
PharmD, EM/CritCare, RCT purist, Biotech analysis & investing
Joined November 2017
- Tweets 4,698
- Following 555
- Followers 6,497
- Likes 12,192
466 Photos and videos







STL Biotech retweeted

$XBI $SLDB $SRPT
This reminds me of something $SLDB shared recently in a fireside—
in dose escalation of their novel DMD gene Tx, which nevertheless bears structural similarities with $SRPT commercial Elevidys, $SLDB “discovered” a region of the gene that should not be disturbed.
Fortunately, the effects as to the patient, a young boy, in question were relatively not severe and reversible. However, it could have been much worse, said $SLDB. They reported out their findings to the scientific community, I believe.
But shortly thereafter, $SLDB learned that this must-preserve region of the gene was already known to $SRPT, as it was (finally) disclosed in their drug’s label upon regulatory approval…
3
23
6,064
STL Biotech retweeted

Jun 12
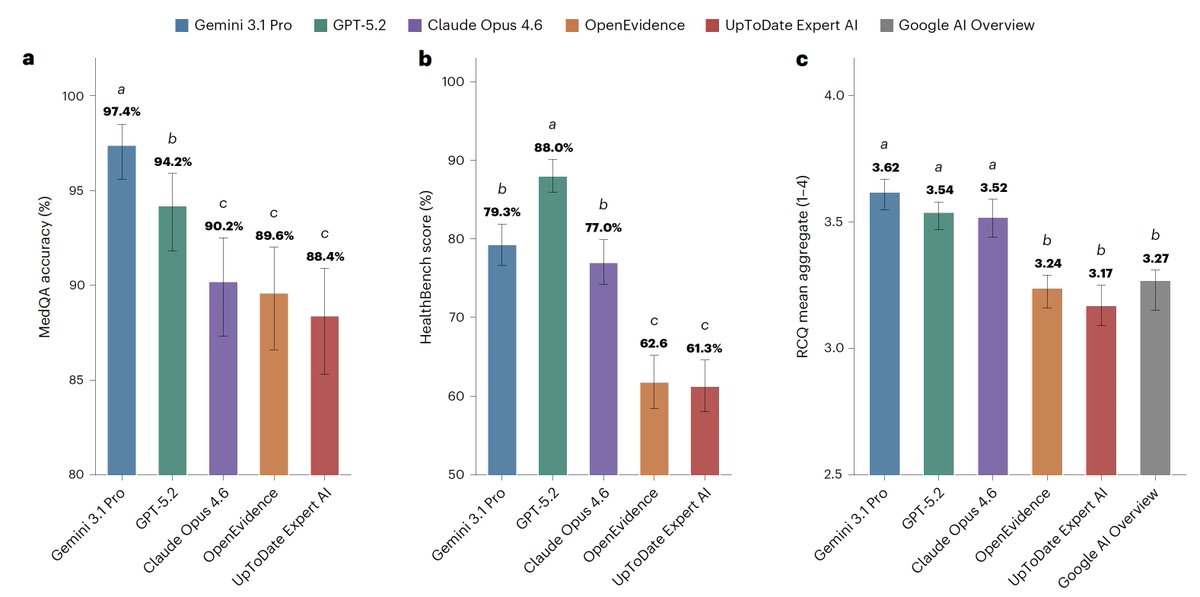
For medical information, general AI frontier models (Google, OpenAI, Anthropic) outperformed specialized @EvidenceOpen and @UpToDate as assessed by 12 US clinicians, randomized and blinded to which model and extensive testing/benchmarks. This was not anticipated. @NatureMedicine
nature.com/articles/s41591-0…
118
522
1,934
809,033

Jun 12
Did we really need another cardiac myosin co?
Or another sGC activator
fiercebiotech.com/biotech/ca…
1
3
1,685
Jun 11
Bought the cancer scare meltdown. Planned for a quick swing trade.
Now I have a "La Lettre" account.
4
66
7,808
STL Biotech retweeted

Jun 10
Your stocks went DOWN because AI stocks went UP
So naturally you thought that your stocks would go UP when AI stocks went DOWN!
You thought wrong, you dumb bitch!
37
52
2,214
132,705
STL Biotech retweeted

Base editing in human embryos fixes some mutations and creates others (and creates other problems) article in reply
Why is Human Heritable Genome Editing controversial?
1) The science is not ready
Embryo editing still has major technical problems, including mosaicism, unintended edits, and uncertainty about long-term effects.
2) The risk is borne by a future person who cannot consent.
The edited child has no say in the intervention, and the change may be passed to future generations.
3) There are often safer alternatives.
For many inherited diseases, IVF plus preimplantation genetic testing can avoid disease without editing embryos.
4) It creates a pathway from disease prevention to enhancement.
The same tools used to prevent disease could be redirected toward traits such as height, cognition, appearance, or perceived “optimization.” h/t @UrnovFyodor for calling the ultrawealthy advocates of HHGE "baby Improvers"
5) It risks privatized eugenics.
If genetic “improvement” becomes a service for the wealthy, it could deepen inequality and normalize the idea that some genomes are preferable to others.
6) Governance is weak and jurisdiction-shopping is likely.
Even where embryo editing is restricted or banned, private actors may seek permissive jurisdictions, weak oversight, or opaque pathways to proceed.
#geneediting #ethics #bioethics

6
7
18
5,193

Jun 7
Nice review of everything nephrology 2025. IgAN LN CAR-T by @FreelyFiltered
With all the talk around issues in neuro at FDA lately, nice to hear such praise for AAs and surrogate endpoints:
"Without this, industry wouldnt have been interested in doing any of these trials"
1
4
2,396
Jun 8
Another reason to not quibble over very small differences between drugs when insurance dealings will matter more in the end.
1
1,050
STL Biotech retweeted

Jun 8
6
25
8,264
STL Biotech retweeted

$JNJ acquiring a pan-KRAS degrader via Firefly Bio for $1B
businesswire.com/news/home/2…
6
15
101
52,207
STL Biotech retweeted

Jun 8
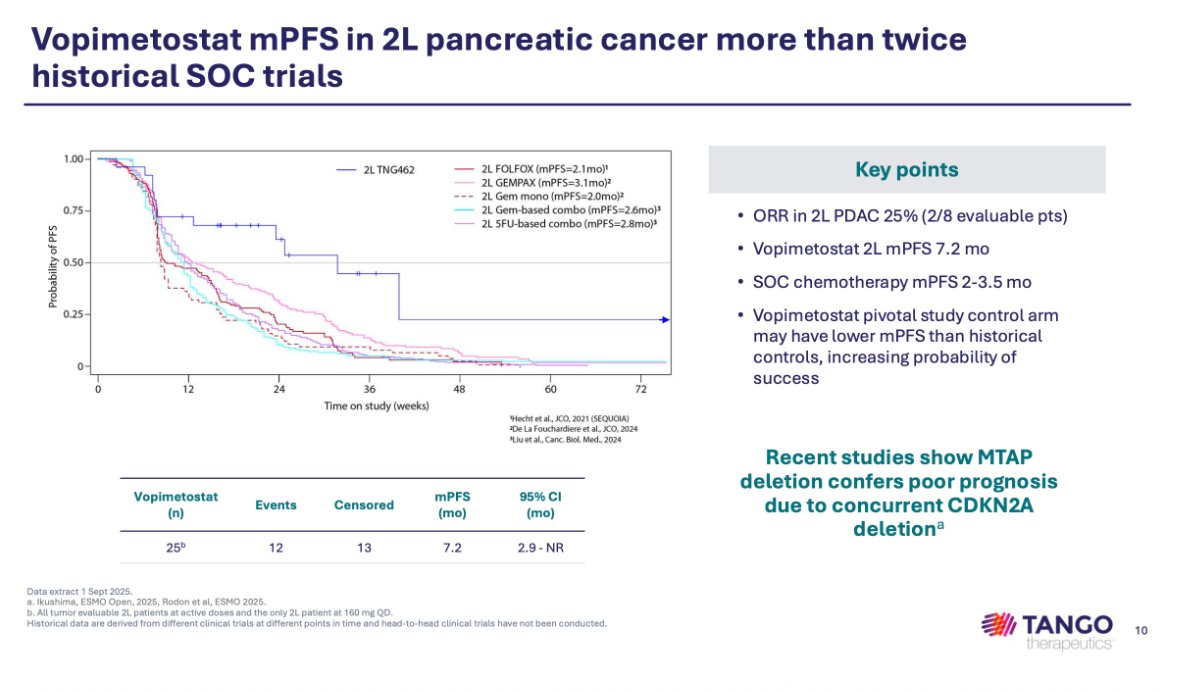
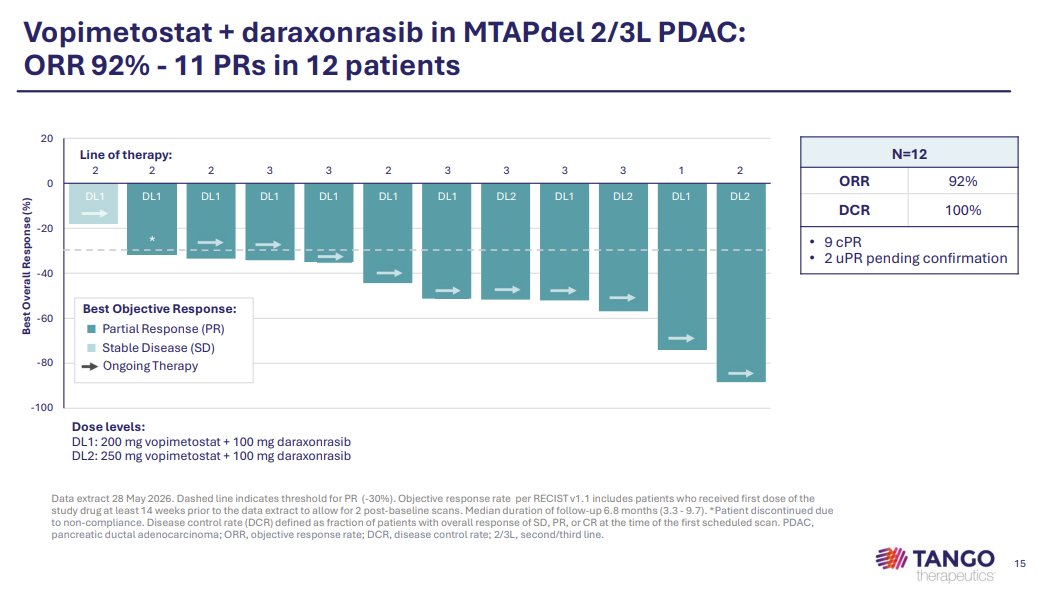
$TNGX Tango Therapeutics Announces Combination of Vopimetostat and Daraxonrasib Demonstrated 92% Objective Response Rate in Pancreatic Cancer | Tango Therapeutics, Inc ir.tangotx.com/news-releases…
3
9
7,582

Yes, small sample size but he’s also making the fallacy of equating equal sample sizes (patient number) to equal AE capture.
Sure, the number of patients in the placebo arm was roughly equal to the 50mg arm, but 66% of the placebo arm patients dropped out of the study before completion, versus only 18% of the 50mg arm!!!
This means the PATIENT YEAR sample from the placebo arm is likely ~half that of the $ABVX 50mg arm’s patient year sample.
So, the placebo arm should naturally be EXPECTED to have a lower rate of cancers, even with the same starting “sample size”, and even with A DRUG THAT DOES NOT HAVE CANCER.
10
4
117
61,078
Jun 7
Endorse. Would add dont get *too* caught up on pre-clin, pk/pd, minor differences, cross trial com. Much more goes into M&A. & Buy the leaders not the distant 3rd/4th/5th.
CAR-T:
KITE / JUNO
APRIL:
KDNY / ALPN
M4:
KRTX / CERE
CMI:
MYOK/CYTK
hs-CRP lowering:
TRML / VTYX
Jun 5

Often times in biotech for a given disease or target, a basket approach proves optimal vs trying to select just one winner $XBI
Occasionally I see longs pounding the table for a given company while belittling the competitor product, failing to realize it doesn't have to be "either or" (both can be compelling)
Ie. For $$ you have ready to deploy, split the funds 50/50 between the two
If you are more bullish on one vs the other but like both (or one is further ahead commercially, the other is cheaper, etc), allocate the funds 2/3rd to Stock A and 1/3rd to Stock B according to your personal preference
Again, both can win (not always a zero-sum game) 🙂
Cheers
3
2
22
5,200
Jun 7
Even kinda worked out with Thr-B, albeit special case.
MDGL/VKTX
1
1
1,150
Jun 4
$ABVX
Rare to get a full 6.5 hour trading day to pull the trigger like this.
With marginal understanding of UC market, stats, and how cancers develop it took maybe 2 hours of work to get comfortable.
Sheep, Adam, others right, price driving narrative. (In both directions)
Jun 2

$ABVX
Bought a little. 75s
Pray for me.
57
6,406
Jun 4
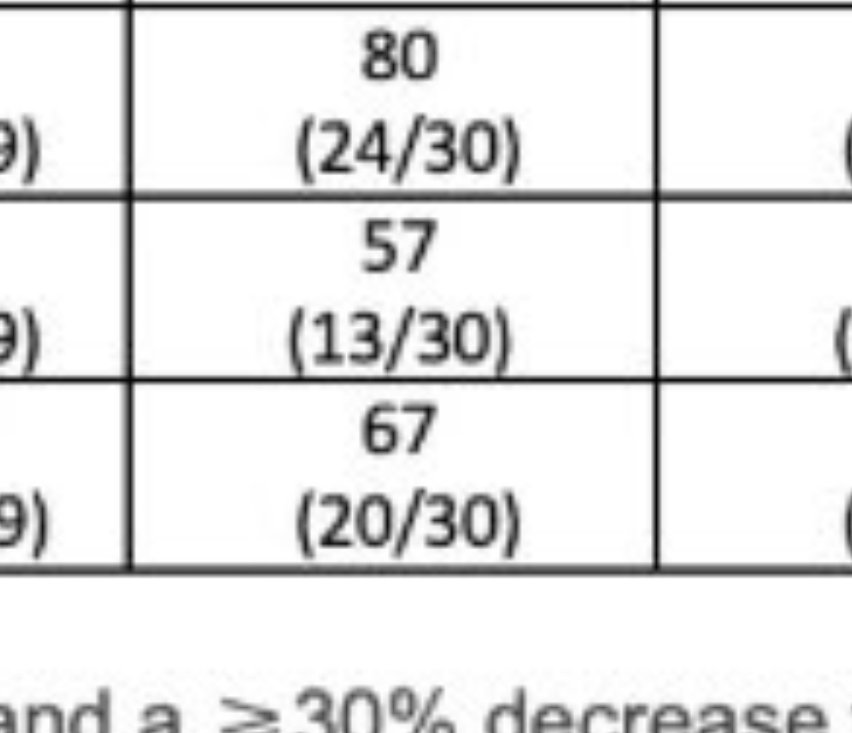
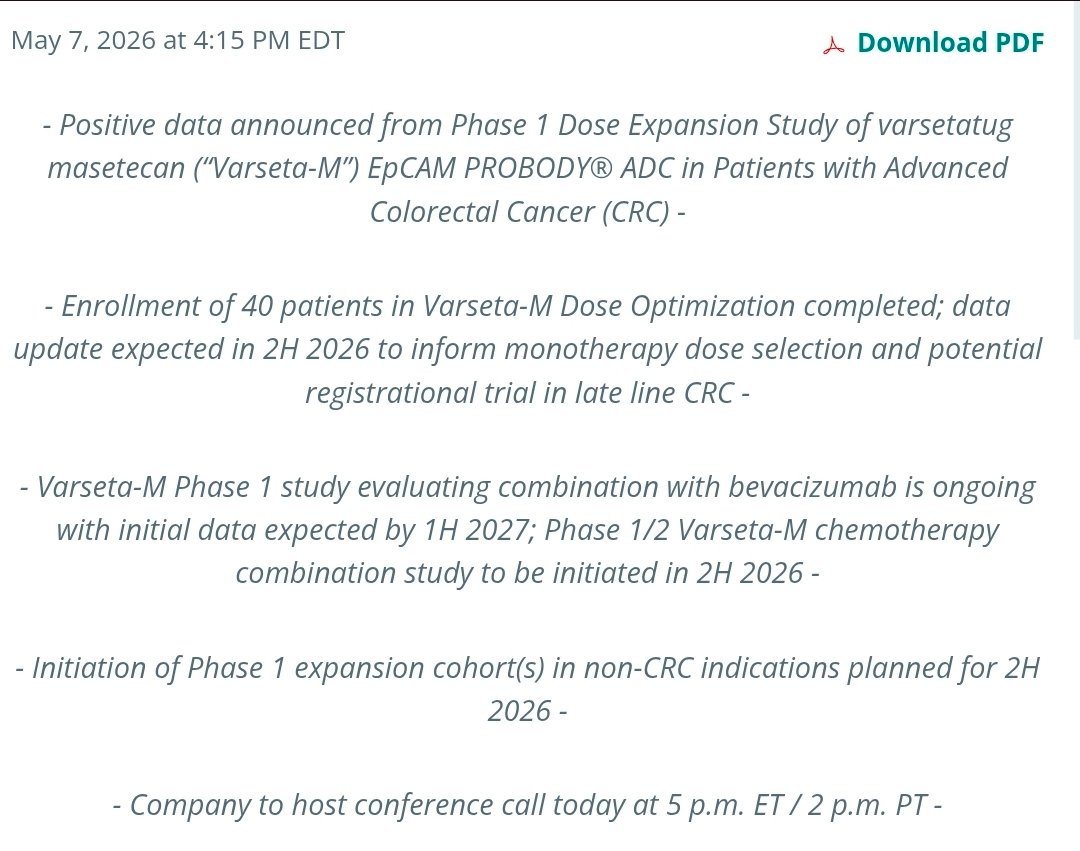
Nice review of current and emerging literature in CRC
Given so much emphasis on low ORRs in late line mCRC, interesting to hear MD quite enthusiastic for 10% delta on OS at 24mos and lower incidence of HFMD for zanzalitnib
Relavent $EXEL, perhaps $CTMX
open.spotify.com/episode/1QQ…
11
1,529