
Raising awareness of psychiatric drug withdrawal. Sharing the reality, the science and fight for recognition. IG - samhall404
Joined September 2012
- Tweets 6,155
- Following 2,529
- Followers 1,396
- Likes 31,587
271 Photos and videos












Pinned Tweet

Apr 30
1/ Thanks to @MikhailaFuller for allowing me to share my story. 🧵
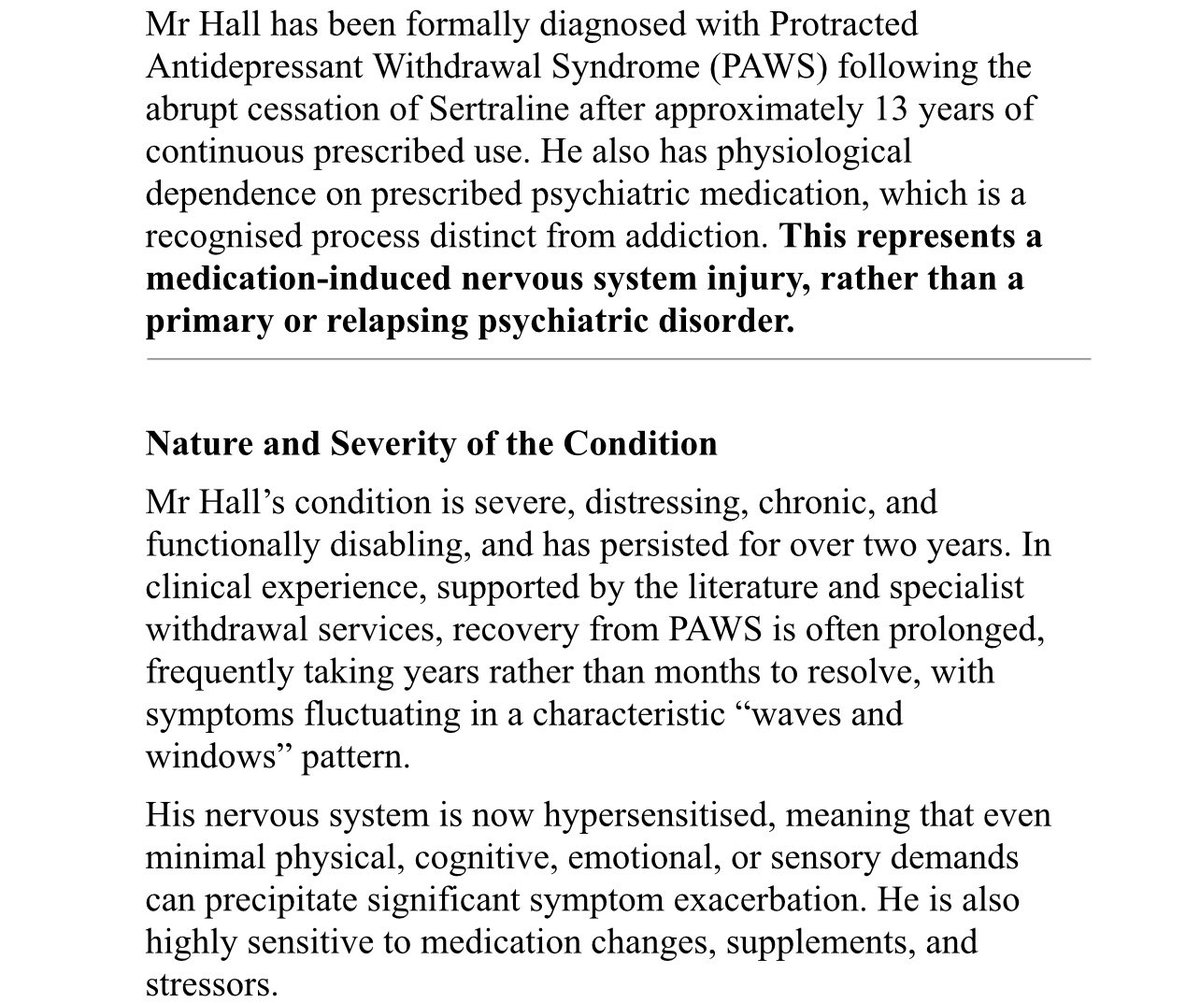
My experience sits in the uncomfortable space between what patients are routinely told about antidepressants and what can, in many cases, actually unfold over time. It is not simply a story of adverse effects, it is a story about the consequences of incomplete information, overconfidence in simplified narratives and a medical culture that too often defaults to explanation rather than investigation when things go wrong.
I was prescribed the antidepressant Sertraline for situational panic attacks following a house fire when I was younger and remained on it for approximately 13 years. During that time, I was never meaningfully informed about the possibility of physiological dependence, nor about the potential difficulty of stopping the drug after long term use. The phrase “safe and effective” was presented as if it were a stable, universal truth, rather than a context dependent conclusion drawn from limited and biased data.
There was no discussion of what happens when the brain adapts to a drug over more than a decade. No acknowledgement that removing that drug might not be a neutral act. No mention of protracted withdrawal or that stopping could result in a severe and prolonged destabilisation of the nervous system. Informed consent, in any meaningful sense, was absent.
When I eventually came off the SSRI, it was done through a rapid doctor led taper that bore no relation to the duration of my use. What followed was not a return of my original symptoms, but the onset of something far more severe, complex, disabling and life changing.
Almost immediately, I began to experience intense and persistent surges of physiological anxiety and panic. These were not thoughts or worries in the conventional sense. They were full body events; overwhelming waves of adrenaline that arose without psychological trigger, accompanied by a profound sense of internal threat. They were not responsive to reasoning, reassurance or standard psychological strategies because they were not primarily psychological in origin.
Alongside this, I developed widespread neurological and sensory disturbances. I experienced constant “electric” sensations throughout my body, moving unpredictably through my arms, legs, hands and across my head and face. These were often painful, presenting as burning, tingling or sharp nerve like sensations. My muscles began to twitch involuntarily, with fasciculations and spasms becoming a daily occurrence. At times, my facial muscles would contract and twitch without warning.
One of the most severe and distressing symptoms I experienced was akathisia. It is often described clinically as restlessness, but that description is profoundly inadequate. What I experienced was an intense, unrelenting inner agitation combined with a powerful urge to escape my own body, alongside a compulsion to move that made stillness feel intolerable. At its worst, it generated intense suicidal urges, not from hopelessness, but from a desperate need to escape the sensation itself. It was not psychological distress in any conventional sense, it was a physical state that overrode any attempt at control. It is difficult to overstate how severe and destabilising this symptom has been for three years.
Sleep became almost impossible at times. I went through prolonged periods of insomnia, sometimes sleeping only three hours across several days. When I did manage to fall asleep, I was frequently jolted awake by hypnic jerks; sudden, violent awakenings accompanied by adrenaline surges. The cumulative effect of this sleep deprivation was profound, amplifying every other symptom and eroding my ability to cope.
Cognitively, I experienced significant impairment. I developed …
prescribed-harm.com/stories/…
18
48
150
35,361
Sam Hall retweeted

It’s good to see wider discussion of withdrawal and hyperbolic tapering, including critiques. My observation is that whenever a clinician who is minimising the existence of withdrawal or the need for hyperbolic tapering is asked about their deprescribing experience they give vague answers like ‘I stop drugs all the time’ but when pressed for details trail off. Of course reading the literature is a part of being informed but actual first hand experience of large volumes of deprescribing teaches you a lot more. Everyone is entitled to an opinion but I think it is worth probing how informed such opinions are. Most friends of mine in psychiatry who are not invested in this debate either way rarely if ever stop long term drugs without switching to another or are seeing people on large numbers of drugs which buffer withdrawal effects. In other words they rarely have the chance to see withdrawal effects. I don’t want to make generalisations but I wonder where some people derive the confidence in their opinions? For example I have overseen about 4000 people coming off their drugs and I have very little idea what these drugs are doing in long term to the brain but there are some let’s say concerning signals - I would like to learn from people with much greater confidence than me what the source of their insights are.
3
19
57
1,241
Sam Hall retweeted

@awaisaftab Yes, the terminology of withdrawalology is muddy. Not the fault of the patient community. Muddy terminology & miscommunication riddle psychiatry & addiction medicine.
In general, iatrogenic conditions are poorly researched & poorly understood throughout medicine.
1
4
10
170
Sam Hall retweeted

Sent client with akathisia, dystonia, nystagmus, visual vertigo to top hospital in US. Person is in severe antidepressant withdrawal. Diagnosis: FND. These doctors are NOT TRAINED to spot withdrawal/ drug injury if it slapped them in the face. FND = iatrogenisis, yet again.
18
16
103
2,868
Sam Hall retweeted

Jun 12
Anyone who tries to shut you down with statements like ‘the science says’ or ‘the data says’ ask them to look at this.
If it takes this much to retract junk science like Study 329 how confident can we be about the accuracy and integrity of what is published?
And remember this is just one of the ones where they got caught….

🚨Study 329 lawsuit collapses
A legal attempt to force a retraction of Study 329 has failed and the journal has gone silent. What happens when science cannot—or will not—correct itself?
LINK 👇👇
@LauraDelano @MikhailaFuller @SecKennedy @AaronSiriSG @newstart_2024 @jchilders98
3
29
62
2,942
Sam Hall retweeted

🚨Study 329 lawsuit collapses
A legal attempt to force a retraction of Study 329 has failed and the journal has gone silent. What happens when science cannot—or will not—correct itself?
LINK 👇👇
@LauraDelano @MikhailaFuller @SecKennedy @AaronSiriSG @newstart_2024 @jchilders98
7
52
115
6,210
Sam Hall retweeted
Jun 11
“I rarely see this in my clinical practice”
All it takes is to ask around one’s social circle and you start to realise how common this is…

Posted on Instagram about the pains of tapering off Cymbalta, and THREE friends out of the 200 who viewed it reached out to share that they've been through this with antidepressants too. One had to take off work because it was so brutal.
This is happening all around us.
2
10
48
2,738
Sam Hall retweeted

"Despite evidence linking #antidepressants, #antipsychotics (& various other medications) with #akathisia, disturbances in thoughts & behavior, & #suicidality,¹⁻³ standard suicide assessments rarely include questions about #medications."

Important rapid response by @MISSDFoundation
"Medication-induced #Akathisia: An overlooked contributor to #suiciderisk and #iatrogenic harm"
👇
bmj.com/content/393/bmj-2025…
1
11
15
528
Sam Hall retweeted

Jun 9
Both times I've been to the psych ward were due to AD withdrawal symptoms from improper tapering, which made me suicidal. The second time I also had akathisia. It makes me wonder just how many people are there because of these very same reasons. Thankfully I survived.
6
12
54
1,454
Sam Hall retweeted

Jun 9
Millions of Americans take multiple psychiatric medications at the same time.
Yet the safety and efficacy of these drugs in combination with one another have never been adequately studied, nor is there a strong evidence base for long-term use.
At one point, I took five different psychiatric drugs simultaneously, completely unaware that I had effectively become part of an uncontrolled experiment.
I am not anti-medication.
I am pro-informed choice.
And informed choice becomes impossible when people take multiple drugs as prescribed for years without first being told what’s known– and what’s not known– about the potential tradeoffs.
@smerconish
14
43
181
9,839
Jun 9
This is a response from an anonymous Australian psychiatrist @LnS7juXQs to my post advocating for safe, hyperbolic tapering protocols and sharing my own experiences with antidepressants. It’s individuals like this who bring the entire profession of psychiatry into disrepute, yet they are regularly platformed by other prominent psychiatrists on this platform. I’m obviously blocked despite never having interacted with them, so I can’t reply directly. I’ll word it in a way they may understand better: “9gshGH/6/ghh56GHt.”
19
16
51
1,670
Sam Hall retweeted

(1/?) PSA: hyperbolic tapering isn't about the length of the taper and doesn't automatically mean patients are tapering for years (which is what some psychiatrists are misleadingly claiming in order to scaremonger/rage bait about hyperbolic tapering).
It's about how the reductions are made so the size of the reduction gets smaller as the overall dosage nears 0.
Here is what NICE (the UK body that develops practice guidelines for UK doctors) said of this in July 2023 (linked below).
In this announcement (and in the full NICE guidelines), NICE signposted the Royal College of Psychiatrists' guide to stopping antidepressants that is based on hyperbolic tapering AND gives examples of a shorter hyperbolic taper and a longer, more conservative one.
Psychiatrists who are saying hyperbolic tapering automatically means years-long tapers are being ignorant or deliberately dishonest. In their desperation to protect their field's reputation, somehow some of them manage to be a combination of both.
No excuse for UK psychiatrists in particular not knowing about this or misrepresenting it:

1
6
16
778
Sam Hall retweeted

Jun 8
What I think about when I see psychiatrists on social media debating semantics and deftly diverting attention, as someone whose life has been profoundly affected by psychiatric drug harm. 🧵 (1/9)

1
14
50
5,542
Sam Hall retweeted

Jun 8
Tyler Black: '"FIRST DO NO HARM" is not a thing.'
IMMDS Review, Julia Cumberlege - The HC system 'is not good at spotting trends in practice and outcomes that give rise to safety concerns. Listening to patients is pivotal to that."' The guiding principle 'First Do No Harm.'
2
4
12
433
Sam Hall retweeted

Jun 8
I never planned to do advocacy work or write posts about iatrogenic harm. I don't have a political motive. I just want my life back and all the lost years. I also want people to listen to me and change the flawed system so others can be spared from avoidable tragedy caused by #SSRIs.
7
23
101
2,591
Sam Hall retweeted

Jun 7
In my first year off Lexapro, my life did a 180. 15 years on SSRIs had numbed me out to the people and places I chose to be around.
It wasn’t until I was off Lexapro that I had my first healthy romantic relationship, worked in a values-aligned job, and listened to my own needs.
4
5
81
2,580
Sam Hall retweeted

Tapering off antipsychotics has been hard for me.
I could only imagine what non verbal autistic children are going through.
The harmed community is helping others. 👏
🙏🙏🙏🧠🧠🧠🙏🙏🙏❤️
Jun 8

As a moderator in antidepressant withdrawal support spaces, you eventually learn to spot the patterns of iatrogenic harm before they are even fully articulated. There is an emerging, deeply harrowing scenario that represents perhaps the most acute failure of the current linear tapering paradigm, with parents of non verbal autistic children arriving in desperation, searching for answers the medical establishment refuses to give them.
The clinical context here is vast but quietly ignored. While the evidence for using SSRIs to treat the core traits of autism is notoriously mixed, they remain a staple of pediatric psychiatric prescribing. Estimates suggest that SSRIs account for roughly 20% to 35% of all psychiatric prescriptions for autistic children and adolescents, frequently deployed to manage secondary behaviors like anxiety, obsessive tendencies or irritability.
The crisis begins when a clinician decides to stop the antidepressant. Operating under outdated guidelines, they implement a rapid, linear taper, cutting doses by halves or quarters over a matter of weeks.
When a non verbal child undergoes the neurological chaos of acute withdrawal, they cannot say, "I have akathisia, my body feels like it is surging with electricity, I have body wide nerve pain, and I feel an extreme panic and anxiety, like I’m being chased by an axe murderer." Instead, their nervous system reacts to the chemical destabilisation the only way it can, often through intense somatic distress, extreme anxiety, sleeplessness and escalations into aggressive or violent behavior.
Due to the fact the child cannot articulate their internal state, the prescribing clinician almost invariably misinterprets these withdrawal symptoms as a "relapse" or an "exacerbation of their baseline autistic behavior." The consequences of this diagnostic error are devastating. The clinician falls into a diagnostic trap where withdrawal is used as retroactive justification that the child "needed" the drug all along, which frequently leads to heavy handed clinical escalation. Instead of recognising a destabilised central nervous system, psychiatrists often double down, introducing heavier, more sedating neuroleptics or antipsychotics to chemically restrain the behavior.
The turning point for these families happens at home. Parents, who know their children better than any clinician, begin to notice a fundamental disconnect. The terrifying, violent or profoundly anxious behaviors emerging after the taper look nothing like the child’s baseline difficulties prior to the SSRI. It isn't a return of the old behaviour, it is an entirely new, foreign state for their child.
Driven by instinct, these parents go online, discover withdrawal advocacy and land in support groups. There, they find an invisible community of hundreds of other parents witnessing the exact same tragic trajectory for their child. They are beginning to create splinter groups for non verbal autistic children in withdrawal.
Hearing these devastating stories day in and day out as a moderator is both heartbreaking and deeply alarming. It forces you to watch a systemic failure play out in real time, where desperate families are stuck between a rigid medical system wilfully blind to the realities of linear tapering and a non verbal child locked inside a chaotic nervous system, unable to articulate their suffering.
I hope sharing this brings some vital visibility to these children and their parents, especially as withdrawal advocacy gains traction and new clinical guidelines begin to roll out worldwide.
1
3
31
2,071
Sam Hall retweeted
“Estimates suggest that #SSRIs account for roughly 20% to 35% of all psychiatric prescriptions for autistic children and adolescents, frequently deployed to manage secondary behaviors like anxiety, obsessive tendencies or irritability.”
Important post by @samhall404 👇
Jun 8
As a moderator in antidepressant withdrawal support spaces, you eventually learn to spot the patterns of iatrogenic harm before they are even fully articulated. There is an emerging, deeply harrowing scenario that represents perhaps the most acute failure of the current linear tapering paradigm, with parents of non verbal autistic children arriving in desperation, searching for answers the medical establishment refuses to give them.
The clinical context here is vast but quietly ignored. While the evidence for using SSRIs to treat the core traits of autism is notoriously mixed, they remain a staple of pediatric psychiatric prescribing. Estimates suggest that SSRIs account for roughly 20% to 35% of all psychiatric prescriptions for autistic children and adolescents, frequently deployed to manage secondary behaviors like anxiety, obsessive tendencies or irritability.
The crisis begins when a clinician decides to stop the antidepressant. Operating under outdated guidelines, they implement a rapid, linear taper, cutting doses by halves or quarters over a matter of weeks.
When a non verbal child undergoes the neurological chaos of acute withdrawal, they cannot say, "I have akathisia, my body feels like it is surging with electricity, I have body wide nerve pain, and I feel an extreme panic and anxiety, like I’m being chased by an axe murderer." Instead, their nervous system reacts to the chemical destabilisation the only way it can, often through intense somatic distress, extreme anxiety, sleeplessness and escalations into aggressive or violent behavior.
Due to the fact the child cannot articulate their internal state, the prescribing clinician almost invariably misinterprets these withdrawal symptoms as a "relapse" or an "exacerbation of their baseline autistic behavior." The consequences of this diagnostic error are devastating. The clinician falls into a diagnostic trap where withdrawal is used as retroactive justification that the child "needed" the drug all along, which frequently leads to heavy handed clinical escalation. Instead of recognising a destabilised central nervous system, psychiatrists often double down, introducing heavier, more sedating neuroleptics or antipsychotics to chemically restrain the behavior.
The turning point for these families happens at home. Parents, who know their children better than any clinician, begin to notice a fundamental disconnect. The terrifying, violent or profoundly anxious behaviors emerging after the taper look nothing like the child’s baseline difficulties prior to the SSRI. It isn't a return of the old behaviour, it is an entirely new, foreign state for their child.
Driven by instinct, these parents go online, discover withdrawal advocacy and land in support groups. There, they find an invisible community of hundreds of other parents witnessing the exact same tragic trajectory for their child. They are beginning to create splinter groups for non verbal autistic children in withdrawal.
Hearing these devastating stories day in and day out as a moderator is both heartbreaking and deeply alarming. It forces you to watch a systemic failure play out in real time, where desperate families are stuck between a rigid medical system wilfully blind to the realities of linear tapering and a non verbal child locked inside a chaotic nervous system, unable to articulate their suffering.
I hope sharing this brings some vital visibility to these children and their parents, especially as withdrawal advocacy gains traction and new clinical guidelines begin to roll out worldwide.
4
8
403
Jun 8
As a moderator in antidepressant withdrawal support spaces, you eventually learn to spot the patterns of iatrogenic harm before they are even fully articulated. There is an emerging, deeply harrowing scenario that represents perhaps the most acute failure of the current linear tapering paradigm, with parents of non verbal autistic children arriving in desperation, searching for answers the medical establishment refuses to give them.
The clinical context here is vast but quietly ignored. While the evidence for using SSRIs to treat the core traits of autism is notoriously mixed, they remain a staple of pediatric psychiatric prescribing. Estimates suggest that SSRIs account for roughly 20% to 35% of all psychiatric prescriptions for autistic children and adolescents, frequently deployed to manage secondary behaviors like anxiety, obsessive tendencies or irritability.
The crisis begins when a clinician decides to stop the antidepressant. Operating under outdated guidelines, they implement a rapid, linear taper, cutting doses by halves or quarters over a matter of weeks.
When a non verbal child undergoes the neurological chaos of acute withdrawal, they cannot say, "I have akathisia, my body feels like it is surging with electricity, I have body wide nerve pain, and I feel an extreme panic and anxiety, like I’m being chased by an axe murderer." Instead, their nervous system reacts to the chemical destabilisation the only way it can, often through intense somatic distress, extreme anxiety, sleeplessness and escalations into aggressive or violent behavior.
Due to the fact the child cannot articulate their internal state, the prescribing clinician almost invariably misinterprets these withdrawal symptoms as a "relapse" or an "exacerbation of their baseline autistic behavior." The consequences of this diagnostic error are devastating. The clinician falls into a diagnostic trap where withdrawal is used as retroactive justification that the child "needed" the drug all along, which frequently leads to heavy handed clinical escalation. Instead of recognising a destabilised central nervous system, psychiatrists often double down, introducing heavier, more sedating neuroleptics or antipsychotics to chemically restrain the behavior.
The turning point for these families happens at home. Parents, who know their children better than any clinician, begin to notice a fundamental disconnect. The terrifying, violent or profoundly anxious behaviors emerging after the taper look nothing like the child’s baseline difficulties prior to the SSRI. It isn't a return of the old behaviour, it is an entirely new, foreign state for their child.
Driven by instinct, these parents go online, discover withdrawal advocacy and land in support groups. There, they find an invisible community of hundreds of other parents witnessing the exact same tragic trajectory for their child. They are beginning to create splinter groups for non verbal autistic children in withdrawal.
Hearing these devastating stories day in and day out as a moderator is both heartbreaking and deeply alarming. It forces you to watch a systemic failure play out in real time, where desperate families are stuck between a rigid medical system wilfully blind to the realities of linear tapering and a non verbal child locked inside a chaotic nervous system, unable to articulate their suffering.
I hope sharing this brings some vital visibility to these children and their parents, especially as withdrawal advocacy gains traction and new clinical guidelines begin to roll out worldwide.
4
18
49
4,014
Sam Hall retweeted
To the 'it's all psychosomatic or FND crowd' who seem to be out in full force at the moment: it would be quite peculiar for 100,000s of people to all develop FND a few days or weeks after stopping antidepressants or other psychiatric drugs. That would be some co-incidence!
And for those charming souls who are going for the 'these sort of people are really nutters and not a word they say can be taken at face value': in the US in some states more than 50% of people have been prescribed an antidepressant at some point in their life: that is a lot of nutters out there who can't be taken seriously!
The comments section to my blog is full of clinicians who did not believe stories about withdrawal until they went through it themselves, including psychiatrists, GPs and nurses: mhorowitz.substack.com/p/why…
But this blog probably needs to be updated at this point to include the point that there are none so blind as those who will not see.
13
36
115
8,411
Sam Hall retweeted

Thank you @MikhailaFuller for sharing my story with such care. My story reflects the experience of countless others, and I am so grateful for the way you continue to shine a light on the devastating realities of psychiatric medication harm. 🤍💊
I encourage everyone to check out Prescribed-Harm.com : an incredible resource created by Mikhaila. It is one of the most comprehensive yet accessible resources on psychiatric medication harm and withdrawal, featuring scientific research, resources for those struggling and hundreds of firsthand stories of psych med injury—all brought together in one place.
If you feel comfortable, consider sharing your own story. Every story matters!
You are not an anecdote❤️
3
16
95
16,452