My plan for the antivirals was to hit about 80-90 days and then wind down, which I’m starting to approach. In truth, the jury is still out on whether it worked or not. My labs show something has happened involving IgM and IgG but I’m still not confident with how to interpret it all yet.
One of the issues is my RNA seq data is lagged by six weeks. So I haven’t even seen day 42 yet. But that should hopefully come soon.
That said, I felt like it would be remiss not to try one anti viral I have avoided over a year - Molnupiravir.
Molnupiravir has a bit of a rocky history. It works in a completely different way than most antivirals. GS441524 targets RdRp which makes it so it can’t copy itself. Paxlovid targets Mpro, which means it can’t sub-assemble its sgRNA proteins.
The problem with each is that Covid has a proofreading mechanism, nsp14, one that can correct mistakes that are introduced by antivirals. So it’s possible it’s actively working to fix the issue with RdRp and Mpro.
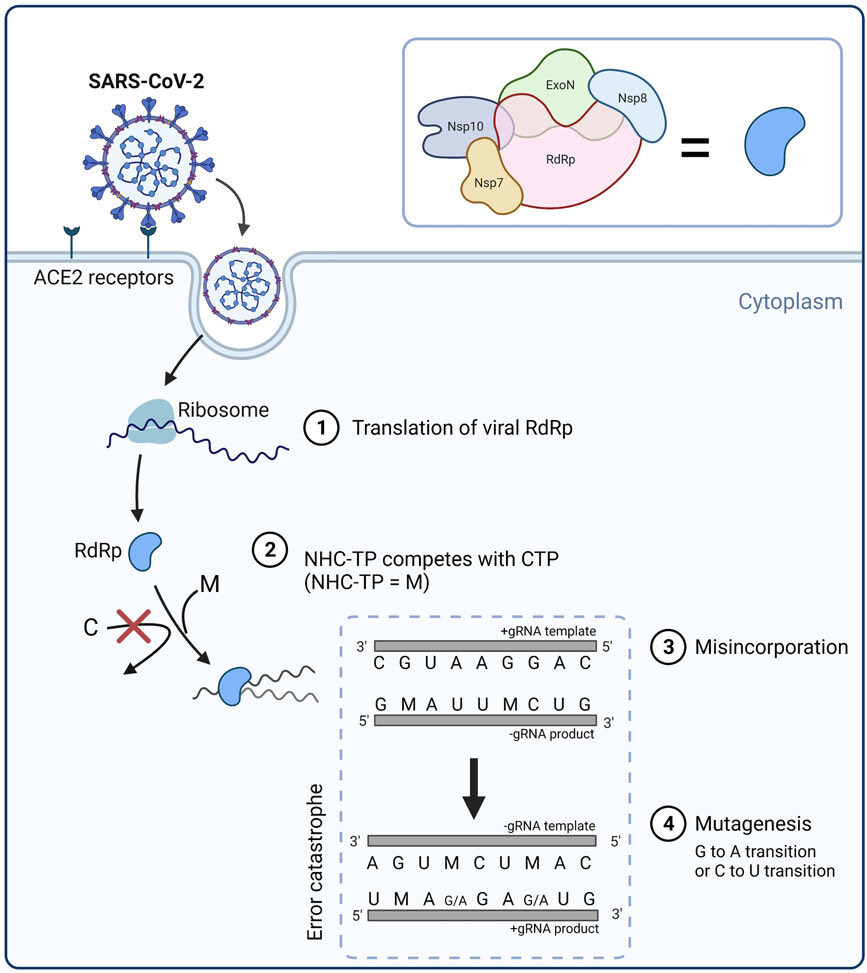
Molnupiravir works by lethal mutagenesis. It literally froms a bastardized versions of A and U bases which can then get erroneously incorporated into the virus’ RNA during a copy. These look like regular bases from the nsp14 perspective so it’s unlikely to be able to fix them.
After one copy you might get five errors introduced. Now maybe it’s partially disabled or less fit. Next copy five more errors are introduced, and now it’s starting to produce little Seth Brundle mutants that can’t fold proteins or make nsps etc. the errors are random and likely fatal after a few generations. The virus basically dies by error catastrophe.
Sounds great, but there are several problems. The first is by definition you are making covid19 clones, and you don’t know if they’ll be defective ones or super ones. In general random errors produce less fit copies, but it’s not impossible the errors can accumulate in a beneficial way. Unlikely though I think.
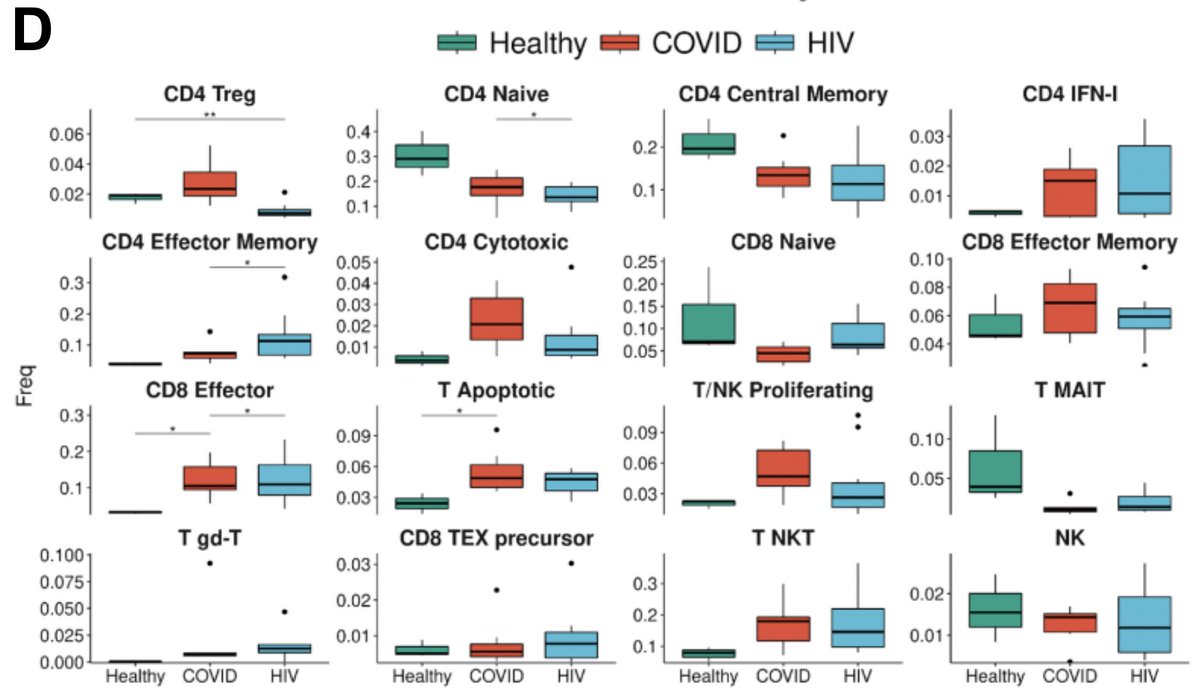
In terms of someone like myself though I’ve been wondering if this might be a good thing. My body has been fighting something for 28 months it can’t seem to get rid. I have no signs of any serious auto immune issues, but what I have is antibody, cytokine, and lymphocyte data that continues to show an active viral antivirus campaign against Covid itself.
So the question becomes, how can I break this 28 month stalemate? One way I can imagine if I take one super evolved covid19 clone that’s inside me, likely due to 28 months of specific Duane like immune pressure, and bust it up. So instead of one super clone, maybe I now get 10-20 partially genetically degraded versions instead. Will my immune system have a new shot at them? Let’s see.
The other problem is there a non zero chance this can happen with regular cells too. Which is why the medication typically is only taken five days. But in theory if Molnupiravir incorporates into human RNA it’ll eventually break down naturally as long as the DNA hasn’t been changed. Regardless, having seen lots of people who tried it for acute infections with seemingly no ill effects I figured it would be the last antiviral in my test before I start de- stacking meds and give my body a chance to clear itself out from all these meds, which I’m spending about $50-$60 on per day.
The fact I haven’t seen clearance yet might not be unexpected In that Madrid study that tested multiple antivirals in immune compromised people, the antiviral courses were ten days but many didn’t officially clear the virus (test negative) for several weeks later all the way out to 100 days before going negative. So it’s possible to stop replication and then spend weeks or months clearing up all the covid viral debris, many of which are still immunogenic.
On Monday and Tuesday I’ll do a massive cytokine test, lymphocytes, antibodies, RNA seq #5, and some of the other tests I did at the beginning to bookend some of the results. After that I’ll probably pop the clutch and see what happens.