
NextMed.Health is a cross-disciplinary program & community from across #healthtech & biomedicine reimagining the future of health & biomedicine.
Joined February 2011
- Tweets 11,457
- Following 3,104
- Followers 26,424
- Likes 8,418
1,479 Photos and videos











Pinned Tweet

5 Apr 2025
Massive thanks to everyone who came together to make NextMed.Health 2025 a magical gathering of innovators and changemakers at the interface of technology healthcare and the human spirit.
#NextMedHealth



1
4
11
2,786
Jun 4
A team of more than 80 researchers working across four continents have identified a set of proteins in the blood that accurately predict lung cancers more than 5 years before diagnosis.
also early evidence that an existing anti-inflammatory drug could significantly reduce lung cancer risk in people with elevated concentrations of these proteins, linked to inflammation.
nytimes.com/2026/06/04/well/…
1
4
7
617

Jun 1
In a small, preliminary study, an experimental gene-editing treatment targeting PCSK9 dramatically lowered cholesterol levels, perhaps permanently, after just one infusion…
nytimes.com/2026/05/25/healt…
3
443
May 31
A pancreatic cancer drug more than four decades in the making has cracked one of the most stubbornly lethal cancers, extending people’s lives and keeping their tumors in check for twice as long as those on regular chemotherapy. @ASCO
washingtonpost.com/health/20…
1
155
NextMed Health retweeted

May 28
Gamification of health
The Vitality program from life insurance company @JohnHancockUSA rewards policyholders with points for healthy behaviors such as going to the gym, buying healthy foods, tracking sleep, getting preventive screenings
npr.org/2026/05/25/nx-s1-582…
1
2
5
501
May 24
A blood-based biological aging score was linked to significantly higher dementia risk in a study of more than 223,000 adults, with the strongest association seen for vascular dementia.
studyfinds.com/blood-age-dem…
5
5
686
NextMed Health retweeted

May 19
A big day for multi-agent AI to accelerate biomedical discovery, hypothesis generation, designing experiments with proof points of new candidate drugs (cancer, fibrosis, macular degeneration, antimicrobial resistance, and more)
2 @Nature reports @GoogleDeepMind @FutureHouseSF
nature.com/articles/s41586-0…
nature.com/articles/s41586-0…
14
146
533
157,647
May 20
Co-Scientist: A multi-agent AI partner to accelerate research
deepmind.google/blog/co-scie…
89
NextMed Health retweeted
The future of mental health isn't a single drug or app, it lies at the convergence of biomarkers, AI, and a real clinical team. I'm excited to see @MeruHealth Advanced, which is bringing that convergence to a category that has needed it for a long time.

I lost my brother Peter to suicide. Standard psychiatry failed him.
Today we launch Meru Health Advanced — the care model I wish he'd had.
For the next Peter.
2
1
10
1,042
NextMed Health retweeted

Check out our updated resource page on digital health accelerators, incubators and funding programs
HTTPS://digital.health/digit…
3
7
670
May 2
Augmenting clinicians with AI co-clinicians
Amazing work from @DeepMind_Health @alan_karthi et al.
deepmind.google/blog/ai-co-c…
4
3,168
NextMed Health retweeted

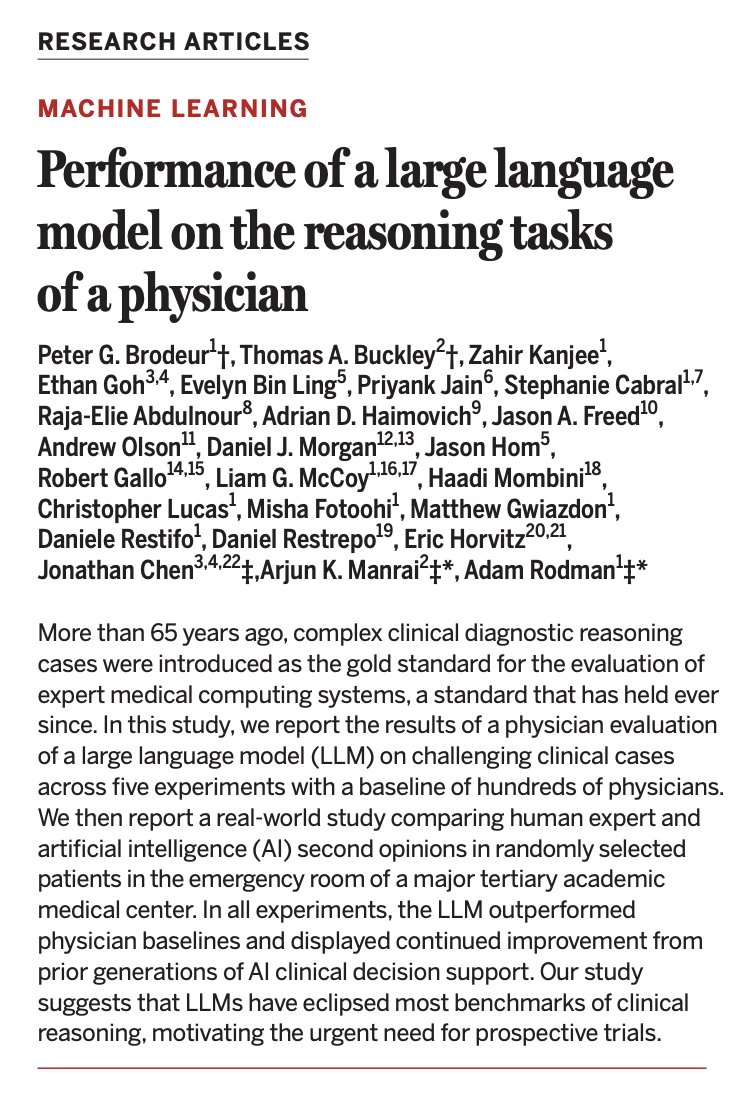
🧵1/ Our new study on AI and physician reasoning just came out in @ScienceMagazine. As co-senior author, I'm excited about our findings, and I do think AI will reshape medicine. But after seeing some of the discussions, I'm also worried about how our findings may be misinterpreted.
31
159
524
161,999
Apr 26
A new level of compatibility between electronic devices and living neural systems.
Engineers @NorthwesternU have created printed artificial neurons that go beyond imitation and can directly interact with real brain cells. These flexible, low-cost devices produce electrical signals that closely resemble those generated by living neurons, allowing them to activate biological brain tissue.
sciencedaily.com/releases/20…
3
7
602
NextMed Health retweeted
Apr 23
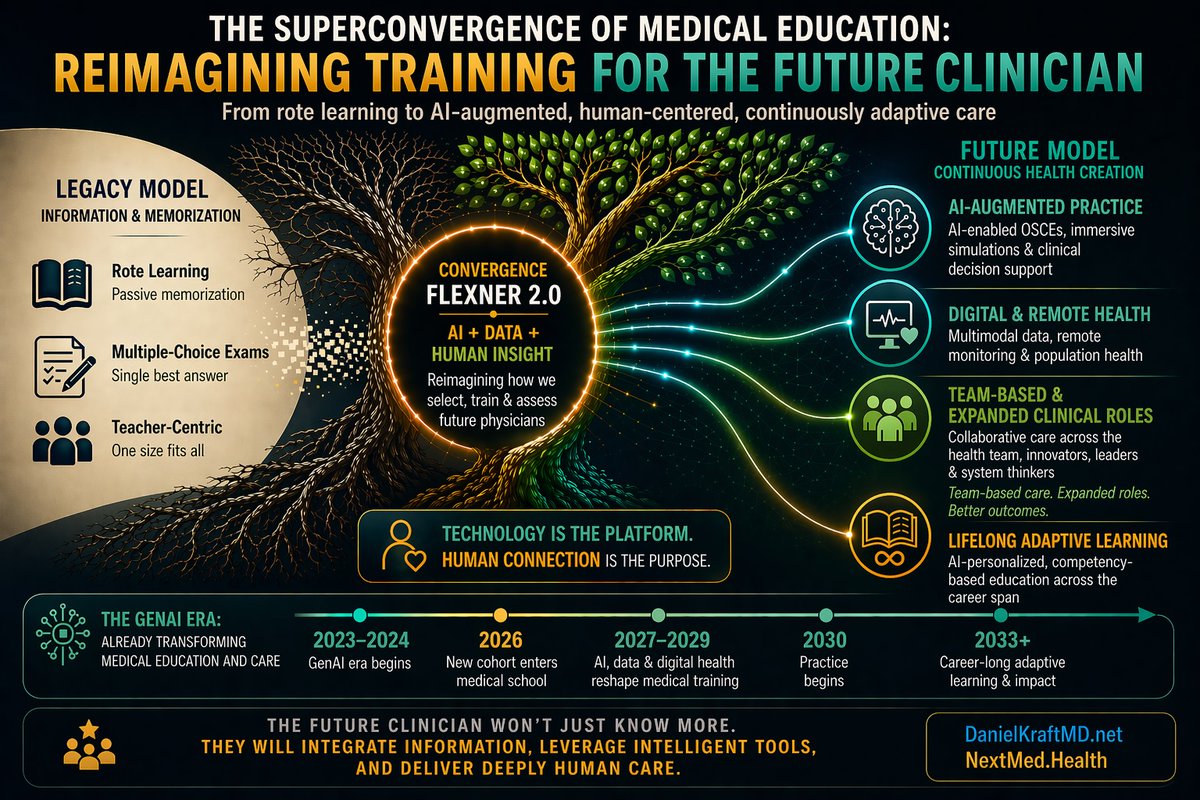
The future of medicine is arriving faster than our training models are evolving.
A student starting medical school in 2026 won’t earn their M.D. until 2030, and likely won’t finish residency or practice independently until 2033 or beyond. By then, the clinical and technological landscape will look dramatically different from the one many current curricula were designed for.
We are only a few years into the #GenAI era, and already medicine is being reshaped by multimodal data, AI-assisted decision support, remote patient monitoring, digital health, and new models of continuous, personalized care—not to mention agentic health and the growing direct-to-consumer shift in health(care).
So we need to ask some uncomfortable but necessary questions:
How should we be selecting future physicians?
What should they actually be trained to do?
And how should we evaluate readiness in a world where information is abundant, AI is increasingly capable, and human judgment matters more than ever?
I recently had the opportunity to keynote the leadership of the NBME, the organization behind the #USMLE exams that serve as a powerful “north star” for much of medical education. To their credit, NBME is proactively exploring the future of assessment and training. My message was simple: if the landscape of care is changing—with many clinicians already using AI to augment diagnostic and therapeutic decisions—the metrics we use to train and assess physicians, and clinicians more broadly, must evolve as well.
It’s time for a kind of Flexner Report 2.0.
That means moving beyond legacy training and assessment models toward medical education built for modern practice:
• Real-world assessment that reflects the complexity and ambiguity of actual care
• AI-enabled OSCEs and immersive simulations using virtual and augmented reality
• Fluency in AI, digital health, multimodal and real-world data, nutrition, prevention, and design thinking
• Training physicians not just to recall facts, but to synthesize information, ask better questions, use tools wisely, and deliver human care
• Preparing clinicians not only to manage disease, but increasingly to optimize healthspan across the lifespan
The key question is no longer just what we should add to the curriculum.
It’s also what we should stop teaching, streamline, or offload to technology to make room for what matters most.
Technology should not just be another subject in medical school. Increasingly, it will become part of the platform through which medicine is learned, practiced, and improved.
The future of healthcare will not belong to those who simply know the most facts. It will belong to those who can integrate data, leverage intelligent tools, adapt continuously, and still show up with empathy, wisdom, and human connection.
The transition is already underway. Are we ready to redesign medical education for the world ahead?
#MedEd
9
25
71
5,914
NextMed Health retweeted
Apr 22
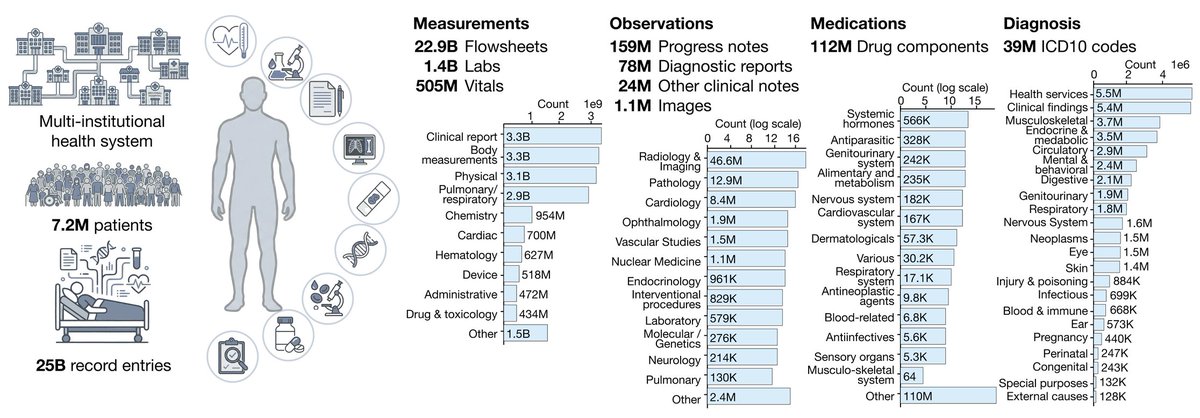
APOLLO: a multimodal temporal foundation model that learns to represent a patient’s entire medical journey in a single computational space.
By learning from millions of care trajectories, Apollo sees the future of each patient from their past.
Trained and evaluated on 25 billion medical records from 7.2 million patients, spanning 33 years of care across 28 clinical modalities and 12 major specialties. Labs, vitals, clinical notes, diagnostic reports, pathology and hematology images, medications, and diagnoses, all fed into a single model.
From @AI4Pathology et al.
arxiv.org/pdf/2604.18570
11
35
178
14,871
NextMed Health retweeted

Apr 18
The hill I will die on - we have to rethink graduate training.
“Scientists are trained for a world where data speaks for itself. Where misinformation moves slowly. Where scientific expertise naturally rises above noise. That world is gone.”
sciencepolitics.org/2026/03/…
55
232
839
104,619
Apr 17
Trump plans to ease access to psychedelics like psilocybin, ibogaine, MDMA
Cc @PaulStamets
wapo.st/41G8MZq
1
1
1
204
NextMed Health retweeted
Apr 17
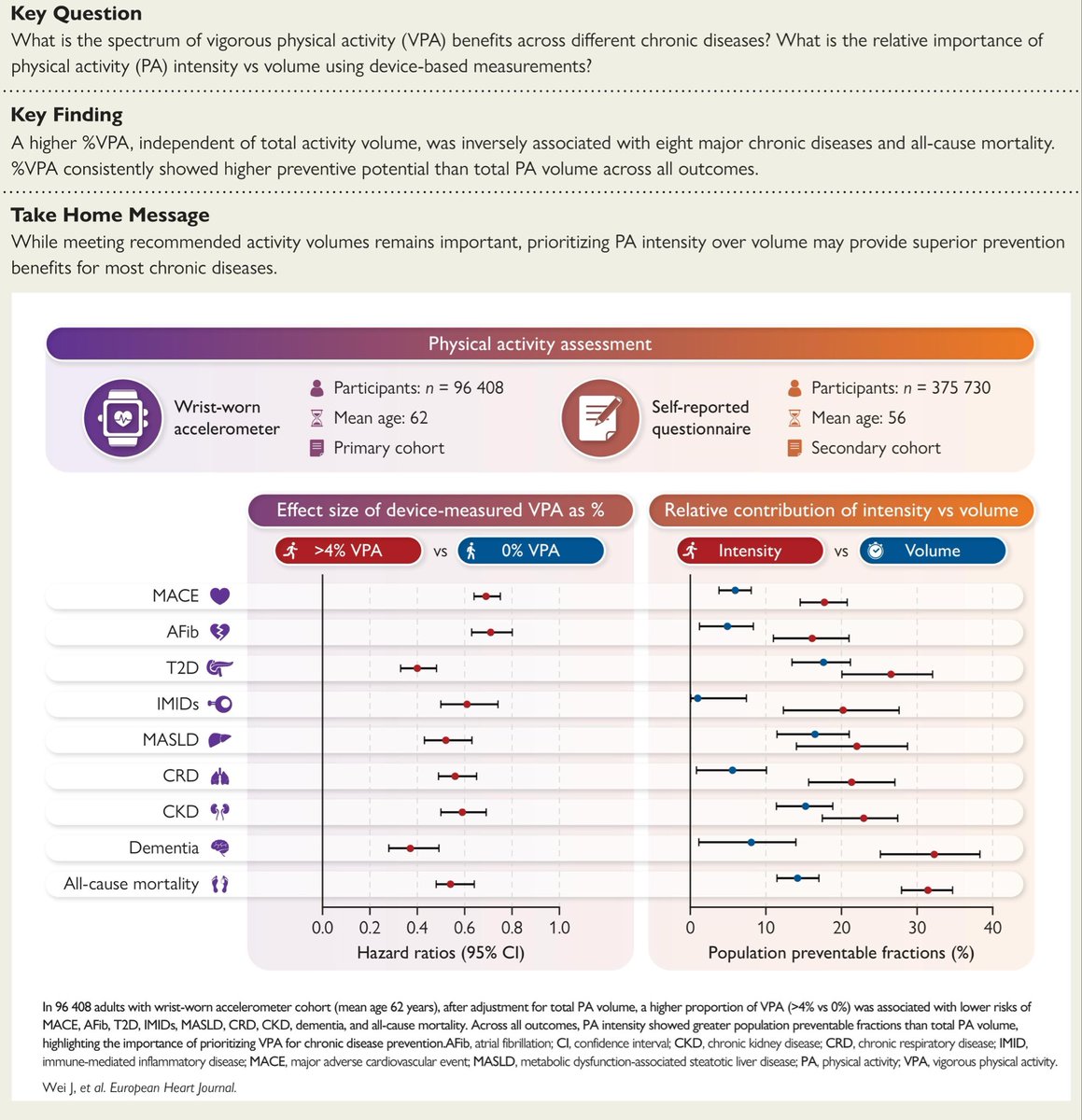
A new study published in the European Heart Journal found that a small amount of vigorous activity may be linked to lower risk of eight different chronic diseases.
academic.oup.com/eurheartj/a…
3
7
685
NextMed Health retweeted
Apr 10
"Sonogenics" is an emerging scientific field that uses ultrasound to non-invasively control and manipulate specific cells in the body, such as neurons or heart cells

Salk Institute scientist Shrek Chalasani has been awarded up to $41.3 million from ARPA-H to advance a breakthrough technology he pioneered, sonogenetics, which uses ultrasound to precisely control cells within the body.
This funding will help transform the Chalasani lab’s discovery into a potential noninvasive therapy for a range of conditions, including peripheral neuropathies. By enabling targeted control of mammalian cells without surgery, sonogenetics could redefine how we treat disease.
Learn more: salk.edu/news-release/salk-i…
#SalkInstitute #ARPAH #Sonogenetics #Neuroscience #BiomedicalInnovation
6
23
3,518
NextMed Health retweeted
Apr 12
The turning point for rare diseases, which affect >300 million people around the world.
A call to get rid of its many structural obstacles, to consider it as molecular surgery unlike drug treatments
gift link:
nytimes.com/2026/04/09/opini…
13
187
620
64,538