
|One does simply what one can in order to apply what one knows.|SWE at @microsoft|@matfyz Alum|petrroll.cz|Life stopped due to LC since July 22|
Joined March 2010
- Tweets 14,545
- Following 397
- Followers 591
- Likes 5,821
233 Photos and videos

Petr Houška retweeted

May 25
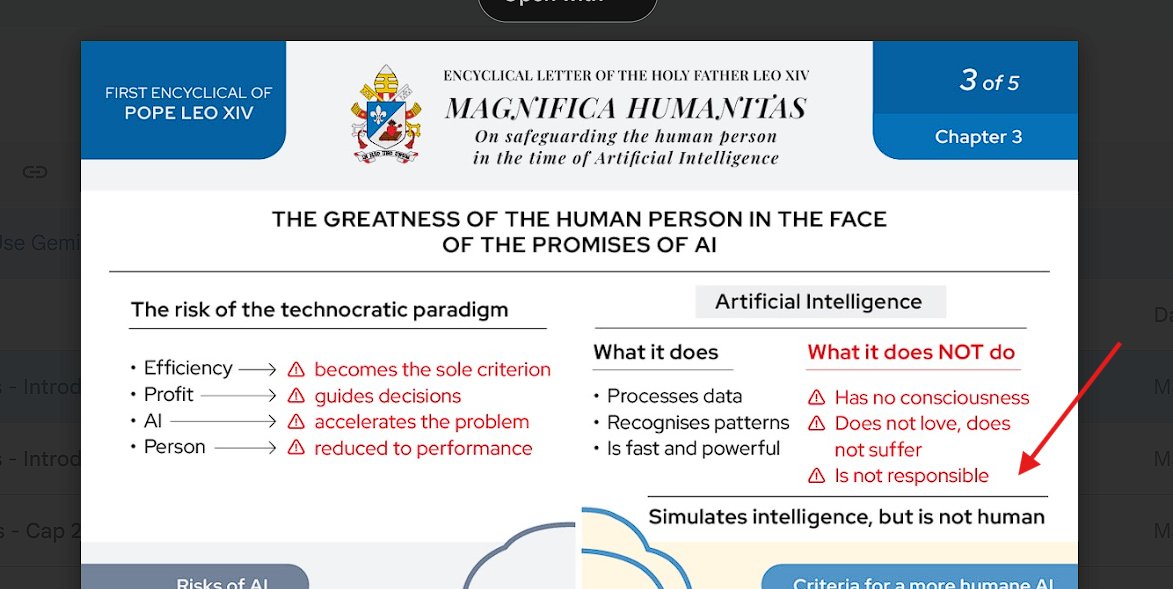
This passage from Leo's Encyclical is perfect. Perfect.

27
1,106
4,631
93,536
Petr Houška retweeted

May 23
The journey feels rather universal. At least for certain kind of people. What I, however, still struggle with (in myself and others) is how to apply the scepticism and how to not over apply it.
Some of the not great science etc is still directionally useful / correct
1
1
1
86
Petr Houška retweeted

May 12
The future of disease elimination lies in engineering. Not in a bazillion monoclonals. We can engineer out this constant disease spread w low indoor CO2, HEPA ventilation, far UVC, in combo w paid sick leave, normalized/free masks/tests, and airborne infx control in healthcare
2
99
365
5,283
May 15
@wtogami hi, I was wondering how you fed antics results to LLM. Just their .MD export or do you some processing? Do you feed it hierarchically by subgroup and extract findings and combine those or one large context?
*Very* interested in your system / approach / prompts.
2
141
May 15
(also, thanks for fedora <3)
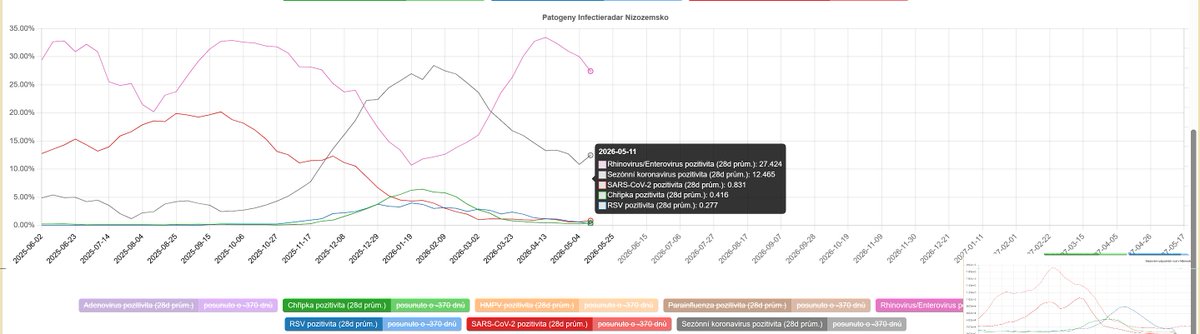
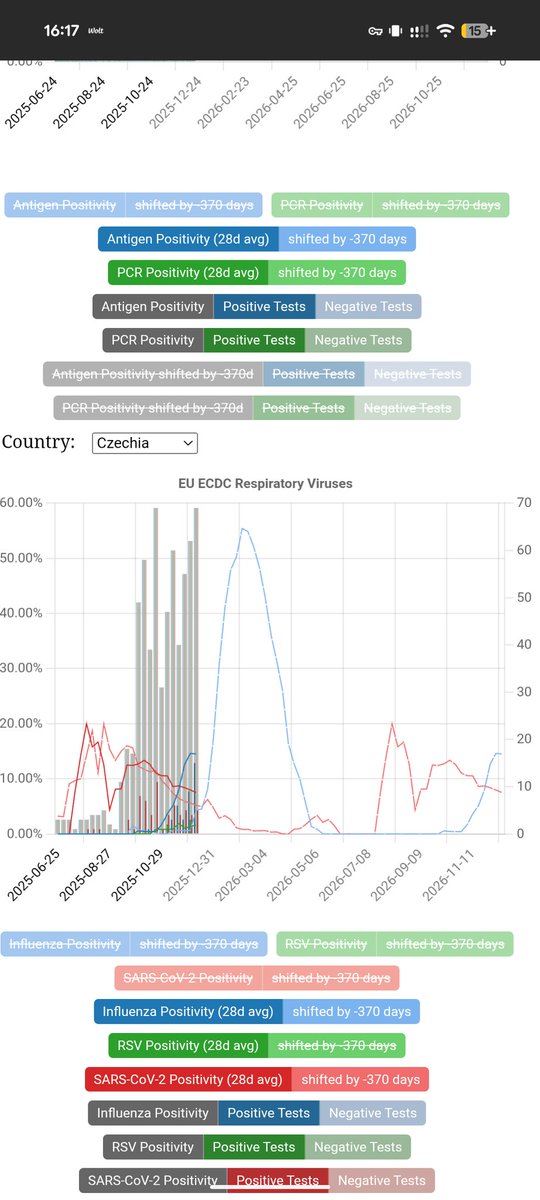
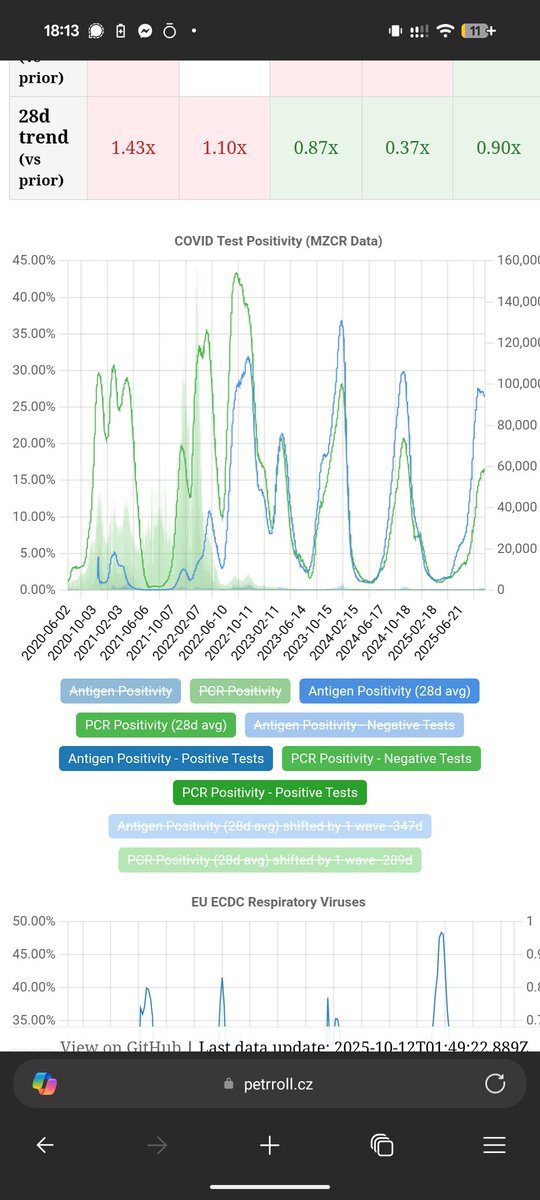
The reason why I'm asking is that I plan to add interpretation of markers also amatica to my local labs projekt github.com/petrroll/illdashb…
But knowing what already works would help a lot. :)
1
85
May 15
Being a high level person in rh (I suppose) I'd also love your thoughts on this: x.com/i/status/2054252949350…
May 12

I've been thinking about it some more, do you think a website with a official campaign smth like tech against LC & MECFS would help? Maybe make it interactive, ability to sign (name company idk, level).
Or even stats which company did most with ability to submit
78
May 11
It's not uncommon that big corpos donate to research of illnesses their employees have. I have been thinking a long time about trying to create a movement for LC & MECFS and big tech.
Some of us work there, many of us have friends there.
4
19
630
May 11
cc ^^ @clarejdaly @atranscendedman @DuaneStorey @grashalm_ ?@diannahaze @spoonless_me @cjmaddison @BlackHC (I know you're mostly recovered but hey), etc.
3
2
188
May 11
There is also finance director at google who's _child_ is affected. Can't remember his name tho.
1
1
125
May 11
I'm not cool enough to come up with a strategy myself. But I'd very much like to join in with folks and help do it.
Among just what I remembered we cover the biggest companies in the world.
1
116
May 9
Tady hezký shrnující vlákno vysvětlující že long COVID fakt není převážně psychosomatika. A "studie se vesměs shodují" je od lekare, pokud stále pracuje, v roce 2026 někde mezi hrubou neznalosti a aktivní ignoraci a ukázkou neschopnosti pracovat se zdroji.
(Už není 2022)
May 9
S prominutím absolutně netušíte, o čem mluvíte. Máte pravdu, že podle české odborné společnosti ano. Podle většiny studií *ani omylem*. Víte kolik stojí ty lidi neléčit?
(jen u mě, jen na ušlých daních miliony)
Pošlu summaries studií v impact časopisech, projdete
4
164
May 4
.@tangero IMHO zajimava esej, mmj. i pro tebe: lucumr.pocoo.org/2026/5/4/co…
(cc oceni i @tomaskafka )
1
1
122
Petr Houška retweeted

Apr 10
this is apparently a two year old clip. which i had not seen.
i have already had a <redacted> call me and tell me this, and try to explain mitigating circumstances. "he was already dead" "they needed to throw him down to id the body, since they would be rapidly under attack" "the youths drop stones on their heads"
the barest mitigating circumstances imaginable in war, but i give him that.
then i say, man, my patience is through the floor. how do you blow up hundreds of bombs in downtown beirut with no warning inside of 24 hours of a ceasefire. how do you blow up a funeral. the kids blown up look like my little cousins (i'm part lebanese). this is fucking fucked man, and it's dragging the US and the whole region into war. i'm pissed.
dude says "lebanon was never part of the ceasefire" it fucking was. I have extensively documented this as have the world media and intelligence. fucking rapid response retweeted this. that's the fucking white house war room. trump returthed it and then went to delete.
dude tells me "you're brainwashed"
me: "fuck you" <hang up>
i am fucking done. dude still hasn't apologized for trying to shade that iran blew up minab school. bro it was fucking us. and we have hit hundreds of hospitals, and universities, and schools since then. what the fuck. and i'm the one who's brainwashed? every fucking state is lying rn. we are at war. it is more than a full time job sorting state lies and propaganda from the situation. i can do without your poison in my ear. see you on the other side, man
x.com/receipts_lol/status/20…
Apr 10

The video is from Qabatiya, south of Jenin.
19 Sep 2024.
genocide.live/event/178
3
1
25
1,136
Petr Houška retweeted
Apr 10
there is nothing in my moral system that justifies this. is there something in yours? please remind me, so i know who to make my enemy
Apr 10

This video of Israel soldiers casually throwing what appears to be a Palestinian youth off from the roof of a building has shocked the world.
Look how comfortable they walk away after throwing the youth to his death.
As if they have done it 100s of times before.
5
7
104
4,431
Apr 8
This is, btw, a surprisingly common experience I also share. There is this weird "everything I don't understand is psychiatric issue" notion shared by all doctors except for (some/many?) psychiatrists.
Kinda makes sense. But also kinda terrifying.
Apr 8

I developed a POTS-like condition that turned me into a semi-invalid for five years. Every doctor I saw diagnosed some version of stress/anxiety/panic disorder—except, ironically, the psychiatrist I consulted. None of them realizes they got it wrong. I think about that a lot.
6
207
Petr Houška retweeted

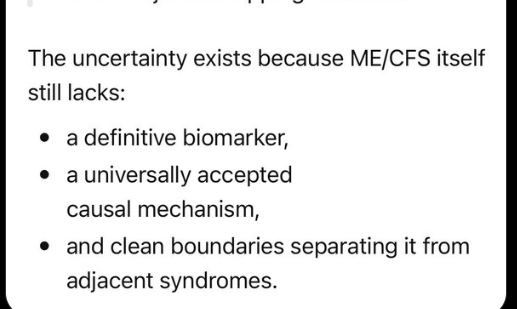
One of the biggest reasons I’ve become theory-agnostic in Long COVID and ME/CFS is how easy it is to become convinced you’ve found the explanation.
That is not because people are irrational. It is because the human brain has to simplify problems in order to handle them. When a disease is extremely complex, with many overlapping systems and huge amounts of literature, we naturally latch onto a theory that seems to connect a lot of the dots.
I saw that in myself very early on with ROCK1. I came across papers suggesting it may be altered after COVID, and the more I read, the more compelling it seemed. ROCK1 appeared connected to mitochondrial dysfunction, vascular dysfunction, viral persistence, and a range of other features that looked highly relevant. It felt like I might have found something that could explain the disease.
Interestingly, in our own data, ROCK1 appears reduced in blood. But even that is not straightforward. Lower circulating ROCK1 may in some contexts reflect cleavage, which could imply increased activity rather than decreased importance. That still needs further research.
The same pattern repeated across other pathways. Angiotensin 1-7, ACE2, PINK1, TGFB, NAD biology, tryptophan and kynurenine metabolism, T-cell exhaustion, NK-cell exhaustion, and mast-cell biology.
Each time, there were mechanisms that looked compelling. There were people who improved when targeting them. But there were also people who worsened from the exact same interventions.
At a certain point, the pattern becomes difficult to ignore. Multiple pathways can each look capable of explaining the disease, which means likely none of them do on their own.
Finally, we are beginning to see the emergence of systems that may be able to hold the full nuance and scale of biological data in context at once, something the human brain has not been able to achieve.
Now the goal is clear. Build the highest-quality datasets to allow those systems to solve these diseases as quickly as possible 💪

14
24
194
8,705
Petr Houška retweeted
Two recent stories suggested AI may help find highly personal treatment routes in cancer, one in Sid Sijbrandij and one in Rosie the dog. There is some nuance here, so I’ll break down what happened in simple language, including cost, and how similar logic could apply to chronic disease.
4
3
26
1,935
Mar 26
293
Petr Houška retweeted

Mar 24
Radši bych psal o jiných věcech, ale it is what it is.
"Covid nezmizel, to je snadno pozorovatelný fakt. Realita se neřídí zbožným přáním."
"Adekvátní snaha o řešení long covidové krize iniciována nebyla."
16minut čtení, ale stojí myslim za to
Díky @A_Rychlikova a @page404cz
4
9
23
884
Mar 24
Jeden z nejlepších článku o long COVIDu.
Odmítnutí šikany zdravotního a sociálního systému, ..., je způsob stávky.
Má to samozřejmě limity. Časem už nemáte co odmítat, ... . Svět na vás zapomene, jakmile nejste alespoň trochu užiteční. Nikoho si už za rukojmí nevezmete.
1
8
224
Mar 24
1
3
105