
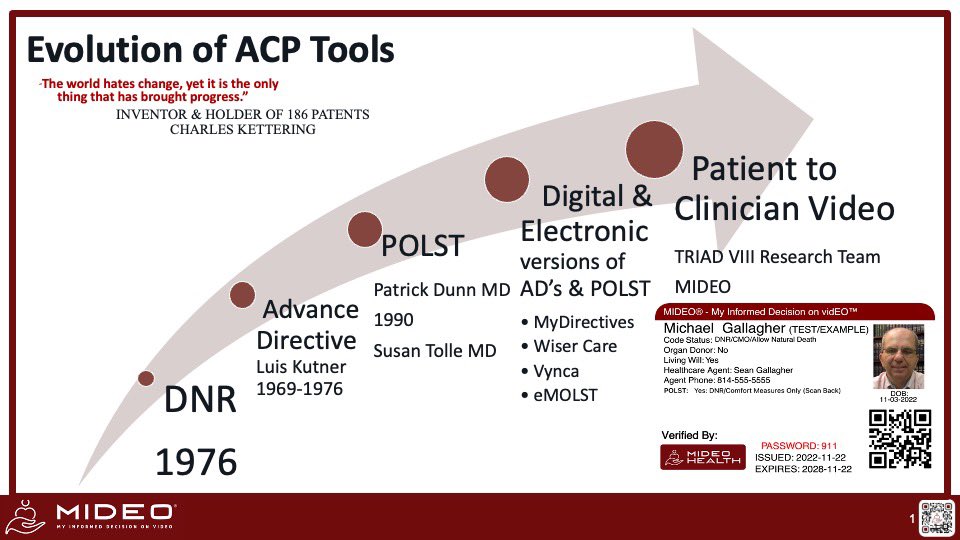
It is not just about End-of-Life. It is about safely getting it right for each patient. Founder of MIDEO (My Informed Decision on Video).
Joined March 2013
- Tweets 4,467
- Following 382
- Followers 630
- Likes 10,895
142 Photos and videos







Pinned Tweet

11 May 2022
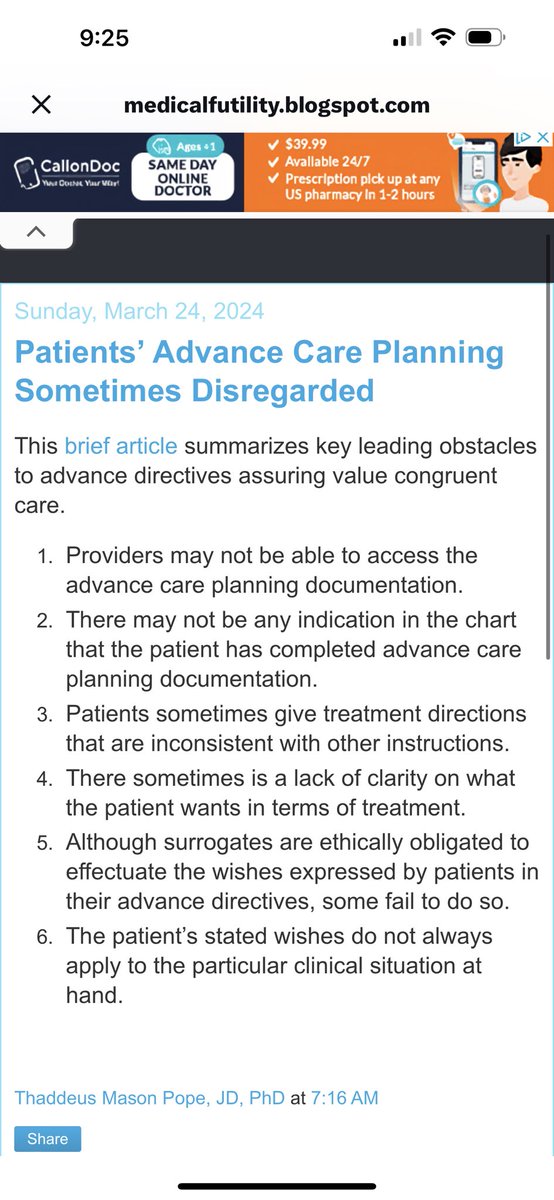
Med-mal re Living wills, DNR & POLST R up. If Ur a #Physician U need 2 wake up. If you #Hospital U need 2 take action. If your a #Payer, then Ur paying for these medical errors & suffering from the Increased Costs as well. Embrace tech & safeguards jems.com/patient-care/family…
1
2
19
Fred Mirarchi retweeted

The influencer telling you to distrust your doctor has no liability if they are wrong.
Your physician does.
That asymmetry matters. It should factor into who you listen to.
390
257
1,600
66,496
May 21
In medicine we are backwards
We wait for symptoms
By then it’s to late
May 20

If you make more than $200k a year get an angiocardiogram before age 40.
I know 3 people under 45 with significant blockages.
All three healthy, good diets, exercise often.
2
167
May 18
It’s not only in big academic medical centers. Happens everywhere.
And that DNR/DNI is often just the misinterpretation of a living will.
If you don’t offer surgery early, then don’t bother consulting them. The patient does not get healthier.

There's a pattern playing out in academic medical centers.
Cardiac surgery isn't being called as a therapy.
It's being called as a last resort.
A patient comes in with endocarditis. DNR. DNI. Medical service admits them.
A week goes by. They throw an embolus. The toe turns blue. The infection isn't clearing.
And then someone says:
"If you don't have an operation, you're going to die."
And now the patient says yes.
"You've been in the hospital for 10 days, you were DNR DNI, and now you're going to have a double valve with a reconstruction of the aortomitral curtain."
Wait a second.
This isn't a heart team decision.
This is what happens when surgery is treated as a disposition for the sickest, most terminal patients — instead of a viable therapy offered early enough to actually matter.
50
May 7
Conflict with organ donation was my #1 medical ethics consult. It’s an area that requires better informed Decision making. Esp in that it is a binding decision and most have a lack of understanding as to what they consent to. We have had many place this decision in their MIDEO with permissions controlled by the appointed decision maker. x.com/GeriPalBlog/status/205…
1
2
43
Fred Mirarchi retweeted
May 6
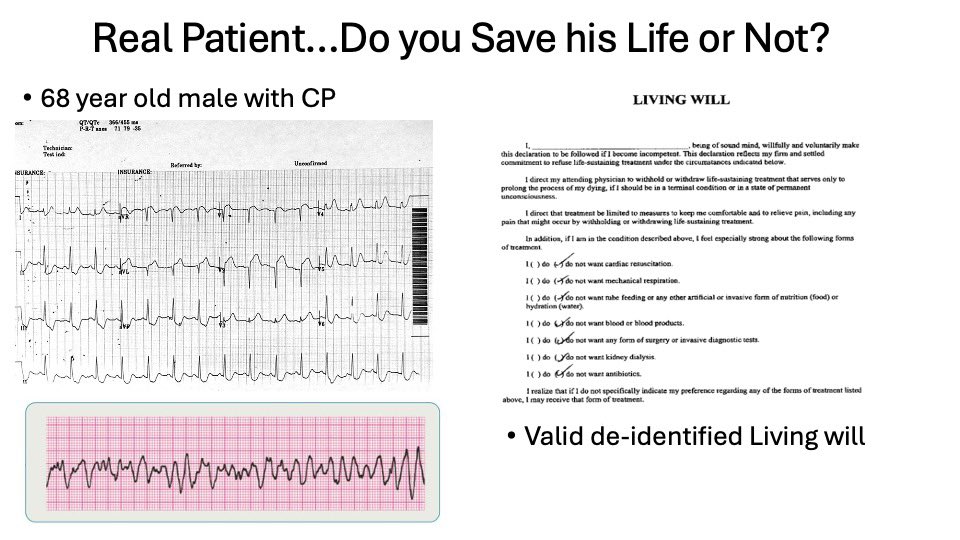
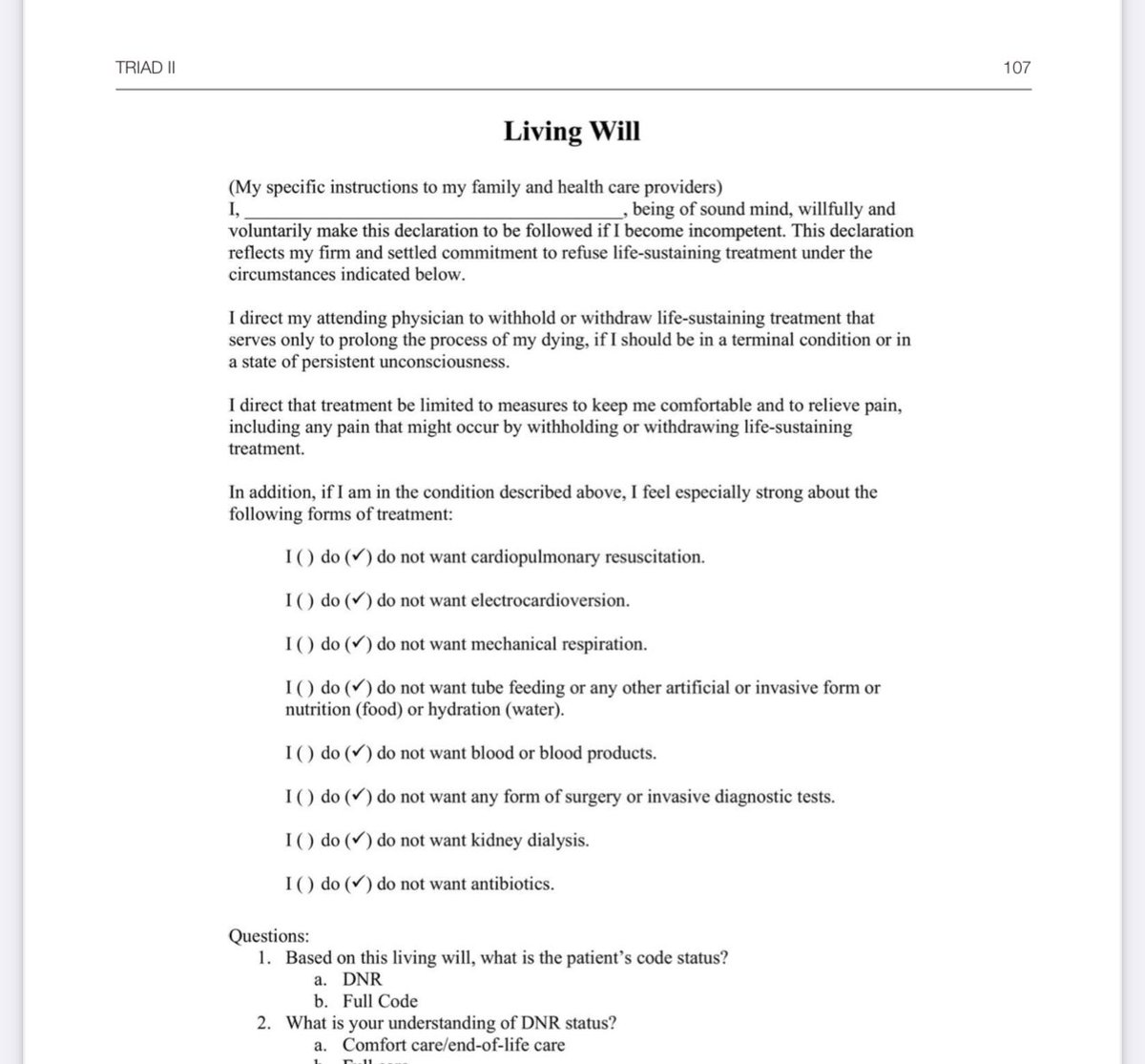
Now imagine if this person had a living will? Would he have been resuscitated? It would literally be a coin toss. We need to stop discouraging CPR so broadly & really make recommendations as far as when it would or would not be successful.
@joerogan
#Resuscitation #cpr

During a CPR lesson at a college in Wisconsin, EMS instructor Karl Arps suddenly went into cardiac arrest. His students noticed the signs and jumped into action, performing CPR and applying an AED to save his life. @DavidMuir reports on the act of heroism. abcnews.link/IbNMzpq
2
2
105
May 6
Kind & genuine people do exist. Just retired as well. RIP.
Nicely done @notthefakeSVP

79
Fred Mirarchi retweeted

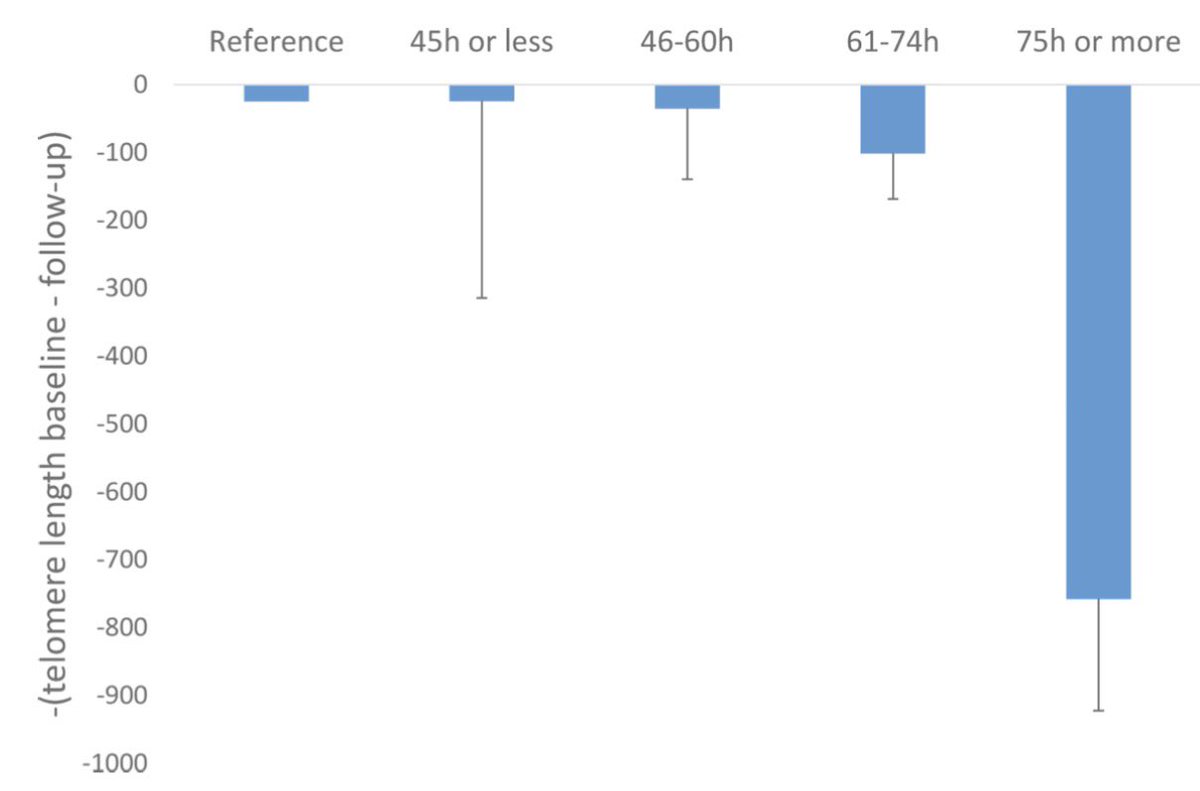
🚨 SER MÉDICO PUEDE ENVEJECERTE 6 VECES MÁS RÁPIDO
Durante la residencia:
• −143 pares de bases en telómeros en 1 año
• ≈6x más envejecimiento celular del normal
• Más horas trabajadas = más acortamiento
💡 No es solo burnout: es daño biológico
69
924
3,676
525,615
Fred Mirarchi retweeted

Maintenance of Certification Controversy - The Impact of the Grandfather Clause
When the American Board of Medical Specialties introduced Maintenance of Certification requirements in 2000, it faced an immediate question: which physicians needed ongoing recertification most urgently? The answer, under any honest patient safety rationale, was obvious. The physicians most likely to be practicing outside current clinical standards were those whose training was farthest removed from contemporary evidence-based medicine. These were the senior physicians who had completed residency in the 1960s and 1970s and whose foundational medical education predated three decades of pharmacological, surgical, and diagnostic transformation. If the purpose of ongoing recertification was patient protection, those were the physicians the program should have reached first.
ABMS grandfathered them entirely. Physicians who had obtained initial board certification before 1990 received permanent, non-expiring credentials with no ongoing recertification obligation. The mandatory commercial program was built around the physicians who had trained most recently. These were the physicians whose knowledge base was most current, who had just completed ACGME-accredited residencies and passed rigorous initial certification examinations. The patient protection rationale, applied honestly, demanded the opposite. The grandfathering decision at launch tells you what the program was actually designed to do.
That decision was not corrected as the program matured. It was institutionalized. The American Medical Association, which founded ABMS in 1933 and retains a delegate vote in the ABMS General Assembly today, has codified grandfathering as permanent policy in H-275.924 Principle 23, which explicitly states that physicians with lifetime board certification should not be required to seek recertification. The organization that built ABMS defends it against every reform effort and owns the AMA PRA Category 1 Credit designation that ABMS member boards require physicians to fulfill as their mandatory CME standard. It has officially and permanently protected the cohort of physicians the patient protection argument would most urgently cover. That means this is not about legacy protections but instead an institutional commitment to an arrangement that has never been about patient safety.
The National Board of Physicians and Surgeons, the organization the AMA has disqualified from recognition, explicitly prohibits grandfathering. NBPAS holds every physician who seeks its certification to the same 24-month CME documentation requirement regardless of when they trained, how long they have been in practice, or what year they completed residency. The Practical Neurology summary of NBPAS's Joint Commission recognition states this directly: NBPAS prohibits the discriminatory practice of grandfathering, which gives lifetime elite status without recertification requirements to a significant portion of US physicians. The organization the AMA has disqualified using patient protection language is the only certifying body in the country that applies the patient protection rationale without exception. The organization the AMA protects exempts the physicians the patient protection rationale would most urgently cover.
This is the efficient demolition of the ABMS patient safety argument, and it requires only the structural choices ABMS and the AMA made themselves. It needs no external critique. The grandfathering decision at launch, the AMA's codification of it as permanent policy, and NBPAS's explicit prohibition of it together establish that the mandatory commercial recertification program was designed to extract fees from new entrants while protecting incumbents. It was not designed to ensure that the physicians treating patients today are current in their specialty knowledge.
On April 30, 2026, the Department of Justice and the Federal Trade Commission issued a joint letter to the Tennessee Supreme Court describing the American Bar Association's exclusive accreditation authority over law schools as a monopoly. The letter documented that the ABA's governance is dominated by parties with financial interests in limiting competition, that its standards exceed any defensible baseline, and that its history includes documented antitrust violations. The ABMS has a concerning similarity to that description. Paul Teirstein, MD, the cardiologist who founded NBPAS, described the ABMS precisely in a Wall Street Journal op-ed published October 19, 2025: a private nonprofit entity that operates like a regulator, controlling a credential held by nearly 95 percent of practicing physicians, required by most hospitals and insurers as a condition of employment, with no accountability to the physicians or patients it claims to serve. The combined net balance of all 24 ABMS member boards, which are all 501(c)3 nonprofits, grew from $237 million in 2004 to $642 million in 2014. The American Board of Internal Medicine alone reported $90 million in revenue in fiscal year 2023, with its President and CEO receiving $1,385,563 that year and $7 million over the preceding six years.
The program was embedded into the Affordable Care Act (ACA) through federal lobbying while ABMS was simultaneously lobbying Congress on its own behalf. You might ask how the ACA codified ABMS certification. The ACA wrote a statutory definition of maintenance of certification that matched the ABMS program, then CMS attached a Medicare bonus payment through PQRS quality reporting of ABMS participation on top of that statutory definition. The taxpayer-funded bonus flowed exclusively to ABMS-certified physicians participating in ABMS MOC. The DOJ and FTC just drew the legal and policy map for challenging exactly that kind of structure. This week I am making the case for reform.
5
17
42
4,487
Fred Mirarchi retweeted

Apr 28
When your practice spends $4 million a year on insurance, $1.8 million of it never pays a claim.
That's the design.
Between 30 and 45 cents of every premium dollar never meets a claim.
That's not a theory.
That's expense ratios plus underwriting margin.
It pays overhead.
Pays commissions.
Sits in surplus.
Gets invested.
Compounds.
For someone.
Just not for you.
This is not a scandal.
The carriers are doing exactly what the model rewards them to do.
The only question worth asking:
Do you want to keep being the customer, or do you want to operate the model?
The independent practice of medicine delivers higher-quality outcomes at lower prices.
I want independent practice of medicine to be the preferred method for all physicians.
This is the way...
8
12
70
3,853
Fred Mirarchi retweeted

Apr 25
Bill Maher asks how the government is “failing the poor so badly” when he pays “60 PERCENT” of his earnings in taxes.
“Last week was tax day… I paid the government probably almost 60% of what I earn. That’s a lot.”
“And I… wouldn’t mind if Bernie Sanders would stop saying the rich don’t pay taxes.”
“The top 10% pay 72% of all federal income taxes. And the bottom half, 3%.”
“The Democratic Socialists talk about socialism like we don’t already have a lot: Social Security, unemployment, Medicare, nutritional assistance, Medicaid, Obamacare, disability, housing subsidies.”
“How can you be soaking the rich and failing the poor so badly? How can it be that the federal government alone took in over 5 trillion in taxes last year, and we still need that?”
“Are we really this incompetent and corrupt?”
3,674
19,855
100,635
3,878,062
Fred Mirarchi retweeted
Apr 21
Don’t forget merit badge courses for CPR/ACLS/ATLS that are required by those physicians who do that work every day.
Lots of hours and lots of hours of lost revenue
1
2
17
1,061
Apr 22
Just another way physicians get forced to pay for state government programs. Renewed my OH medical license and had to pay a mandatory Physician student loan repayment fee. @DutchRojas @DrDiGiorgio
Wasn’t much but still, why?
2
35
Fred Mirarchi retweeted

Apr 18
Truth NUKE: Calley Means: “There’s nothing more expensive than the mental health crisis in America. 21% of Americans have a diagnosable mental health condition. The second leading cause of death for young adults today is su*cide. Antidepressants right now are the most prescribed class of medications in the country. Over 20% of women are on an antidepressant.”
“There’s highly problematic research that women are on these drugs that are prescribed for life.”
25
213
1,178
48,403
Fred Mirarchi retweeted

just a reminder about this study — do you know what was the most effective intervention to help prevent a patient from developing delirium?
the presence of a loved one at the bedside.
Apr 16

💬 Editorial: Routine physical restraints in mechanically ventilated ICU patients did not alter delirium, self-extubation, or mortality rates; individualized assessment is imperative in #CriticalCare.
ja.ma/4tLow9f

6
17
70
4,038
Fred Mirarchi retweeted

Apr 16
Warning shot for all the school districts out there with bloated administratuons that cant find money in the budget to pay for a full time AT. If you're going to have interscholastic sports on campus, an AT is non-negotiable.
nbcboston.com/news/local/par…
7
29
92
18,578
Fred Mirarchi retweeted

Apr 14
Pancreatic cancer explosion: Father-of-three brushed off digestive discomfort as simple indigestion - but it was an early sign of deadly disease that's on the rise in younger adults | Daily Mail Online dailymail.co.uk/health/artic…
1
2
247
Fred Mirarchi retweeted
Apr 12
Everyone thinks Stark Law prevents corruption.
It does not.
It prevents independent physicians from operating integrated clinical delivery models.
Hospital-employed physicians face no such constraint.
The law does not ban self-referral.
It bans self-referral by the wrong kind of physician…
15
58
362
40,039
Fred Mirarchi retweeted

Apr 10
Dad with stage 4 cancer dies after insurance company said tumor-shrinking treatment was 'not medically necessary' trib.al/aYAtuEv

988
2,150
12,482
8,522,954
Apr 10
RT @YounisJoseph: Ok, looks like some non doctors got triggered. Let’s try this another way?
Neurosurgeon: $251 an hour
Master Electricia…
90