
UCL old age psychiatrist | Improving dementia and mental health treatment | Layla | Clinical academic training
Joined November 2015
- Tweets 53,856
- Following 2,800
- Followers 18,437
- Likes 165,803
2,109 Photos and videos
















Robert Howard retweeted

Jun 12
Awesome new paper by the amazing Samei Huda on “Criticals” well worth a read
cambridge.org/core/journals/…
2
10
25
4,988
Robert Howard retweeted

Jun 10
It was important for me to engage with critics of my WIRED piece about long Covid. I think journalists owe the public and their critics this kind of engagement, especially on a topic as fraught as this one. But at this point I think I've said everything that's useful. I'll be stepping away from this specific topic on social media for the next few months.
If you are interested in how it has all played out, I encourage you to go through my timeline. You'll see my posts, which include links to longer critiques of my piece, as well as my replies to people on here. They also include threads laying out more extended discussions of topics that couldn't get adequate treatment in the piece.
wired.com/story/the-painful-…
63
6
50
27,383
Robert Howard retweeted

Jun 10
Trying to help eldely parents navigate hospital and other provider IT platforms is a disaster. The ridiculous IT security to protect the dignity of the 100s of thousands of 70 year olds with buggered hips and knees, and the endless demands for other useless personal information is frankly abusive.
2
3
18
1,039
Robert Howard retweeted

This panel (not the families) missed the point
The #NottinghamInquiry wasn’t about someone desperately wanting services
He wasn’t going to pay for private care or seek help at a religious place
He was very psychotic, dangerous & totally avoidant
He needed Assertive Outreach
Jun 9

‘Valdo Calocane's family weren’t told he had schizophrenia’
Majorie Wallace, Chief Executive of the mental health charity SANE, says that when families are not given enough information about a relative’s mental health condition, it becomes much harder for them to deal with such a ‘serious problem’.
7
18
127
20,549
Robert Howard retweeted

Jun 9
"I'm not anti-vaccine, I'm just pro-vaccine safety!"
"I'm not anti-psych, I'm just pro-informed consent!"
Both can be true, and both can be ways of smuggling in antivax and antipsych.
I'm seeing a lot of the latter.
13
6
63
3,183
Robert Howard retweeted

Mental illness existed before the DSM. Psychosis existed before antipsychotics. Suicide existed before antidepressants.
Claiming treatment creates suffering is not bold. It is dangerous misinformation.

You missed the drug treatment part.
24
20
94
6,849
Robert Howard retweeted

Jun 9
Nice post. Psychiatrists are treating the symptoms from multiple diseases, because other medical doctors often refer patients to us because they can’t manage the effects of theses patient’s diseases.
Often we can help, sometimes not, and hopefully rarely do we make things worse.
Other specialists and their patients are often relying on us to help them with their patients who have some of the worst symptoms of medical illness, because our treatments are broad spectrum, potentially improving things from multiple angles including improving cardiovascular, neuro-hormonal, and inflammatory states etc.

Psychiatry cant be ignored - here’s why 👉Many medications that make a meaningful difference in ME/CFS, POTS and Long Covid are often classified as “psychiatric medications”. 🚨
The clinical question is not whether a medication is psychiatric, neurological, immunological or cardiovascular. The question is whether it targets a relevant biological process.
Psychopharmacology provides a major framework for targeting several domains seen in ME/CFS, POTS and Long Covid: autonomic instability, hyperarousal, sleep disruption, pain amplification, cognitive dysfunction, sensory sensitivity, fatigue, threat circuitry, inflammatory signalling and mast-cell-related pathways.
But psychiatry is portrayed as the emery. Most patients are seen by psychiatry late in the picture and it’s often when physicians have tried everything and now they refer to psychiatry .
So the irony is psychiatry is really a refuge for the physician’s hopelessness here .
So the list - not exhaustive, but includes
1. Naltrexone / low-dose naltrexone
2. Aripiprazole / low-dose aripiprazole
3. Memantine
4. Prazosin and clonidine
5.Guanfacine
6. Vortioxetine
7. Psychostimulants - methylphenidate, dexamphetamine, lisdexamfetamine
8. Modafinil and armodafinil
9. SNRIs :duloxetine, venlafaxine, desvenlafaxine, milnacipran
11. TCAs : amitriptyline, nortriptyline, doxepin
12. Mirtazapine, Trazodone
13. Gabapentinoids : pregabalin, gabapentin
14.Beta-blockers : propranolol
15.’Benzodiazepines
16.Melatonin
17.Low-dose antipsychotics with antihistaminergic properties where hyperarousal, sensory amplification or agitation are dominant
18. Mood stabilisers / anti-kindling agents -e.g lamotrigine in highly selected neuropsychiatric phenotypes
Many of these medications are called psychiatric because psychiatrists are often the clinicians most familiar with their mechanisms, dosing, adverse effects, interactions and clinical sequencing.
Most physician’s struggle to use these appropriately because this is psychopharmacology.
That does not mean they are only treating depression or anxiety.
And if the construct infront of them is anxiety or ADHD or agitated depression then the medications re used in a very specific way that makes a difference
Several agents used in psychopharmacology have effects on inflammatory signalling, autonomic tone, sleep architecture, pain processing, cognition, arousal, mast-cell-related symptoms, or central threat prediction.
This is where the mind–body split becomes clinically unhelpful.
A patient may decline an “antidepressant” because they do not have depression.
A clinician may avoid a medication because it is seen as psychiatric.
A biological target may then be missed because the medication carries the wrong label.
In practice, when brain–body integration is understood, the framing changes.
These medications are biological tools.
And in complex conditions such as ME/CFS, POTS and Long Covid, dismissing them because of category stigma can limit treatment options and reinforce the very split that prevents more integrated care.
6
5
38
5,290
Robert Howard retweeted
Your words were all very powerful
Sinead made a vital point about the Ritchie Report
So disappointing senior figures from the world of mental health still don’t get it
This isn’t about lack of access for people who want services
It’s about those who avoid them at all costs
2
8
20
962
Robert Howard retweeted

So prescient “A new world-view is emerging, one which attempts to explain all manner of ills as the result of inflammation or immune dysfunction. While motivated by some genuinely exciting science, this seductively uncritical reductionism is symptomatic of an increasingly widespread cultural uneasiness with nuance or uncertainty…. ( Tom Pollak)
@tompollak

As a neurologist, it is now patently clear to me that the vast majority of people on the planet are suffering from neuroinflammation or brain damage (likely both)
The way people speak & behave has changed. Markedly so.
Whether irl, or via messaging/social media. It’s noticeable
6
4
30
2,592
Robert Howard retweeted

There's unlikely to be a crime dictate to stop detaining black men. However, given the focus of the 2018 mha review on overrepresentstion of black men in hospital and then the black lives matters uprisings, it's reasonable to suggest psychiatrists may be questioning themselves
1
1
19
1,273
Robert Howard retweeted
Psychiatry cant be ignored - here’s why 👉Many medications that make a meaningful difference in ME/CFS, POTS and Long Covid are often classified as “psychiatric medications”. 🚨
The clinical question is not whether a medication is psychiatric, neurological, immunological or cardiovascular. The question is whether it targets a relevant biological process.
Psychopharmacology provides a major framework for targeting several domains seen in ME/CFS, POTS and Long Covid: autonomic instability, hyperarousal, sleep disruption, pain amplification, cognitive dysfunction, sensory sensitivity, fatigue, threat circuitry, inflammatory signalling and mast-cell-related pathways.
But psychiatry is portrayed as the emery. Most patients are seen by psychiatry late in the picture and it’s often when physicians have tried everything and now they refer to psychiatry .
So the irony is psychiatry is really a refuge for the physician’s hopelessness here .
So the list - not exhaustive, but includes
1. Naltrexone / low-dose naltrexone
2. Aripiprazole / low-dose aripiprazole
3. Memantine
4. Prazosin and clonidine
5.Guanfacine
6. Vortioxetine
7. Psychostimulants - methylphenidate, dexamphetamine, lisdexamfetamine
8. Modafinil and armodafinil
9. SNRIs :duloxetine, venlafaxine, desvenlafaxine, milnacipran
11. TCAs : amitriptyline, nortriptyline, doxepin
12. Mirtazapine, Trazodone
13. Gabapentinoids : pregabalin, gabapentin
14.Beta-blockers : propranolol
15.’Benzodiazepines
16.Melatonin
17.Low-dose antipsychotics with antihistaminergic properties where hyperarousal, sensory amplification or agitation are dominant
18. Mood stabilisers / anti-kindling agents -e.g lamotrigine in highly selected neuropsychiatric phenotypes
Many of these medications are called psychiatric because psychiatrists are often the clinicians most familiar with their mechanisms, dosing, adverse effects, interactions and clinical sequencing.
Most physician’s struggle to use these appropriately because this is psychopharmacology.
That does not mean they are only treating depression or anxiety.
And if the construct infront of them is anxiety or ADHD or agitated depression then the medications re used in a very specific way that makes a difference
Several agents used in psychopharmacology have effects on inflammatory signalling, autonomic tone, sleep architecture, pain processing, cognition, arousal, mast-cell-related symptoms, or central threat prediction.
This is where the mind–body split becomes clinically unhelpful.
A patient may decline an “antidepressant” because they do not have depression.
A clinician may avoid a medication because it is seen as psychiatric.
A biological target may then be missed because the medication carries the wrong label.
In practice, when brain–body integration is understood, the framing changes.
These medications are biological tools.
And in complex conditions such as ME/CFS, POTS and Long Covid, dismissing them because of category stigma can limit treatment options and reinforce the very split that prevents more integrated care.

A recent review proposes integrating POTS, ME/CFS, and Long COVID into the neuroimmunology subspecialty. Here is their compelling case.
\ Overlapping Drivers of Disease:
The authors outline several major overlapping pathophysiological mechanisms shared by POTS, ME/CFS, and Long COVID. This includes:
1. Autonomic Dysfunction (Dysautonomia)
2. Mitochondrial Dysfunction
3. Cerebral Hypoperfusion
4. Immune Dysregulation
5. Neuroinflammation
6. Autoimmunity
\ The Harm of Psychiatric Misdiagnoses:
For decades, patients have been wrongly labeled with "functional neurological disorder," anxiety, or somatization because routine tests often look normal.
\ A Call for Better Diagnostics:
Researchers and clinicians urgently need advanced tools such as:
- 7T MRIs
- Targeted PET scans
- Autoantibody and cytokine panels
- Comprehensive autonomic function testing
Routine tests are simply not enough.
\ The Authors’ Core Proposal:
Classify and treat POTS, ME/CFS, and Long COVID as neuroimmune disorders under the subspecialty of neuroimmunology.
This shift would:
• Improve clinical care
• Accelerate research
• Enable effective neurotherapeutics (including repurposed immunomodulatory and anti-inflammatory treatments)
Thanks, Dysautonomia Clinic, for the awesome paper!
#MECFS #POTS #LONGCOVID #PASC
Read more here: buff.ly/HqR7NKH

14
17
73
14,672
Robert Howard retweeted

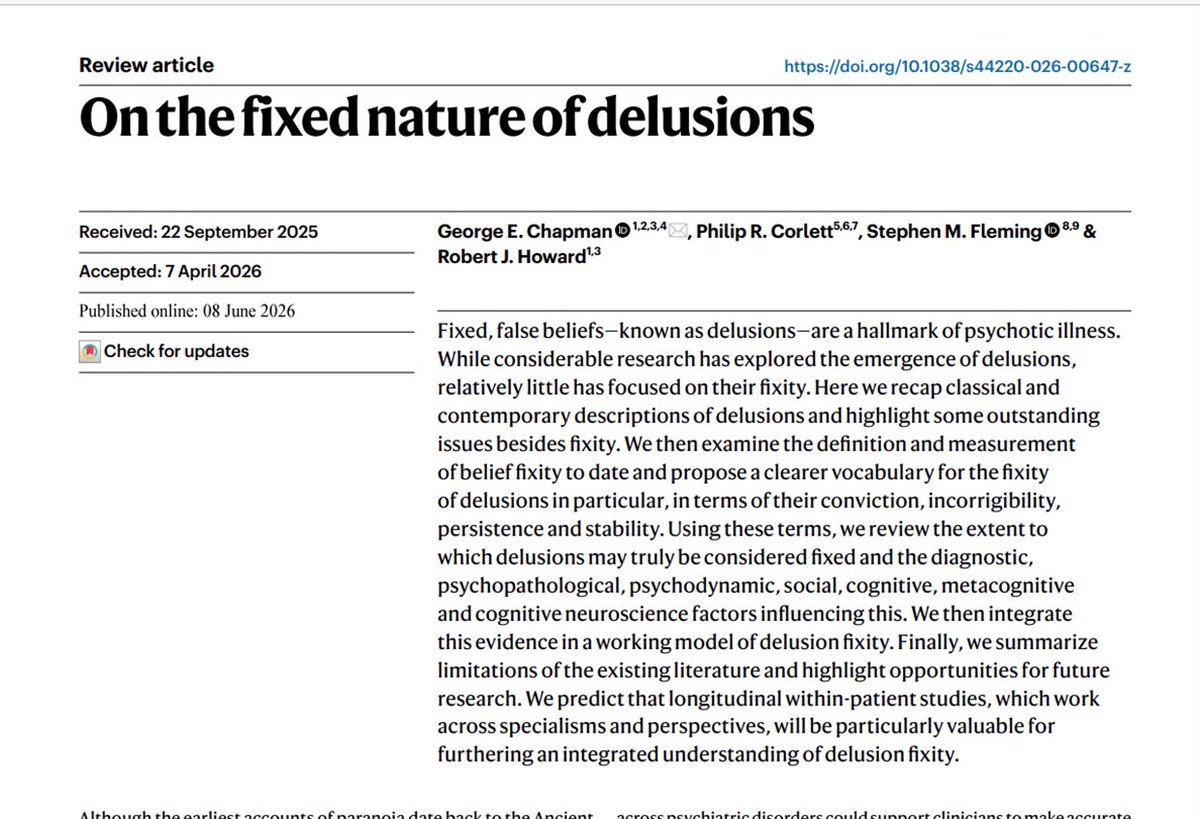
Delighted to see our Review out today in @NatMentHealth
Since Jaspers, delusions have been (perhaps somewhat economically) described as “fixed” false beliefs
We set out to find all articles that have touched - to a greater or lesser extent - on the issue of delusion “fixity” 📄

Led by @Chapman_GE our new paper on the fixed nature of delusions is out today in Nature Mental Health.
2
5
13
2,118
Robert Howard retweeted
.@MrsEmmaWebber @drsanjoykumar @coatesaholic
Saw your press conference
I think you & your families are truly inspirational
As a psychiatrist, I hope your campaign for true justice will also bring about the positive change in mental healthcare so desperately needed for years
6
28
252
3,474
As part of her 90th birthday, my mother announced that she was going to ride pillion on a friend’s Harley Davidson. She’s just sent me photographic proof.
9
8
193
3,172
Robert Howard retweeted

If only more people around here were like this…
Jun 7

Yes, I had a very severe reaction to my second Moderna shot. But part of being a responsible scientist with a large platform is not extrapolating my personal experience to the entire population.
I also have a rare autoimmune condition called Parsonage-Turner syndrome (diagnosed in 2013), so I may have been particularly vulnerable to side effects.
Given my bad experience with the first mRNA vaccine I've ever taken, I have made the personal decision to avoid them in the future.
However, it would have been incredibly unscientific and highly irresponsible of me to take this personal experience of mine and start telling millions of people online to not get vaccinated for COVID.
There's a reason quack alternative medicine practitioners plaster personal testimonies all over their websites. They sound convincing to a lot of people. But it's purely manipulation. Personal testimony, even a large collection of them, isn't a substitute for real, population-level data.
I am not an expert on vaccines, the COVID vaccine, or epidemiology in general. So when I experience a serious side effect taking something with a non-zero rate of serious side effects, I understand that my personal experience likely isn't an indication that we're all being lied to about safety.
You should understand that as well.
The impulse to extrapolate a very negative personal experience to the entire population is very strong. But responsible scientists, and especially those with large public platforms, should resist that impulse.
9
1
22
3,086
Led by @Chapman_GE our new paper on the fixed nature of delusions is out today in Nature Mental Health.
4
18
70
7,594
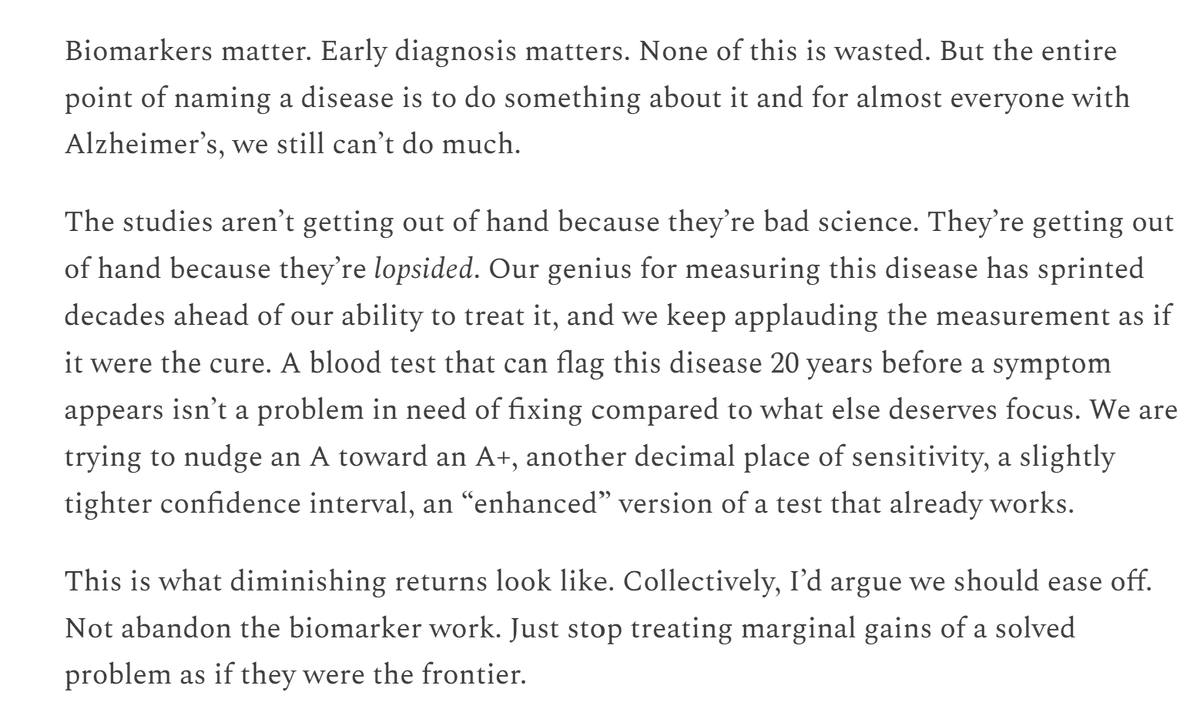
I can't repeat myself too often on this point. The Alzheimer's biomarkers should have no place outside of a comprehensive clinical evaluation. They only have value in identifying the likely pathology once a diagnosis of dementia has been made.

The Alzheimer’s Biomarker Studies Are Getting Out of Hand: Confessions of an Alzheimer’s researcher #AndrewBubak . we’ve gotten brilliant at diagnosing a disease we still can’t treat and most of us know it.
profbubak.substack.com/p/the… @ProfRobHoward
3
10
39
4,118
Robert Howard retweeted
This article neatly illustrates what’s wrong with UK mental healthcare
The case cited is a world apart from VC, who had psychosis, poorly engaged & non treatment compliant
Why do people, inc psychiatrists, think this group will engage with Open Dialogue?!
#NottinghamInquiry
What Lapland can teach @NHSEngland about treating psychosis: The Nottingham killings inquiry has highlighted major flaws in mental health provision. Is a system pioneered in Finland the way forward?
thetimes.com/article/6d722d6… via @RoisinKKelly_ @nuwandiss
5
15
32
8,424