
137 Photos and videos





Max Kates retweeted

Jun 9
Women's #BladderCancer program addresses sex-specific gaps in care and research. @akfsurgeon @brady_urology joins @TiansterZhang @UTSWMedCenter to discuss the Women's Bladder Cancer Program at @sibleyonline, a multidisciplinary initiative integrating urology, medical oncology, gynecology, social work, and physical therapy with female-specific quality-of-life questionnaires. #WatchNow on UroToday > bit.ly/4t72gXv

5
8
685

Incredible Commitment to Cancer Research by @davidjtrone. Trone Family Division of Urologic Oncology will be a place to accelerate innovation and progress for cancer patients everywhere. giving.jhu.edu/story/brady-u…. @brady_urology
Jun 10

🎉 Big news at @brady_urology! Deeply grateful for a transformational gift to establish the Trone Family Division of Urologic Oncology under leadership of @MaxKates! Honored & Inspired by @davidjtrone to "move the needle towards better cancer outcomes" giving.jhu.edu/story/brady-u…

1
4
37
3,021
Max Kates retweeted

Jun 10
🎉 Big news at @brady_urology! Deeply grateful for a transformational gift to establish the Trone Family Division of Urologic Oncology under leadership of @MaxKates! Honored & Inspired by @davidjtrone to "move the needle towards better cancer outcomes" giving.jhu.edu/story/brady-u…
1
6
45
6,808
Max Kates retweeted

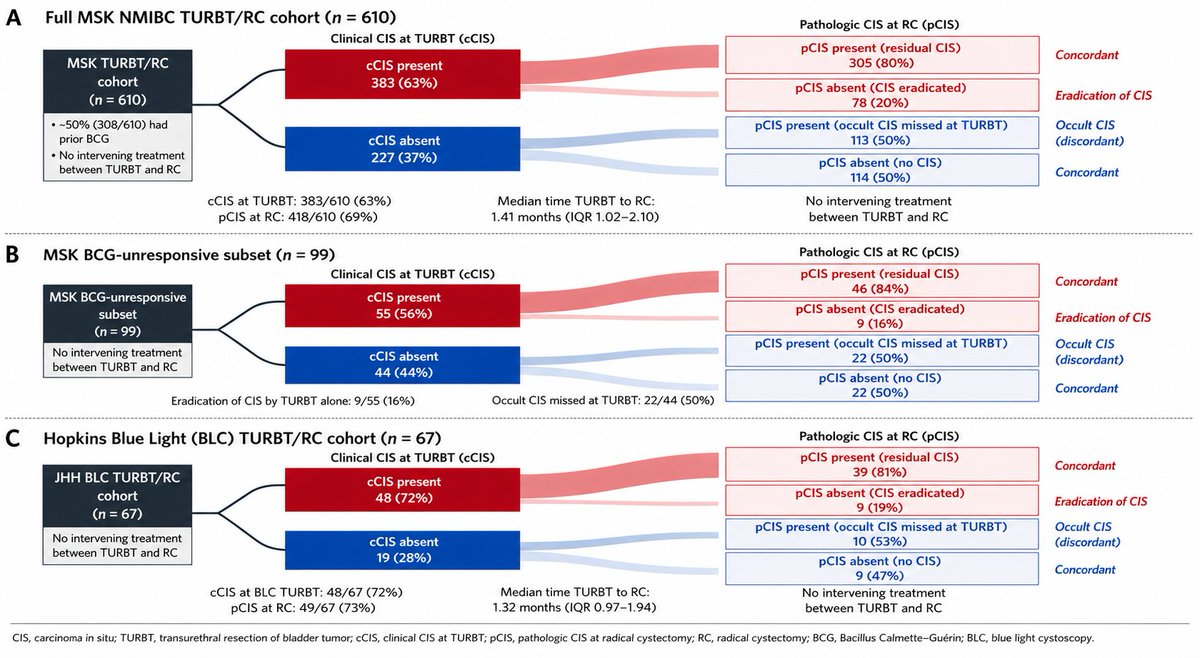
This effort lead by @DrAndrewKatims , former @UrologyMSK @SUO_YUO fellow now at @nymedcollege , first looked at 610 NMIBC patients treated with radical cystectomy without any intervening treatment after their pre-RC TURBT; across multiple NMIBC subsets (BCG-Naïve, BCG unresponsive, use of Narrow Band Imaging, etc) we found that ~20% of patients with CIS on pre-RC TURBT had no residual CIS within their cystectomy specimen & equally important was that ~50% without CIS on pre-RC TURBT had occult CIS within their cystectomy specimen.
We then partnered with @MaxKates & @Sadra_Sepehri to look at a NMIBC cohort who had blue light TURBT before cystectomy without intervening treatment @HopkinsGBCI @brady_urology and found nearly identical results; ~20% eradication of CIS by TURBT alone & ~50% occult CIS on cystectomy
n/3
1
2
7
825
Max Kates retweeted

(1/) A transformational $10 million gift from the Robert & Lynda Carter Altman Family Foundation, championed by actress, philanthropist, & devoted advocate Lynda Carter, has made possible the naming & advancement of the Robert Altman Division (RAD) of Minimally Invasive Surgery.



4
22
123
8,367
Big congrats our BCAN Quale Fellows. And thank you to all the reviewers in this incredibly competitive application cycle We are fortunate to be in a golden age of bladder cancer progress. Thrilling to see that we are able to recruit such talent to the field.
@BladderCancerUS

Congratulations to the 2026 John Quale Travel Fellowship recipients! We are proud to support the next generation of bladder cancer researchers and clinicians as they join us at the 2026 Bladder Cancer Think Tank. Your dedication to advancing bladder cancer research will help shape the future of patient care. @UofCalifornia @MSKCancerCenter @WeillCornell @Yale @theNCI @UW @MoffittNews @UHhospitals
1
7
28
2,297
Interesting thought experiment. If you take the 5% absolute difference in RFS, and instead give BCG IO as reinduction after the 10% of all patients recur at 3mo, would you get same benefit of IO and limit toxicity/over treatment? @WesKassouf @UroDocAsh
May 29

Agree. The other question is does combo therapy for all outperforms sequential therapy for only some ( ie bcg for hr-nmibc then IO upon HG recurrence). I have not yet seen convincing data to suggest outcomes would be different between the two approaches
3
8
2,868
Max Kates retweeted

May 29
Agree. The other question is does combo therapy for all outperforms sequential therapy for only some ( ie bcg for hr-nmibc then IO upon HG recurrence). I have not yet seen convincing data to suggest outcomes would be different between the two approaches

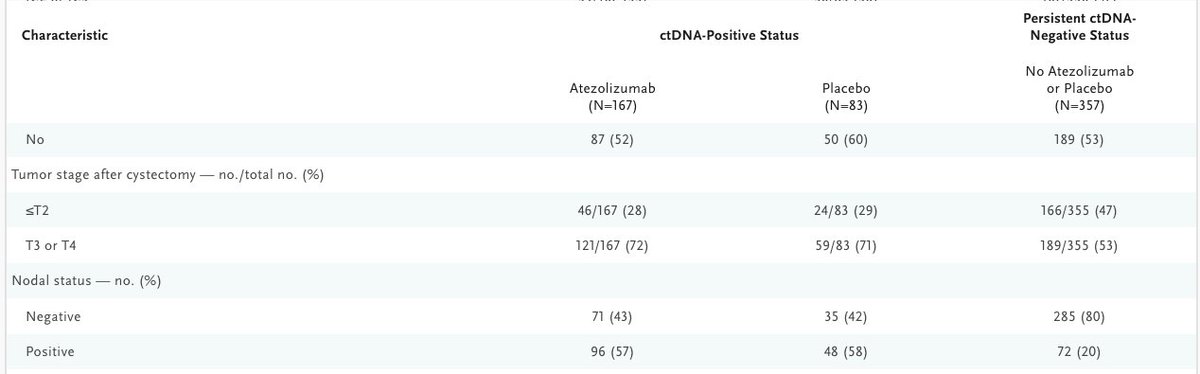
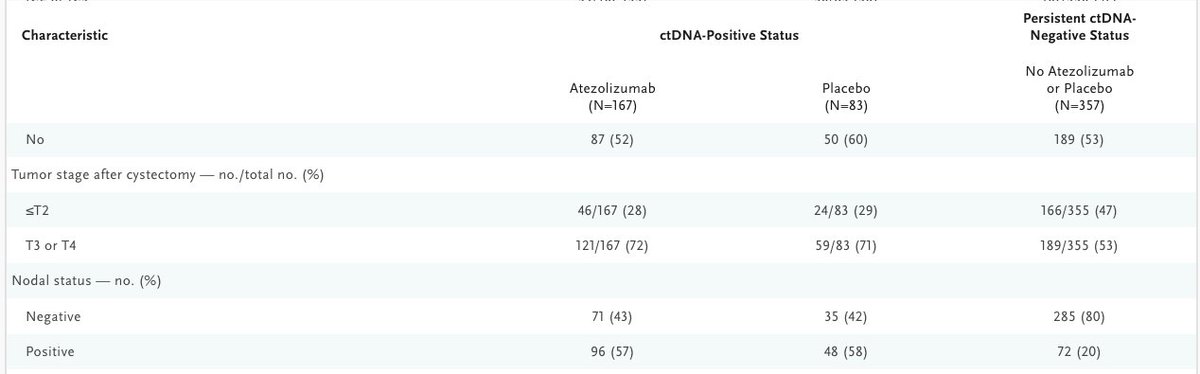
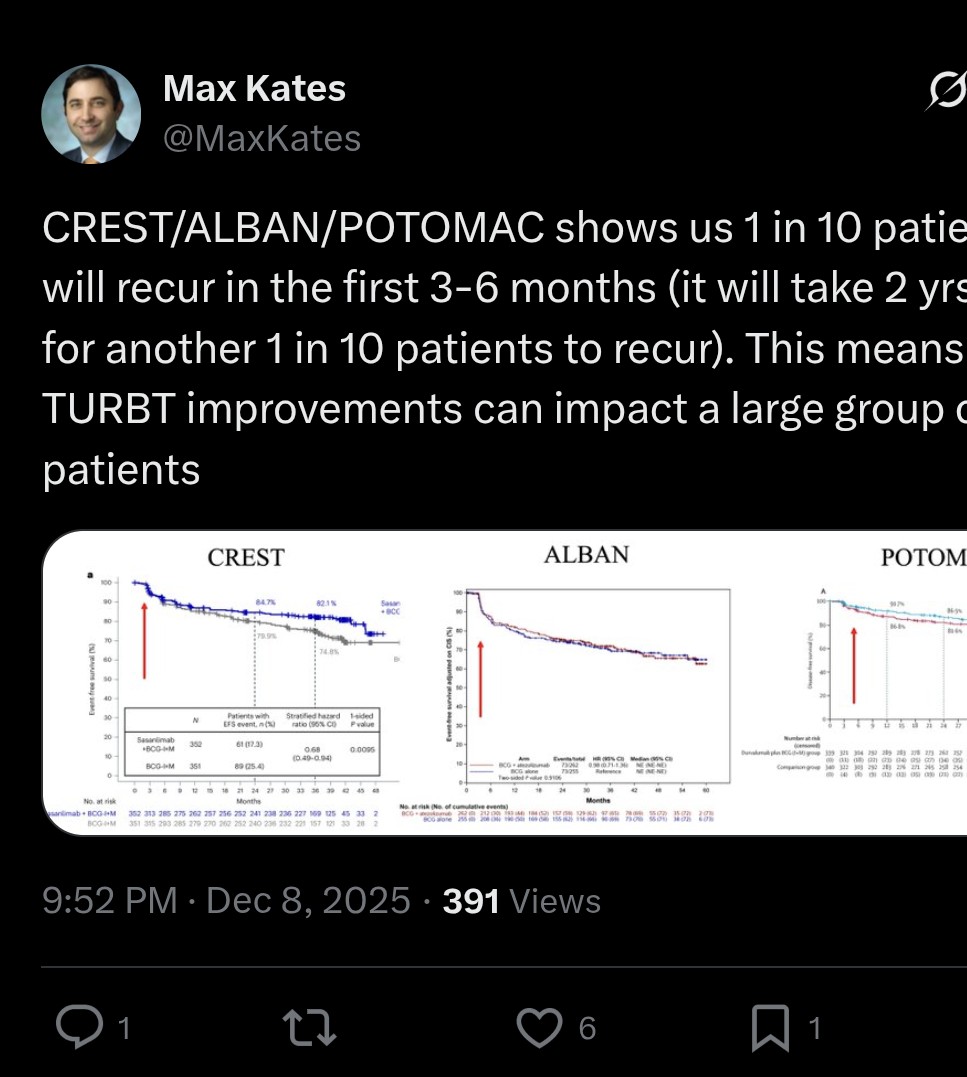
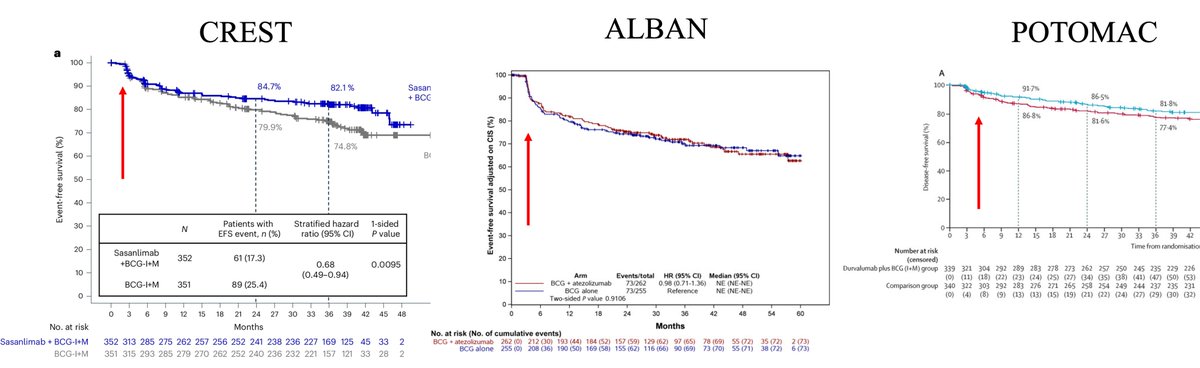
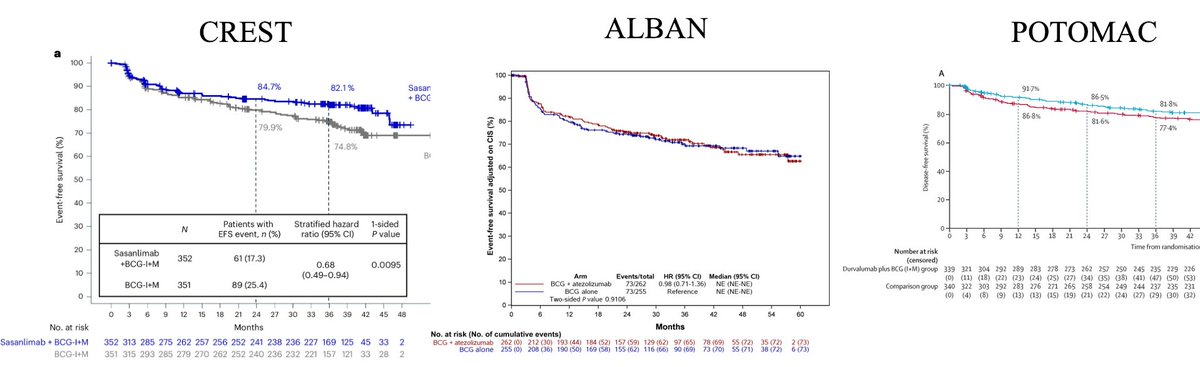
📐 HR 0.68 = a 32% relative risk reduction in recurrence at any given moment during follow-up.
That sounds like a large benefit.
But the absolute numbers tell a different story:
BCG alone: 81.6% disease-free at 2 years
BCG durvalumab: 86.5% disease-free at 2 years
Absolute difference: ~5%
Since BCG already works well, a big relative reduction maps to a modest absolute gain. @MaxKates @UrogerliMD @JoshMeeks
1
5
3,459
1) Approval based on marginal improvements in efficacy (without improvement to CSS/OS)
2) Toxicity that isn't G5 (death) doesn't seem to impact approval. 10-15% serious autoimmune AEs in NMIBC is deemed ok
3) little weight given to efficacy vs toxicity balance of a drug
May 28

#FDA approves a treatment for high-risk non-muscle invasive bladder cancer. fda.gov/drugs/resources-info…
ALT FDA announcement that reads FDA approves a treatment for high-risk non-muscle invasive bladder cancer
3
7
14
3,608
4. Any NMIBC patient I am considering for early cystectomy i think reasonable to consider BCG IO if patient wants bladder preservation
5. Trials didn't address who is highest risk, but we know multifocal HGT1 w/CIS is the bad actor so these folks who may benefit. Time will tell
1
3
457
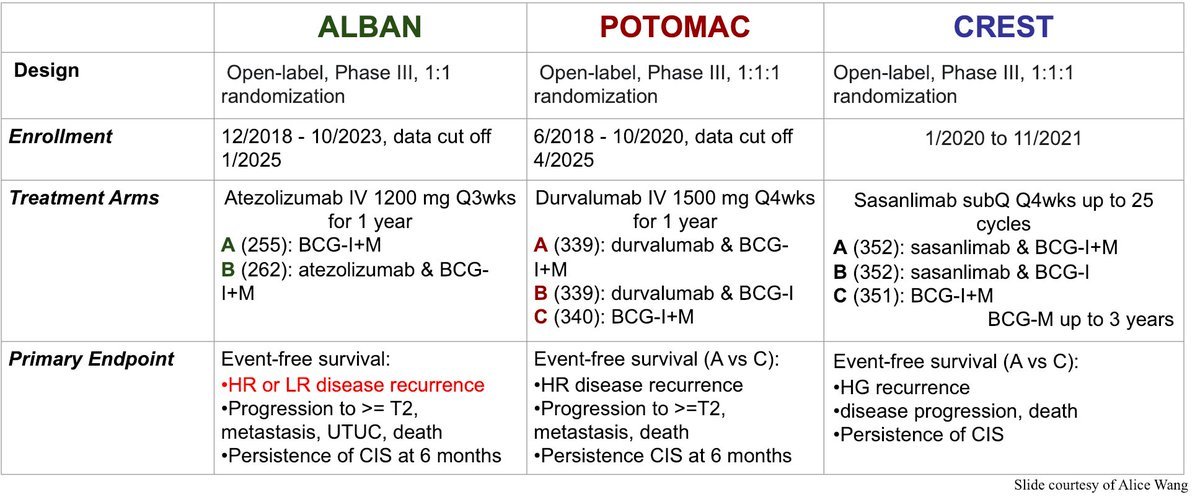
6. Finally, we need to better understand why Alban was negative, CREST was marginally positive but company pulled FDa registration for now (unclear exactly why) & POTOMAC approved based on marginal improvements
7. Multiple trials in same space force us to interpret collectively
4
293
Max Kates retweeted

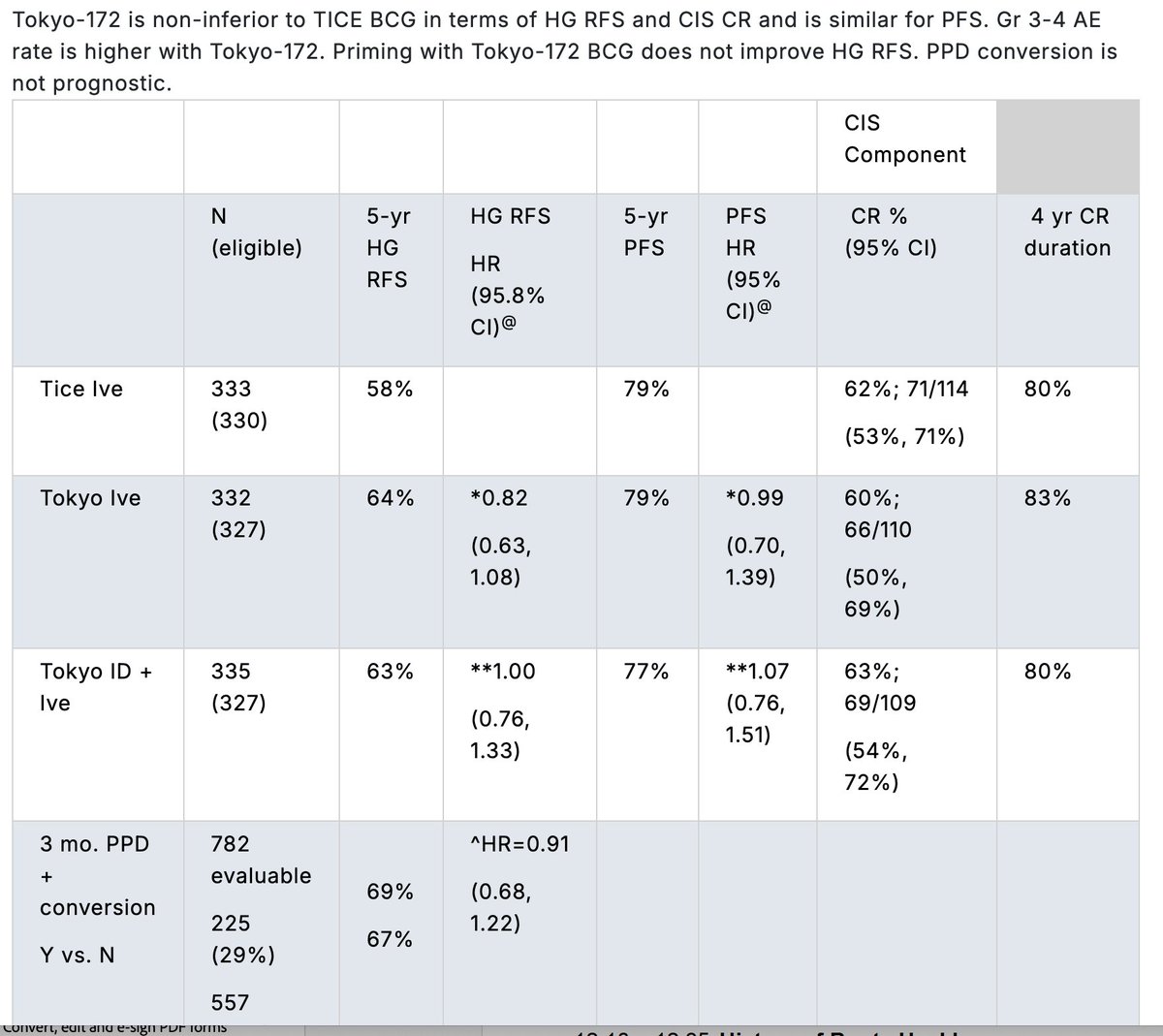
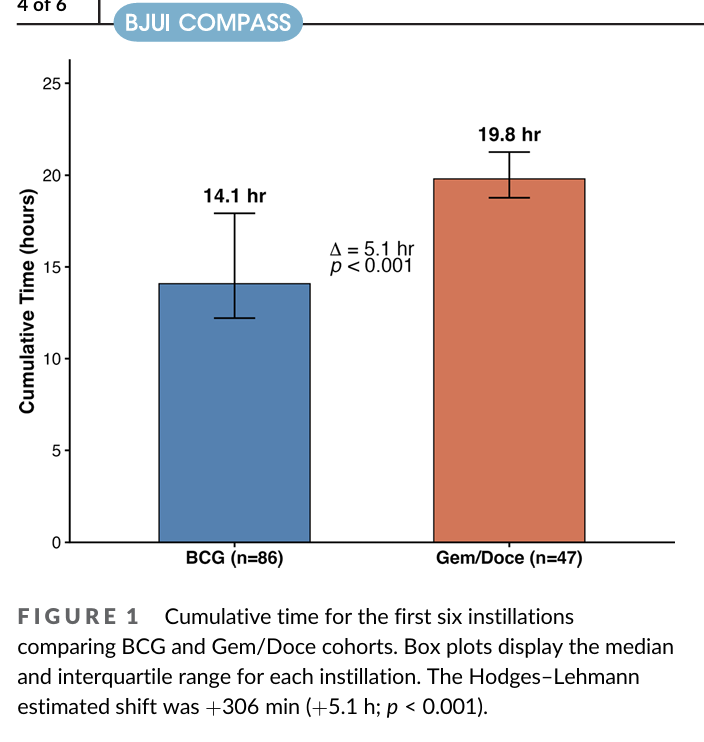
If BRIDGE shows non-inferiority (I think likely)... need to choose treatments in real world. One of main issues if Gem/Doce is logistics, especially in community.
But there is also a time burden on the patient which can impact shared decision making
pubmed.ncbi.nlm.nih.gov/4214…
1
2
16
1,771
Max Kates retweeted

Marianna Zahurak • @MaxKates • Michael Goldstein • @nirmishsingla • Noah Hahn • @noel_onika • Roy Elias • @Imaging4Health • Stephanie Russell •
@SHPatelMD1 • Tamara Lotan
@brady_urology @hopkinskimmel
1
4
238
Max Kates retweeted
Aditya Halthore • @Andres_Matoso • @akfsurgeon • Rusty Johnson • @cjvand • Daniel Song • Dorothy Davis • Dorothy Rosenthal • Ezra Baraban • @JCensits • @jonathandudley • Jun Luo • Kalli Veldman
1
1
5
214
Max Kates retweeted
Collaboration in Action!
Our Working Groups bring together multidisciplinary experts committed to advancing bladder cancer research and care. Together, we’re tackling the most pressing challenges and turning ideas into impact.
Stay tuned to learn more about the people/progress
1
2
5
260
Max Kates retweeted
View our schedule for the final day of #AUA26!
Thank you to everyone from @brady_urology who presented, attended, and contributed to the #AUA26 Annual Meeting!
You can find our full AUA schedule and more resources for clinicians here: hopkinsmedicine.org/clinical…
1
1
4
385
Max Kates retweeted

May 15
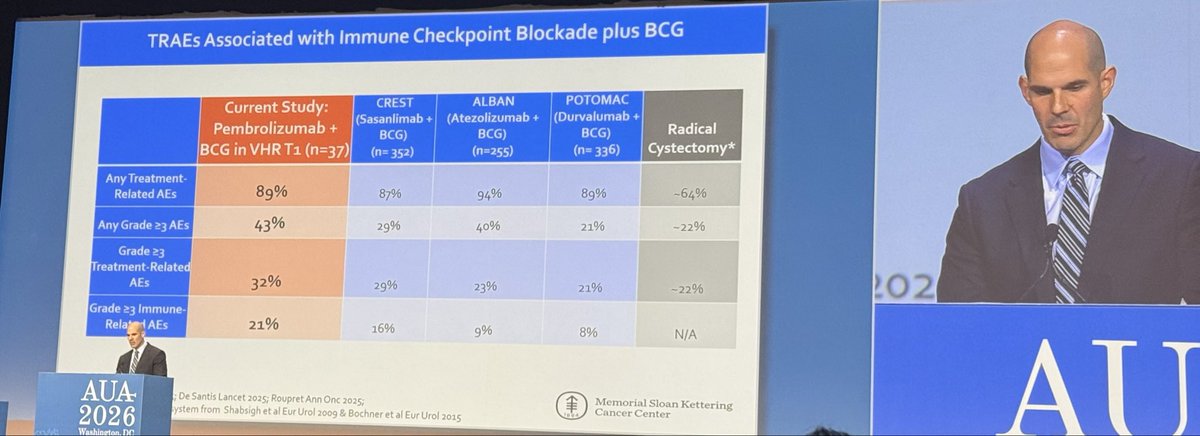
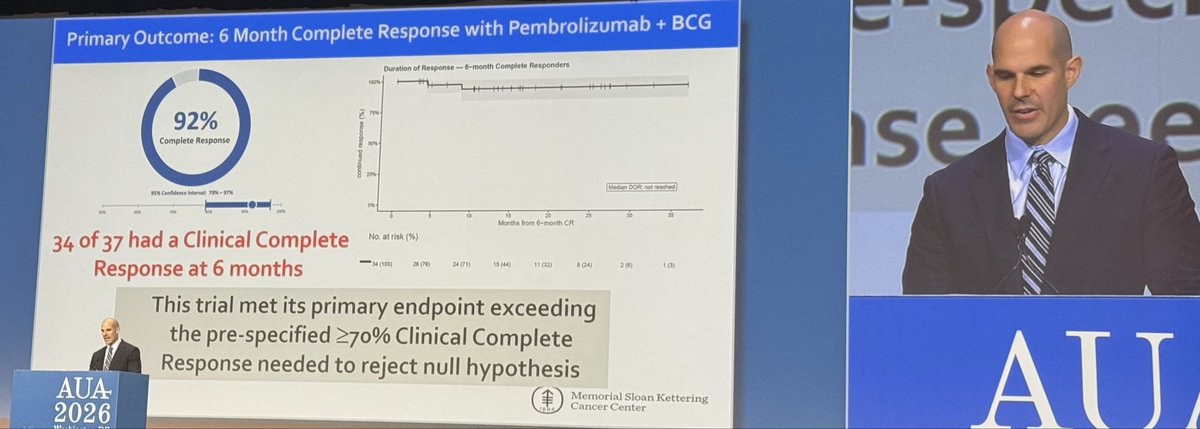
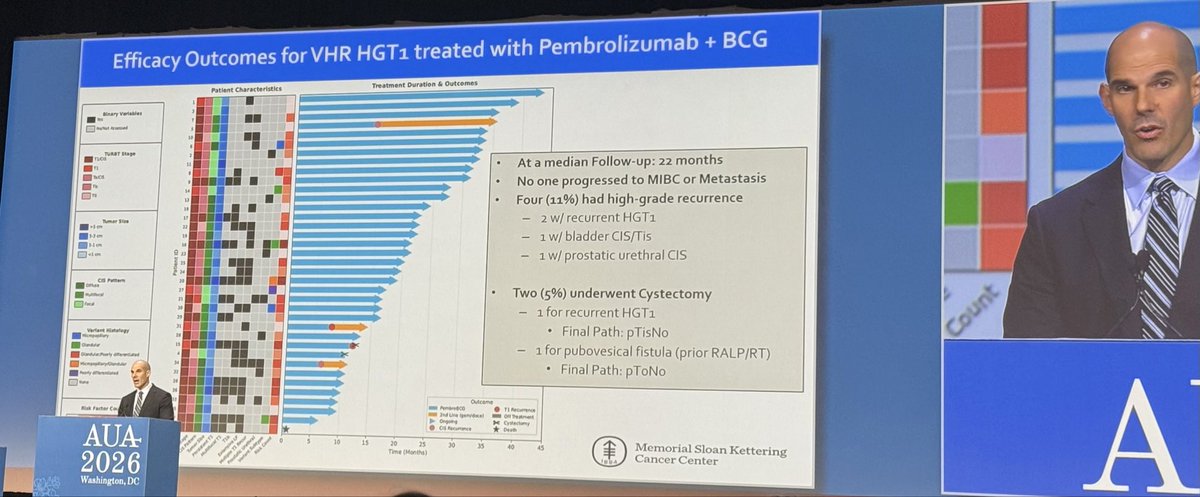
@eugene_pietzak incrediblely elegant P2 on bcg Pembro in VHR T1. 92% response, 94% RC- free. 1 early death and 21% iAEs. n=37 but great job to consider risk - based strategy. #AUA26
7
14
4,994

Max Kates retweeted
We have a full day on Saturday for #AUA26! Preview our afternoon schedule.
View all of our sessions here: hopkinsmedicine.org/clinical…


1
1
5
452