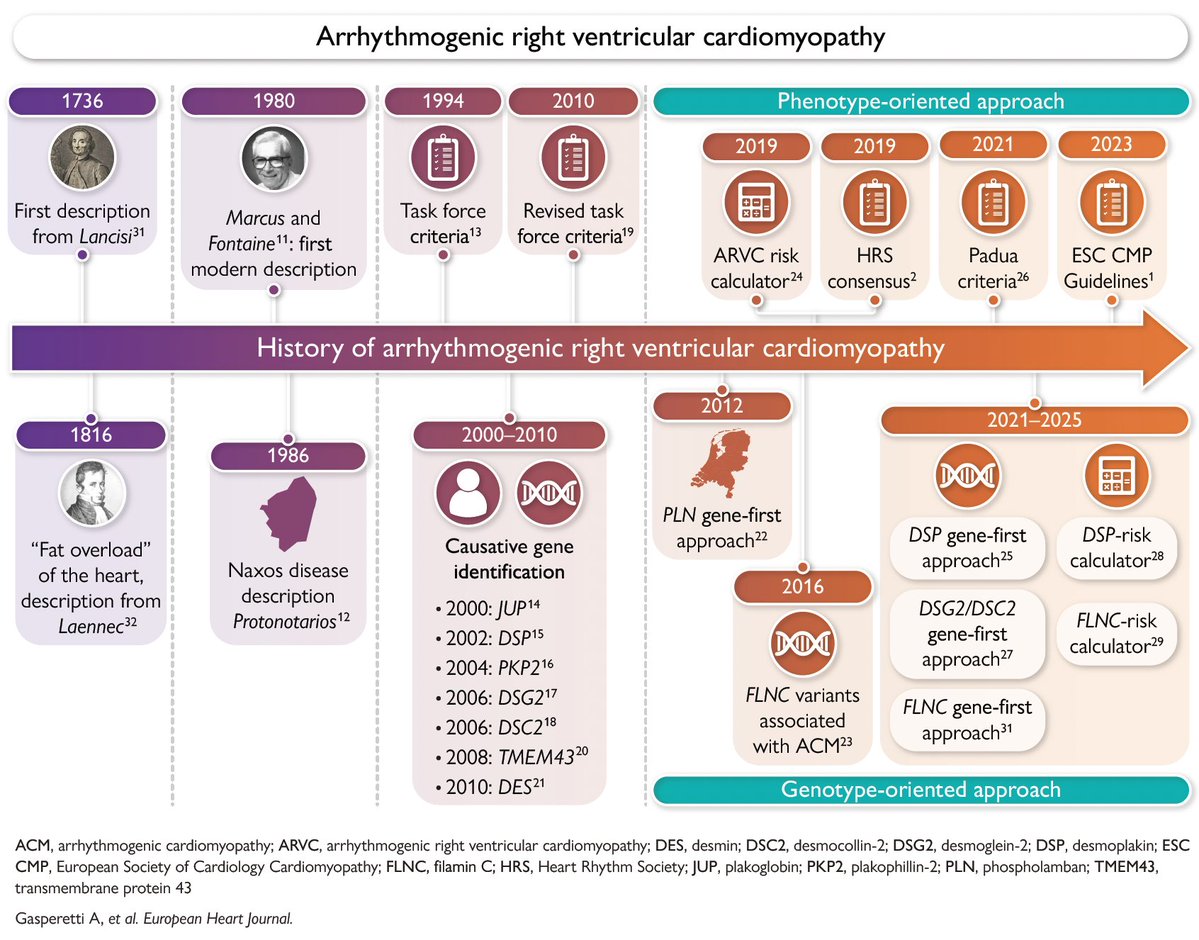
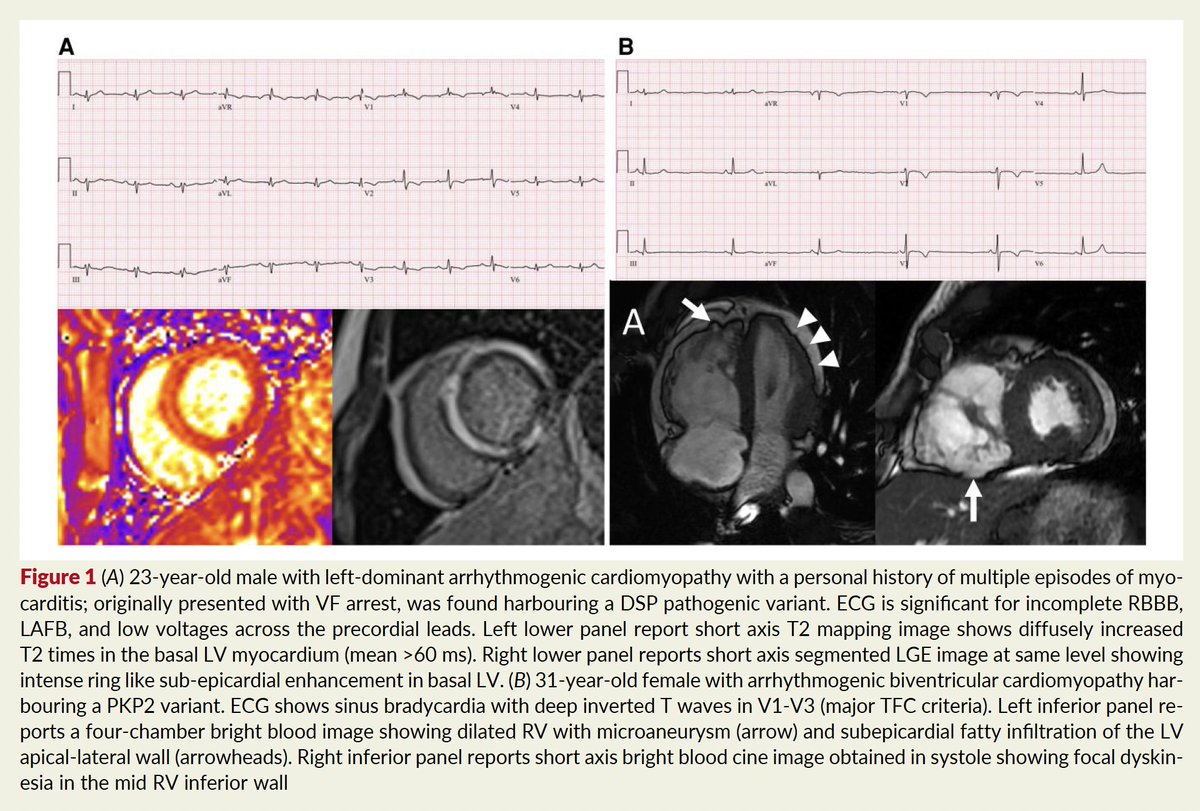
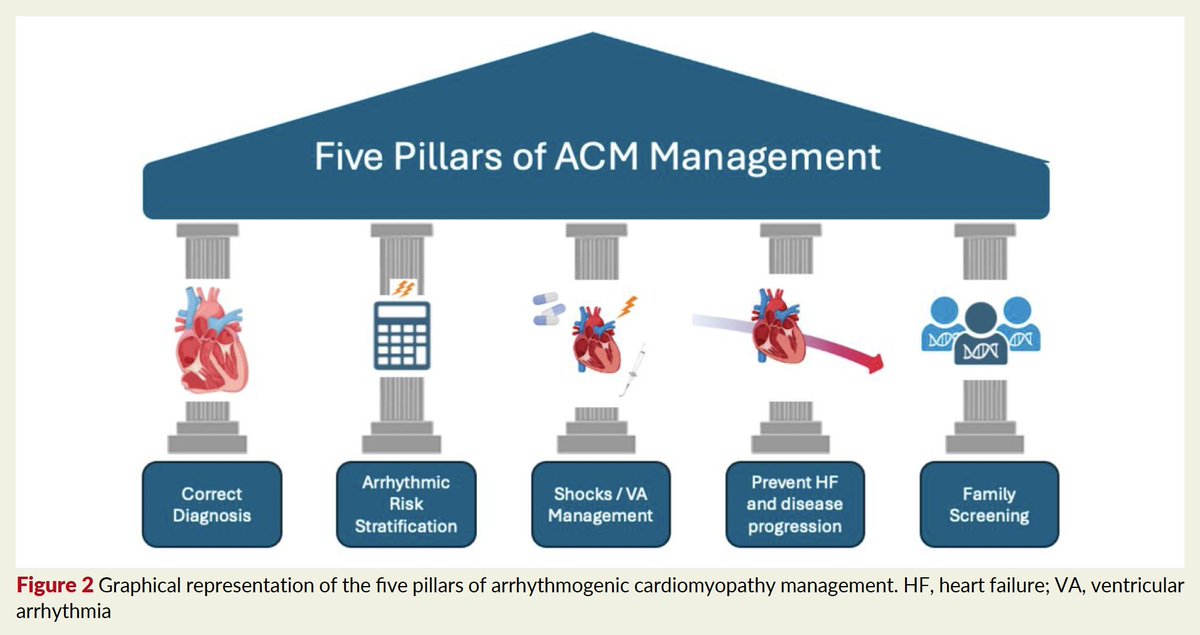
CARDIOPATÍA ARRITMOGÉNICA DEL VENTRÍCULO DERECHO
Revisión @ESC_Journals 👌
🔴Miocardiopatía hereditaria
🔴Escara ventricular y reemplazo graso
🔴Enfermedad multifascética
🔴Transición del enfoque centrado en el fenotipo ⏩genotipo
academic.oup.com/eurheartj/a…
83
201
9,491
Veeresh Hubballi retweeted

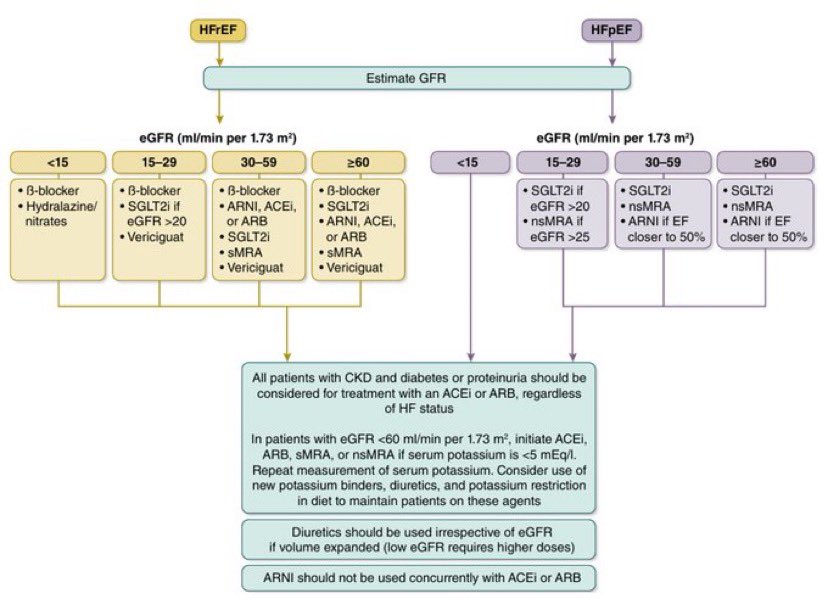
🧵 Managing HF in CKD: the eGFR-guided algorithm you need to know 👇
Heart failure management gets complicated when kidneys are involved. Here’s the evidence-based framework stratified by eGFR — for both HFrEF and HFpEF.
6
49
1,605
Veeresh Hubballi retweeted

11 Jun 2022
2023: Corona ended
2026: Hantavirus
29,953
92,080
410,906
Veeresh Hubballi retweeted

At the University of Minnesota, a human heart beats outside the body, without a pacemaker, connected to machines that keep it oxygenated. It has its own internal electrical system. It’s not a simulation: it’s a real organ beating outside the chest.
398
1,909
8,593
834,338
Veeresh Hubballi retweeted

Apr 23
Instead of watching an hour of Netflix, watch this 60 minute lecture from Steve Jobs after being fired from Apple. It will teach you more about building companies than most startup books ever will.
60
2,411
10,543
897,657
Veeresh Hubballi retweeted

Apr 21
The worlds largest Rangoli art of Shri Guru Raghavendra Swami
#ರಾಯರಿದ್ದಾರೆ 🚩🙏🏼
2
152
1,263
13,360
Veeresh Hubballi retweeted

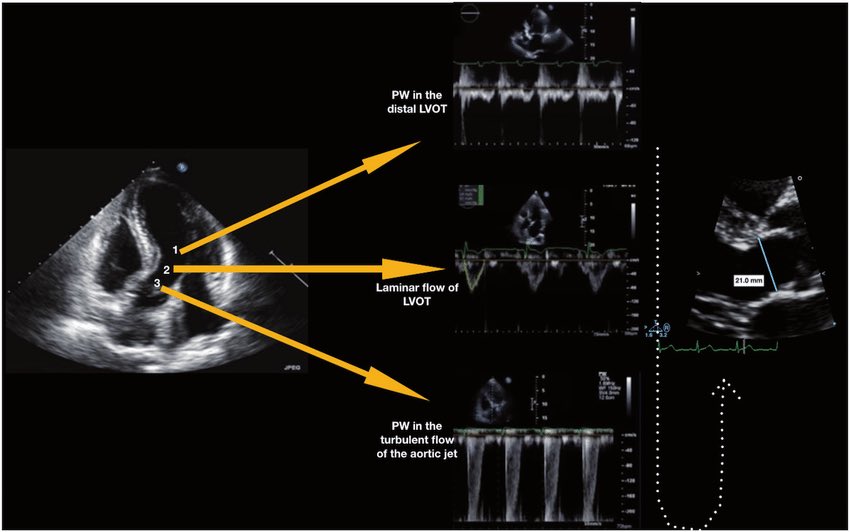
🫀 Did you know where the recommendation to place the pulsed wave Doppler sample volume 0.5–1 cm from the aortic valve to measure LVOT VTI comes from?
The answer is more interesting than it seems. It doesn’t come from a single study or an experiment designed for that purpose. It comes from a historical chain spanning nearly 40 years:
🔬 1982–1984 — The physical foundation
Pasipoularides and Murgo demonstrated using invasive catheters and mathematical models that in aortic stenosis there is a real zone of flow acceleration in the LVOT, just proximal to the valve, without any second anatomic obstruction. Pure hemodynamics — no Doppler yet.
👉 Bird et al. Circulation 1982 → doi.org/10.1161/01.CIR.66.4.…
👉 Pasipoularides et al. Am J Physiol 1984 → doi.org/10.1152/ajpheart.198…
📐 1984 — The apical 5-chamber view
Lewis, Kuo and Quinones were the first to validate cardiac output measurement using pulsed wave Doppler from the cardiac apex. They described placing the sample volume “immediately proximal to the aortic valve leaflets” — but without specifying any distance in centimeters.
👉 Lewis et al. Circulation 1984 → doi.org/10.1161/01.CIR.70.3.…
📏 1985 — The first numerical distance
Skjaerpe, Hegrenaes and Hatle (the Norwegian group) were the first to quantify this in Doppler: they empirically observed that flow acceleration began 0.5 to 1.5 cm proximal to the valve, and placed the sample volume just proximal to that zone. They directly cited Pasipoularides as supporting evidence. This was the first time a numerical distance appeared in the technique.
👉 Skjaerpe et al. Circulation 1985 → doi.org/10.1161/01.CIR.72.4.…
📊 1986–1988 — Practical consolidation
Otto et al. used ~1.0 cm. Oh, Tajik and the Mayo Clinic group explicitly established the range of 0.5 to 1.0 cm in 100 patients, justifying it as necessary to avoid the subvalvular acceleration zone. This is the figure we all recognize today.
👉 Otto et al. JACC 1986 → doi.org/10.1016/S0735-1097(8…
👉 Zoghbi et al. Circulation 1986 → doi.org/10.1161/01.CIR.73.3.…
👉 Oh et al. JACC 1988 → doi.org/10.1016/0735-1097(88…
📋 2002 — It becomes “official”
Quinones, Otto, Zoghbi and colleagues codified it in the ASE guidelines as “~5 mm proximal to the aortic valve”… but without citing any specific study to support it. It had already become expert consensus.
👉 Quiñones et al. JASE 2002 → doi.org/10.1067/mje.2002.120…
⚔️ 2017 — The debate reopens
Baumgartner et al. (EACVI/ASE) maintained the 0.5–1 cm recommendation. However, Hahn and Pibarot responded with a critical letter pointing out that the original articles from the 1980s measured at the aortic annulus, not 0.5–1 cm below it, and that moving away from the annulus introduces errors due to the elliptical and irregular shape of the subannular LVOT.
👉 Baumgartner et al. Eur Heart J Cardiovasc Imaging 2017 → doi.org/10.1093/ehjci/jew335
👉 Hahn & Pibarot. JASE 2017 → doi.org/10.1016/j.echo.2017.…
💡 Bottom line:
The 0.5–1 cm figure was never experimentally validated as the optimal distance. It emerged from empirical observations in the 1980s aimed at avoiding a flow acceleration zone that had been demonstrated with invasive catheters. It was adopted through accumulated clinical practice and later elevated to a formal recommendation by consensus. The debate over whether to measure at the annulus or 0.5–1 cm below it remains open to this day.
One of those recommendations we all follow but few know where it actually came from 🙂
Dr Benigno Valderrábano Salas
@MDBeni
@JaeKOh2 @ottoecho @WilliamZoghbi @ASE360 @EACVIPresident @NephroP @iamritu @PPibarot @hahn_rt @MAecocardio @SISIACOficial @SONECOM_AC @VazyurVasquez @Cardiotweets83 @HEARTof_echo @echobasics
17
134
411
54,372
Veeresh Hubballi retweeted

Apr 22
facebook.com/reel/8245149507…
🫀 Standard Coronary Angiographic Projections
🔹 RAO Caudal → LM, LCx, OMs
🔹 RAO Cranial → LAD, Diagonals
🔹 LAO Cranial → LAD foreshortening-free
🔹 LAO Caudal → "Spider view" — LM bifurcation
🔹 LAO/RAO 30° → RCA territory
#Cardiology #CathLab
2
154
736
47,919
Veeresh Hubballi retweeted

Apr 10
ಈ ಸಹೋದರಿಗೆ ಎಷ್ಟು ಅಭಿನಂದನೆ ಹೇಳಿದರು ಕಮ್ಮಿನೆ 😊 ಇವ್ರು ಸಂಸದ ತೇಜಸ್ವಿ ಸೂರ್ಯ
ಅವರ ಪತ್ನಿ, ಮಾತೃ ಭಾಷೆ ತಮಿಳು.
ಅದ್ರೆ ನೋಡಿ ಮದುವೆ ಆದ 2 ವರ್ಷಕ್ಕೆ
ಎಷ್ಟು ಸ್ಪಷ್ಟ, ಸ್ವಚ್ಛ ಕನ್ನಡ ಮಾತನಾಡೋದು ಕಲಿತಿದ್ದಾರೆ 😄
ಅವರ ಕನ್ನಡ ಪ್ರೇಮ ಕ್ಕೆ ಅಭಿನಂದನೆಗಳು 😊
ನಮ್ಮ ಪ್ರಶ್ನೆ ಇಲ್ಲೇ ಹುಟ್ಟಿ ಬೆಳೆದ ನಮ್ಮ ಝಮೀರ್ ಅಣ್ಣ, ಮತ್ತೆ ಆ ಪಂಗಡದ ಬಹುಪಾಲು ಜನಕ್ಕೆ ಹಾಗೂ ಕೆಲವು ಕನ್ನಡ ಉಳಿಸೋರಿಗೂ ಈ ಸ್ಪಷ್ಟತೆ ಭಾಷೆ ಯಲ್ಲಿ ಯಾಕೆ ಸಿಗಲ್ಲ. .??
ಅದು ಸಂವಿಧಾನದ ಹಕ್ಕೋ. .??
ಏನು ಮಾಯಾವೋ 😇😇
ಆದ್ರೂ ಬಿಜೆಪಿ ಕನ್ನಡ ವಿರೋಧಿ 💁💁💁
@Tejasvi_Surya 👍👍
26
145
1,106
79,622
Veeresh Hubballi retweeted

🩸 Bleeding on anticoagulation is NOT a complication… it’s a turning point
⚠️ The problem
We prescribe anticoagulants to prevent:
👉 Stroke
👉 MI
👉 VTE
But the most frequent complication is:
👉 Bleeding
And here’s the uncomfortable truth:
> Bleeding often determines prognosis more than thrombosis
🧠 Why this matters
Bleeding is NOT just an event.
It triggers:
❌ Treatment interruption
❌ Fear-driven underdosing
❌ Permanent discontinuation
👉 Leading to ↑ stroke, ↑ MI, ↑ mortality
🔥 Key clinical reality
📊 Major bleeding:
~1-3% per year
30-day mortality >15%
1-year mortality >25%
👉 That’s NOT benign
⚖️ The real battlefield
Every anticoagulated patient lives here:
👉 Thrombosis vs Bleeding
And we often focus on only one side.
🧠 What experts are telling us (ESC)
This is the new paradigm 👇
1️⃣ Risk is dynamic
Bleeding risk is highest:
👉 Early after starting anticoagulation
👉 In elderly / multimorbid patients
👉 Reassess continuously, not once
2️⃣ Not all bleeding is equal
🚨 Critical sites = high mortality:
Intracranial
GI
Retroperitoneal
Pericardial
👉 Even small volumes can kill
3️⃣ Combination therapy is dangerous
👉 OAC antiplatelet = 2–3× ↑ bleeding
✔️ De-escalate EARLY
✔️ Avoid triple therapy when possible
4️⃣ Prevention is powerful
Simple interventions:
✔️ PPI for GI protection
✔️ Avoid NSAIDs / SSRIs when possible
✔️ Correct dosing (DOAC underdosing = worse outcomes)
👉 Most bleeding is preventable
🚨 When bleeding happens
Think in 3 steps:
🩸 1. Stabilize
Stop anticoagulant
Airway, oxygen, access
Fluids transfusion
🧪 2. Reverse (if needed)
VKA → PCC Vitamin K
Dabigatran → Idarucizumab
FXa inhibitors → PCC (± Andexanet)
🔎 3. Find and control the source
Endoscopy
IR embolization
Surgery
⚠️ The biggest mistake
> “Let’s stop anticoagulation and never restart”
🧠 The evidence says:
👉 NOT restarting = ↑ stroke ↑ death
✔️ Restart early when safe
✔️ Individualize timing dose
🔄 The future
We are moving toward:
👉 Personalized anticoagulation
👉 Dose tailoring
👉 Drug selection based on bleeding profile
🎯 Take-home message
Anticoagulation is NOT binary.
It is:
👉 A continuous balance
👉 A dynamic decision
👉 A personalized therapy
🤓 Final thought
> The goal is not to avoid bleeding
The goal is to survive both bleeding AND thrombosis
📚 Reference
Galli, M., Simeone, B., ten Berg, J., et al. (2026). European Heart Journal: Acute Cardiovascular Care.
doi.org/10.1093/ehjacc/zuag0…
ALT
2
114
321
23,837
Veeresh Hubballi retweeted

I don’t usually post anything here apart from cricket, but man.
These words by Samay Raina really hit me straight in the heart 💔😢
34
987
5,726
160,877
Veeresh Hubballi retweeted

Mar 28
Bappa, please be with my team the way you were last year. ❤️🙏🏻
10
132
2,098
15,162
Veeresh Hubballi retweeted

Mar 28
There’s something about cricket in India that you can’t really explain. It’s been there since childhood, in the background of every home, every conversation, every summer. And then IPL comes around and suddenly it’s everywhere again.
And RCB fans, honestly, the most patient and loyal. Every year it’s “e sala cup namde” with the same belief, same excitement. You have to respect that kind of love for a team. ❤️
34
426
3,809
79,559