
Finding hidden value in under-followed companies. Posts are not advice. Do your own due diligence.
Joined July 2016
- Tweets 17,007
- Following 244
- Followers 8,723
- Likes 48,744
622 Photos and videos





Pinned Tweet

Jun 8
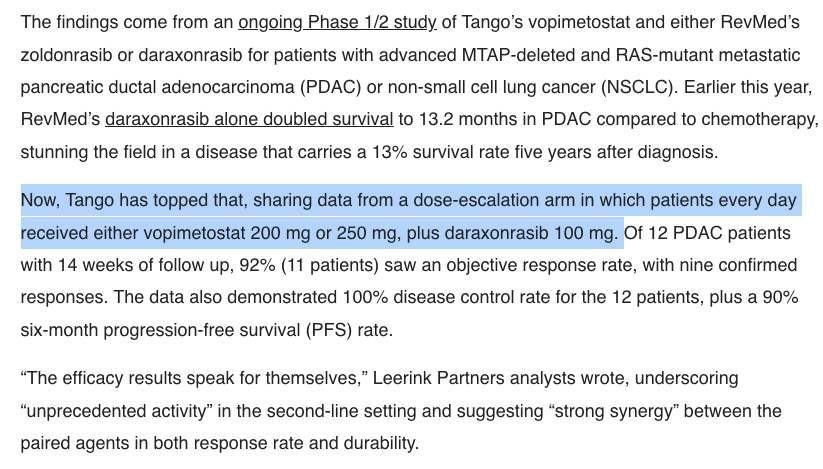
Most stunning: $RVMD daraxonrasib 3L mono showed 32% ORR, and $TNGX PRMT5 drug showed ~25% mono ORR in 3L—yet the combo in 2L/3L delivered 92% ORR, with synergy and potentially better safety than dara alone. Wonde how long it takes for resistance mechanisms to be blocked as well?

1
5
2,126
Jordan Alexander retweeted
$qure $clpt
I think what is interesting is if you cross reference Sung’s interview in December 2025 he said
“so all my patients had surgery almost 4 years ago”
“Sung: Yes. I’ve been the site PI here at UAB, and we had seven patients in the trial. We have one patient in the fourth cohort, which has just completed, but in the second and third cohorts where we had the data readout in September, we had seven of those patients. One of our patients was a sham-treated patient and then six of them were treated with high dose AMT-130.”
So December 25, a large percentage of the 6 were almost at 4 years, so technically he likely is speaking on 6 that could be around 4.5 years and 1 patient at 3 years. He isn’t just speaking on 4 year data here. The longest patient would be at 5 years in the cohort 2 but we don’t know which site had that person.
Today
“The patients Sung treated, all in the early stages of Huntington disease, have now been followed for more than 4 years.”
1
3
26
2,386
Jordan Alexander retweeted

Jun 15
$qure $clpt
Hell yeah SUNG, he just said this drug works
The patients Sung treated, all in the early stages of Huntington disease, have now been followed for more than 4 years.
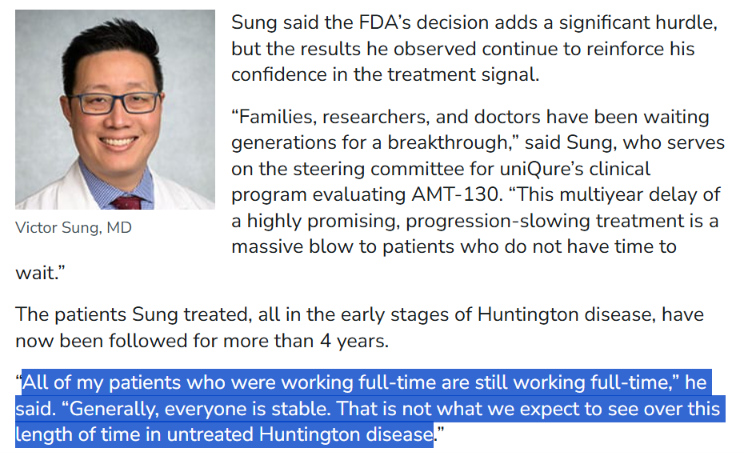
“All of my patients who were working full-time are still working full-time,” he said. “Generally, everyone is stable. That is not what we expect to see over this length of time in untreated Huntington disease.”
Victor Sung, MD, director of the Huntington’s Disease Clinic at the University of Alabama at Birmingham and a principal investigator in the trial, treated seven participants: Six received the high-dose infusion, and one initially had the sham procedure and later received AMT-130.
Sung said the FDA’s decision adds a significant hurdle, but the results he observed continue to reinforce his confidence in the treatment signal
“Families, researchers, and doctors have been waiting generations for a breakthrough,” said Sung, who serves on the steering committee for uniQure’s clinical program evaluating AMT-130. “This multiyear delay of a highly promising, progression-slowing treatment is a massive blow to patients who do not have time to wait.”
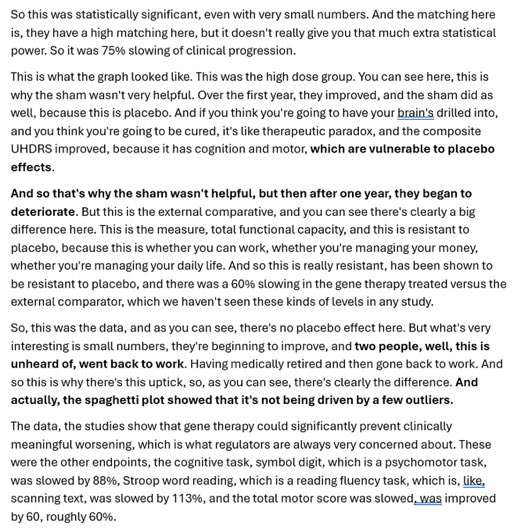
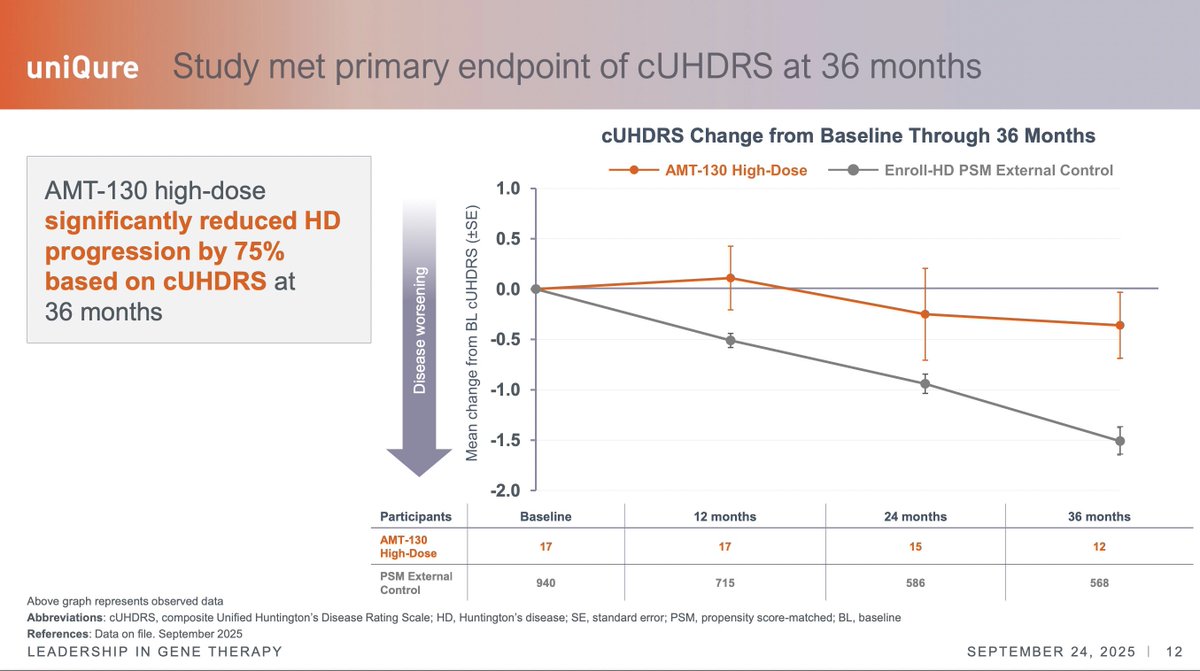
Sung described the treated group’s course as striking even without focusing on the 75% figure or the external comparator. The progression over 3 years, he said, was “closer to zero than it is to one point of progression.”
“We provided MHRA with the 3-year follow-up results,” Kapusta said. “They encouraged us to include those results as part of an application for a license.”
Sung said the possibility of approval outside the US raises difficult questions for patients and families, including whether some might travel for treatment if AMT-130 becomes available elsewhere first. Because the therapy requires specialized neurosurgical delivery and intraoperative MRI, broad access would take time even if it were approved.
“This is not going to go like wildfire,” Sung said. “It will go very slow because of the invasiveness of the procedure.”
Even with those constraints, Sung said, the patient community’s response to the FDA decision has been clear. “If I could summarize their stance, it has been ‘let us be the arbiter of our own risk tolerance,’” he said.
“I was literally riding a roller coaster when I found out that the trial data had been rejected,” he said. “There is something symbolic in that.”
@peter_mantas @Tim_Corr @biggercapital @Prof_Dollar @DesertDweller93 @laurencurehd @Christina4HD
medscape.com/viewarticle/hun…
7
26
95
16,364
Jordan Alexander retweeted

Must be the dreaded placebo effect, NOT!!!
How can anyone disagree that @uniQure_NV $QURE AMT130 should get approval to file BLA? This is criminal.
Mike, you are the best, uncovering all these articles and evidence to support my belief that the FDA will realign shortly.
1
4
35
5,356
Jordan Alexander retweeted
Jun 12
$qure $clpt
Tabrizi at UCL
“Professor Sarah Tabrizi gave us a thrilling story - her groundbreaking work on targeting the gene that causes Huntington’s disease. This devastating inherited condition is often described as a combination of Alzheimer’s, schizophrenia, and Parkinson’s and until recently, families blighted by it have had very little hope of a cure being found. Now Professor Tabrizi’s work on gene therapy has shown that the brakes can be put on the progression of Huntington’s and she even held out the prospect of a treatment that could be given to people with the rogue gene twenty years before the onset of the disease and prevent it from ever occurring.”
rorycellanjones.substack.com…
2
2
35
2,722
Jun 11
What happened to all those fools that were saying $AXSM Auvelity was cough syrup combined with a generic drug when the stock was single digits?
doctors would prescibe the generics and mix it.
…now at $256.
There were so many of you. Now everyone is a bull.
2
16
1,356
Jordan Alexander retweeted

Jun 9
An important slide on the PD1xVEGF class from Merck's #ASCO26 event.
It's a limited data set but clearly shows these drugs are unlikely to meaningfully change lung cancer treatment as they don't really work in patients who failed PD1 and/or VEGF agents.
Numbers are small but trends are clear:
➖Of 9 patients who had prior PD1 and VEGF treatments, only 1 had a PR
➖Of 9 patients who had prior VEGF, only 1 had a PR
➖Of 10 responders, 7 were PD1 and VEGF naive
This isn't different than what one would expect with Keytruda or Avastin rechallenge. Also, this study is from China so efficacy in the west may be even worse.

4
6
63
16,227
Jordan Alexander retweeted

Jun 8
Just weeks after RevMed's historic pancreatic cancer results that prompted standing ovations at a conference, a small study is showing even better "unprecedented" results when it's paired with another new drug
biospace.com/drug-developmen…
6
17
152
83,450

$ABVX
STIL here is making another highly relevant point - What he is referring to here is basically the "latency" point. It basically goes like this:
"A cancer signal seen so early is likely not a real cancer signal because cancer doesn't "develop" that fast. What you are actually seeing is "latent" cancer that was there but undetectable at baseline."
This is also why it is important that...they've had >100 patients on the drug for ***5-7 YEARS WITH ZERO CANCERS***. If it was a "super mega carcinogen" you'd now from the extremely long phase 2 study!
How could it be possible that the drug somehow causes cancer in a few weeks after NOT causing it in 5-7 YEARS? The answer is *IT DOESN'T* - what we saw in those 2 cases in the P3 is just statistical NOISE!
I expect sharper minds to look at these facts and come to the same conclusion tomorrow.
Jun 2

Another thing to think about: It was only 44 weeks. If it's a carcinogen, it's a super mega carcinogen.
If they assigned half the trial a pack a day smoking habit and an alkylating agent, we probably wouldnt get 7 *new* measurable cancers by wk44. Its probably noise.
17
12
249
50,297
I keep hearing people referring to "7" cases of cancer in the high dose arm for $ABVX. I get it - that's what they technically showed in the table, but in observing a lot of conversation about this I gather that people don't actually realize what really matters there. I am strongly of the opinion that there are really only 2 malignancy cases that matter for adjudication - the prostate cancer and breast cancer cases.
I initially started talking about these cases as "the 2" cases from the very beginning because I assumed that everyone would be on the same page that these were the only 2 that mattered...but I've found that people really are considering this as a case of *7* full blown malignancies in the 50mg arm...This is just not correct.
Let's break this down.
First of all, they're counting "colonic dysplasia" in this table as one of the "malignancies". I cannot stress this enough: Colonic dysplasia is, by definition, LITERALLY not cancer. This is actually an unequivocal point that I don't understand how it could even be up for debate.
"Dysplasia" is a "precancerous" lesion. Cervical dysplasia, colonic dysplasia, melanocyte dysplasia. Terms exist for these PREcancerous findings because they are, by definition NOT CANCER (otherwise, if they were cancer, we'd call them cervical cancer, colon cancer, and melanoma)...
Dysplastic lesions, not being cancer, often regress on their own or simply never evolve into cancer, staying in the "dysplastic" state until death. However, if they *do* become cancer, they do so through a process that is called "malignant transformation". Literally, something that is NOT malignant TRANSFORMS into something that is.
Why did the ABVX management team include this in the list of "malignancies"? Honestly, I don't know. I think it is an evident mistake, and a strong piece of evidence that they didn't think they'd actually have to explain away a "cancer signal" in this dataset because their analysis of the data told them that there isn't one. If they were worried that the market was going to interpret these data as a catastrophic malignancy risk (which, make no mistake, is what the current low $70s price tag is assuming), they would've likely adjudicated this more thoroughly and left the "malignancy" that is by definition NOT malignancy off of the "malignancy" table...
So that is tossed out easily IMO. 6 cases left now. 4 of those are NMSC (non-melanoma skin cancer). I gather that people are dramatically overestimating what a diagnosis of NMSC means. Far be it from me to minimize NMSC (since it is what I treat for a living as a dermatologist), but guys....this is NOT in the same category as ANY other malignancies. NMSC is a milder category of its own, and I don't mean that as a matter of opinion. Literally, "non-NMSC malignancies" is a distinct endpoint used to gauge risk of "serious" malignancies in clinical trials. NMSCs are left out of that category because they almost never are "serious" - certainly almost never life threatening.
Here's an exercise anyone can do to drive this point home. Google, or ask an LLM "what are the 10 most common cancers in the United States?". They are all going to give you the same answer: Breast & prostate will be the top 2 at slightly >300,000 cases/year.
So breast and prostate are the #1 and #2 most common cancers according to every source...except, those sources either ignore completely or footnote at the bottom that there is a type of cancer 15x more common...NMSC!!!
The point? Ubiquitously, NMSC isn't even included on the list of "most common cancers" because they're frankly in a separate category altogether from cancers like breast and prostate. It actually is controversial whether or not it is even possible for basal cell carcinoma to metastasize, and (aside from transplant patients), CSCC is almost never fatal unless left ignored/untreated for years (people ignoring a giant bleeding skin cancer is perhaps more common than you'd think, but not happening in any clinical trial patients).
These 4 50mg NMSC cases (vs 1 in the placebo group) are a not representative of serious malignancy risk even if the market is acting as if they are...they are absolutely in milder a category all their own, and lumping these all together is a mistake.
Again, if people think these 4 NMSC cases are some scary life threatening event, they're just flat out wrong. There are >15x more cases of NMSC than breast cancer in the US/year, yet >10x more breast cancer deaths occur in the US per year.
Again, not to minimize my own career too greatly, but almost *always* NMSC are removed by VERY simple, ~10 minute procedures under local anesthesia. Cutting out (or scraping away) the lesion typically takes me around 60 seconds, and the bulk of the procedure is actually spent stitching the patient back up. Drive yourself to the office, drive yourself home, local anesthesia, under an hour, you're cured. Hell, in many places in Europe it is actually standard practice to not even "treat" a basal cell carcinoma! On many body locations they are simply biopsied, and once diagnosed they are considered cured by the biopsy itself!
It has become very clear to me that people are thinking that these NMSC cases are highly relevant cases of severe, potentially fatal cancer. They simply are not. There are *millions* of these in the US per year and most are treated with <15 minute procedures. These are in a TOTALLY different, far less serious category of "cancer".
So again, why wasn't $ABVX prepared to discuss/explain this? I legitimately think they did not expect to need to. They may have overestimated the market's knowledge here and underestimated its potential for a knee-jerk reaction to the "C-Word". It's a mistake, yes, but it ultimately doesn't change the profile of the drug.
So, I think we have compelling cases to write off the colonic dysplasia (literally not cancer) and NMSC cases, as I have usually found to be standard in these situations.
That leaves the breast and prostate cancer cases. Again, the otherwise #1 and #2 most common cancer types...funny how that worked out! I sincerely do not believe that these two cases alone represent a signal against 0 in the placebo arm. This is textbook small sample statistical noise, ESPECIALLY for a drug with no mutagenic risk AND no immunosuppression (literally, HOW would this drug even be causing cancer then???).
However, clearly the market will want more info here on these two cases.
Hopefully the market will wake up to the points above (that $ABVX and I mistakenly thought were obvious) highlighting that the colonic dysplasia and NMSC cases can be almost completely written off. After that, hopefully $ABVX can give us more info on these two "legit" cancer cases (breast and prostate).
Yes, they should've been ready to do so on the call. they messed up, but let's see what the details show. Some are saying we will see updates sooner than the October conference like they initially guided for on the call (at which point they clearly did not expect the market to be freaking out at all).
After that, we also need to see the data from the 50mg "escape/placebo" arm that was not part of the primary efficacy analysis. That's is own topic of conversation, but that could significantly rewrite the narrative (now that $ABVX is aware a narrative needs to be rewritten after it got away from them).
I think the market thinks they are hiding these "escape/placebo" arm 50mg patients' data. I believe they were just totally caught off guard by the market's reaction to the "cancer signal" here and didn't think they'd need to have that dataset ready to prove there's no cancer risk (they thought the initial dataset spoke for itself...I agree, but so far the market clearly doesn't).
There should be several hundred patients worth of extra 50mg patients in that group. Ideally they can move up the release of that dataset to help qualm the market's fears and try to prove they aren't trying to hide anything there. Depending on the sample size there, we should very likely expect a few "cases" there too, but if the rate comes in lower than the original 50mg data we got, this narrative could snap back rapidly. Let's hope!
53
29
392
150,509
There are going to be case studies written about this initial $ABVX reaction, and (if we can get it) the subsequent rapid snap back ( 🤞🏻 ).
My HEAVILY BIASED opinion is that if the market comes to its senses and realizes this thing is not getting a black box warning we are going to >$150 in no time.
In reality if the “malignancy overhang” can be completely dispelled, there’s no reason we couldn’t see it go back to the brief initial market reaction of ~$180. Personally I’m already convinced that the malignancy stuff is statistical noise, but let’s see what the company can show the market about these cases and the extra data to convince people. This could’ve been upfront if they were just ready to explain what they already had, but oh well.
Once this black box warning stuff is put to bed, I can’t emphasize enough that the efficacy results here were at a level I literally didn’t even model for. Those endoscopic remission rates in particular are at levels I didn’t even think were possible for a single drug to produce.
With a clean label and a hit in crohn’s (which is now much more likely given the *extreme* efficacy in UC), this is an $8-$10B/year peak sales drug...pick your multiple on that…🤷🏻♂️
Again, I’m heavily biased and there’s no such thing as a guarantee, but this all seems very clear to me already. Unfortunately it’s not my opinion that matters! Let’s see what Mr. Market has in store.
23
16
281
28,951
Jordan Alexander retweeted

Jun 2
$ABVX thoughts:
The Phase 3 maintenance data showed strong efficacy, with results comparable to best-in-class JAK inhibitors.
The market's sell-off has been driven by cancer-related safety concerns. These events were concentrated in the 50 mg arm (n=6), with one case each in the 25 mg arm (n=1) and placebo arm (n=1). Reported malignancies included one prostate cancer, one breast cancer, one case of colonic dysplasia, and four non-melanoma skin cancers (NMSCs).
As others have pointed out, the solid tumors are likely incidental rather than drug-related. The latency is too short, the tumor types are not those typically associated with immunomodulatory therapies, background incidence rates appear plausible, and the dataset includes up to 7 years of exposure alongside a clean DSMB review. That leaves the dose-dependent NMSC imbalance as the only potentially meaningful safety signal.
It's also worth highlighting the 25 mg arm. Despite years of accumulated exposure, there has been no emergence of the major safety signals that ultimately drove boxed warnings across the JAK class. While the dataset is not large enough to conclusively rule out future risk, the evidence at 25 mg remains remarkably clean. If regulators ultimately view the 50 mg findings as dose-related, there is a plausible path where 25 mg becomes the preferred commercial dose, preserving much of the drug's value proposition.
Importantly, NMSCs alone are unlikely to result in a boxed warning. That would be consistent with the broader JAK class, where NMSCs were explicitly excluded from boxed-warning language.
The issue, however, is not necessarily the magnitude of the risk but the change in perception. The drug has gone from having "no safety footprint" to having "some safety footprint." Once that happens, investors no longer need to prove harm; the company needs to prove its absence.
That question cannot be answered by re-analyzing existing data. It likely remains an overhang until the label decision in 2027 and more definitive long term data.
From a valuation perspective, this matters more than the absolute risk itself. The bull case depended on a pristine safety profile justifying a premium to upadacitinib. "Almost clean" does not command the same premium as "clean."
1
5
46
6,214
Jordan Alexander retweeted

May 4
$CNTX data on June TCE targeting claudin 6 ( with high specificity vs other Claudins ) in ovarian ca. Co reported a PR at cohort 3 ( low effective dose ) and low CRS due to gentle use of steroids.
CAR T cell targeting claudin 6 by $BNTX reported high RR .. but toxicity and durability ?
$CNTX referenced possibility of beating 30% RR in heavily pretreated OC including ADC from $ABBV
Data in June. Very interesting set up with CEO benchmarking 30% RR which is much better than 5-10% with standard chemotherapy
May 3

Candid T cell engager ( BCMA -CD3b) was engineered to have reduced CRS. But still phase 1. ? Company claims deep B cell depletion. $UCB is paying $2 B upfront by for phase 1 b
$CNTX is developing TCE for oncology including data in June for Cauldin6 in ovarian cancer
$MGNX Cd123 TCE in partnership with $GILD against AML was also engineered to reduce CRS
1
8
11,762
Jordan Alexander retweeted

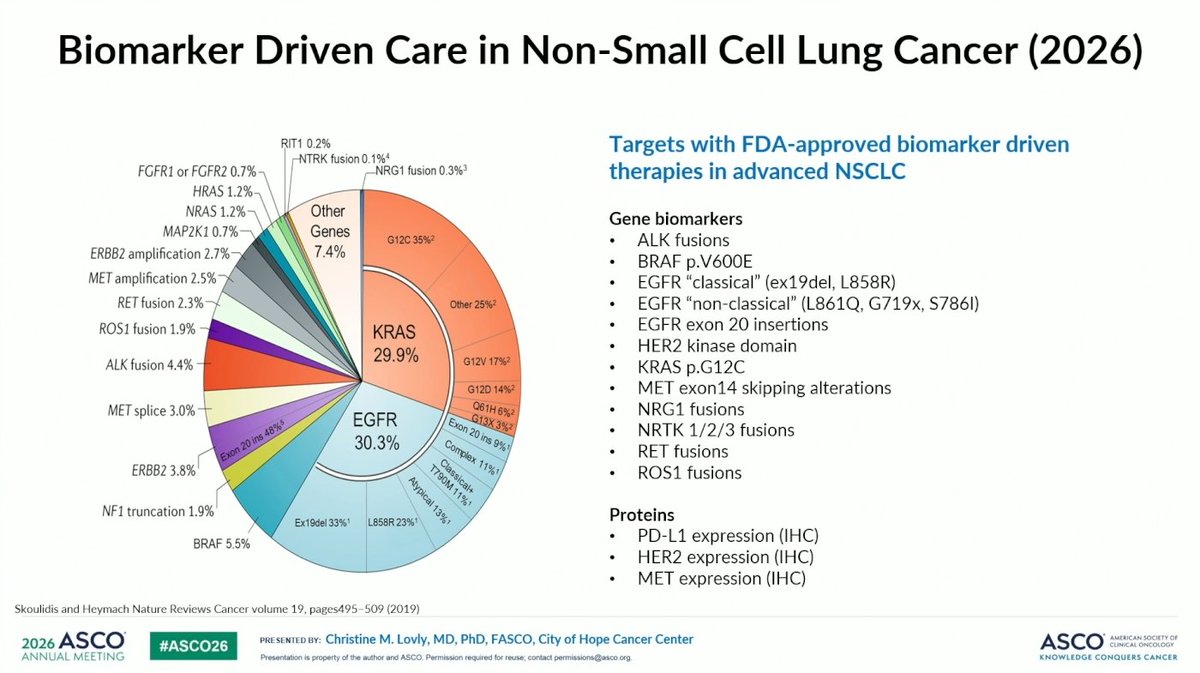
May 31
NSCLC driver mutation prevalence slide from Libretto-432 discussant Christine Lovly #Asco26
8
47
5,109
Jordan Alexander retweeted

May 29
$REPL Gets Third Try at FDA Approval After Makary Departure. cc: $QURE $CLPT wsj.com/health/pharma/replim…
1
2
21
3,298
I've got to complain about $APGE again. You're welcome to take my opinion with a grain of salt since I've disclosed that I am short, but IMO they are spewing absolutely *blatant* bullshit about ISRs (add them to the LLY legal team!).
I heard them in 2 recent calls saying that "the most common reason for discontinuing Dupixent is ISRs". Huh? What?! ISRs are the most common cause of stopping Dupi???
That is absolutely INSANE to me, because I have treated hundreds of patient with Dupixent and LITERALLY NOT EVER (NOT ONCE) HAVE I HAD TO DISCONTINUE A PATIENT'S DUPIXENT BECAUSE OF ISRs. In fact, I've never even had to go as far as giving them advice on how to mitigate ISRs, such as treating the injection site with a cold compress. Literally: Nothing. Ever. In hundreds of patients.
I *have* discontinued patients due to conjunctivitis. If we are talking AEs, the most common causes for discontinuation in *my* experience are
1) Conjunctivitis
2) Facial erythema (some derms believe this to be psoriasis caused by the drug)
***gap***
3) Joint pain (rare)
Again, I can't even rank ISRs on that list at all because *LITERALLY* this has never ever happened with any of my patients.
So, that is *my* clinical experience, which goes directly in the face of what $APGE is claiming. I say that I've literally never even seen it happen, yet $APGE says that ISRs are the literal top cause of dupixent discontinuations...Sure, I'm biased, but so are they.
They want to convince you that conjunctivitis is not a big deal because they've seen higher rates of that side effect than dupixent/ebglyss so far. Instead, they want to create a strawman side effect that they can point at and say...
"Hey, we caused more conjunctivitis so far, but it's actually ISRs that are the problem!"
So, if we are both biased, what can we do to resolve the discrepancy? Look at the actual clinical data! In clinical trials, were patients more likely to discontinue from conjunctivitis, or from ISRs? Let's look at the actual data!
P3 5-year extension trials (n~2700):
-> 14 patients discontinued due to conjunctivitis
-> Zero (?) patients discontinuing due to ISRs? ISR is not even listed as a reason for discontinuation in the publication.
Real world dataset from the Netherlands (n~1300):
-> 38 patients discontinued due to conjunctivitis...the most common cause of AE-related discontinuation in the study *by far*
-> 2nd place for discontinuations was muscle/joint pain
-> Yet again...***ZERO*** cases of discontinuation due to ISR. None. ZERO!
So, $APGE is going out on these roadshows and repeatedly telling everyone that ISRs are literally the single most common cause of dupixent discontinuation, yet with only a few minutes of research you can get to a sample size of ~4,000 patients treated with dupixent for multiple years showing DOZENS of cases of discontinuation due to ISRs and LITERALLY NOT ONE SINGLE CASE of discontinuation from ISRs...Again, this matches my clinical experience precisely, where conjunctivitis is the most common cause and I've *never* seen ISRs drive discontinuation once.
So WTF is $APGE talking about? How are they making this bold claim that goes directly in the face of the entire body of medical evidence?
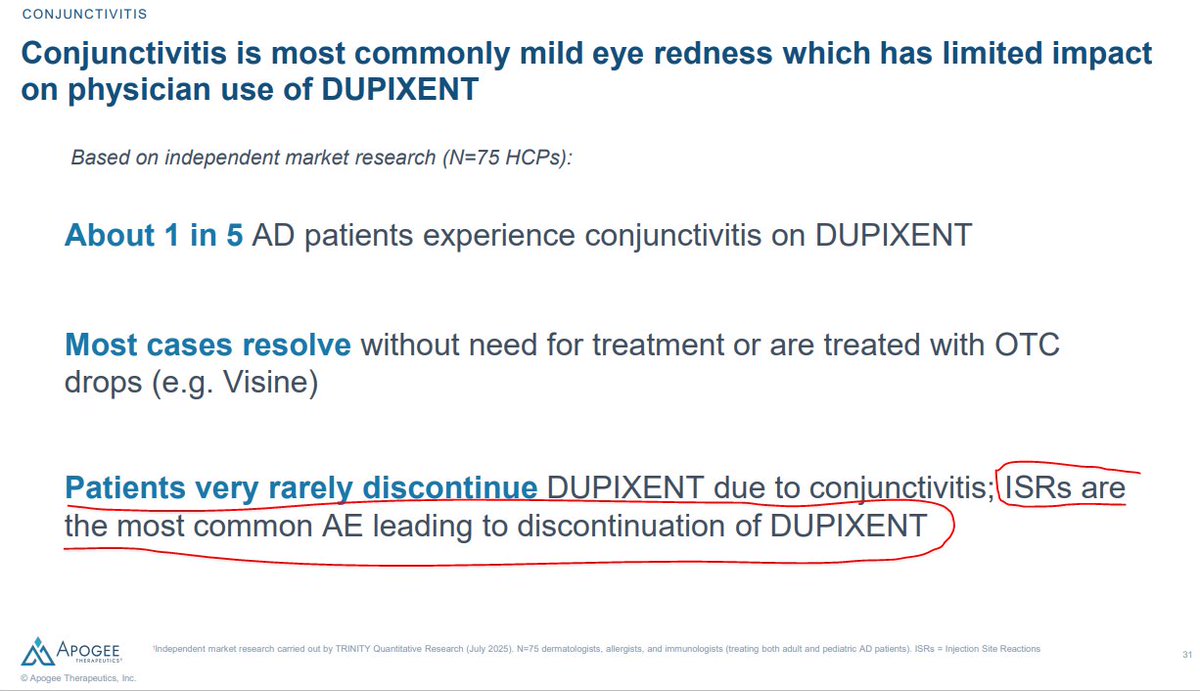
Well, if you read the tiny footnote in this slide from their corporate deck, this bold claim is apparently coming from "independent market research" via some sort of physician survey...
...ok. Well, hopefully I don't have to convince people that you can design a survey such that it gives you almost any result you want. IDK how this internal dataset looks, how it was collected, etc etc, so I can't tell you exactly what's wrong with it. But, I can tell you that across my own clinical experience and literally THOUSANDS of patients in the literature, I cannot find a SINGLE case of discontinuation due to ISR, whereas there are DOZENS of confirmed cases due to conjunctivitis.
Yet here is $APGE going around and repeatedly spreading the same ISR FUD that the $LLY legal team has tried to invent in order to screw over $NKTR. You can take my biased word that this is absolute bullshit if you want, but fortunately thousands of patients worth of objective clinical data happen to be on my side here.
I think $APGE is absolutely *Full*. *Of*. *Shit*. with this ISR vs conjunctivitis nonsense.
Fortunately for me, the publicly available data unequivocally agree.
16
9
152
55,451
Jordan Alexander retweeted

May 22
$QURE APPROVE IT, HEAL US
@WhiteHouse @POTUS @RobertKennedyJr @FDA_KyleD @FDACBER @US_FDA @SenRonJohnson @SenRickScott

4
25
117
26,777