Professor, Clinical Psychology, University of East London. Chair, International Institute for Psychiatric Drug Withdrawal iipdw.org. Opinions my own
Joined February 2014
- Tweets 19,514
- Following 2,032
- Followers 12,748
- Likes 11,589
250 Photos and videos






Pinned Tweet

Jun 6
Truly bizarre account of a man with learning difficulties given ECT, without his consent, 100 times a year for 5 years.
Not as an example of reprehensible unethical conduct but as ‘precision medicine’ endorsed by ‘senior’ psychiatrists.
Sickening.
sciencedirect.com/science/ar…
7
29
81
5,235
Dr John Read retweeted

The phrase “treatment resistant” often tells us more about the arrogance of the system than about the suffering of the patient.
A treatment fails — and the patient receives the label.
A drug causes harm — and the harm is minimized as a side effect.
A person objects — and their objection is interpreted as pathology.
This is how medicine can quietly lose its moral centre.
Antipsychotics are not neutral tools. They are powerful interventions with profound effects on body, mind, identity, movement, metabolism, sexuality, emotion and memory. To call them simply “highly efficacious” while ignoring the human cost is not science. It is institutional storytelling.
The real question is not whether these drugs can suppress symptoms. The real question is whether suppression is being confused with healing.
Were they developed to restore human freedom — or did they also become instruments of behavioural control, institutional convenience and social management?
A humane medicine must be brave enough to ask this.
#PatientRights #MedicalEthics #InformedConsent #PatientSafety #WomenInMedicine
2
8
17
312
Well said @markhoro
@awaisaftab is so close minded he blocks most people who correct his fallacious arguments , including me

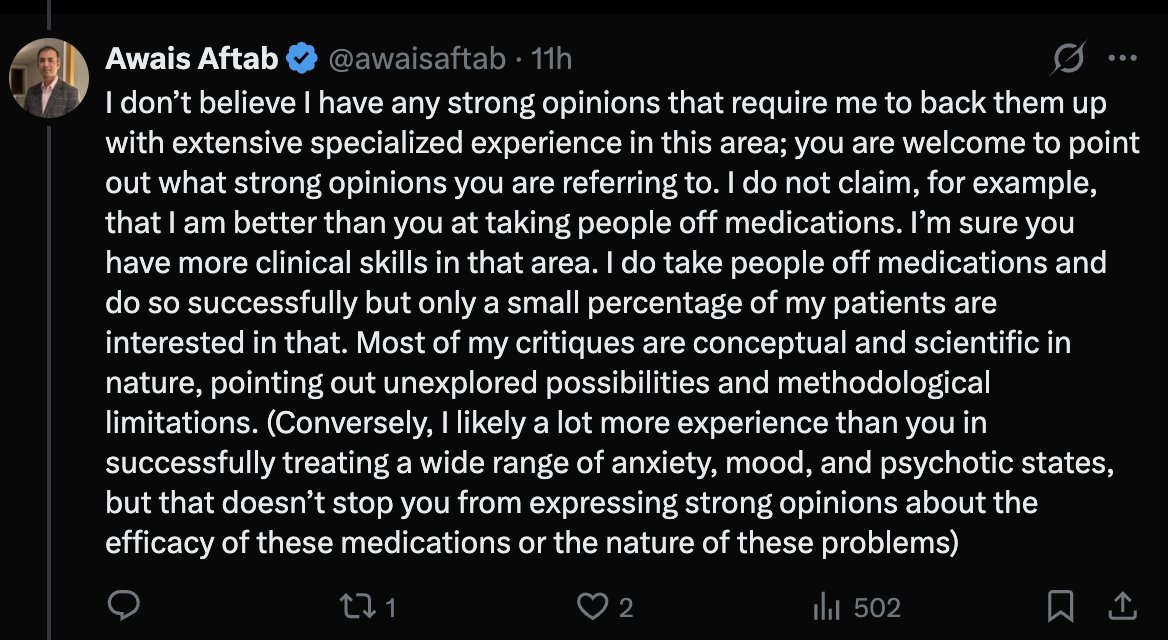
As I said I think you are entitled to your opinions and of course you have read some of the literature. But I do think it is a telling admission that you do so only in a small % of your patients (I understand that that is driven by their lack of interest rather than yours) and so have limited firsthand experience. Your strong opinions is that you simply do not believe protracted withdrawal is 'credible' condition (you also do not cite any literature for your throw away reasons for why), strong opinions about delayed onset withdrawal etc, etc. I do think that it is somewhat difficult to be a credible commentator about a process you don't undertake very much, about which there is unfortunately limited research and so where clinical experience counts for disproportionately more. Normally limited experience would lead someone to be more cautious and less certain of their position.
4
3
22
1,958
Yet another false claim that “anti-psychotics” are “highly efficacious” (they are barely better than placebo and have awful adverse effects) while trying to blame their not working by labelling patients as “treatment resistant”
psychiatryonline.org/doi/abs…
6
16
57
1,060
Dr John Read retweeted

New Research Challenges the Logic of Coercion in Psychiatry
By Richard Sears
Recent studies examine long-term harms of psychiatric detention, ward environments as a major driver of coercive interventions, and why some staff support coercive practices.
buff.ly/BenbLBR

2
24
42
1,387
Apr 22
The latest (8th) paper from our international survey.
Full. Free.
Great to give a voice to so many previously unheard people.
“An international survey of the relatives and friends of electroconvulsive therapy recipients” - Harrop et al
bpspsychub.onlinelibrary.wil…
3
16
26
1,411

If you think ECT patients are consenting to their injuries, read on and think again. This scandal will erupt for psychiatry at some point. They've got away with this for far too long.
Jun 10

How Accurate Are ECT Patient Information Leaflets Provided by Mental Health Services in England and the Royal College of Psychiatrists? An Independent Audit connect.springerpub.com/cont…
3
17
42
1,313
Dr John Read retweeted

"How They Rig Clinical Trials and The Price We All Pay For It -
A practical guide to spotting doctored research and finding the therapies that actually help"
By @MidwesternDoc
midwesterndoctor.com/p/how-t…
4
5
300
Dr John Read retweeted

Jun 10
The brain is not meant to be in a drugged state.
6
25
77
1,717
Dr John Read retweeted
Sharing for awareness. While we may still have a long way to go, and may not agree with everything being said, the media coverage is increasing and more conversations are opening up on this topic and this is a positive thing.
stuff.co.nz/wellbeing/360988…
2
4
10
342

Dr John Read retweeted

Jun 9
This is a response from an anonymous Australian psychiatrist @LnS7juXQs to my post advocating for safe, hyperbolic tapering protocols and sharing my own experiences with antidepressants. It’s individuals like this who bring the entire profession of psychiatry into disrepute, yet they are regularly platformed by other prominent psychiatrists on this platform. I’m obviously blocked despite never having interacted with them, so I can’t reply directly. I’ll word it in a way they may understand better: “9gshGH/6/ghh56GHt.”

19
16
51
1,676
Dr John Read retweeted

I think kaddles speaks for a lot of patients here. A lot of clever psychiatrists on here missing the point because they are blind to the scale of the issue for reasons I outline in this blog. Unfortunately this leads to so many people's lives upended or worse from mostly preventable harm. mhorowitz.substack.com/p/why…
Jun 8

What I think about when I see psychiatrists on social media debating semantics and deftly diverting attention, as someone whose life has been profoundly affected by psychiatric drug harm. 🧵 (1/9)

1
22
52
3,948
Dr John Read retweeted
Beyond Medication: What England’s Experience Can Teach Us About Psychosis Care
By Alison Brabban
For over 20 years, NICE in England has recommended that people experiencing psychosis should be offered psychological therapy—not simply medication alone.
buff.ly/RcTw3iG

1
9
18
920
Jun 10
Thoughtful analysis from Dr Alison Brabban
Beyond Medication: What England’s Experience Can Teach Us About Psychosis Care - Mad In America madinamerica.com/2026/06/bey…
5
6
345
Jun 10
How Accurate Are ECT Patient Information Leaflets Provided by Mental Health Services in England and the Royal College of Psychiatrists? An Independent Audit connect.springerpub.com/cont…
1
13
28
2,084
Dr John Read retweeted

(1/?) PSA: hyperbolic tapering isn't about the length of the taper and doesn't automatically mean patients are tapering for years (which is what some psychiatrists are misleadingly claiming in order to scaremonger/rage bait about hyperbolic tapering).
It's about how the reductions are made so the size of the reduction gets smaller as the overall dosage nears 0.
Here is what NICE (the UK body that develops practice guidelines for UK doctors) said of this in July 2023 (linked below).
In this announcement (and in the full NICE guidelines), NICE signposted the Royal College of Psychiatrists' guide to stopping antidepressants that is based on hyperbolic tapering AND gives examples of a shorter hyperbolic taper and a longer, more conservative one.
Psychiatrists who are saying hyperbolic tapering automatically means years-long tapers are being ignorant or deliberately dishonest. In their desperation to protect their field's reputation, somehow some of them manage to be a combination of both.
No excuse for UK psychiatrists in particular not knowing about this or misrepresenting it:

1
6
16
787
Dr John Read retweeted
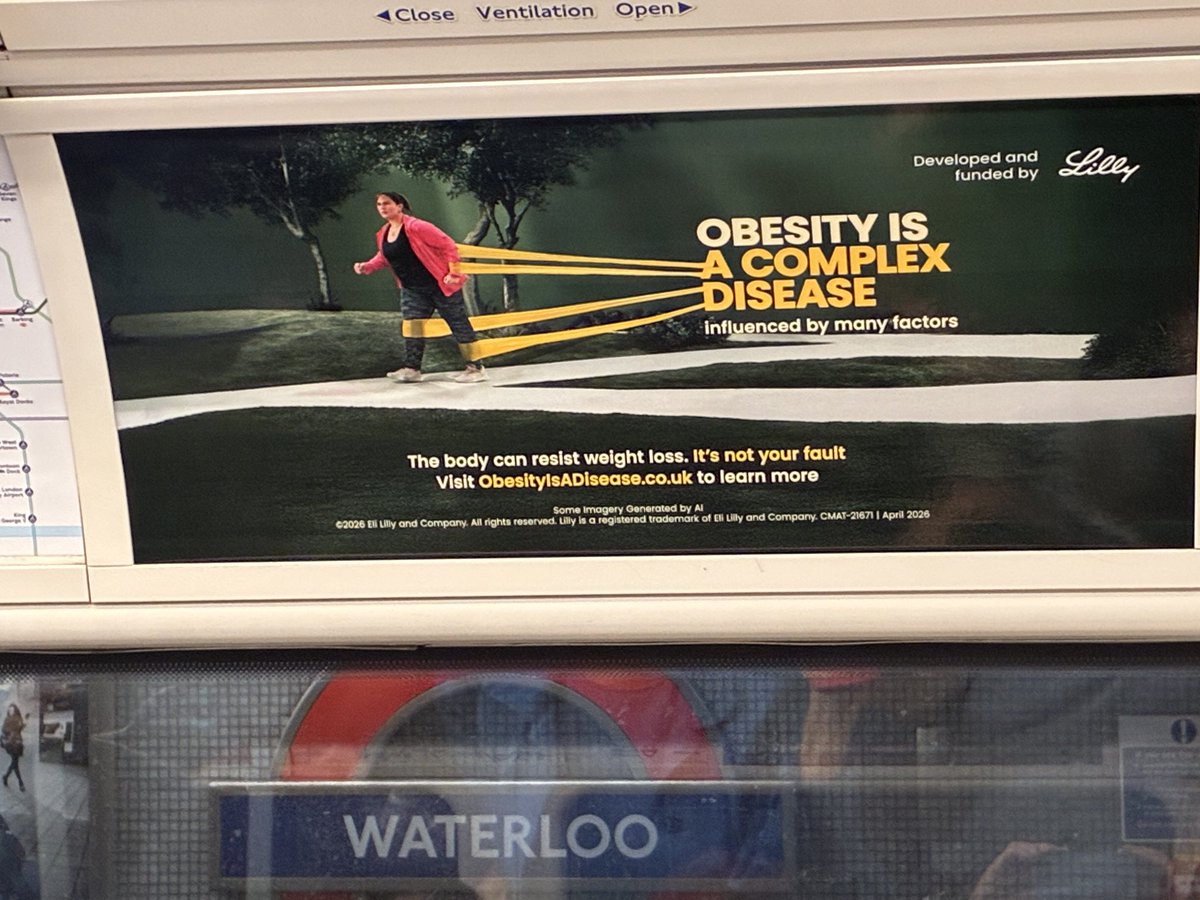
(1/2) A psychiatric clinic in New Zealand is running an advert in a major NZ media outlet talking about antidepressant withdrawal to draw attention to what it calls "medication optimisation" and its wider services. Makes me wonder if this clinic is reading the room...
"Stopping antidepressants too quickly can lead to withdrawal symptoms such as anxiety, insomnia, dizziness, nausea, and mood swings. Clinical guidance recommends a gradual reduction to minimise these issues, mainly because withdrawal can be mistaken for a return of the original condition***. Without proper support, individuals may become stuck: unable to stop, unsure whether they are experiencing withdrawal or relapse, or returning to medication."

2
6
16
2,910
Dr John Read retweeted

They’ll leave you on for life without questioning why you’re even on it, but god forbid you ask to come off slowly, to let the taper be patient-led & symptom dependent, to keep current level of functioning and suddenly we are the crazy ones. 😳

Loving the new argument against hyperbolic tapers ... "you're keeping people on the drug too long!"
Brought to you by the medical speciality that augments treatment with an additional drug several times more often than they discontinue one.
1
6
44
1,519
Dr John Read retweeted

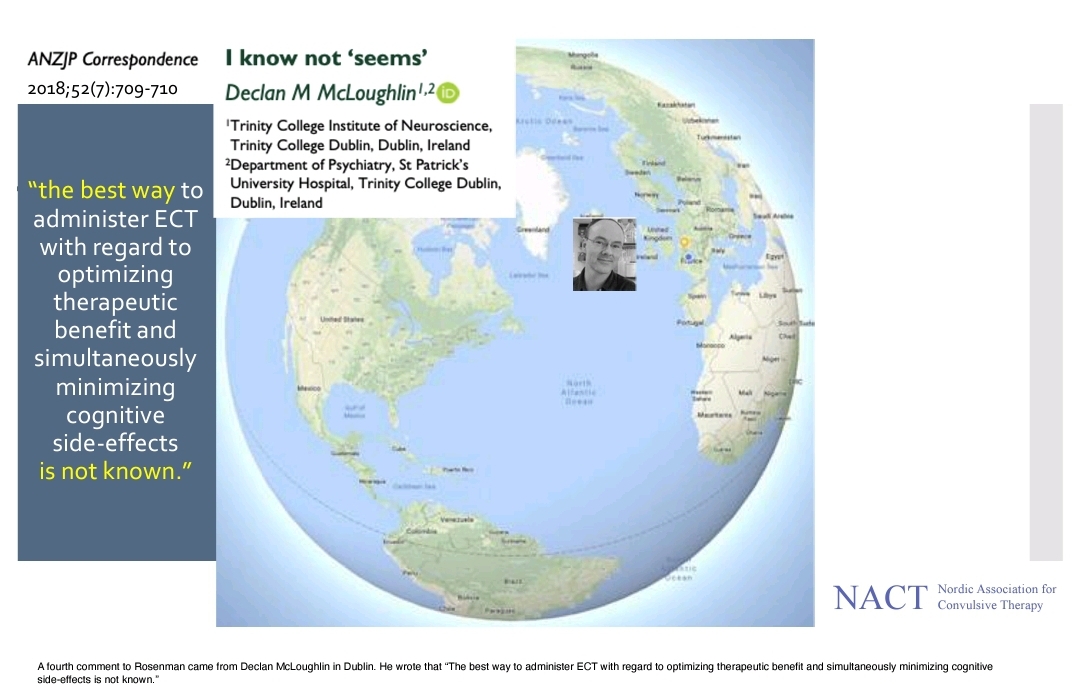
Like you, @Valarie_gw, I am extremely grateful a neuroanestesiologist is willing to step up and acknowledge ECT's risk of serious injury. Without safety testing and dosing consensus protocols to ensure reliable replication of positive outcomes, it's risks far exceed it's benefits making modern ECT unethical. At the very top of every patient information leaflet it should acknowledge the following:
"the best way to administer ECT with regard to optimizing therapeutic benefit and simultaneously minimising cognitive side-effects is not known." -Dr. Declan McLoughlin, MECTA/SigmaStim ECT device rep and psychiatrist.
According to the late Richard Abrams (CoFounder of Somatics, LLC who makes the Thymatron Devices) ECT's standard clinical guidelines regarding theraputic seizures lasting at least 30 seconds: "plucked it out of the air, as far as I know. There was no research data that I was aware of at the time ... [determined by Dr. Kalinosky], not research based but rather-clinically based..."
All of that established in 1940's by doctors who knew nothing about the histopathology of electrical injury and certainly without knowing what we know in 2026 about "euphoria"/adrenaline rush caused by trauma brain injury or the consequences of repetitive traumatic brain injury.
Medical tradition ≠ Evidence-Based medicine. @ReadReadj @Mad_In_America
#AuditECT

2
3
10
253