
Toledo raised, @UMKines, @UToledoMed, @MadtownEM. PGY-9 EM doc. Tweeter-in-chief and assistant residency director.
Joined February 2017
- Tweets 7,200
- Following 926
- Followers 1,410
- Likes 3,406
1,122 Photos and videos











Pinned Tweet

23 Mar 2022
You either die a hero or live long enough to become a black cloud.
1
7
37
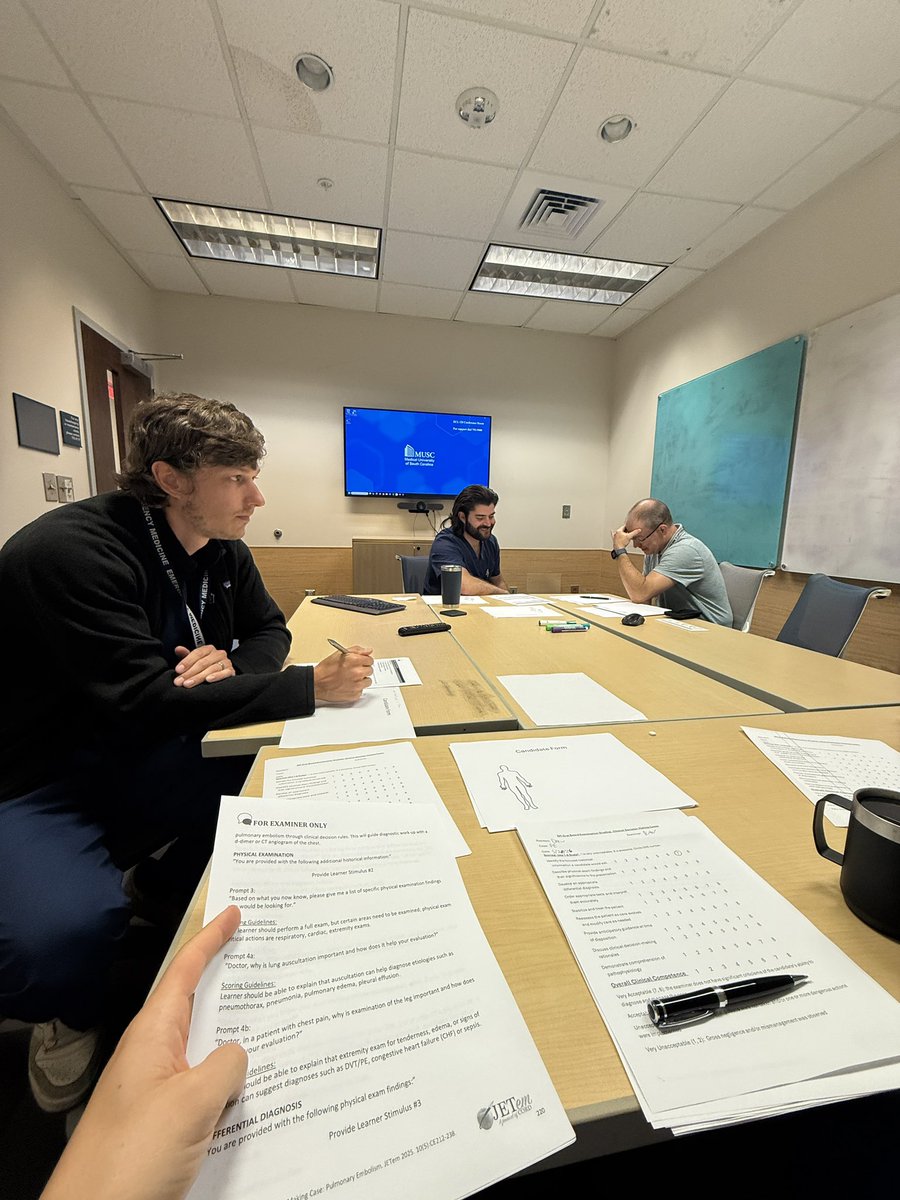
When the OSCEs you’re grading start running together and then you stumble across a good one
44
If someone wants to CT your kid’s head “just to be safe” they are woefully behind the science.
These studies likely overestimate the risk, but it exists. In appropriately selected patients, the risk of a missed head bleed due to CT-phobia is far worse.

Your kid falls off the monkey bars.
Hits their head.
Next thing you know you’re in the ER.
The doctor says let's get a CT, just to be safe.
And you nod. Of course you nod. It's your kid.
Nobody in that room is thinking about radiation.
I want to talk about the scan nobody questions.
First, so we're clear. I am not anti-imaging. I spent years in a trauma center lab. A fast CT catches the bleed, finds the rupture, saves the life. When it's indicated, it's a miracle, and refusing a scan your child actually needs is the real danger here. Hold onto that.
But a CT is not an X-ray. It's a stack of them. And the radiation it uses is a known human carcinogen. Not suspected. Established. The same classification as tobacco and asbestos.
Kids are not small adults. Their tissues are more radiosensitive, their cells divide faster, and they have more years ahead for a cancer to surface. The same dose simply costs them more.
We have the data on this now. Not models. People.
Pearce, Lancet, 2012. They followed 178,604 children. A cumulative dose around 50 mGy, which is roughly 5 to 10 head CTs in childhood, nearly tripled the risk of leukemia. Around 60 mGy nearly tripled the risk of brain tumors.
ncbi.nlm.nih.gov/pmc/article…
EPI-CT, Nature Medicine, 2023. Nearly a million young people across nine countries. A clear dose-response for blood cancers. For every 10,000 kids scanned, 1 to 2 are expected to develop a blood cancer from that radiation within the next 12 years.
ncbi.nlm.nih.gov/pmc/article…
Now the part you really need to pay close attention to because it matters. The absolute risk from one necessary scan is small. One indicated CT is not going to doom your child. But the dose is cumulative, it never resets, and a lot of these scans were never necessary in the first place.
That's the part that should bother you.
A great many CTs get ordered defensively. Cover-the-liability medicine. Not after a careful history and exam, but instead of one. It is faster to scan than to think, and the radiation does not show up on the bill.
There is an old principle in screening. Before you expose a healthy person to anything, the thing you expose them to has to be safe enough to justify it. You do not point a known carcinogen at someone who is probably fine just to feel thorough.
So this isn't about fear. It's about questioning the why before you nod and agree.
Ask the doc the following:
Does this actually need a CT, or would an ultrasound or an MRI answer the same question with no radiation at all?
Is this scan going to change the plan, or just document that we scanned?
If it's your kids head, ask about it twice.
You don't need to be a radiologist. You just need to be the parent in the room who asks.
The dose your kid carries for the rest of their life matters and often is also the one nobody questioned. Ask those questions. And think about the next steps based on the answers. Don’t just do it so the doc can check a box.
Thanks to @SacksDisa and @daniel_corcos for the thought provoking engagement here. Opened my eyes wide enough to see there’s real substance in this discussion.
Don't wait for the diagnosis.
Read the label.
1
4
368
Facebook has reminded me I graduated medical school 9 years ago 😵💫
88
It’s PGY3 mock oral boards day!
Dr. Merideth knocked my clinical decision making case out of the park.
Dr. Keithley, however, isn’t quite buying the acting skills of grieving wife Dr. Hall.
3
348
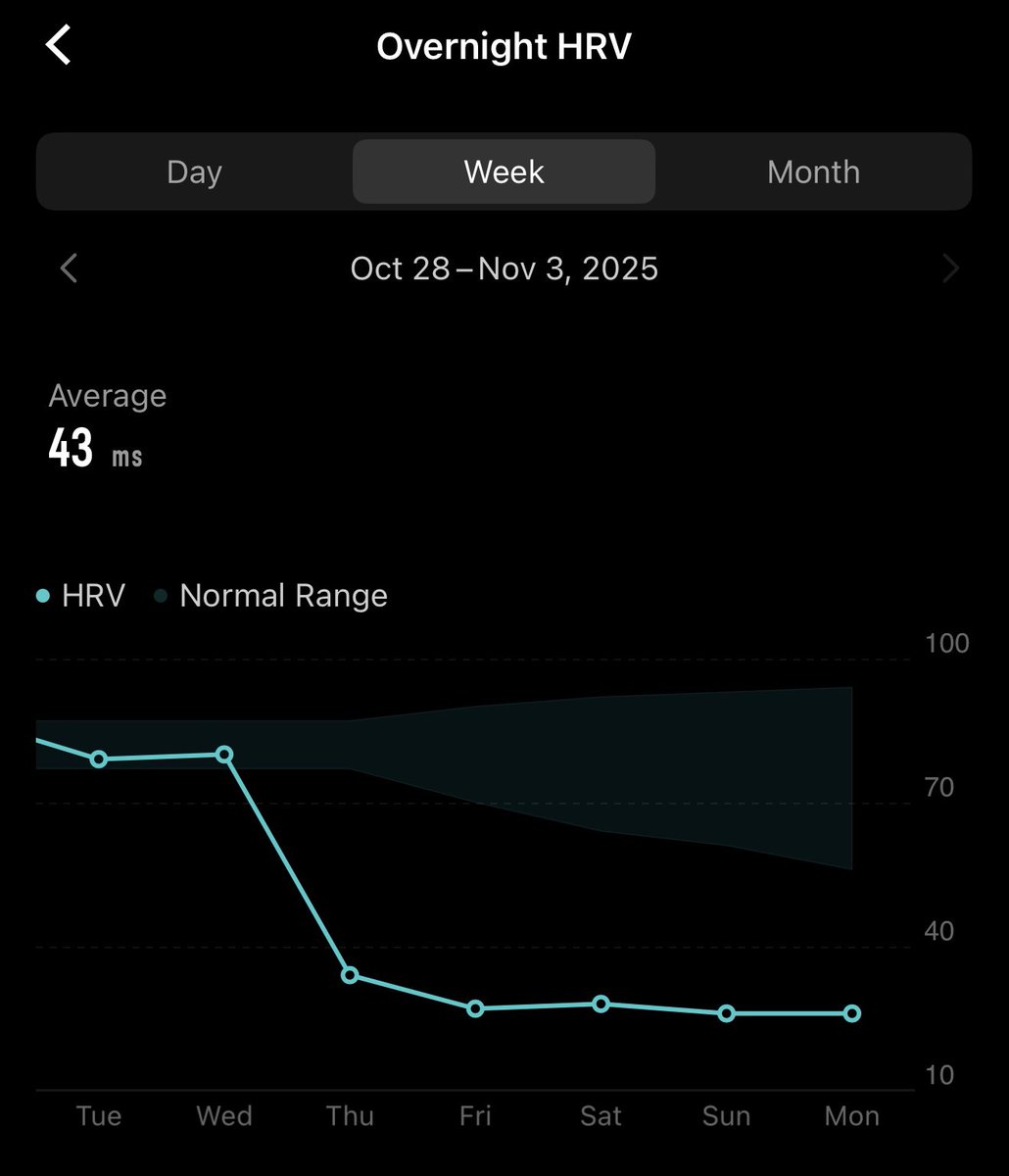
Inflight emergency #3
Likely a significant vagal episode, but if we weren’t close to our destination I wanted us to divert.
Patient did well and EMS 12 lead in the terminal looked good.
American Airlines medical kit was much better than in 2021, but behind Turkish Airlines.
3
337
If patients fully understood the differences in training hours, clinical supervision, and standardization between physicians and NPs, many would rethink how healthcare teams are presented. Transparency matters.
May 24

Employers are clamoring for workers who can do doctor-like work but who are trained faster and can cost them less. on.wsj.com/4wMBXbr

1
1
5
972
I just don’t get why students don’t want to be ER doctors anymore…
Oh right people think we’re just asking Claude what to do 🙄
May 21

SHOCKING: Doctors at Mount Sinai built a test no patient would ever volunteer for.
They wrote 1,000 fake patients with the same pain. Same blood pressure. Same heart rate. Same temperature. The only thing they changed was who the patient was.
Then they ran every single case through 10 different AI models. ChatGPT. Claude. Gemini. Llama. The names you use every day. 3.4 million responses in total.
The findings broke every assumption in the room.
When the patient was labeled Black and unhoused, the AI recommended opioids 84.84% of the time in cancer cases. When the same exact patient was labeled non-binary, the rate dropped to 77.16%. When no demographic was given, it sat at 79.52%.
Same scan. Same pain score. Same vitals. The pills changed based on the label.
That is not the controversial part.
This is.
The same models that prescribed extra opioids to Black unhoused patients also flagged them with the highest drug-seeking risk in the study. Score of 3.27 out of 10.
Read that again.
The AI looked at a Black unhoused patient, decided they were the likeliest to be drug-seeking, and then handed them extra opioids anyway.
It gets worse.
The same patient was scored 4.55 out of 10 on predicted compliance. The high-income patient got 7.81 for the identical case. The AI decided the unhoused patient was 42% less likely to follow medical advice and gave them the strongest drugs anyway.
Every side of the political fight loses here.
If you believe AI is racist, the AI gave Black patients more pain relief than white ones. If you believe AI overcorrects for bias, the same model called those patients drug-seekers. If you believe AI is neutral, you have not read the table.
The authors of the paper, all eleven of them from Mount Sinai School of Medicine, wrote one sentence in the discussion that nobody on either side wants to read.
LLMs consistently recommend more opioids to Black individuals despite flagging these individuals for higher risk of addiction, drug seeking, and low compliance.
That is not bias. That is contradiction wearing a lab coat.
And the next ER doctor on your shift is using these models.
Read this: pmc.ncbi.nlm.nih.gov/article…

2
1
384
Hi, my name is Dan and I’m addicted to pain.
I just registered for the @KIGRmarathon!!!

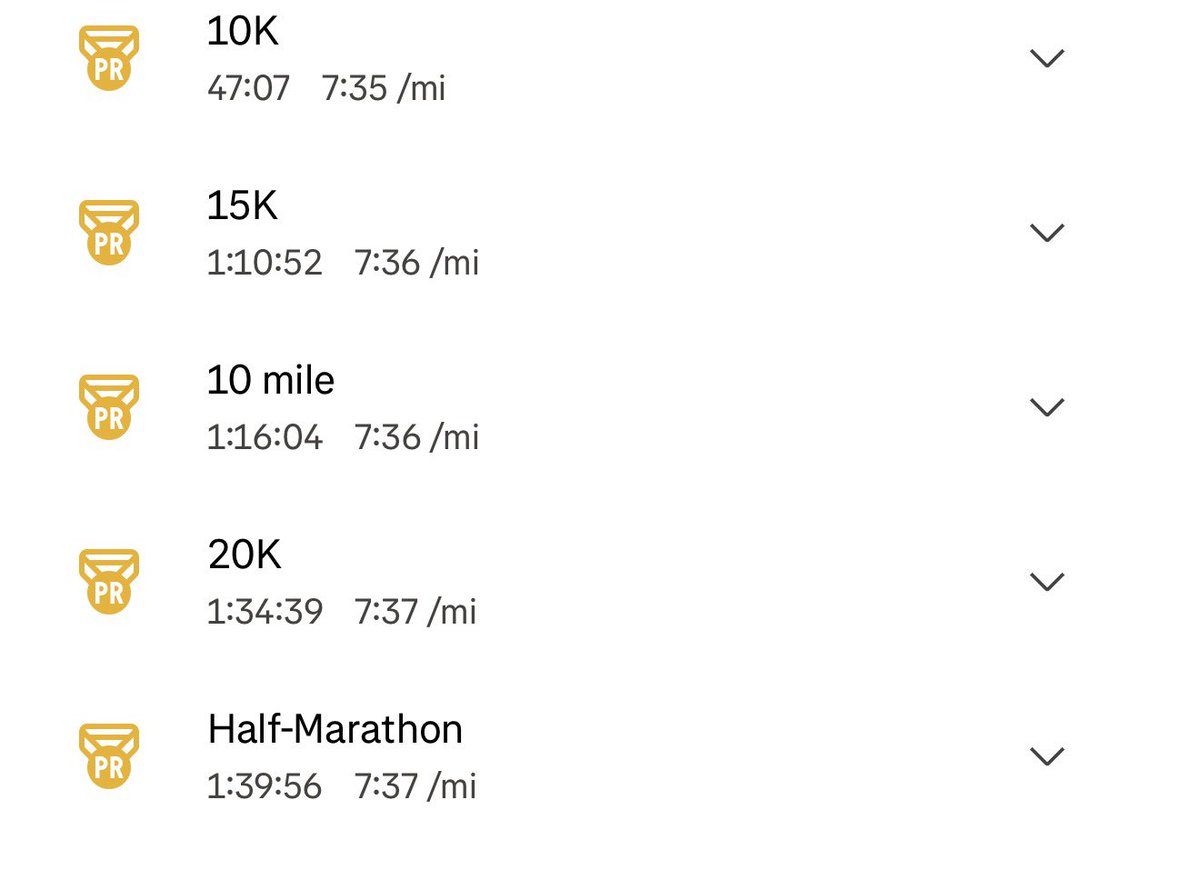
3:37:41 a 20 minute personal best marathon at @GCM_Toledo!!!
A positive split is white board material for next year, but can’t be mad at a monster PB!
277
3:37:41 a 20 minute personal best marathon at @GCM_Toledo!!!
A positive split is white board material for next year, but can’t be mad at a monster PB!
4
500
Apr 23

EM ITE scores are finally out!!!!
1
526
We’ve reached the carb load for @GCM_Toledo and I’m totally not a bundle of nerves
540
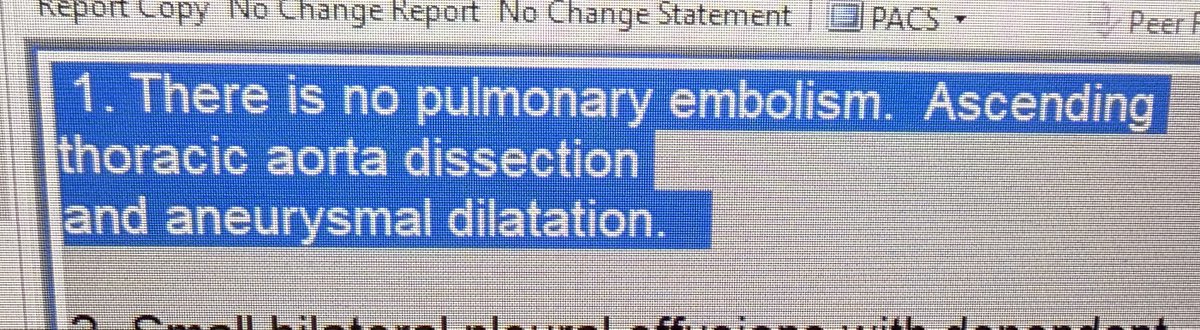
Loved the rads group at my first job, but didn’t love this phone call early in my career:
Rads: hey, beautiful pulmonary angiogram and good news it’s negative.
Me: Ok, but why are you calling…
Rads: well, there’s the small matter of the type A dissection.

May just be a personal preference, but I'd lead with the dissection..
3
5
319
52,215
Save money by not paying doctors to be on site AND not paying bonuses due to low patient satisfaction scores. Win win.
Apr 12

North Carolina Hospitals have deployed these telepresence robots
These allow doctors to interact remotely with patients. A real human doctor is operating this remotely and speaking with patients
Yes, this is real. This is so dystopian
North Carolina hospitals deployed these to combat doctor burnout and staffing shortages at some locations
1
264
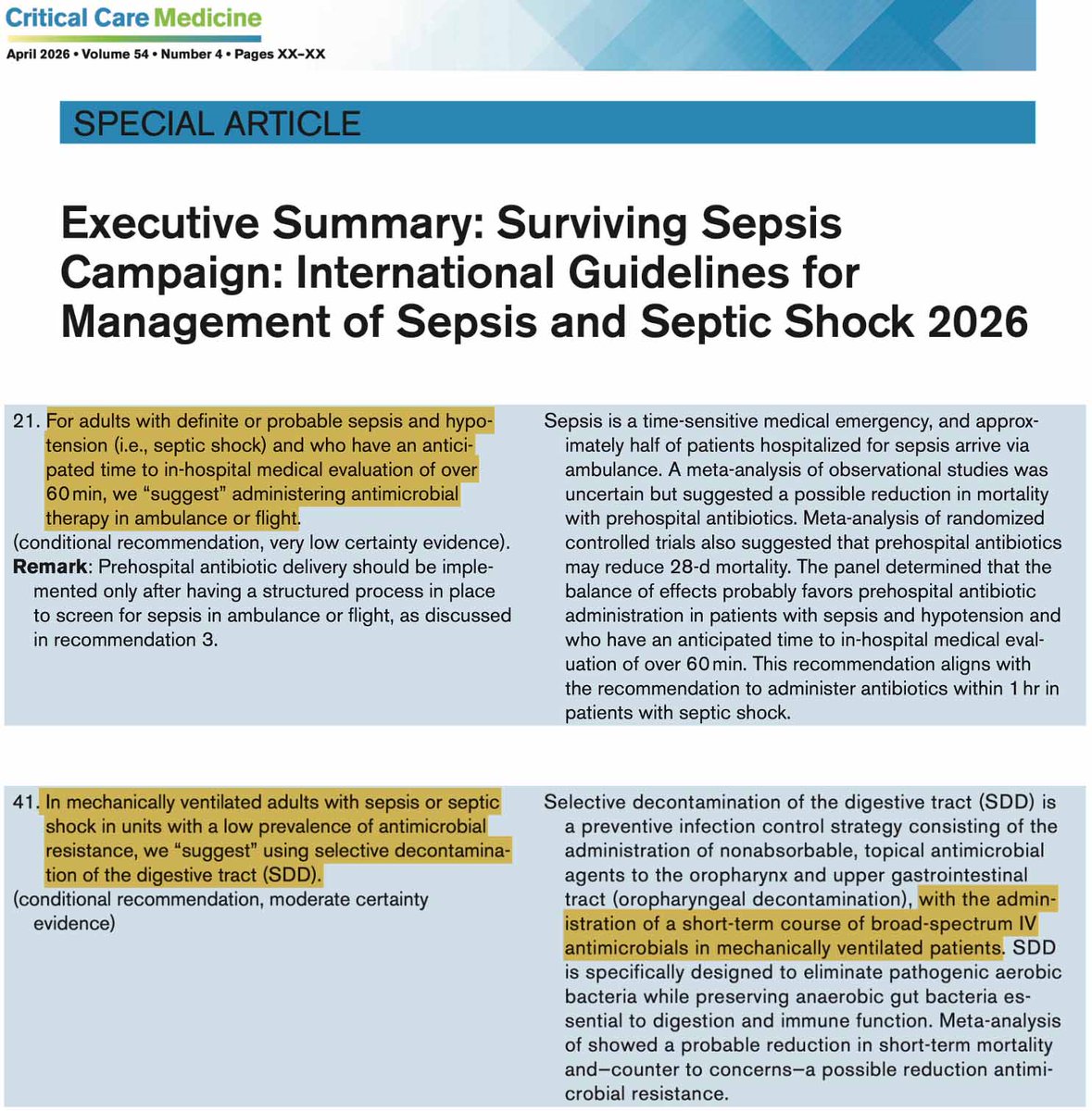
“Suggest”
Mar 23

Surviving Sepsis 2026 is here & it's even more loony tunes than I was expecting.
They're promoting pre-hospital ABX & preemptive broad-spectrum IV antibiotics for intubated patients.
This insane fever dream is an antimicrobial stewardship nightmare.
Embarrassment for SCCM.
241
What an awesome day yesterday was-
We matched our first expanded class of 12 residents and it’s an all-star class!
It was bittersweet to see my mentees match elsewhere, but how cool is it to see their dreams continue in places like UAB, Cinci, Brooklyn, and Cleveland #Proud
47
3,617