
Galleguiño 🌊 | Med Onc resident @ICO_oncologia | Skin cancer, IO & cell therapy 🎯 | 2025 Rotation Research @UTMDAnderson 🇺🇸 | @OncoAlert team💥 | Pianist 🎹
Joined March 2023
- Tweets 1,041
- Following 692
- Followers 1,652
- Likes 2,365
361 Photos and videos





Pinned Tweet

Apr 28
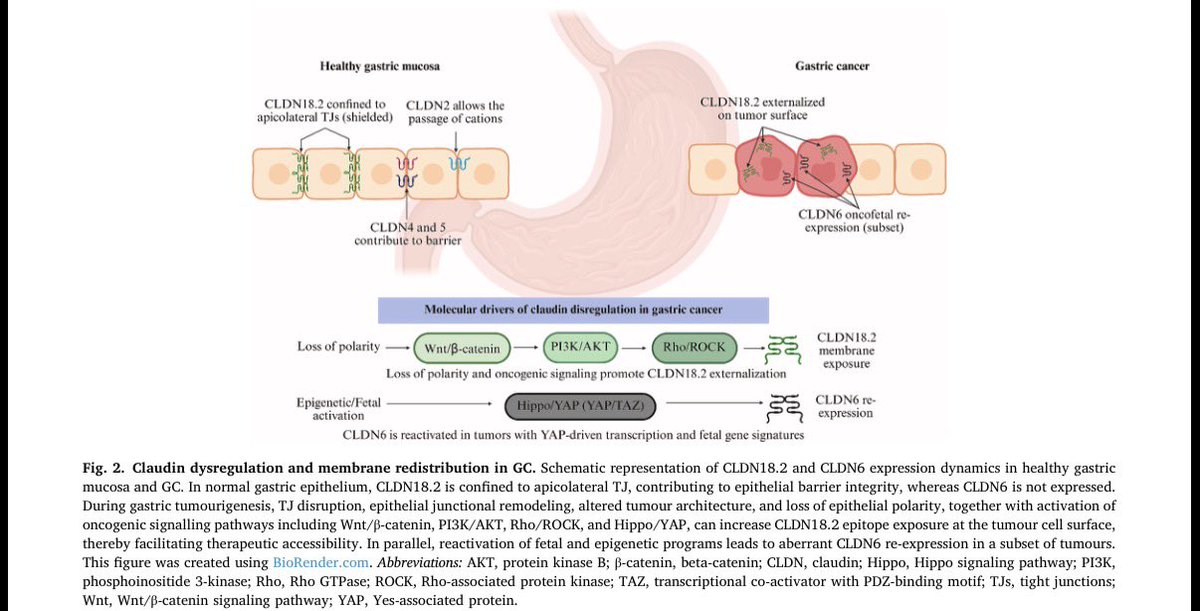
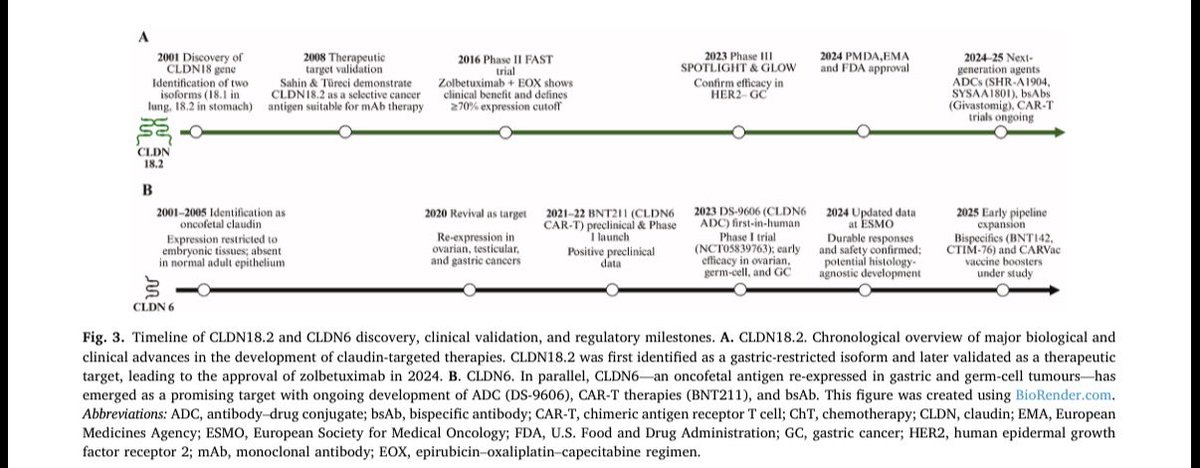
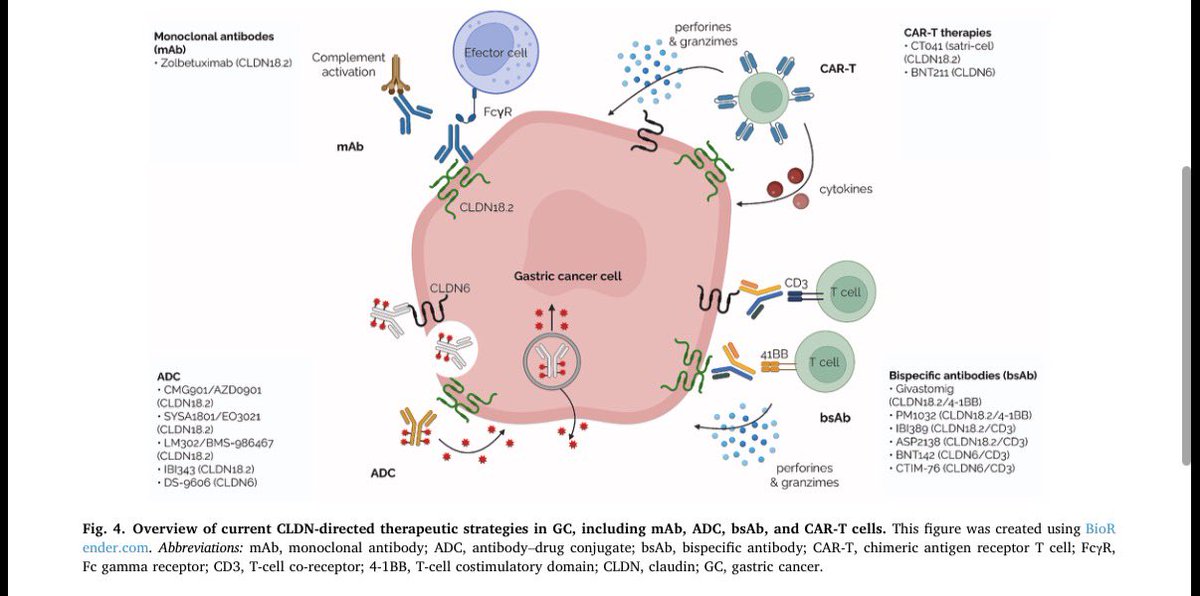
✨ Our new review is OUT! Targeting claudins in gastric cancer
sciencedirect.com/science/ar…
From tight junction biology to real clinical impact 💥
▪️ CLDN18.2: from “hidden” protein to actionable target
▪️ Beyond mAbs → ADCs, bsAbs & CAR-T incoming
▪️ CLDN6 & CLDN1 emerging as the next frontiers
▪️ Expression ≠ accessibility → biology matters
Time to CLAUD-in on the opportunity and let gastric cancer finally GLOW in the SPOTLIGHT 💡
Thank you @DrMirallas @EduardoTB94 @CalvoMariona @tfleitask @BugesCris @RobertMontal for your great work! And special thanks to Dr. @chierrocarbo for her invaluable teaching and inspiration! 🧡
@OncoAlert @OncoReporte @myESMO @_SEOM @GrupoTTD @ICO_oncologia

4
28
73
9,443
Jun 12
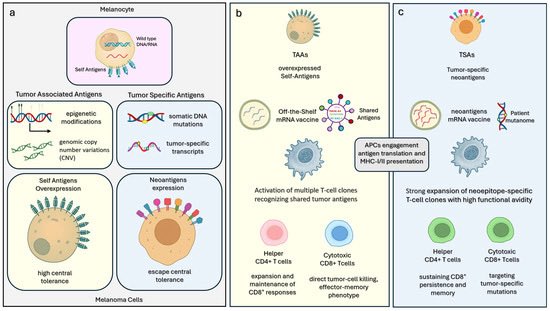
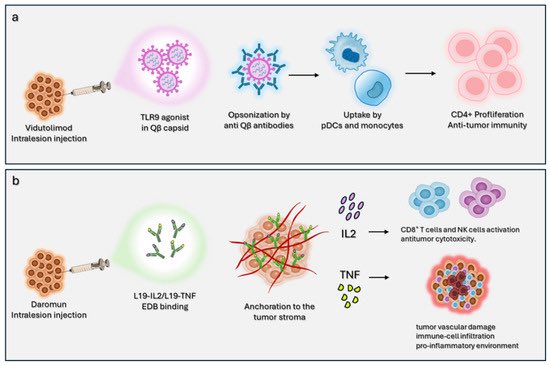
🧬 How deeply can mRNA vaccines affect responsiveness to ICI in melanoma? (review)
mdpi.com/2073-4409/15/11/986
🎯 mRNA vaccines may convert “cold” tumors into “hot” tumors
▪️Enhanced antigen presentation and CD8 T-cell infiltration
💥 TME remodeling may be as important as antigen targeting itself
The message may be RNA, but the goal is clear: teach the immune system a language the tumor can no longer ignore 😉
@OncoAlert
@OncoReporte @_SEOM @myESMO

1
5
22
1,636
Jun 11
Wow…🤯
Jun 10

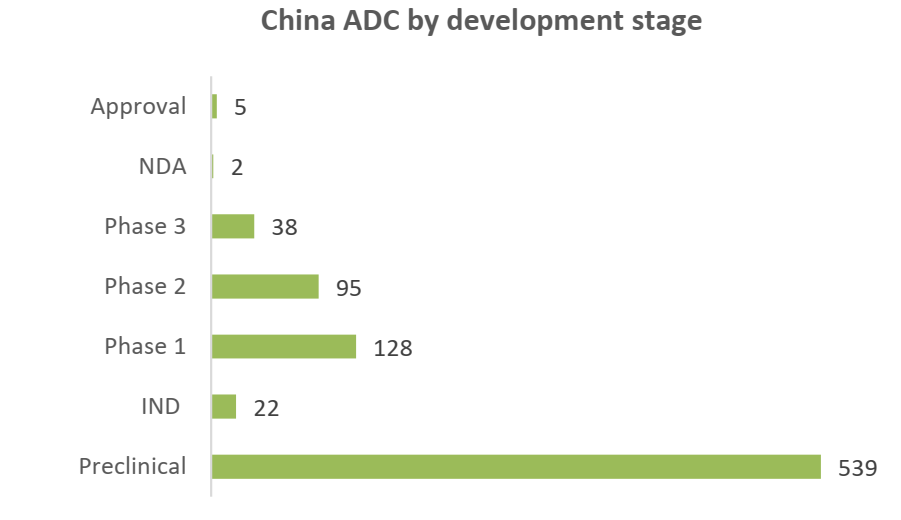
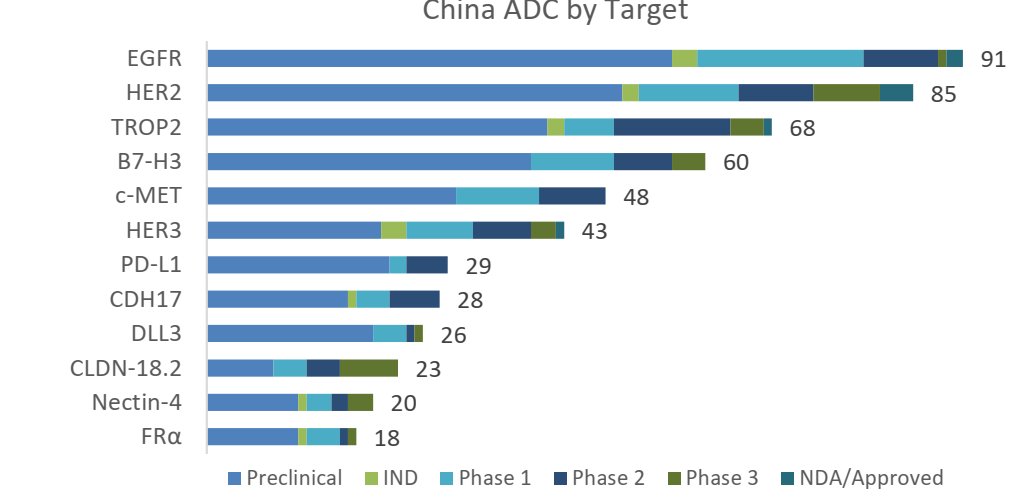
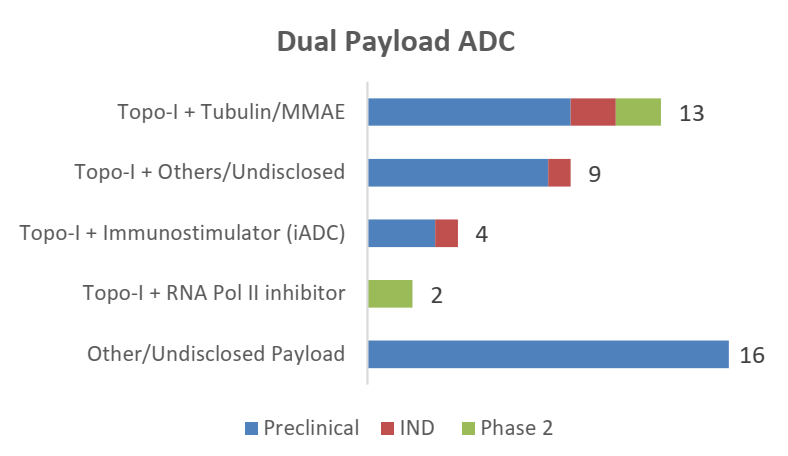
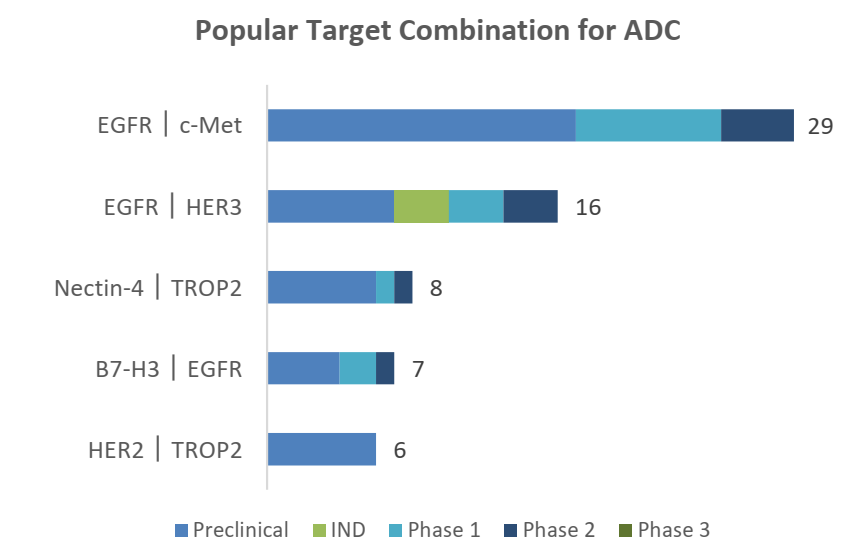
China ADC landscape (Great report from Locust Walk)
Next wave is more innovative (bispecifics, new payloads dual payload)
1
4
725
Jun 11
💥Delighted to receive the 🥈 2nd Prize at Pulmón Target 2026 (ALK & EGFR)!
Perhaps the most meaningful part is that this will likely be my last resident competition before completing my Medical Oncology residency next month.
A wonderful way to close an unforgettable chapter! 🎯
My sincere thanks to the coordinators and to my mentor Dr. Mosteiro, for creating such a valuable educational initiative 🧡
Congratulations to all participants! 🙌
@_SEOM @ICO_oncologia
2
9
595
Jun 11
⛪️ “Primer l’amor, després la tècnica”. Translation: “love first, technique later”.
Last night, Gaudí’s words illuminated the sky above the Sagrada Família.
They were written about architecture, but they could just as easily apply to medicine 🩺
Every era has its great technological revolutions. Ours is happening now in oncology💥
Yet innovation only matters when it serves a human purpose:
👥 To cure more patients
🫂 To reduce suffering
🎯 To spare unnecessary toxicity
☝🏼 To remember that every biomarker belongs to a person, not just a tumor
Gaudí had it right: first the purpose, then the technique 🧡
@OncoAlert
@OncoReporte @myESMO @_SEOM
2
10
329
Jun 11
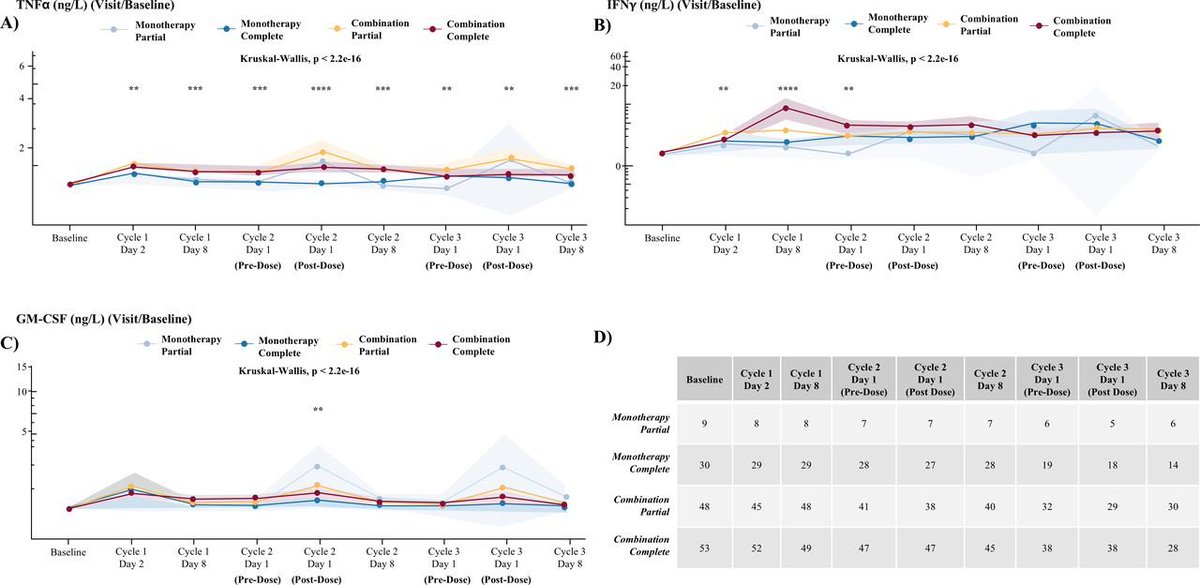
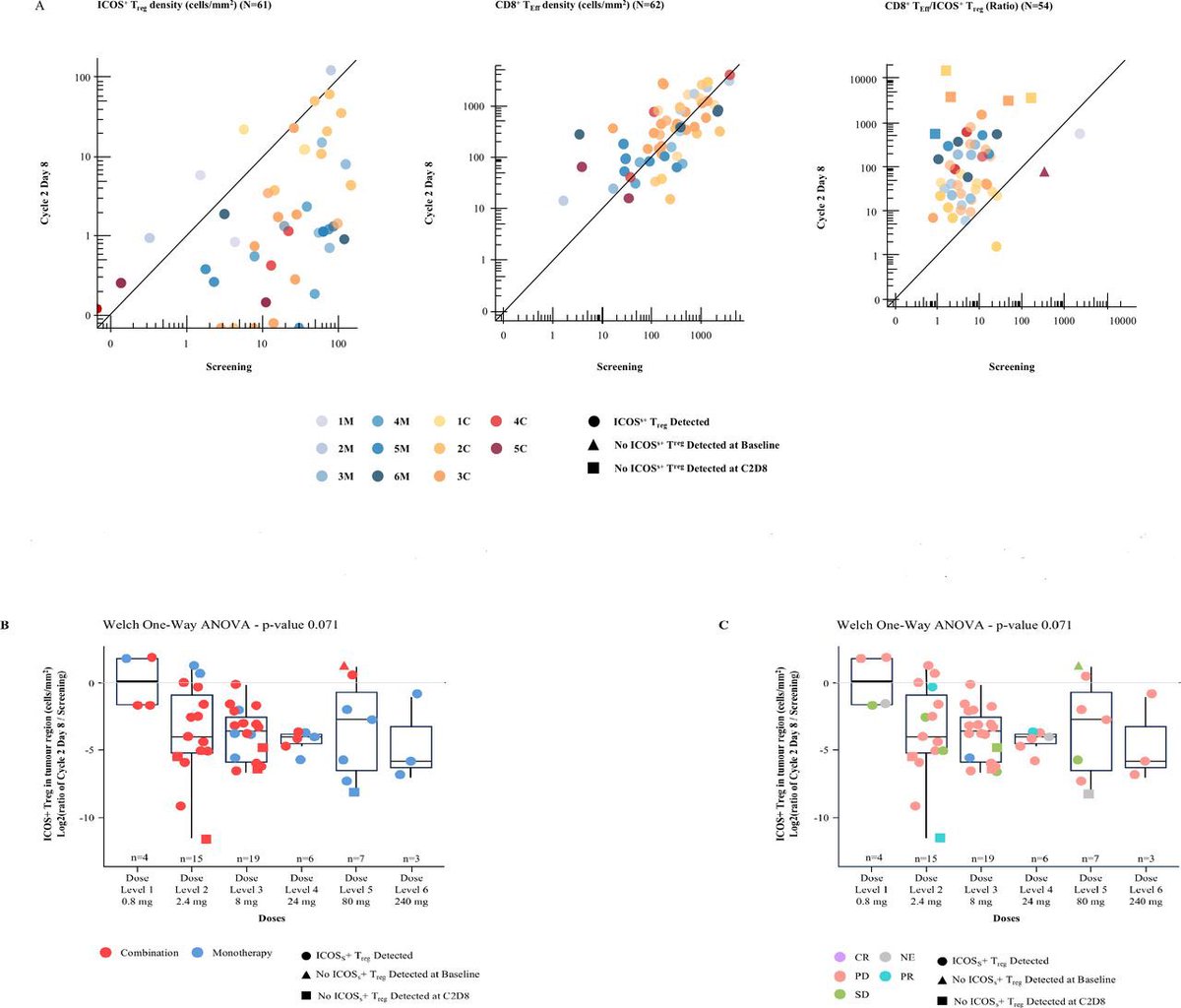
🚨 Alomfilimab (anti-ICOS) ± atezolizumab in advanced solid tumors (phase I, n=140: 38 in monotherapy, 102 in the combination therapy cohort)
jitc.bmj.com/content/14/6/e0…
🔹 Manageable safety profile
🔹 ICOS Treg depletion confirmed
🔹 Increased CD4 /CD8 effector activity
⭕️ ORR 0% with monotherapy
🔴 ORR 6.8% with combination, mPFS 2m…
ICOS may be a target, but this trial suggests it is not the whole answer 🤔
@OncoAlert
@OncoReporte @_SEOM @myESMO
1
6
10
1,161
Mario Balsa retweeted

Veiem per primera vegada la torre de Jesucrist il·luminada!
L'espectacle de llum iniciat des de la base fins a la il·luminació de la creu ha culminat amb una composició de llums guiats per drons, que han dibuixat la figura Gaudí i la frase «primer l'amor, després la tècnica».
505
11,348
44,759
2,284,114
Mario Balsa retweeted

#ASCO26 GU | RADICAL Alliance A031801
Official ASCO abstract: @DrRanaMcKay
@ASCO @OncoAlert
asco.org/abstracts-presentat…
RADICAL tested a biologically attractive strategy:
radium-223 cabozantinib vs cabozantinib alone in RCC with bone metastases.
The rationale made sense.
Bone metastases are a major unmet need in RCC, and cabozantinib has known activity in this setting.
But the primary endpoint was negative.
Adding radium-223 did not improve symptomatic skeletal event–free survival, and the study crossed the futility boundary.
Important nuance:
A numerical OS signal was observed, but this remains hypothesis-generating and should not override the negative primary endpoint.
My take:
RADICAL is a useful negative trial.
It tells us not to add radium-223 to cabozantinib outside trials for RCC bone metastases.
But it also reminds us that bone-dominant RCC still needs better strategies: pain control, skeletal-event prevention, radiotherapy integration, bone-targeted supportive care, and better trial design.
Negative trials are not failures.
They are how algorithms become safer.
#RCC #KidneyCancer #GUonc #ASCO26
@DrChoueiri 🇺🇸@hoperugo 🇺🇸 @matteolambe 🇮🇹 @TiansterZhang 🇺🇸 @CathyEngMD 🇺🇸 @stolaney1 🇺🇸 @montypal 🇺🇸 @tompowles1 🇬🇧 @brian_rini 🇺🇸 @cdanicas 🇪🇸 @NiuSanford 🇺🇸 @amerseburger 🇩🇪 @GlopesMd 🇺🇸 @Icro_Meattini 🇮🇹 @PGrivasMDPhD 🇺🇸 @DrYukselUrun 🇹🇷 @nataliagandur 🇦🇷 @ElisaAgostinett 🇧🇪 @HHorinouchi 🇯🇵 @realbowtiedoc 🇺🇸 @to_be_elizabeth 🇮🇹 @UOzkerim 🇹🇷 @p_ciracimd 🇮🇹 @DrVilmaPBarcia 🇪🇸 @DraMartinezLago 🇪🇸 @DrMirallas 🇺🇸 @GaiaGriguolo 🇮🇹 @MarioBalsaMD 🇪🇸 @scocmem 🇬🇧 @AmandaNizamMD 🇺🇸


2
7
17
1,613
Jun 10
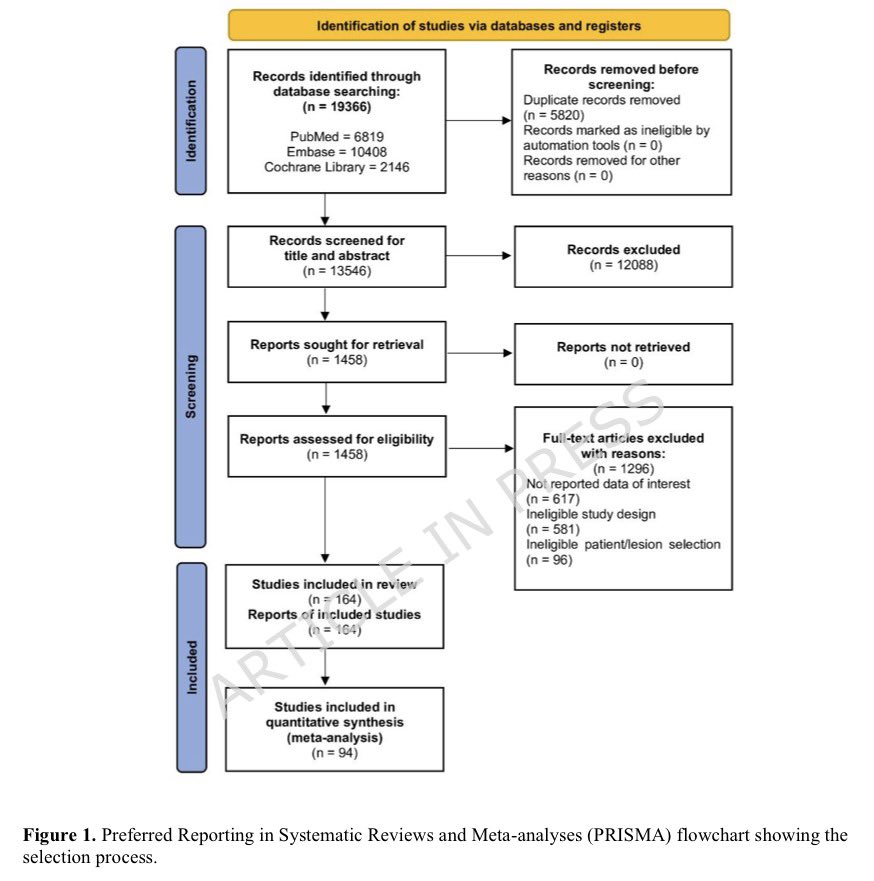
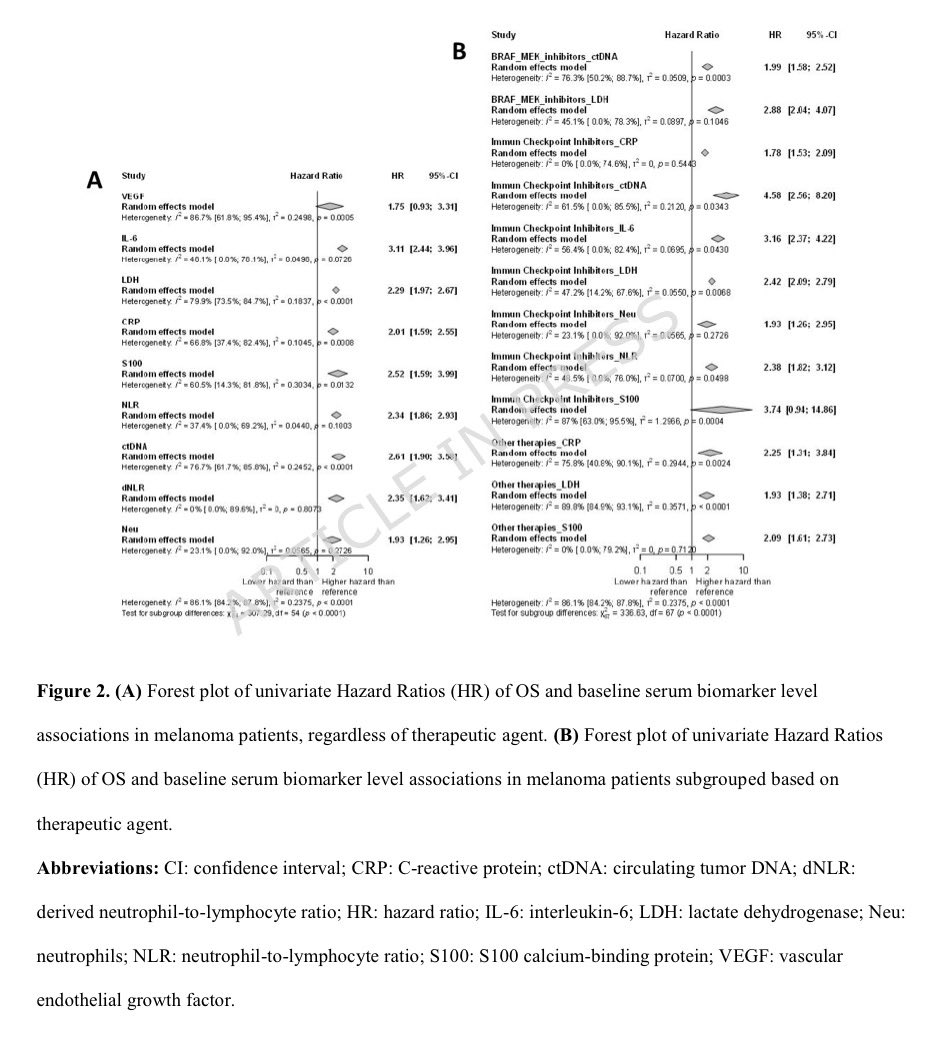
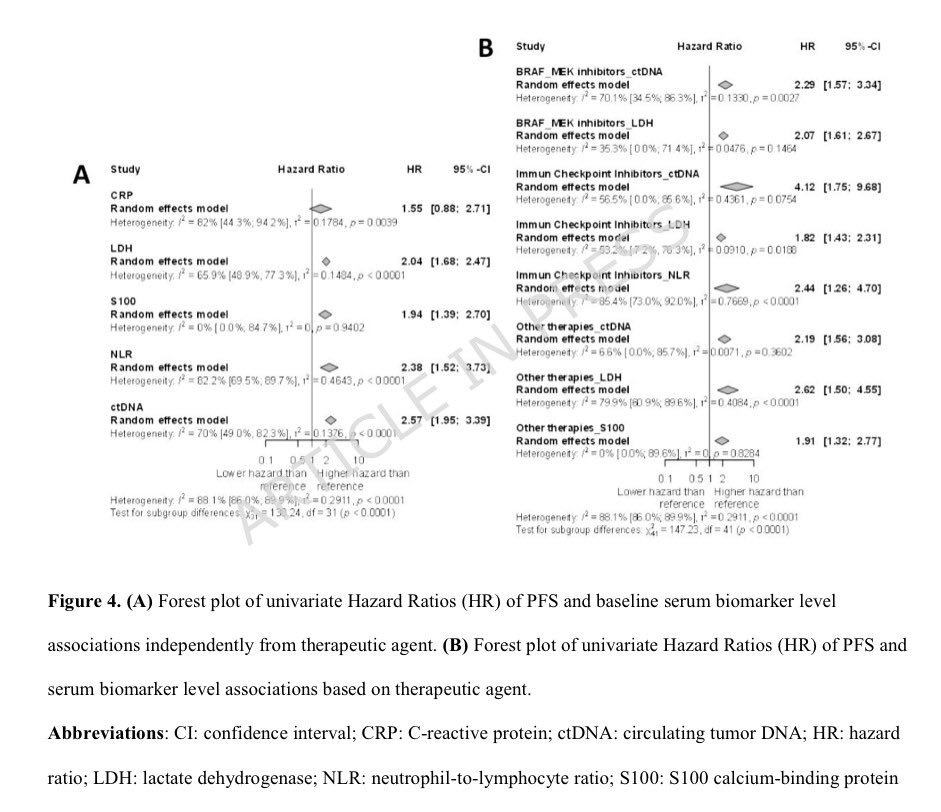
🩸 Predictive value of serum biomarkers for survival in melanoma: a systematic review and meta-analysis (94 studies)
🎯 OS: LDH (HR 2.29), ctDNA (HR 2.61), S100B (HR 2.52), NLR (HR 2.34), IL-6 (HR 3.11)
⏳ PFS: ctDNA (HR 2.57), NLR (HR 2.38), LDH (HR 2.04), S100B (HR 1.94)
💥 Associations remained significant in multivariable analyses, supporting their independent prognostic value
Biomarkers shaping the prognosis narrative🔬
@OncoAlert
@OncoReporte @_SEOM @myESMO

7
12
4,424
Jun 9
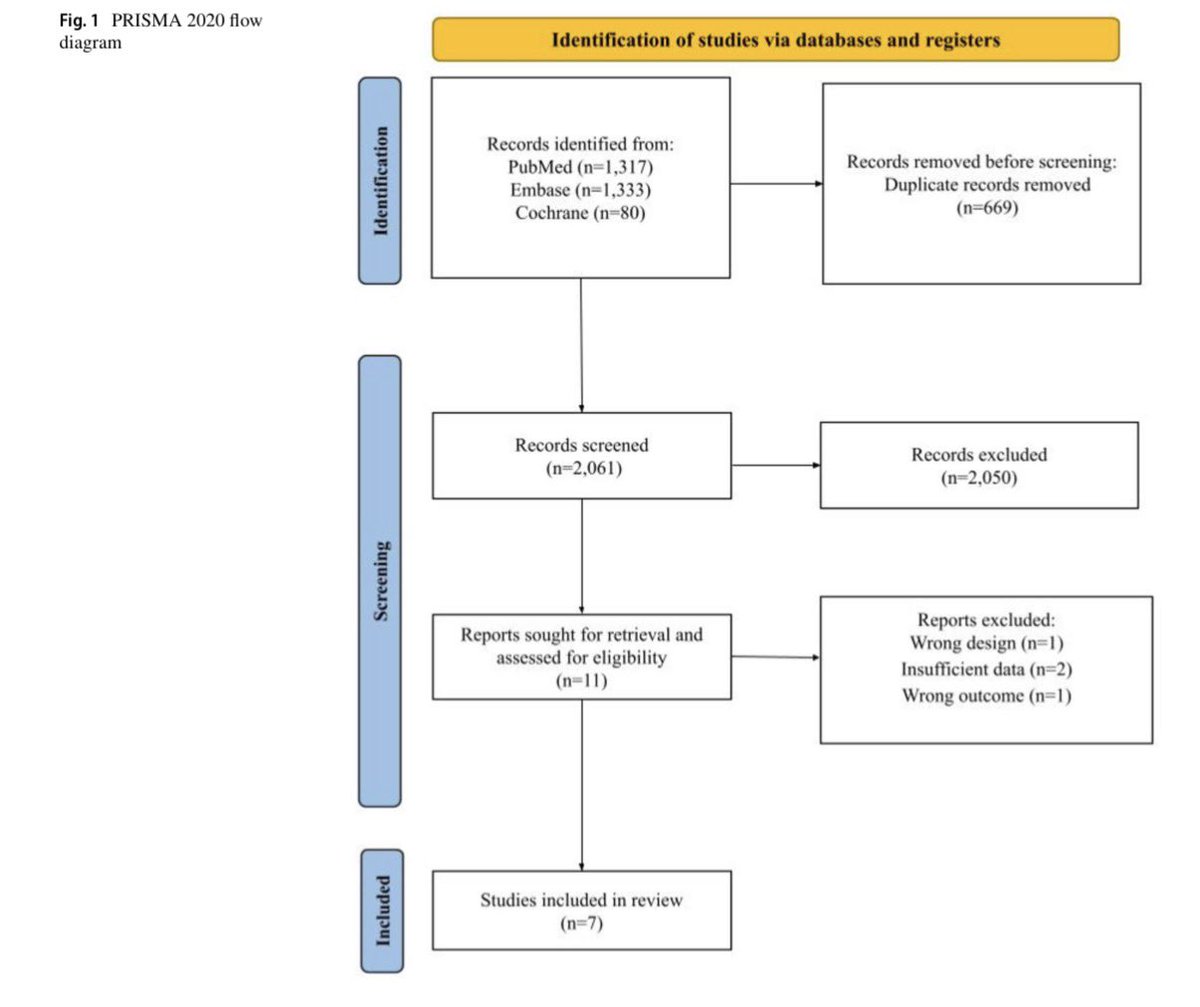
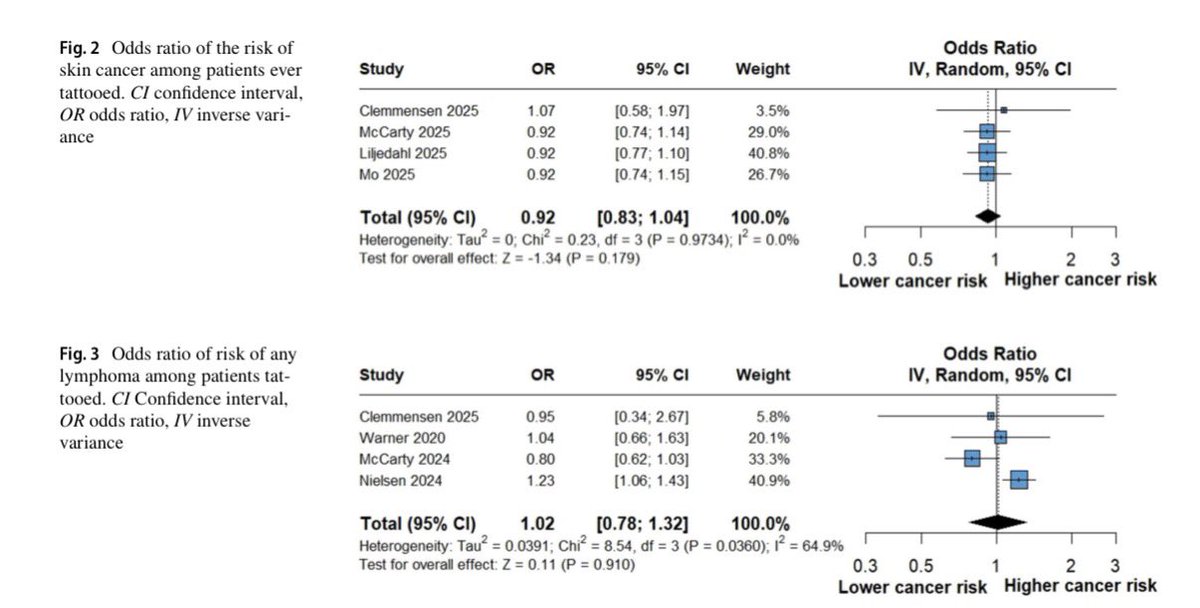
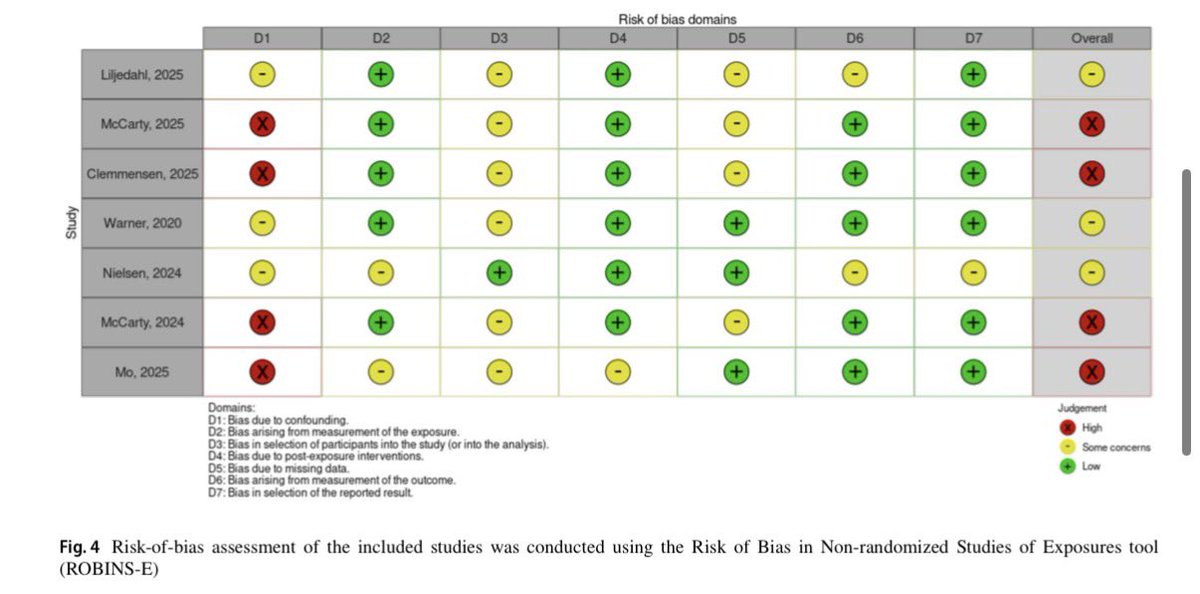
🤔 Are tattoos linked to cancer? A new meta-analysis says probably not
link.springer.com/article/10…
▪️ Systematic review and meta-analysis of 7 observational studies (n=140,841)
🎯 No association between tattoos and overall skin cancer risk (OR 0.92)
🩸 No significant association with hematologic malignancies in the primary analysis (OR 1.02)
🔍 A signal for hematologic cancers emerged only in sensitivity analyses, requiring cautious interpretation
Looks like the data are keeping this debate under the skin for now 👀 #CancerPrevention #Dermatology #Oncology
@OncoAlert
@OncoReporte @_SEOM
4
5
416
Mario Balsa retweeted

Great start of #EACR2026: Women in Science discussion panel with #JohannaJoyce, #XinLu, #JaneSmith, @samuels_yardena, #CarolibeDive and a great group of female researchers on the rise!


3
10
894
Jun 8
🚨 Missed a session? Couldn’t be in every room at #ASCO26?
🔗 oncoalert.m-pages.com/nhMpwe…
That’s exactly why the @OncoAlert Complete ASCO26 Newsletter exists!!!
-The biggest studies
-The key take-home messages
-The trials everyone will be talking about
ASCO ends. The reading starts 😏
Jun 8

Dear Colleagues at #ASCO26
Thank you for joining us and reminding you that THE COMPLETE ONCOALERT NEWSLETTER with ALL of our picks from #ASCO26 comes out this Thursday and conveniently to your Inbox
REGISTER HERE 👉buff.ly/bTpzTQY
@DrChoueiri 🇺🇸
@hoperugo 🇺🇸
@matteolambe 🇮🇹
@TiansterZhang 🇺🇸
@CathyEngMD 🇺🇸
@stolaney1 🇺🇸
@montypal 🇺🇸
@tompowles1 🇬🇧
@brian_rini 🇺🇸
@cdanicas 🇪🇸
@NiuSanford 🇺🇸
@amerseburger 🇩🇪
@GlopesMd 🇺🇸
@Icro_Meattini 🇮🇹
@PGrivasMDPhD 🇺🇸
@DrYukselUrun 🇹🇷
@nataliagandur 🇦🇷
@ElisaAgostinett 🇧🇪
@HHorinouchi 🇯🇵
@realbowtiedoc 🇺🇸
@to_be_elizabeth 🇮🇹
@UOzkerim 🇹🇷
@p_ciracimd 🇮🇹
@DrVilmaPBarcia 🇪🇸
@DraMartinezLago 🇪🇸
@DrMirallas 🇺🇸
@GaiaGriguolo 🇮🇹
@MarioBalsaMD 🇪🇸
@scocmem 🇬🇧
@AmandaNizamMD 🇺🇸
& @weoncologists 🇺🇸
1
6
484
Jun 8
🫁 Do NF1 mutations drive lung tropism in melanoma?
pubmed.ncbi.nlm.nih.gov/4225…
▪️ Analysis of 520 M1 melanoma pts from MSK-MET
💥 NF1 was the strongest genomic correlate of lung M1 (34.9% vs 20.2%, OR 2.11)
🎯 Association remained significant after multivariable adjustment and across sensitivity analyses
🔥 NF1-mutant tumors carried ~2× higher TMB than NF1 wt melanoma
Looks like NF1 isn’t just a melanoma subtype marker…it may have a real lung-guage preference 🫁 #Melanoma #NF1
@OncoAlert
@OncoReporte @_SEOM
4
11
1,415
Mario Balsa retweeted

📅 Avui és el Dia Mundial dels Tumors Cerebrals.
🧠 Un tumor cerebral és un creixement anormal de cèl·lules al cervell, que pot ser benigne o maligne (càncer).
🧍 Els tumors benignes són més comuns en joves, i els malignes en majors de 60 anys.
➕ Info a #PortalCLÍNIC 👉 clinicbarcelona.org/ca/asist…
2
5
15
1,639

Aquesta setmana, a l'IDIBAPS...
Teresa Macarulla i Tian Tian lideren el nou grup de recerca de l'#IDIBAPS "Oncologia translacional del càncer gastrointestinal superior"
👉f.mtr.cool/glsclhxzqa
1
5
711
Jun 6
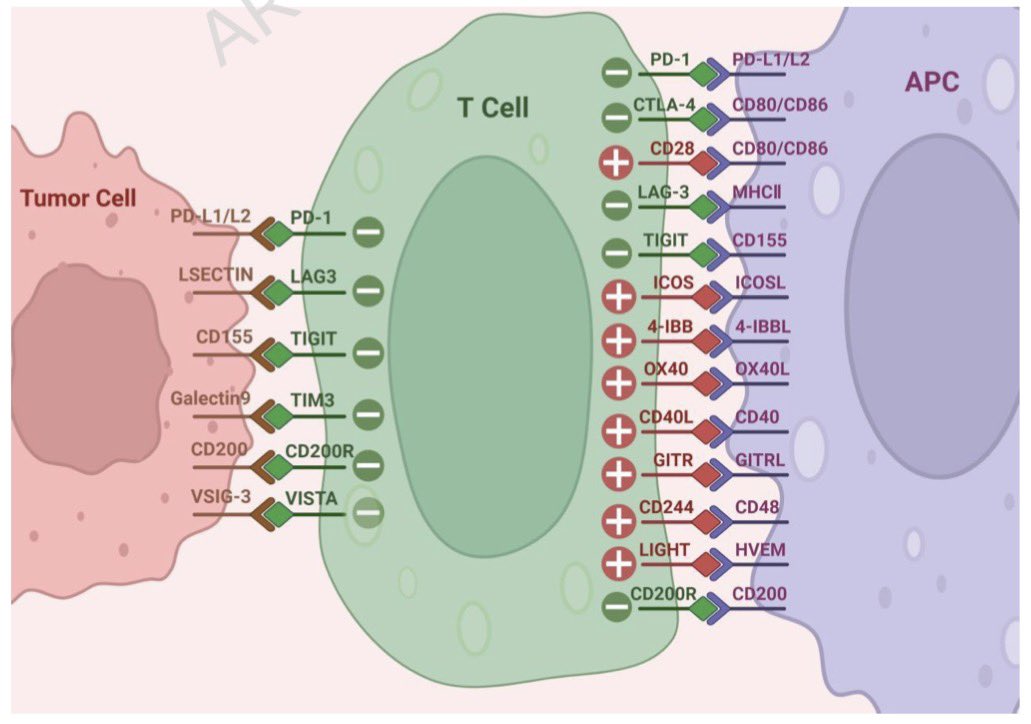
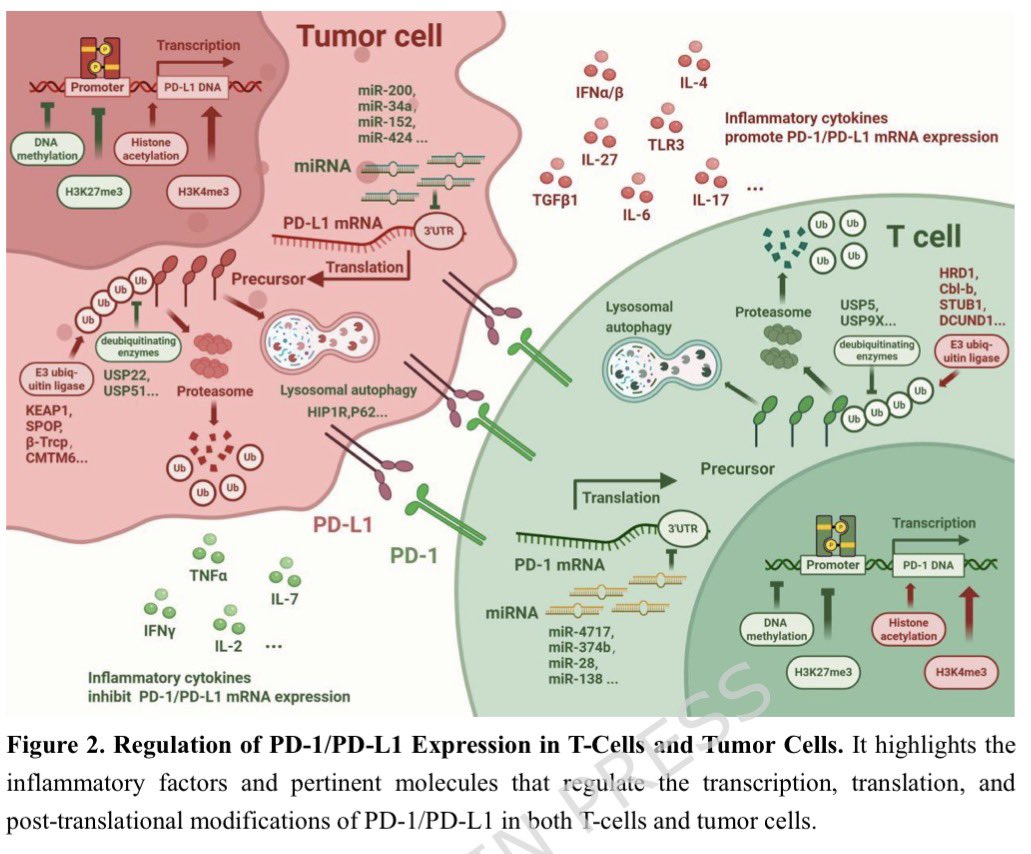
📄 Insight of immune checkpoint blockades in melanoma (review)!
link.springer.com/article/10…
🧬 Comprehensive overview of PD-1, CTLA-4, LAG-3, TIGIT and emerging checkpoint pathways
🔍 Mechanisms of response, resistance and immune escape
🎯 Highlights biomarkers and personalized IO strategies
💥 A roadmap for the next generation of melanoma IO
Checkpoint by checkpoint, learning that the biggest barrier isn’t the blockade itself…it’s what slips through the checkpoints 🔓🧠#Melanoma #Immunotherapy #PD1 #CTLA4 #TIGIT #LAG3
@OncoAlert
@OncoReporte @myESMO @_SEOM
2
19
56
4,138
Jun 6
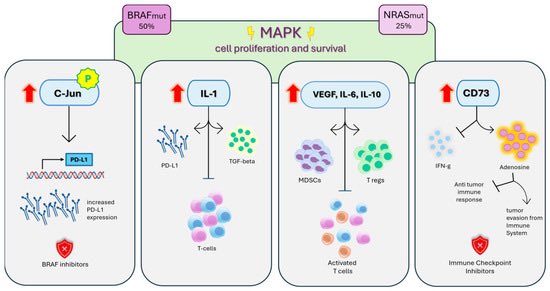
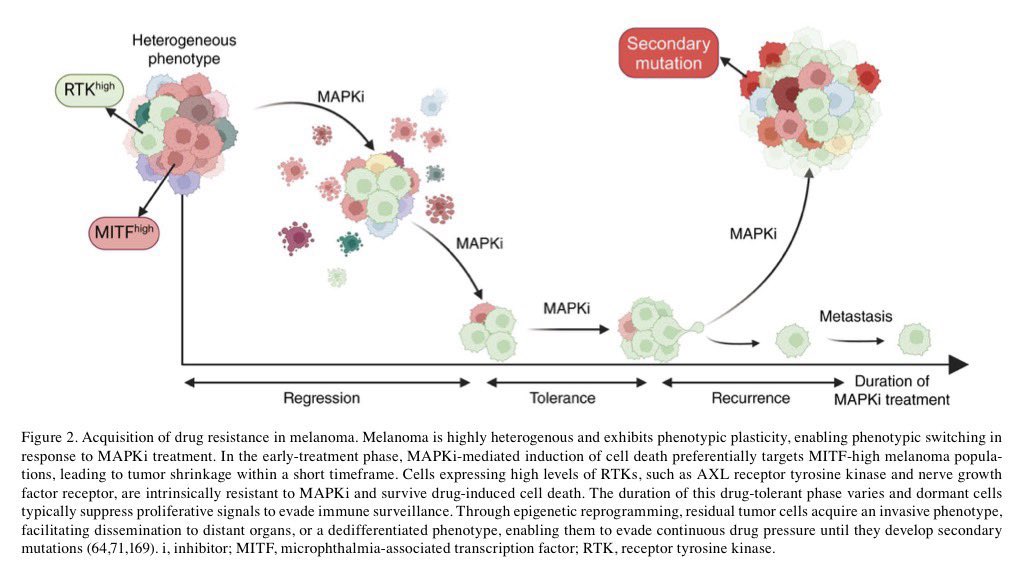
📚 New review! Targeted therapy in BRAF-mutant melanoma: advances and challenges
spandidos-publications.com/1…
🎯 BRAF/MEK combos reshaped melanoma care
💥 Long-term benefit, but resistance remains the rule
🧬 Key culprits: MAPK reactivation, MITF plasticity & phenotype switching
🤔 Next step? Smarter sequencing combinations
We know how to block BRAF, melanoma keeps teaching us how not to get BRAF-fled🧬
@OncoAlert
@OncoReporte @myESMO @_SEOM
1
9
28
2,730
Jun 4
💥 The final #ASCO26 newsletter is out.
🔗 oncoalert.m-pages.com/nhMpwe…
From RASolute302 and LIBRETTO to EV-302, BREAKWATER and beyond, @OncoAlert has curated the studies that will shape oncology long after Chicago.
The meeting is over but the conversations are just beginning ✨
Jun 4
The @OncoAlert 🚨COMPLETE #ASCO26 Newsletter is NOW in your INBOX 📥 OUR picks of the TOP trials presented in Chicago🇺🇸
If you haven't REGISTERED, DO IT Now to GET it
👉buff.ly/25YHTzM
If you have REGISTERED and have not gotten it, Check your SPAM folder if not there email us📨 at OncoAlertNetwork@oncoalert360.com and we will get you sorted.
A HUGE Thanks to ASCO for an Amazing Meeting
@DrChoueiri 🇺🇸 @hoperugo 🇺🇸 @matteolambe 🇮🇹 @TiansterZhang 🇺🇸 @CathyEngMD 🇺🇸 @stolaney1 🇺🇸 @montypal 🇺🇸 @tompowles1 🇬🇧 @brian_rini 🇺🇸 @cdanicas 🇪🇸 @NiuSanford 🇺🇸 @amerseburger 🇩🇪 @GlopesMd 🇺🇸 @Icro_Meattini 🇮🇹 @PGrivasMDPhD 🇺🇸 @DrYukselUrun 🇹🇷 @nataliagandur 🇦🇷 @ElisaAgostinett 🇧🇪 @HHorinouchi 🇯🇵 @realbowtiedoc 🇺🇸 @to_be_elizabeth 🇮🇹 @UOzkerim 🇹🇷 @p_ciracimd 🇮🇹 @DrVilmaPBarcia 🇪🇸 @DraMartinezLago 🇪🇸 @DrMirallas 🇺🇸 @GaiaGriguolo 🇮🇹 @MarioBalsaMD 🇪🇸 @scocmem 🇬🇧 @AmandaNizamMD 🇺🇸 & @weoncologists 🇺🇸
2
6
540
Mario Balsa retweeted

ASCO 2026 HIGHLIGHTS
#ASCO26 delivered a striking mix of practice-changing late-stage data, long-term follow-up, molecularly guided treatment strategies and rare-tumor studies that would once have struggled to attract this level of attention.
I used @Larvol CLIN data to identify the ten most exciting trial results. Here they are:
RASolute 302: daraxonrasib in metastatic pancreatic cancer
RASolute 302 was arguably the most important single therapeutic readout at ASCO 2026. Daraxonrasib, a multi-selective RAS(ON) inhibitor, was tested in previously treated metastatic pancreatic ductal adenocarcinoma.
The trial showed median overall survival of 13.2 months with daraxonrasib versus 6.7 months with chemotherapy, corresponding to a 60% reduction in the risk of death. Reuters also reported tumor shrinkage or disappearance in more than 30% of treated patients, compared with about 10% on chemotherapy.
This is strategically important because pancreatic cancer has long been one of the most difficult tumors to treat, and RAS has historically been considered hard to drug. If approved, daraxonrasib could become a major new treatment option and a platform asset for earlier-line and combination strategies.
CROWN: LORBRENA in first-line ALK-positive advanced NSCLC
The seven-year CROWN update is one of the strongest long-term targeted therapy datasets in advanced solid tumors.
In previously untreated ALK-positive advanced or metastatic NSCLC, LORBRENA showed a 55% probability of remaining alive without disease progression at seven years, compared with 3% for crizotinib. Median progression-free survival was still not reached, with a hazard ratio of 0.19, representing an 81% reduction in the risk of progression or death. Pfizer also reported a 94% reduction in the risk of intracranial progression.
The strategic meaning is clear: for some molecularly defined lung cancers, long-term disease control is now a realistic expectation. The CROWN data also reinforce the commercial value of CNS penetration and durable intracranial control in ALK-positive NSCLC.
HARMONi-6: ivonescimab plus CT in first-line squamous NSCLC
HARMONi-6 is important because it was not simply another chemo-immunotherapy trial.
Ivonescimab, a PD-1/VEGF bispecific antibody, plus chemotherapy was compared directly with tislelizumab plus chemotherapy in previously untreated advanced squamous NSCLC. The study showed median overall survival of 27.89 months versus 23.69 months, with a hazard ratio of 0.66. The 24-month overall survival rates were 64.7% versus 48.6%.
This matters because the comparator was an active PD-1 plus chemotherapy regimen, not chemotherapy alone. If confirmed in global studies, HARMONi-6 could challenge the current PD-1/chemotherapy paradigm and accelerate interest in PD-1/VEGF bispecific antibodies.
PROTEUS: ERLEADA before/after surgery in high-risk localized PC
PROTEUS tested perioperative ERLEADA plus androgen deprivation therapy in newly diagnosed high-risk localized or locally advanced prostate cancer undergoing radical prostatectomy.
The trial met both primary endpoints. Pathological complete response or minimal residual disease was 8.9% versus 1.0%, and metastasis-free survival improved with a hazard ratio of 0.80. Five-year metastasis-free survival was 78.2% versus 73.5%. Time to subsequent therapy was also extended to 74.2 months versus 41.5 months.
This trial is important because it brings systemic intensification into the curative-intent surgical setting. The effect size is not spectacular, but the paradigm shift is meaningful: high-risk localized prostate cancer may need earlier systemic control, not only salvage treatment after recurrence.
KEYNOTE-A39: PADCEV plus KEYTRUDA in 1L advanced urothelial cancer
KEYNOTE-A39 / EV-302 confirmed the durability of PADCEV plus KEYTRUDA in previously untreated locally advanced or metastatic urothelial carcinoma.
With 42.8 months median follow-up, median overall survival was 33.6 months with PADCEV plus KEYTRUDA versus 15.9 months with chemotherapy, with a hazard ratio of 0.53. The 3.5-year overall survival rate was 44.0% versus 24.6%. Objective response rate was 67.5% versus 44.2%, and complete response rate was 30.4% versus 14.5%.
This is now one of the clearest examples of an antibody-drug conjugate plus immunotherapy combination replacing platinum chemotherapy as the central first-line standard. The long-term data strengthen confidence in durability, although neuropathy and treatment management remain important in real-world practice.
LIBRETTO-432: RETEVMO in RET fusion-positive early-stage NSCLC
LIBRETTO-432 extends precision oncology into curative-intent lung cancer.
The study enrolled patients with resected stage IB-IIIA RET fusion-positive NSCLC and randomized them to adjuvant RETEVMO or placebo. The trial reported a statistically significant event-free survival benefit and is positioned alongside ADAURA in EGFR-mutant disease and ALINA in ALK-positive disease.
The key strategic point is testing. If RET-targeted adjuvant therapy becomes standard, molecular profiling at diagnosis and resection becomes even more important. This is another example of the metastatic precision oncology model moving into early-stage disease.
NATALEE: KISQALI plus endocrine therapy in HR , HER2- early BC
NATALEE continued to support adjuvant KISQALI plus a nonsteroidal aromatase inhibitor in HR-positive, HER2-negative early breast cancer.
At a median follow-up of 55.4 months, the 36-month invasive disease-free survival rate was 90.8% with KISQALI versus 88.0% with aromatase inhibitor alone. The 60-month invasive disease-free survival rate was 85.5% versus 81.0%. The broader eligibility criteria included high-risk node-negative patients, where KISQALI showed a hazard ratio of 0.606.
The commercial and clinical question is not whether CDK4/6 inhibition works in early breast cancer, but which patients should receive it. NATALEE broadens the addressable population, but also raises familiar questions around access, toxicity, treatment duration and patient selection.
IMvigor011: TECENTRIQ guided by ctDNA in bladder cancer
IMvigor011 is one of the most conceptually important trials on the list.
In muscle-invasive bladder cancer after surgery, serial ctDNA testing was used to identify molecular residual disease. ctDNA-positive patients randomized to TECENTRIQ had median disease-free survival of 9.9 months versus 4.8 months with placebo, and median overall survival of 32.8 months versus 21.1 months. Persistently ctDNA-negative patients had excellent outcomes, with 88% disease-free survival at two years.
This trial may prove influential beyond bladder cancer. It supports a future in which adjuvant therapy is not given simply because clinical risk is high, but because molecular residual disease is detected. That is a major shift in how oncology treatment could be personalized after curative-intent surgery.
SARC041: VERZENIO in dedifferentiated liposarcoma
SARC041 is notable because it is the first positive phase 3 trial ever reported in dedifferentiated liposarcoma.
VERZENIO improved median progression-free survival to 9.7 months versus 1.5 months with placebo, with a hazard ratio of 0.38. Six-month progression-free survival was 60% versus 22%, and 12-month progression-free survival was 39% versus 13%. Median overall survival was not reached versus 25.5 months, with an overall survival hazard ratio of 0.55, despite high crossover from placebo to VERZENIO.
The response rate was modest, but that is not the main point. In this disease, durable disease control is clinically meaningful. SARC041 may establish CDK4/6 inhibition as a real treatment option in a rare sarcoma subtype where systemic standards have been weak.
KEYNOTE-564: KEYTRUDA in adjuvant clear-cell RCC
KEYNOTE-564 remains one of the most important adjuvant immunotherapy datasets in kidney cancer.
The trial evaluated KEYTRUDA after nephrectomy in patients with clear-cell renal cell carcinoma at increased risk of recurrence. Earlier analyses established KEYTRUDA as the first adjuvant regimen to significantly improve both disease-free survival and overall survival versus placebo after surgery. Reported outcomes include disease-free survival hazard ratio of 0.71 and overall survival hazard ratio of 0.66.
At ASCO 2026, the focus shifted toward ctDNA analysis in KEYNOTE-564, exploring whether molecular residual disease could help identify patients at highest risk of recurrence and potentially refine adjuvant treatment decisions.
This is strategically important because KEYNOTE-564 is no longer only a positive adjuvant immunotherapy trial. It is now part of the broader question of how to personalize adjuvant treatment in renal cell carcinoma. If ctDNA can help distinguish patients who truly need treatment from those who may be safely observed, it could reshape future trial design, treatment selection and health-economic modelling in kidney cancer.
See attached Summary Table of Key Trial Results from ASCO 2026
Strategic interpretation
Several patterns stand out. First, ASCO 2026 strongly reinforced the move into earlier disease. PROTEUS, LIBRETTO-432, NATALEE, IMvigor011 and KEYNOTE-564 all address treatment before overt metastatic relapse. The future oncology battleground is increasingly the prevention of recurrence, not only treatment after recurrence.
Second, molecular selection is becoming embedded across the disease continuum. RET fusions in early NSCLC, ALK in metastatic NSCLC, ctDNA in bladder cancer and renal cell carcinoma, RAS in pancreatic cancer and CDK4 biology in liposarcoma all show the same direction of travel: treatment value depends on identifying the right patients at the right time.
Third, ADCs and bispecific antibodies are now challenging major standards. PADCEV plus KEYTRUDA has transformed first-line urothelial cancer. Ivonescimab may challenge PD-1 plus chemotherapy in squamous NSCLC if global data confirm the China results.
Fourth, rare tumors are no longer peripheral. SARC041 shows that prospective data in rare cancers can still change practice, even when the commercial story is smaller than in lung, breast, prostate or kidney cancer.
© Robert F. Siegmund, PhD MBA | Life Code GmbH
I deliver strategic insights and product forecasting models to biopharma companies across the product lifecycle. Reach out to me!

3
23
53
3,846
Jun 2
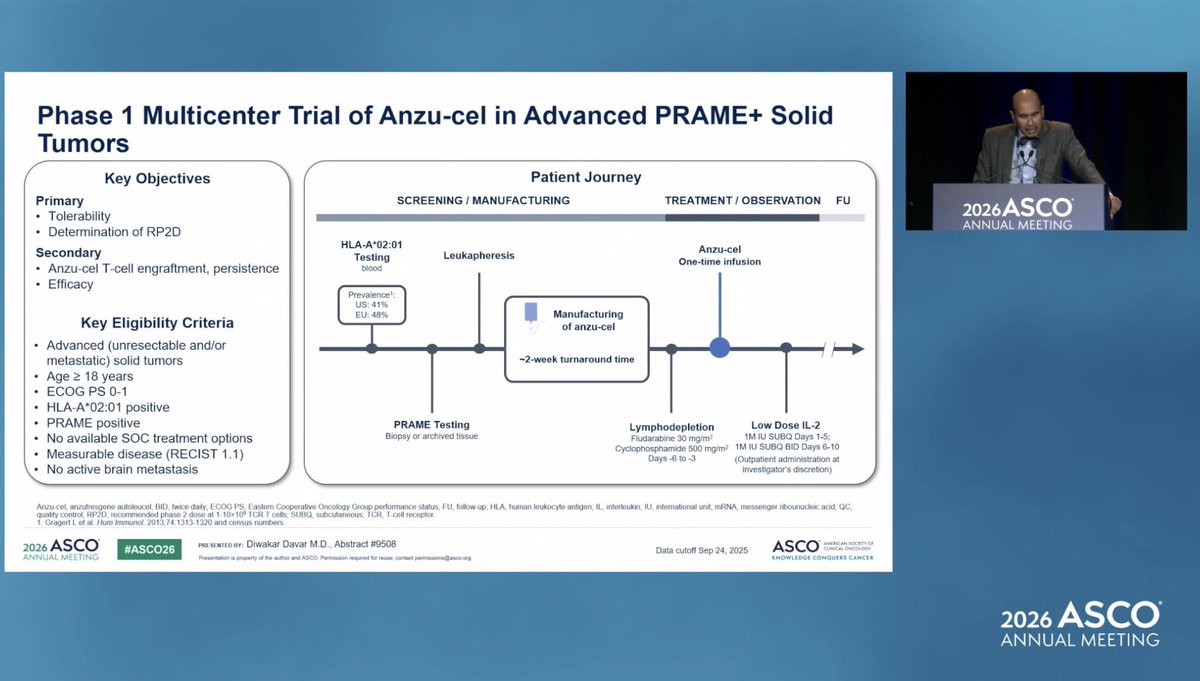
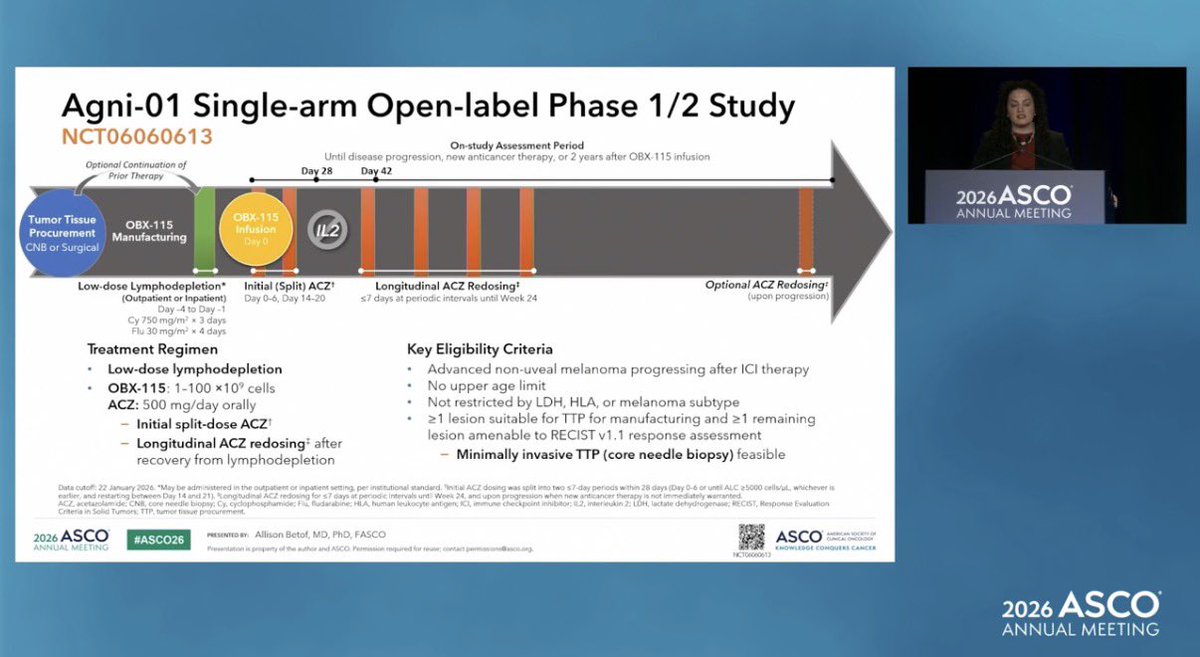
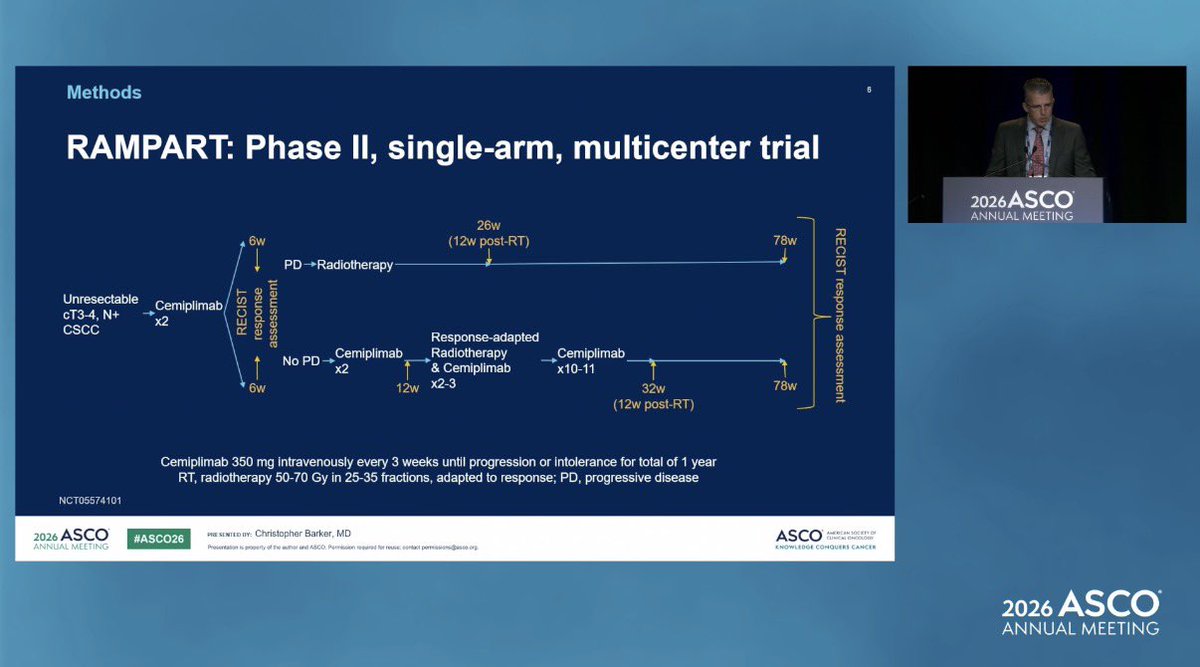
👋🏼 After covering my #ASCO26 Top 10 melanoma studies, one thing feels clear: the future is personal!!!!
🎯 Personalized vaccines
🎯 Next-generation TILs
🎯 PRAME-targeted TCR therapies
🎯 Smarter neoadjuvant IO
Different approaches. Same goal: helping more patients live longer and better.
Thank you to the amazing @OncoAlert community, and especially to @weoncologists for the mentorship, inspiration, and countless lessons along the way 🙏
I came to #ASCO26 looking for answers. I’m leaving with even better melanoma questions 🖤
The science was inspiring…but people behind it even more @OncoAlert 📡
@DrChoueiri 🇺🇸
@hoperugo 🇺🇸
@matteolambe 🇮🇹
@TiansterZhang 🇺🇸
@CathyEngMD 🇺🇸
@stolaney1 🇺🇸
@montypal 🇺🇸
@tompowles1 🇬🇧
@brian_rini 🇺🇸
@cdanicas 🇪🇸
@NiuSanford 🇺🇸
@amerseburger 🇩🇪
@GlopesMd 🇺🇸
@Icro_Meattini 🇮🇹
@PGrivasMDPhD 🇺🇸
@DrYukselUrun 🇹🇷
@nataliagandur 🇦🇷
@ElisaAgostinett 🇧🇪
@HHorinouchi 🇯🇵
@realbowtiedoc 🇺🇸
@to_be_elizabeth 🇮🇹
@UOzkerim 🇹🇷
@p_ciracimd 🇮🇹
@DrVilmaPBarcia 🇪🇸
@DraMartinezLago 🇪🇸
@DrMirallas 🇺🇸
@GaiaGriguolo 🇮🇹
@scocmem 🇬🇧
@AmandaNizamMD 🇺🇸
& @weoncologists 🇺🇸
9
19
1,952