
Chief of Surgery at City of Hope - Chicago; colorectal surgeon researching antisense abx to treat C. difficile.
Joined January 2018
- Tweets 6,773
- Following 329
- Followers 939
- Likes 38,467
95 Photos and videos













David B. Stewart, MD, MHA, FACS, FASCRS retweeted

Jun 9
The problem is the fairy tale universities and their academic medical centers sold to the people they recruited.
These positions were never supposed to exist in this form. NIH should never have enabled universities to treat faculty as grant-chasing mercenaries whose purpose is generating indirect cost revenue.
NIH enabled university medical centers to expand without limits using this model that allows them to offload the cost.
Scientists were convinced it was reasonable to be hired as faculty while being responsible for their own salaries and receiving minimal institutional support. Meanwhile institutions with billions in annual revenue somehow find money for seven-figure administrators but not for the scientists they employ.
The result is a system where faculty spend their time writing grants and paperwork rather than doing science, while universities collect overhead and tell the government on their effort certifications that they are spending time on research when they are not. They are spending time on grant writing and paperwork.
If a university wants to hire a scientist, it should pay that scientist’s salary. Everything else is a scheme to extract money pretending to be a research enterprise.

The reality is that most of us are already applying for 30 or 50 grants per year and getting none. Not sure more limits is better. Also no one can really support their own salary (like we have to), their staff's, and all the research costs on 400k/year. American science is dying
12
31
207
30,678
David B. Stewart, MD, MHA, FACS, FASCRS retweeted

After heart surgery, the parents of a 13-year-old girl were told that their daughter was dying, and that they should start making end-of-life decisions, including donating her organs.
Upon transferring their daughter to another hospital however, they were told that doctors at Oregon Health and Science University had installed her new heart valve upside down.
“Doctors at Seattle Children's removed the inverted valve and replaced it with a different one, properly positioned. Her heart promptly began to function correctly. She was successfully taken off cardiac bypass and no longer required ECMO.
Her condition continued to stabilize over the following days in Seattle Children's ICU. After more than a month in critical condition, she was able to return home with her parents.”

1,447
12,583
46,547
1,668,245
David B. Stewart, MD, MHA, FACS, FASCRS retweeted

Jun 8
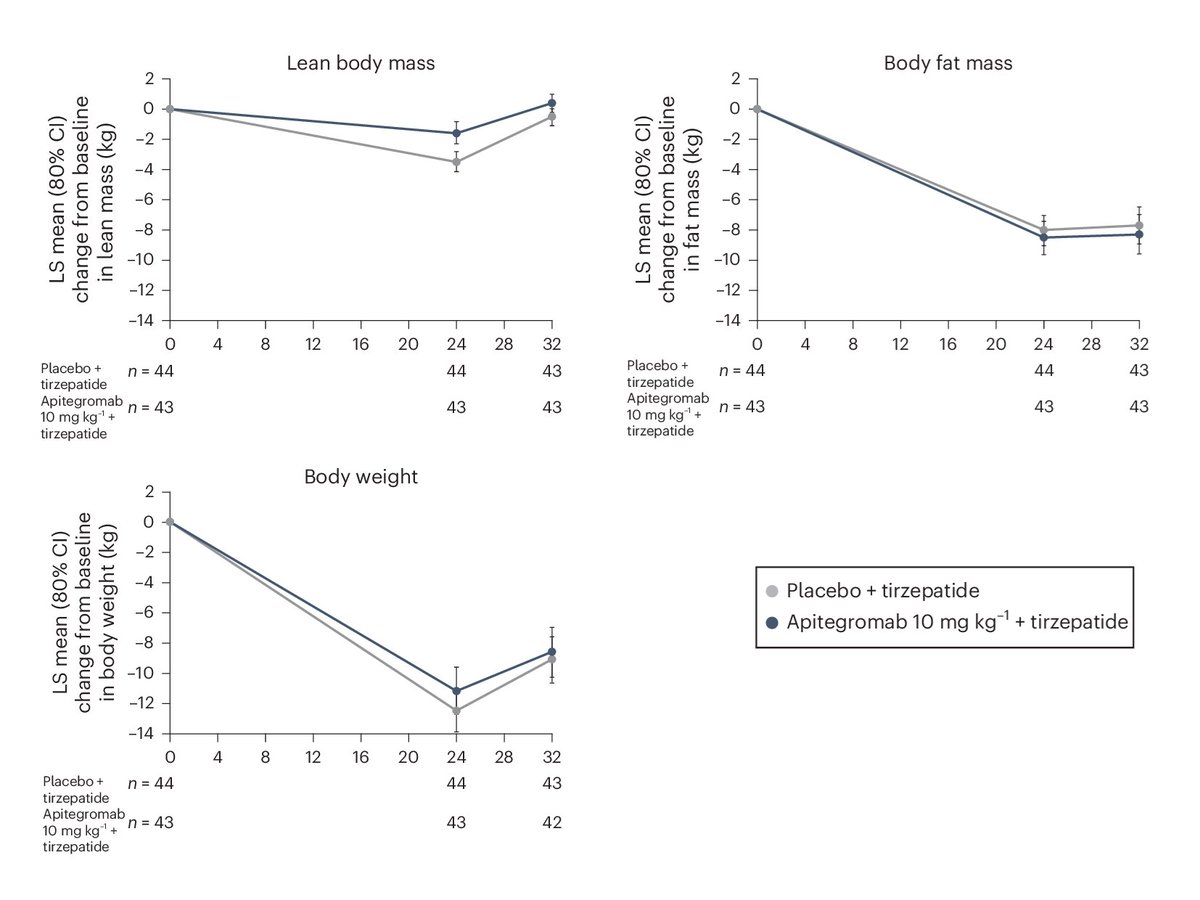
New myostatin inhibitor results!
Over 24 weeks, people on tirzepatide lost ~30% of body weight as lean mass.
People on tirzepatide plus a myostatin inhibitor lost ~15% of body weight as lean mass!
It'll soon be possible to lose weight while barely losing muscle!
42
45
615
57,432
David B. Stewart, MD, MHA, FACS, FASCRS retweeted

This thread is a perfect example of Hayek’s fatal conceit.
Here a pro- central planning pundit points to one preferred version of price setting, declares that it “works,” and then treats every other failure of price setting as somehow unrelated.
Maryland has all payer hospital rate setting and global budgets. You like the outcome, so that counts as smart planning (not to mention Maryland has plenty of flaws).
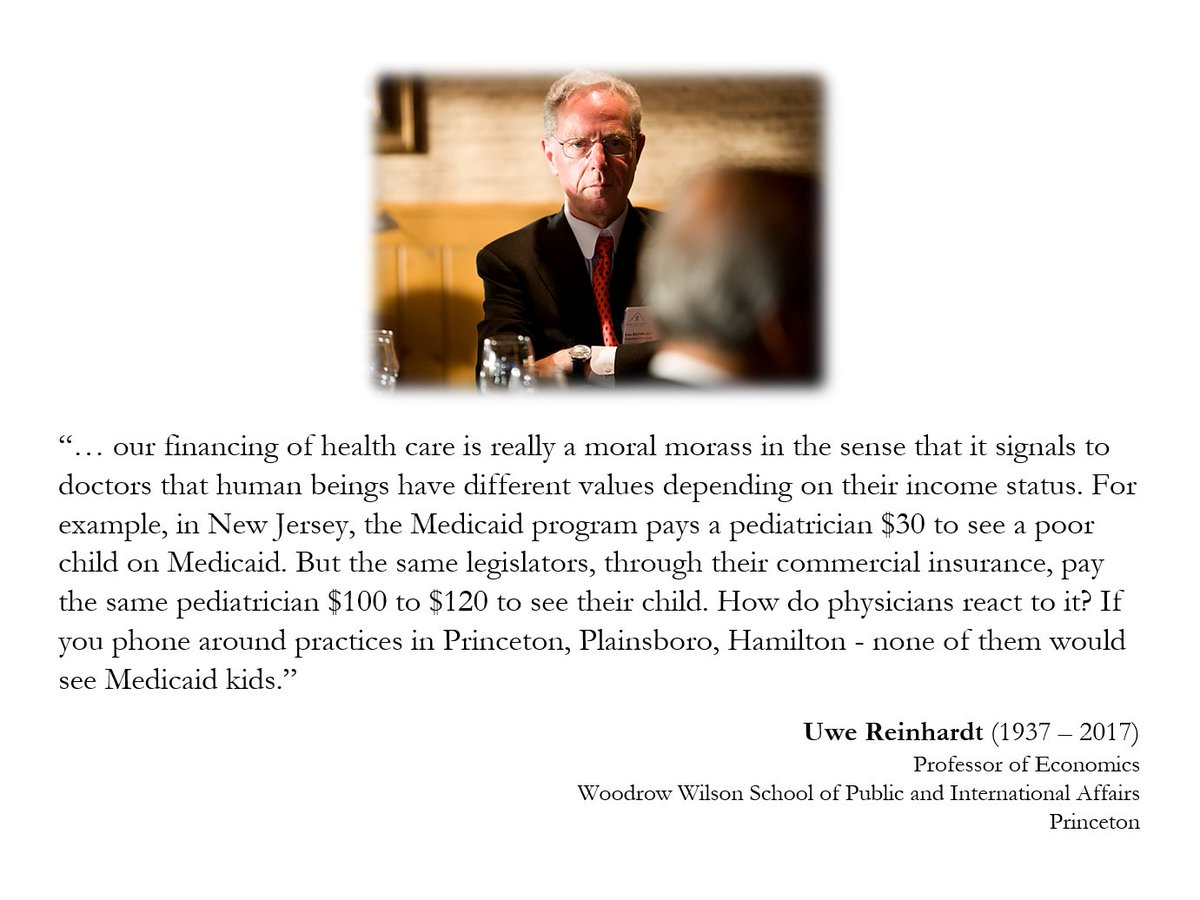
Medicaid pays pediatricians far below commercial rates, patients struggle to find doctors who participate, and suddenly that is not a problem with rate setting per se. That is just the wrong rate setters, or the wrong politicians, or the wrong program. Or Medicare pays hospitals 5x what a doctors office charges. Just the wrong central planners again.
But the core problem is the same. No commission has access to the dispersed knowledge needed to set the right price at the local level.
It cannot know the capacity of each pediatric office, staff wages, rent, malpractice costs, supplies, local demand, physician burnout, opportunity cost, patient urgency, or how much a parent values being seen today instead of six weeks from now.
Prices are signals that coordinate resource use in the face of scarcity.
When planners suppress or manipulate prices, the cost does not vanish.
That is the unseen harm.
The fatal conceit is believing the problem is never central planning itself. It is always that the right central planners have not been put in charge yet.
If the concern is access, subsidize patients. Give people purchasing power. Do not pretend a commission can calculate the right price for every clinical situation from above.
There’s zero reason that every American can’t have access to pediatrician visits without any more government involvement than a means tested cash equivalent subsidy. There’s no more of a market failure there than with food.
But central planners don’t want that. They just want control.
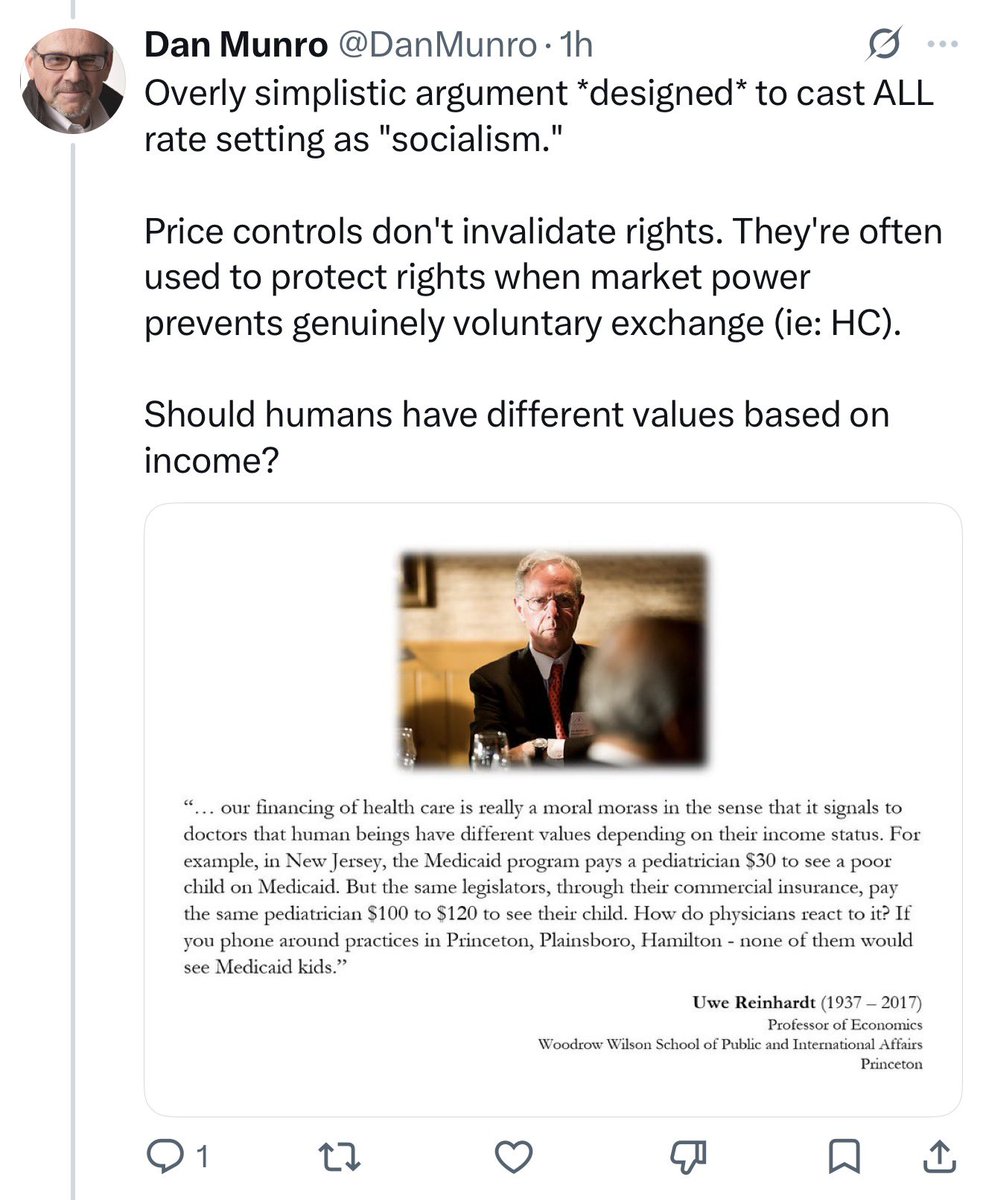
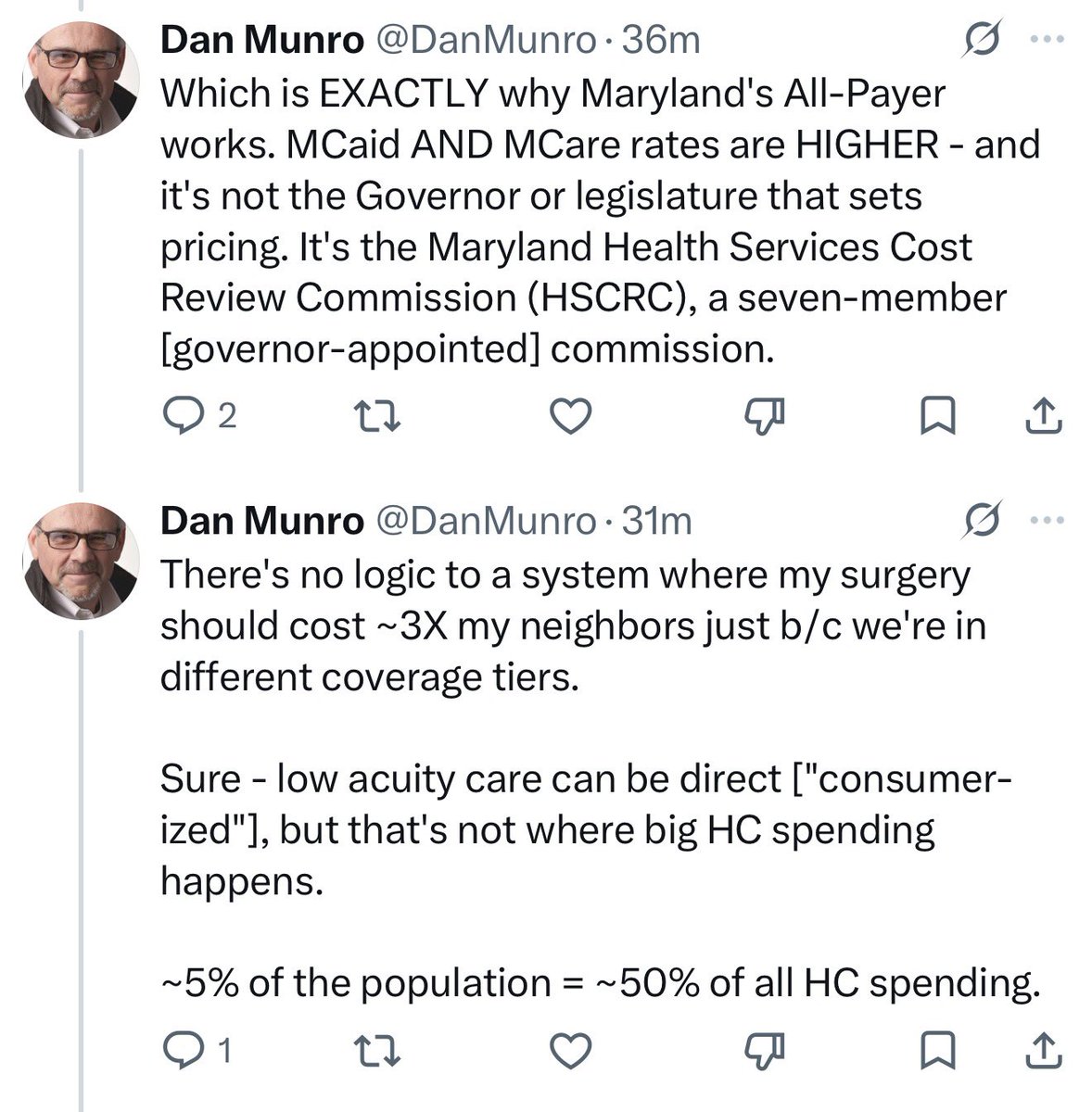

Overly simplistic argument *designed* to cast ALL rate setting as "socialism."
Price controls don't invalidate rights. They're often used to protect rights when market power prevents genuinely voluntary exchange (ie: HC).
Should humans have different values based on income?
1
11
42
4,424
David B. Stewart, MD, MHA, FACS, FASCRS retweeted
Admin: “we are rolling out Epic Chat!”
Doctor: “ok… how many messages will I be getting”
Admin: “only about 10-20 per hour, 24/7.”
Doctor: “oh… so I need to silence my notifications then”
Admin: “oh heavens no! Then you might miss that one message that is critical. And we will hang you out to dry if you do.”
Doctor: “what about when I sign into epic in my clinic”
Admin: “well that’s a different context for epic. So none of your messages will reach you until you log back into the hospital epic.”
Doctor: “but I’m still responsible for all the messages even when they don’t reach me?”
Admin: “bingo”
52
39
550
54,955
David B. Stewart, MD, MHA, FACS, FASCRS retweeted
I see Medicaid patients in my neurosurgery clinic who have to wait months for a standard epidural steroid injection. It is a typical, straightforward procedure. A privately insured patient would have it done in a matter of days. California's Medicaid can't figure out how to fund the system to offer the same level of access in Medicaid.
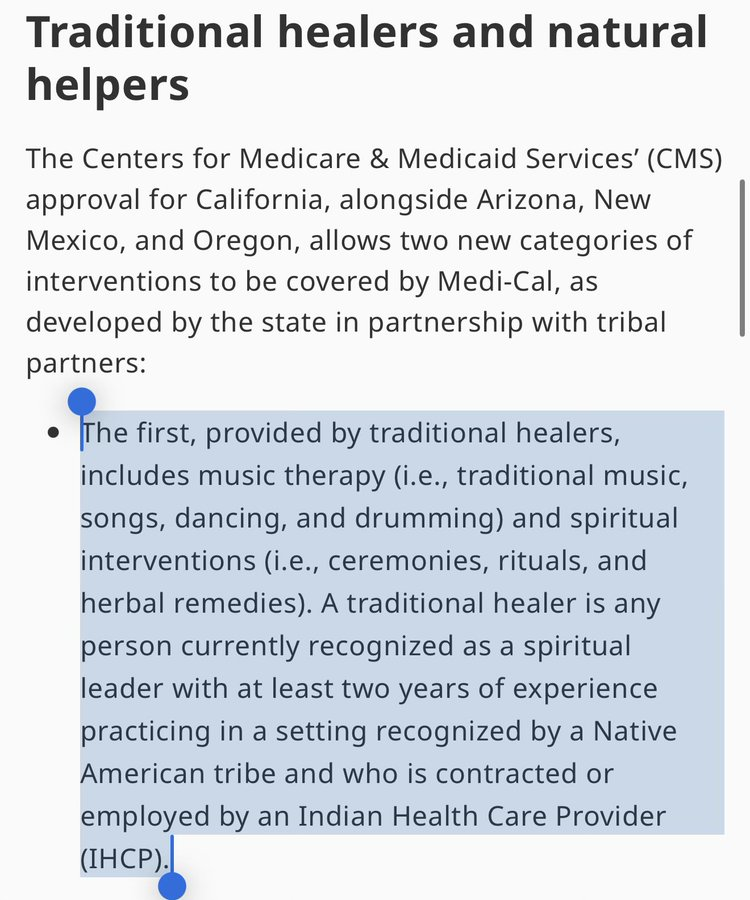
Yet California recently found a way to use Medicaid funds to pay for "Traditional Healers," a benefit that officially includes music, dancing, drumming, ceremonies, herbal remedies, and spirituality.
This is jarring, but the real issue is not simply that a state is paying for quasi-spiritual services. It is what this reveals about how Medicaid actually works.
Through a complex architecture of federal waivers, managed-care capitation rates, and matching funds, a program meant to be a medical safety net has morphed into a generalized fiscal machine.
States have learned to use federal matching dollars to fund favored social priorities while disguising the true cost to taxpayers. The result is a bizarre asymmetry in how we police care. When a physician requests a spinal injection or an MRI, the system demands strict documentation, guidelines, and prior authorization.
But for politically protected, hard-to-verify services like spiritual healing, the system is remarkably deferential. The payer is billed for subjective encounters it cannot easily observe. It is the exact kind of blind-spot architecture that makes massive fraud possible in areas like hospice and home health, where billing easily outruns verification.
Medicaid was created for a moral purpose: to provide concrete medical care to people who cannot afford it. But a safety net needs a floor, not a slush fund. Pretending that everything is health care just ensures the sickest patients are the ones kept waiting. You can read my full essay on how the Medicaid machine really works below:
26
74
429
647,258
David B. Stewart, MD, MHA, FACS, FASCRS retweeted

May 25
🚨BREAKING: Delta Dental calls itself a "nonprofit" for the tax breaks, while its CEOs raked in $48 MILLION over four years.
Her pay jumped from $4.5M to $15M a year.
Meanwhile, they slashed dentist reimbursements and patients paid more.
This is how "nonprofits" game the system.

1,290
15,274
24,456
418,362
David B. Stewart, MD, MHA, FACS, FASCRS retweeted

May 24
Capitalism is the solution in healthcare. But, there is a reason we have anti-trust laws. There are reasons why we have the @FTC
We are at a point in time where the big vertically integrated carriers and providers are abusing their market positions. Neither agency has done shit to stop them over the past decade
There is a bill, the Break Up Big Medicine Bill from @HawleyMO and @SenWarren. I have talked to democratic senators who have said they will support it if more republican senators do. They want to match 1 dem to 1 rep. Totally dumb shit. So they say nothing.
Other than Josh, not a single republican senator I have talked to has the guts to stand up for it. Period. They won’t give a reason. They just won’t do it.
If you want less government in healthcare, it can’t happen until these conglomerates are broken up
If you want single payer or M4A , it can’t happen until these conglomerates are broken up
Quit bitching and call your senator and tell them to grow a spine and support this bill
May 24

This free market BS is ridiculous!! Capitalism (the basis of free market BS) is not the correct solution for social services. EVER! Once a social service system is implemented with a profit motive rather than a people motive, it is lost. Case in point, health insurance.
224
133
848
172,980
David B. Stewart, MD, MHA, FACS, FASCRS retweeted

May 22
We deserve better.
151
7,243
51,298
482,784
David B. Stewart, MD, MHA, FACS, FASCRS retweeted

May 22
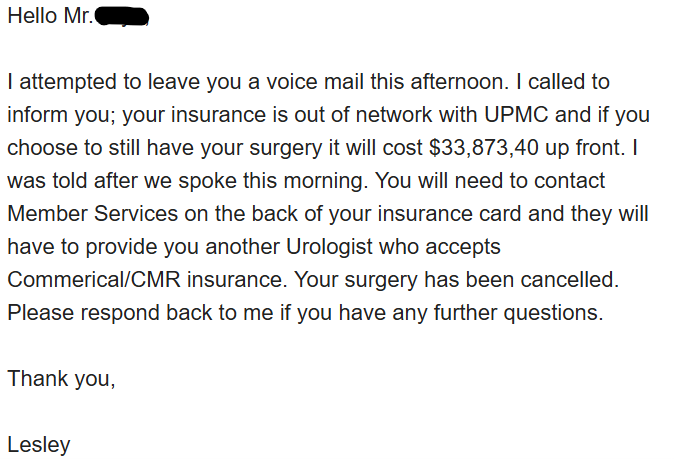
"Your surgery has been cancelled."
That is the exact message UPMC sent directly to a patient via email because his employer runs a self-funded plan that refused to play their PPO pricing games.
They demanded $33,873.40 upfront instead. They thought they could hold his health hostage to force a payout. They picked the wrong plan.
What we did:
1️⃣ Caught them in writing violating IRS 501(r) Extraordinary Collection Action rules
2️⃣ Copied the IRS Tax-Exempt Division and the State AG directly on the thread.
3️⃣ Handed the patient the legal scripts to protect themselves.
UPMC's team never bothered to answer our compliance questions after we copied the PA AG and IRS. Meanwhile, in the background, the patient was quietly routed to another facility. His surgery was successfully completed yesterday.
The employer's capital is protected.
The patient is safe and will not face financial ruin.
The healthcare cartel loses.
It's just execution.
Posted in full with patient's permission.
28
190
1,037
51,012
David B. Stewart, MD, MHA, FACS, FASCRS retweeted

May 21
The IDEAL Macro Breakdown to overhaul body composition:
Protein g = .75 x Bodyweight (in lbs)…yes, this is enough
Fat g = .25 x Bodyweight (in lbs)…yes, your hormones will be fine with this much fat per day
Carb g = Fill in the rest
As alluded to in the header, this is how you want to distribute Macros IF your objective is achieving the best possible outcome as far as body composition enhancement is concerned




May 21

Understood. Any recommendations on Macro %'s?
Currently at 35% protein and carbs and
30% fat.
15
6
189
37,823
David B. Stewart, MD, MHA, FACS, FASCRS retweeted

May 21
Cats aren’t worms. You don’t casually double the lifespan of a mammal.
What we have is evidence of a large 1-year survival benefit in a tiny group of cats already suffering from advanced kidney disease. The 30-year claim is based on nothing.
It's still exciting but for a different reason. The comparative biology angle is more interesting: cats may have a species-specific AIM vulnerability that makes kidney failure a major lifespan bottleneck and fixing that could matter a lot. But “doubling lifespan” is doing far more work than the data support.
May 20

Scientists in Japan have developed a groundbreaking treatment that could double the average lifespan of cats, extending it from around 15 years to nearly 30 years.
The key lies in a protein called AIM (Apoptosis Inhibitor of Macrophage), discovered by Dr. Toru Miyazaki. While cats naturally produce AIM, they lack the ability to activate it effectively. This deficiency leads to the gradual buildup of waste in the kidneys, the leading cause of death in domestic cats.
Dr. Miyazaki’s team created an injectable form of activated AIM that directly restores the kidneys’ natural cleaning function. In clinical trials, cats with advanced kidney disease showed dramatic improvement after treatment. The therapy works both as a preventive measure for healthy cats and as a treatment for those already ill.
If approved, the treatment could revolutionize feline healthcare. Commercial rollout is expected to begin in Japan as early as 2025, with wider availability projected for 2027.
The research has also sparked interest for its potential applications in human medicine, as the AIM protein plays a similar waste-clearing role across species.
1
3
37
4,763
David B. Stewart, MD, MHA, FACS, FASCRS retweeted
This is the problem with socialism.
The answer is always more money. Never a number. Never a limit. Never a point where voters are allowed to ask, after we spent all this, why are the results still mediocre?
NYC Public Schools is already running a roughly $44.6 billion budget. Depending on how you count the all in costs, that puts spending in the neighborhood of $40,000 plus per student.
That's more than most private schools charge. So what's the amount of money per pupil that will make New York public schools adequate? How much wealth should be redistributed to those Queens teachers to make the system "fair?"
We see this in healthcare, too. Any potential cut to Medicaid is dooming poor people to die. @SenSchumer claimed over 50,000 people were going to die if we made even the slightest cut to Medicaid. Fine. Then say the quiet part out loud.
What is the target spend per Medicaid enrollee? What happens when spending rises and patients still cannot get care?
Let's get those numbers out there, find a way to fairly tax the wealthy to fund the safety-net, and then be done with it. $50k per student per year? $10,000 per Medicaid beneficiary with some age-adjustment? $200,000 per mile of high speed rail track?
They can never tell you.
One, because they have never run a business before, so they have no idea how to actually look at a balance sheet.
But, two, they don't want the money to go to the teachers, students, patients, or choo choo train. They want wealth redistributed from class enemies like Bezos to their political allies. They want to fund things that sound nice. "Free childcare" "Free diapers" "Free Faith Healers" so they can take money from people they don't like and give it to people they do like.
But, again because they have never run an actual business and because their only motiviation is to just not fail badly enough to prevent their re-election, the services come in way over budget and under-quality. They're spending other people's money on other people, and as Milton Friedman points out, that's when you stop caring about both price and quality. So the people to whom they promised free stuff look at their free stuff and are disappointed.
"I was supposed to get healthcare but now I need to wait a year for my knee replacement."
So they blame their class enemies and say "well it would work if we could just take MORE of their money and redistribute it."
So they take more money, but the quality doesn't improve. Their political allies, the union bosses and NGO CEOs get big paychecks they then funnel back into their campaigns.
And again, and again. Until all the people who actually produce wealth have been taxed into oblivion. You have no more Amazon. No more abundance. Just bread lines and poverty.
And that teacher in Queens still isn't getting paid what they are worth.

I know a few teachers in Queens who would beg to differ.
52
177
1,142
71,566
David B. Stewart, MD, MHA, FACS, FASCRS retweeted

May 21
Toru Miyazaki gave 11 cats with advanced kidney disease an experimental injection. 15 others didn’t get it. A year later, 9 of the 11 treated cats were alive. Only 3 of the 15 untreated cats survived. He just filed for approval, and the drug fixes a defect only cats have.
Most cats die from one thing: their kidneys fail. By age 10, 4 in 10 cats already have chronic kidney disease, and by age 15, the rate doubles to 8 in 10. Once diagnosed, a cat has about 2 years left.
The reason kidney disease hits cats so hard is a broken protein in their blood. All mammals carry a protein that helps the kidneys clean out waste. In humans and dogs, the protein floats freely and goes to work when the kidneys are in trouble. In cats, it stays stuck to another protein and can’t get loose. So the waste piles up, and the kidneys eventually give out.
Miyazaki originally found the protein in 1999, back when he was at the University of Tokyo. He figured out the cat-specific glitch in 2015. The paper he published in the Veterinary Journal in February laid out the trial. The injection is a working version of the missing protein. His company, the Institute for AIM Medicine, filed the approval paperwork with Japan’s Ministry of Agriculture on April 24, 2026. If the review clears, the drug goes on sale in spring 2027.
The 30-year lifespan figure in the tweet is Miyazaki’s own projection of what cats could reach without kidney disease. The trial only ran a year, and the average cat today lives 15. Most die from the same disease this injection treats.
The research almost died in 2020. After running out of funding during COVID, Miyazaki went public. Cat owners across Japan responded by sending in 300 million yen, around 2 million dollars total. He resigned from the University of Tokyo and worked on the drug full time. The treatment in front of regulators today exists because cat lovers refused to let the research die.
May 20

An injection that can double a cat’s lifespan to 30 years has been developed
Clinical trials have begun, with regulatory approval projected in 2027


Community note
The vaccine addresses kidney disease, the primary cause of death in elder cats. While this would increase the average lifespan of cats by an unknown amount, the claim that it "can double a cat's lifespan" is unverified.
u-tokyo.ac.jp/focus/en/featu… greycoatresearch.com/blogs/news/cat…
238
7,022
49,549
3,592,308
David B. Stewart, MD, MHA, FACS, FASCRS retweeted

May 19
The main reason I quit academia and gave up a tenured faculty position at @EastCarolina was because I caught a student red-handed plagiarism a term paper. Failed them.
But administration forced me to change their grade and I was threatened with a lawsuit by the parents 1/2
May 18

I have a senior on my roster who hasn’t attended my class a single day this semester. She showed up today for the first time.
We have 7 days left before grades are finalized for seniors.
My administrator just asked me to see what I can do to help her graduate.
In case anyone here is a new follower, this is why I’m leaving public education.
79
269
7,126
1,907,781
David B. Stewart, MD, MHA, FACS, FASCRS retweeted

I'm an obesity medicine physician. If I could change one thing about my patients' health, it wouldn't be their weight.
It would be this. 🧵
3
8
51
9,359

Super Mario is named after real-life businessman Mario Segale, who was renting out a warehouse to Nintendo.
After Nintendo fell far behind on rent, Segale did not evict them but gave them a second chance to come up with the money.
Nintendo succeeded and named their main character after him.
9
93
1,112
29,695
David B. Stewart, MD, MHA, FACS, FASCRS retweeted

May 13
"Harvard-trained" sounds really good, because of the prestige of the university. It is not an argument for or against anything.
Here are a non-exhaustive list of retracted scientists who affiliated with Harvard:
/1
3
6
26
3,036
David B. Stewart, MD, MHA, FACS, FASCRS retweeted

May 13
the greatest harm of mandated quality improvement metrics is the crowding out of actual quality improvement
instead of improving what matters, hospitals have legions of staff and resources directed to optimizing quality measures that have no evidentiary basis for improving health
SEP-1 is a great example
We should not be chasing and treating lactates in sepsis, especially for the many people with SIRS who get billed as sepsis but never had such physiology to begin with
5
4
24
2,780
David B. Stewart, MD, MHA, FACS, FASCRS retweeted

Blue Cross continues to want a 6 month renewal form to support anti-obesity drugs that require filling out a 13 page form with incessant details that take 30 minutes to complete, have no evidence based credibility to many of them, a 3 week turn around at times for approval, and lead to numerous drug interruptions. It seems criminal?
8
5
31
3,325