
Health inequalities researcher @UofGlasgow. Systems science, economic determinants, place-based policy. Leading OPTIMA project. Views my own
Joined May 2012
- Tweets 2,040
- Following 877
- Followers 886
- Likes 3,128
Photos and videos
Pinned Tweet

Apr 22
Some communities have everything they need on their doorstep. Others have almost nothing.
We built a dashboard to make that visible, linking service provision and health needs at neighbourhood level across Great Britain.
Explore your neighbourhood 👇
🔗 optima-dashboard.org/
1
53
Jun 5
Everyone's framing NHS records as "data sharing vs privacy". I think that misses the point.
The real question is who gets the value: patients and public services, or tech firms building products on public trust?
That feels like governance, not comms. What do you reckon?
26
Jun 4
'Health in all policies' is useless unless it also means accountability in all policies. Otherwise it's just asking the NHS to be nicer about absorbing the damage. Too blunt?
1
1
23
Jun 1
The more I work on 20-minute neighbourhoods, the less I believe proximity is the point.
A GP, park or shop nearby only matters if people can actually use it, afford it, and feel it's for them. Equity is in the mechanism, not the map. What do you reckon?
16
May 15
The new @Spotify agent integration is awesome! I've wired mine into a daily paper-briefing: agent picks a paper from my Notion queue, drafts a personalised researcher-grade script, runs it through text-to-speech, and uploads to a personal podcast I listen to on the nursery run 🎶
1
46
May 8
Everyone's reading today's local election map as party drama. Fine. But councils are where buses, housing, air quality, leisure and public health budgets actually live. If prevention is local, why do we still talk about it like Westminster theatre or NHS responsibility?
1
50
Apr 29
We keep asking the NHS to fix what housing, transport, wages and planning keep breaking. Then we call prevention difficult. It isn't difficult; it's inconvenient because the levers sit outside the health system.
1
30
Apr 27
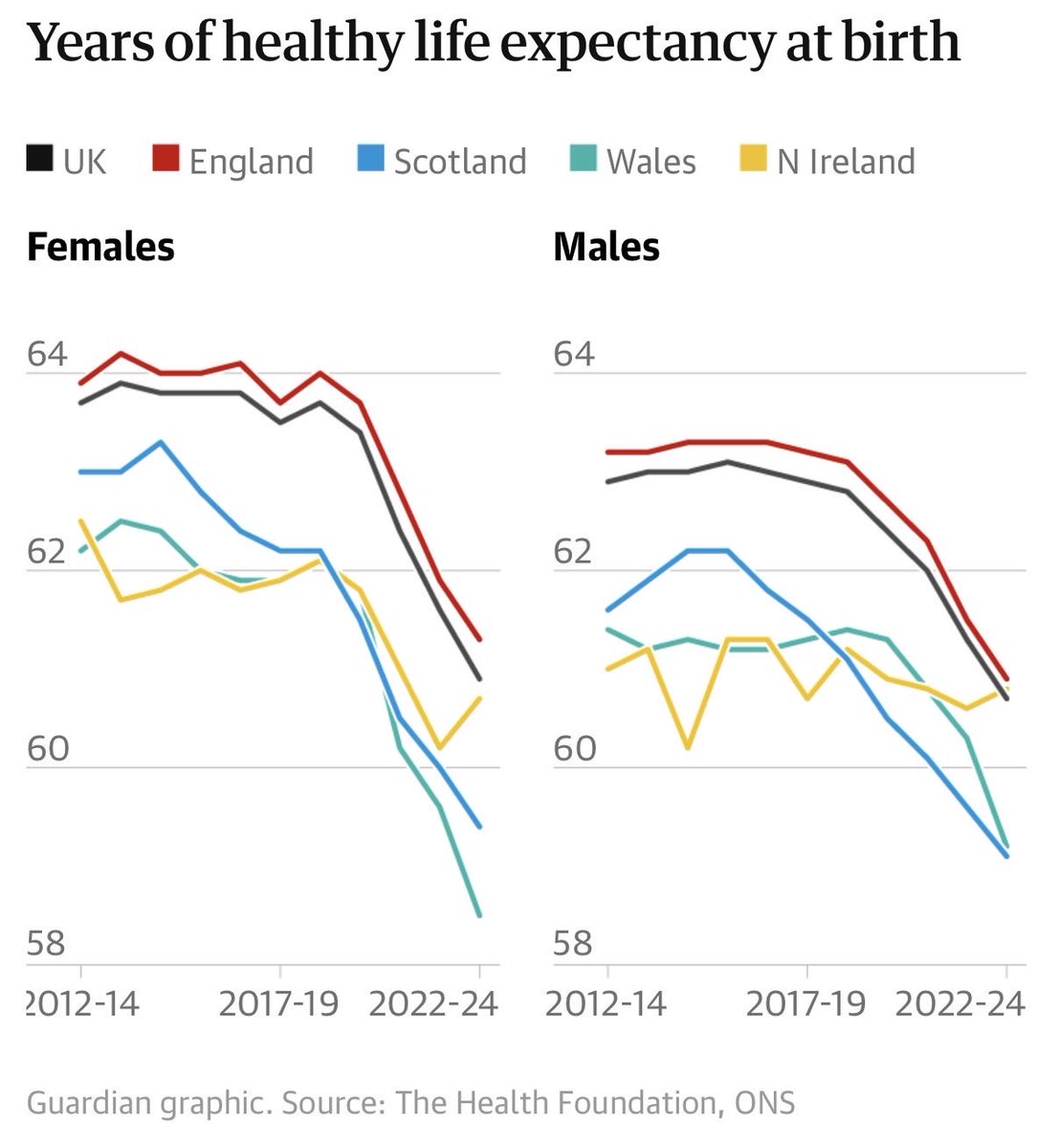
“Ministers should force food firms to make their products healthier, introduce minimum unit pricing of alcohol in England, as Scotland has done, and tackle drug-related harm, Dixon urged.” - seems strange to use Scotland as exemplar here. Gap widening theguardian.com/society/2026…
31
Apr 21
A lot of policy "evaluation" is, unfortunately, just politely documenting damage after the big decisions are already locked in. If public health only turns up once implementation starts, it’s not upstream, it’s clean-up. Too harsh?
1
40
Apr 20
If your prevention strategy can be delivered entirely by the NHS, it probably isn’t prevention. It’s earlier treatment with better branding. Prevention lives in things like income, housing, transport and work. What am I missing?
33

Using OpenClaw is basically is like driving your own Ferrari (that you have to be a mechanic for yourself) and it's broken down all the time, but gives you the time of your life
vs driving a reliable Honda (Hermes Agent)
vs riding the bus (Claude / ChatGPT)
432
244
3,336
244,111
Apr 17
5) The boring admin stuff too: help with formatting of papers for different journals, pulling citation data, compiling papers for evidence summaries. The kind of work that used to eat entire afternoons
1
23
Apr 17
6) The flexible model selection and cron job automation is where it really shines. Things running in the background 24/7 that still no other tool can quite do right now. Outstanding when used alongside @AnthropicAI Claude Code, a tool @causalinf and others have been highlighting
1
29
Apr 15
Welcome move. But as someone who works on health inequalities — the gap between "closer to home" and "reaching the people who need it most" is where most policies quietly fail. Would love to see the access data by deprivation/other inequality indicators once these are live.

We're investing in 36 new and improved Community Diagnostic Centres.
This means patients can get tests, checks and scans closer to home - without having to travel across town to a hospital.
We're building a new, modern NHS, fit for the future.
Read more: gov.uk/government/news/nhs-p…
53
Apr 14
If every bit of public spending is being judged on growth, public health needs to get much better at making the equity case in those terms too. Prevention isn’t a nice add-on, it’s economic policy. What do you reckon?
33
Apr 8
I’m broadly sympathetic to this, but proximity isn’t the same as equity. The real test is whether neighbourhood models reach the people with the worst access, not whether services have simply moved location.
🏘️ We're bringing the NHS closer to home and making it work around the lives of patients.
The first 27 Neighbourhood Health Centres will be one-stop shops for care in ordinary, hard-working communities.
Part of our 10 Year Health Plan.
Find out more: gov.uk/government/news/commu…
44