
Urologist @nhsUHLG | National Audit @BAUSUrology | Urological Education | Interested in technology in general | Father of 4 | views my own
Joined September 2020
- Tweets 2,046
- Following 1,051
- Followers 1,519
- Likes 2,869
465 Photos and videos











Rob Calvert retweeted
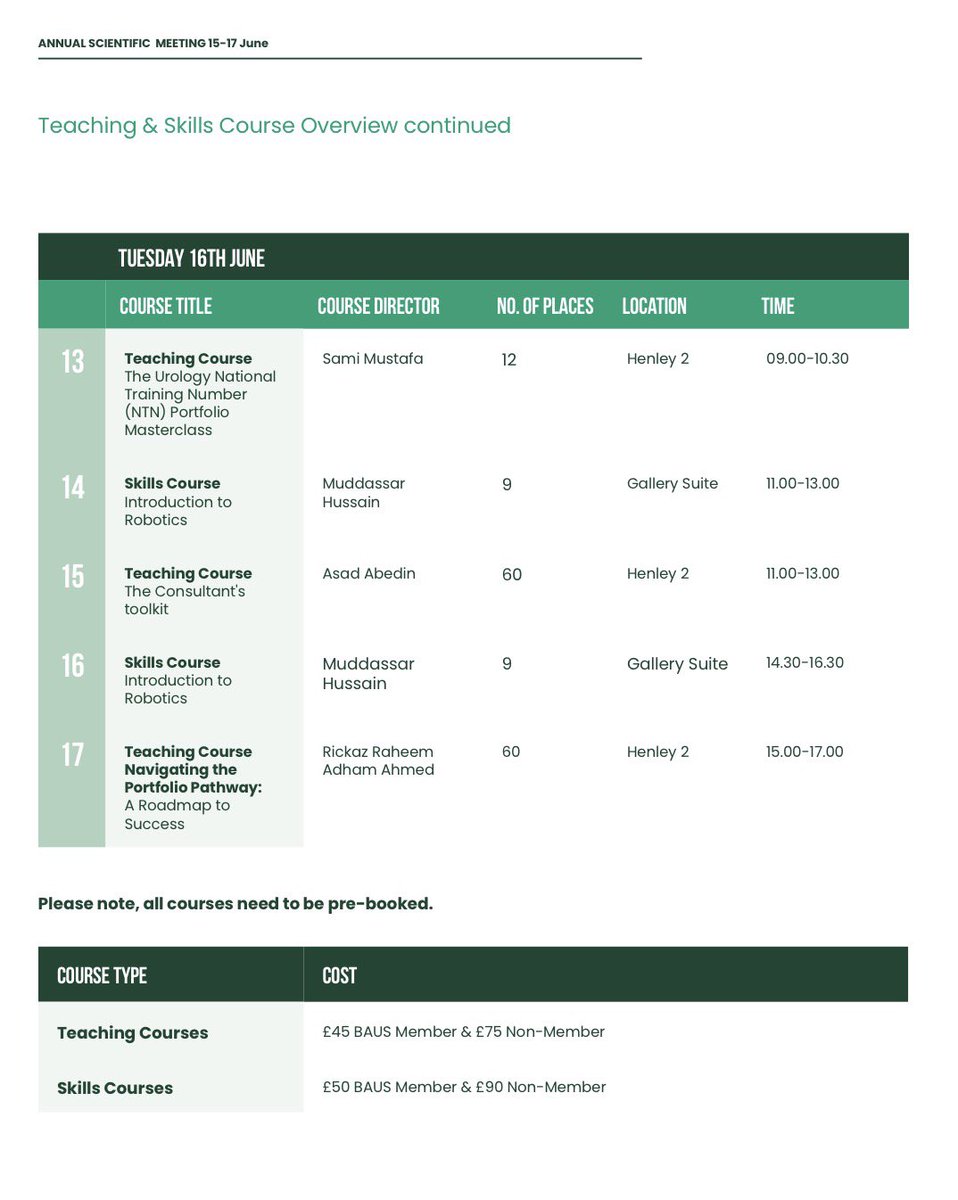
Heading to #BAUS26? Don’t forget there is still time to register for our plethora of teaching courses - including Navigating the Portfolio Pathway led by our SSTU colleagues 👇 come see us at registration tomorrow to sign up

1
2
78

Jun 12
Turning data into better care - @BAUSurology National audits plenary
*BREAKING NEWS*
Results from BOOMERANG (recurrent UTIs), National BOO surgery audit, Penile # audit and EMPAST (testicular cancer)
Monday 13.45 👀 Olympia
3
8
447
Jun 10
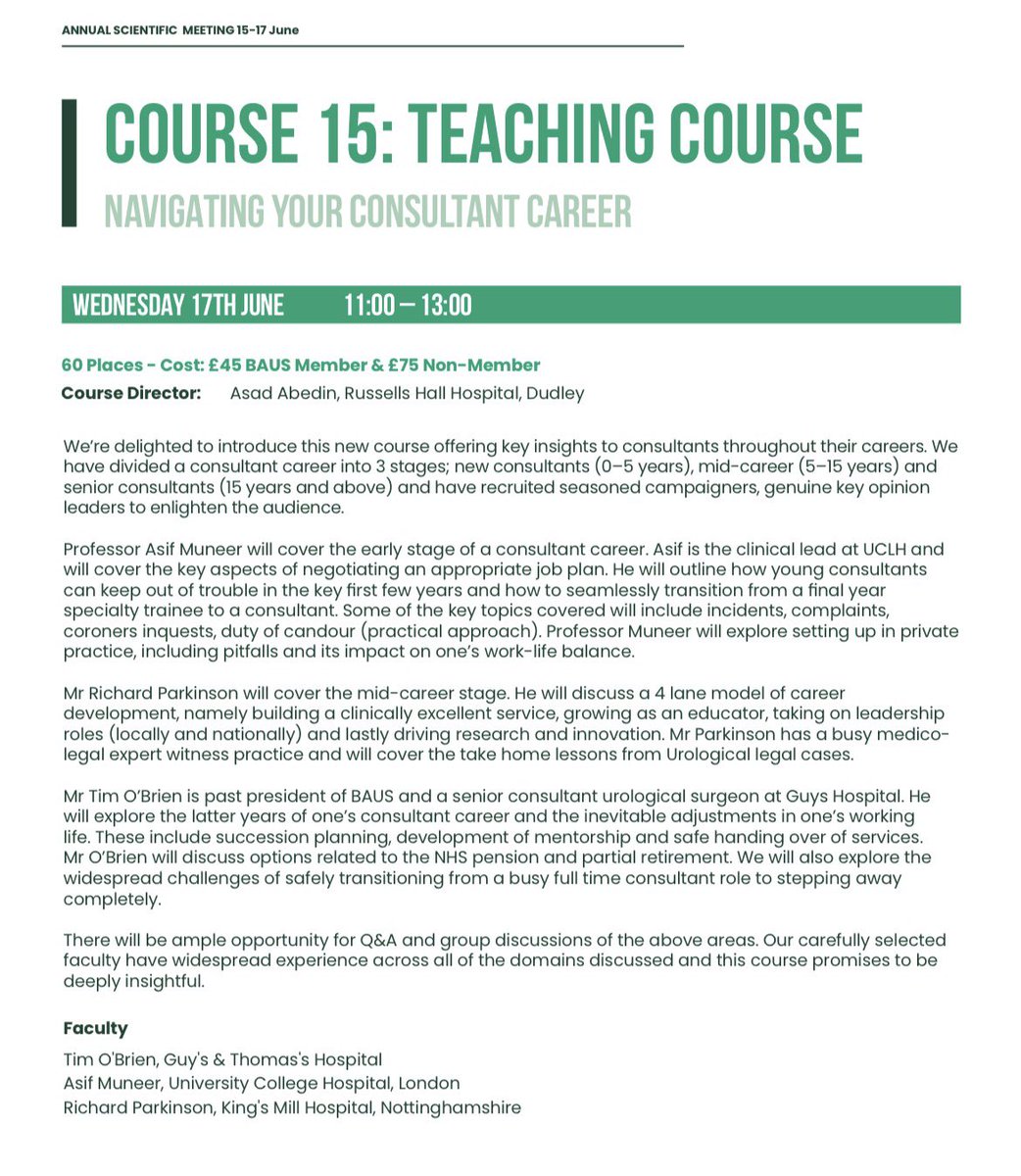
Navigating your Consultant Career. New course @BAUSurology with Asad Abedin, Richard Parkinson, Asif Muneer and Tim O’Brien. Get the best from your career at each stage. Book today or at the meeting.
3
6
711

GLP-1 drugs, like Ozempic and Mounjaro, keep doing things in places that have nothing to do with appetite. Bladder cancer is the newest.
In high-risk early bladder cancer treated with BCG, patients who happened to be on a GLP-1 were 57% less likely to progress to invasive disease, and 35% less likely to die of any cause. Almost 1,600 patients, matched head to head.
Read the fine print before you celebrate. This is propensity-matched data, so it’s a strong association and the randomized trial hasn’t happened.
Then the strange part. The tumor recurrence rate didn’t budge at all, only the progression and the deaths did, which is a real clue about how a hunger drug might be touching cancer at all.

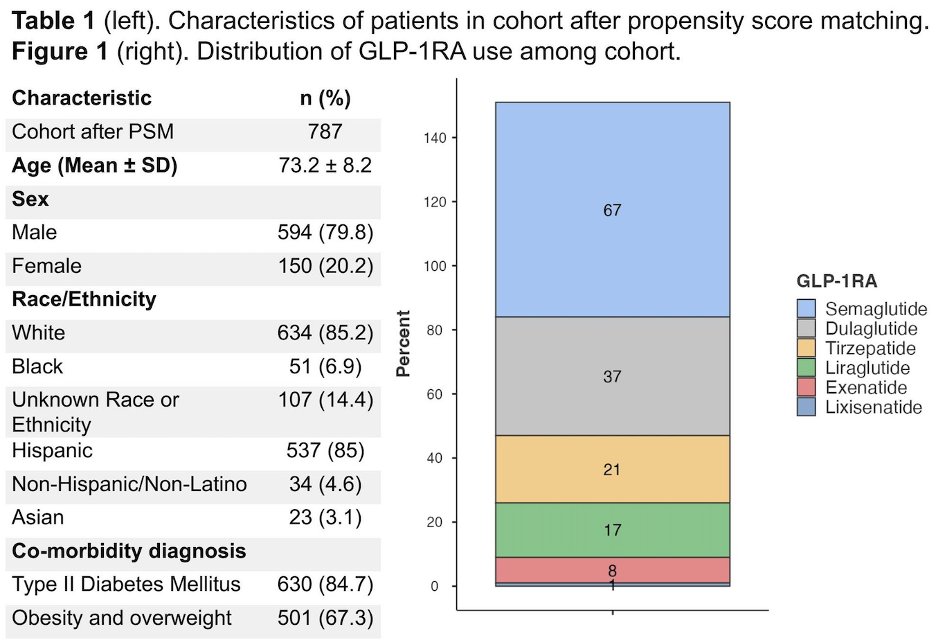
#ASCO26 Provocative PSM data presented evaluating GLP-1 RA exposure in high-risk NMIBC patients receiving BCG:
After matching:
🔹 791 GLP-1RA exposed patients
🔹 787 matched controls
GLP-1RA exposure was associated with:
🔹 Reduced risk of progression to MIBC →RR 0.43 (p=0.018)
🔹 Reduced all-cause mortality →RR 0.65 (p=0.017)
🔹 No significant differences in NMIBC recurrence, radical cystectomy, or distant metastasis rates.
@UroToday @ASCO

15
31
260
67,741
Rob Calvert retweeted

Studies suggest role of GLP-1s in cancer prevention, including the anti-inflammatory properties of these drugs. The studies presented at American Society of Clinical Oncology #ASCO meeting throws some interesting insights. reuters.com/business/healthc…
1
10
30
4,543
Jun 6
80% disease free survival at 1 year in bladder preserving Rx for MIBC using durvalumab and chemoradiotherapy. A significant step up from historical controls @Prof_Nick_James

#ASCO26 🔬 Abstract 4504 | RAD-IO
Durvalumab chemoradiotherapy in muscle-invasive bladder cancer
Presented by Nicholas D. James, PhD, MBBS, FRCP
@OncoAlert
@ASCO
Bladder preservation in MIBC remains one of the most important curative-intent questions in GU oncology.
The key question here:
➡️ Can immune checkpoint inhibition be safely integrated with standard chemoradiotherapy?
RAD-IO evaluated durvalumab with bladder-directed chemoradiotherapy using 5-FU mitomycin C in patients with muscle-invasive bladder cancer.
🧪 Study design
Stage 2 efficacy cohort:
• T2 N0–2 M0 MIBC
• CRT durvalumab
• Single-arm phase II design
• Primary endpoint: 12-month disease-free survival
• 12-month DFS used as a surrogate for longer-term outcome
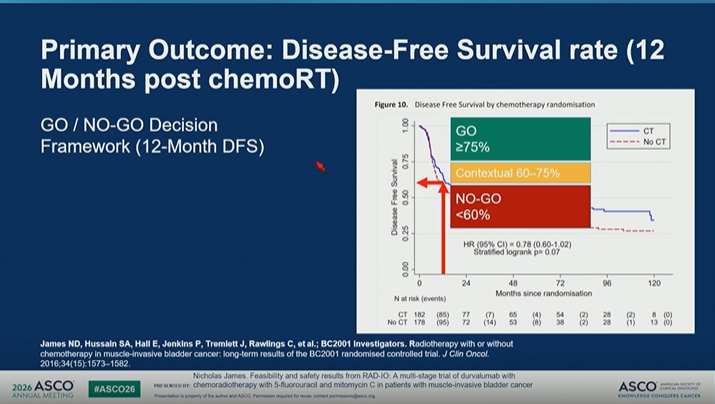
The trial used a clear GO / NO-GO framework:
🟢 GO: DFS ≥75%
🟡 Contextual: 60–75%
🔴 NO-GO: <60%
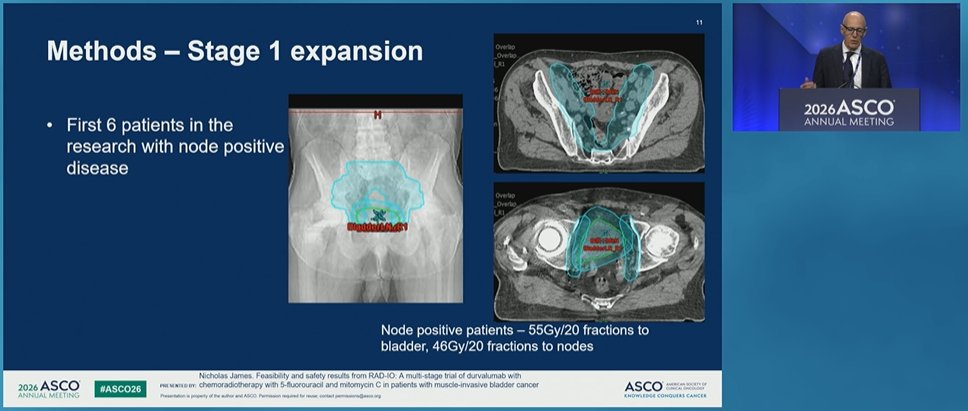
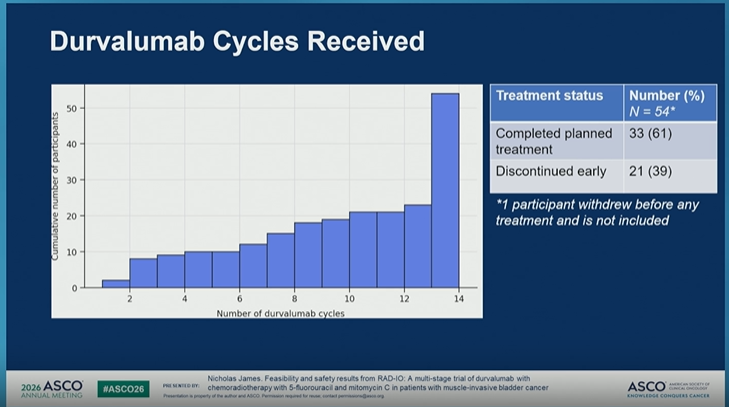
📌 Feasibility
Among 54 participants who started treatment:
• 100% received full radiotherapy: 55 Gy in 20 fractions
• 0 stopped radiotherapy early
• 87% had no RT extension or delay
• 100% received mitomycin C
• 100% received week 1 5-FU
• 78% received week 4 5-FU
• 61% completed planned durvalumab
• 39% discontinued durvalumab early
So, delivery of CRT was highly feasible, while immunotherapy completion was more challenging.
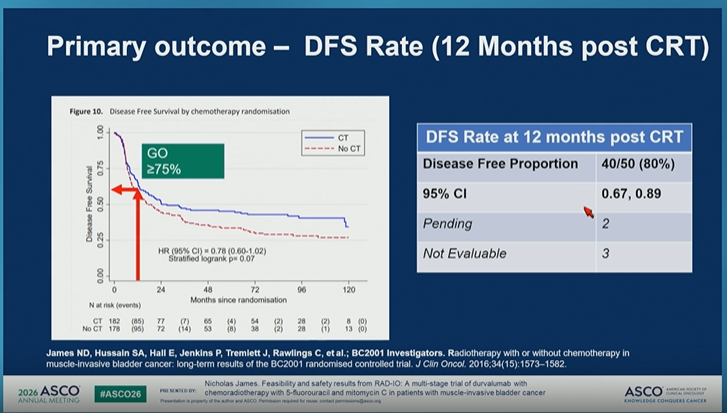
📊 Primary outcome
At 12 months post-CRT:
• DFS rate: 80%
• 40/50 disease-free
• 95% CI: 0.67–0.89
This crossed the prespecified GO threshold.
Secondary outcome PFS was consistent:
• No event: 83.6%
• Distant metastasis: 9.1%
• Local disease: 7.3%
💬 My take
RAD-IO provides an encouraging signal that durvalumab can be integrated with bladder-preserving chemoradiotherapy in MIBC.
But this is not yet practice-changing.
Important caveats:
🔹 single-arm phase II design
🔹 12-month endpoint
🔹 no randomized comparator
🔹 durability and late toxicity remain critical
🔹 completion of durvalumab was imperfect
Still, this is a very relevant direction.
In an era where systemic therapy is becoming increasingly active in urothelial cancer, bladder preservation strategies need to evolve too.
The next question is not simply whether CRT works.
It is:
➡️ Which patients are best suited for bladder preservation?
➡️ Can immunotherapy improve cure without compromising safety?
➡️ How should we integrate systemic therapy, radiation, surgery, and patient preference?
For MIBC, the future may be a more personalized curative-intent pathway — not one-size-fits-all cystectomy versus CRT.
#ASCO26 #GUOnc #BladderCancer #UrothelialCancer #MIBC #Immunotherapy #RadiationOncology #BladderPreservation
4
14
2,278
Rob Calvert retweeted

Jun 2
Brilliant news. Not full screening for every man yet, but a genuine step in the right direction. The extra £18m for the TRANSFORM trial will help find the best way to screen men for prostate cancer, with all eligible Black men aged 45 to 74 invited to take part. Not a national programme, but excellent progress. Well done to all involved.

BIG NEWS 📢
The Government has announced up to £18 million in additional funding for TRANSFORM - recognising the crucial role our trial is playing in shaping the future of #ProstateCancer screening.
➡️ Read more: bit.ly/4x9jOVE
#MensHealth l #Screening

ALT Breaking news banner with the text: 'Government backs our groundbreaking TRANSFORM trial with an additional £18 million in funding.'
1
5
14
6,445
Jun 2
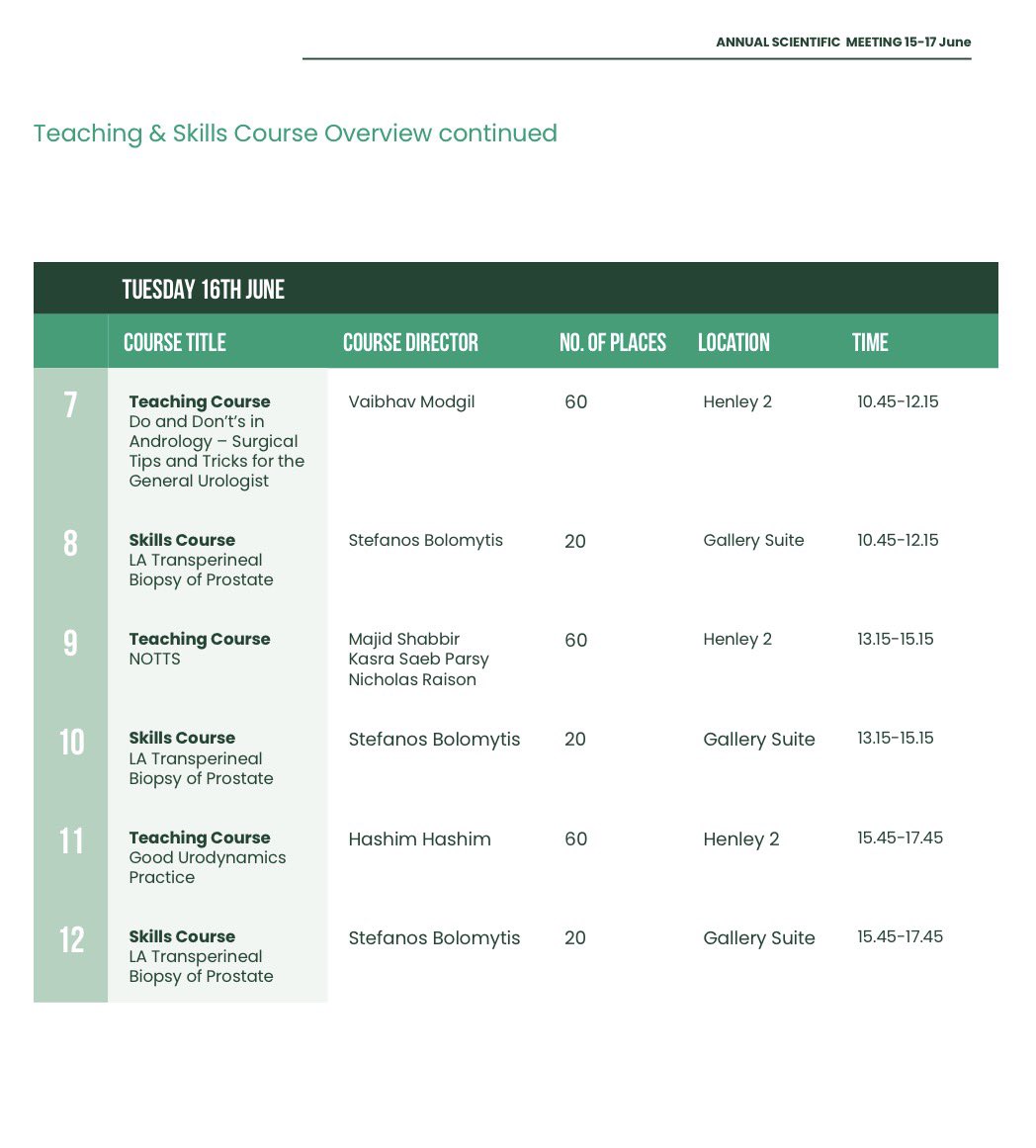
We have a wide range of interactive teaching and skills courses at the @BAUSurology annual scientific meeting to suit every career stage including some brand new courses.
Filling up fast- don’t miss out:
baus.org.uk/professionals/ev…
1
1
1
377
Rob Calvert retweeted

Jun 1
🗣️ BAUS Statement on the UK National Screening Committee Recommendation on Prostate Cancer Screening
▶️ Read our full statement here: baus.org.uk/professionals/ba…

2
8
17
1,442
Jun 1
Day 3 Bike4TUF - the home straight.
Edinburgh across to Fife, the Campsie fells and into Glasgow - tired legs
Please consider donating to @TUF_tweets
justgiving.com/page/robert-c…



1
15
359
May 30
Day 2 Bike4TUF - still going! Berwickshire and East Lothian coast into Edinburgh. Windy but scenic.
Please consider donating to @TUF_tweets
justgiving.com/page/robert-c…



1
13
317
May 29
Day 1 of the Bike4TUF challenge completed along the beautiful Northumberland coast. Next stop Scotland. Please consider supporting @TUF_tweets
@benchallacombe @tbivala1 @FolkardSam @benstarmer
justgiving.com/page/robert-c…

5
24
927
Rob Calvert retweeted

May 24
Humanoids are quietly crossing the line from lab demo to operational endurance machines.
What started as an 8 hour stress challenge just ran for 200 continuous hours without failure. The real breakthrough in robotics is persistence, reliability, spatial intelligence and long duration autonomy.
As humanoids scale into logistics, manufacturing, retail and real world navigation, they will need more than computer vision alone. They need to understand where they are, what surrounds them and how humans interact with space in real time...
"decentralized spatial infrastructure becomes important"
Projects like @AukiLabs are building machine perception layers that allow robots, devices and AI agents to share spatial understanding collaboratively.
trends most people are missing:
• Humanoid robotics is shifting from cloud dependent AI toward edge & distributed intelligence because latency becomes critical in physical environments
• Spatial mapping markets are expected to become foundational infrastructure for warehouses, smart cities and autonomous commerce
• Multi agent robotics systems will likely require shared localization protocols, similar to how the internet needed TCP/IP
• The next trillion dollar AI opportunity may not be chatbots, but embodied AI interacting with the physical world 24/7
200 hour uptime tests are a glimpse of what’s coming, companies building the robots will matter and protocols enabling machines to understand and coordinate in the real world would become even bigger
3
3
15
3,978
Rob Calvert retweeted

May 21
Cochrane updated its PSA screening meta-analysis. 789,086 men across 6 RCTs.
➡️ PCa-specific mortality: rate ratio 0.87 (moderate certainty)
➡️ Metastatic diagnosis: RR 0.65
➡️ Adverse events / QoL: little to no difference
Why this matters: 💡 PSA screening is back on stronger evidentiary footing for disease-specific mortality. Shared decision making still drives the recommendation downstream and additional tools (biomarkers and MRI) continue to improve the gap.
bit.ly/CochranePSA2026
@EBMUrology #ProstateCA #Screening #Cochrane #GUonc #AUA26

9
10
955
Rob Calvert retweeted

There is only one European nation with fewer hospital beds per capita than the UK
Sweden but they have the highest number of care home & nursing home beds
26% fewer care home beds
23% fewer nursing beds
Fewer hospital beds
Then people wonder why A&E is blocked




May 21

Since 2012 there's been a 26% decline in the number of care home beds in England per 100 people aged over 75, with a similar drop (23%) seen for nursing home beds.
Read our analysis of this indicator of health and care quality:
👉 buff.ly/kS8yTDr
#QualityWatch
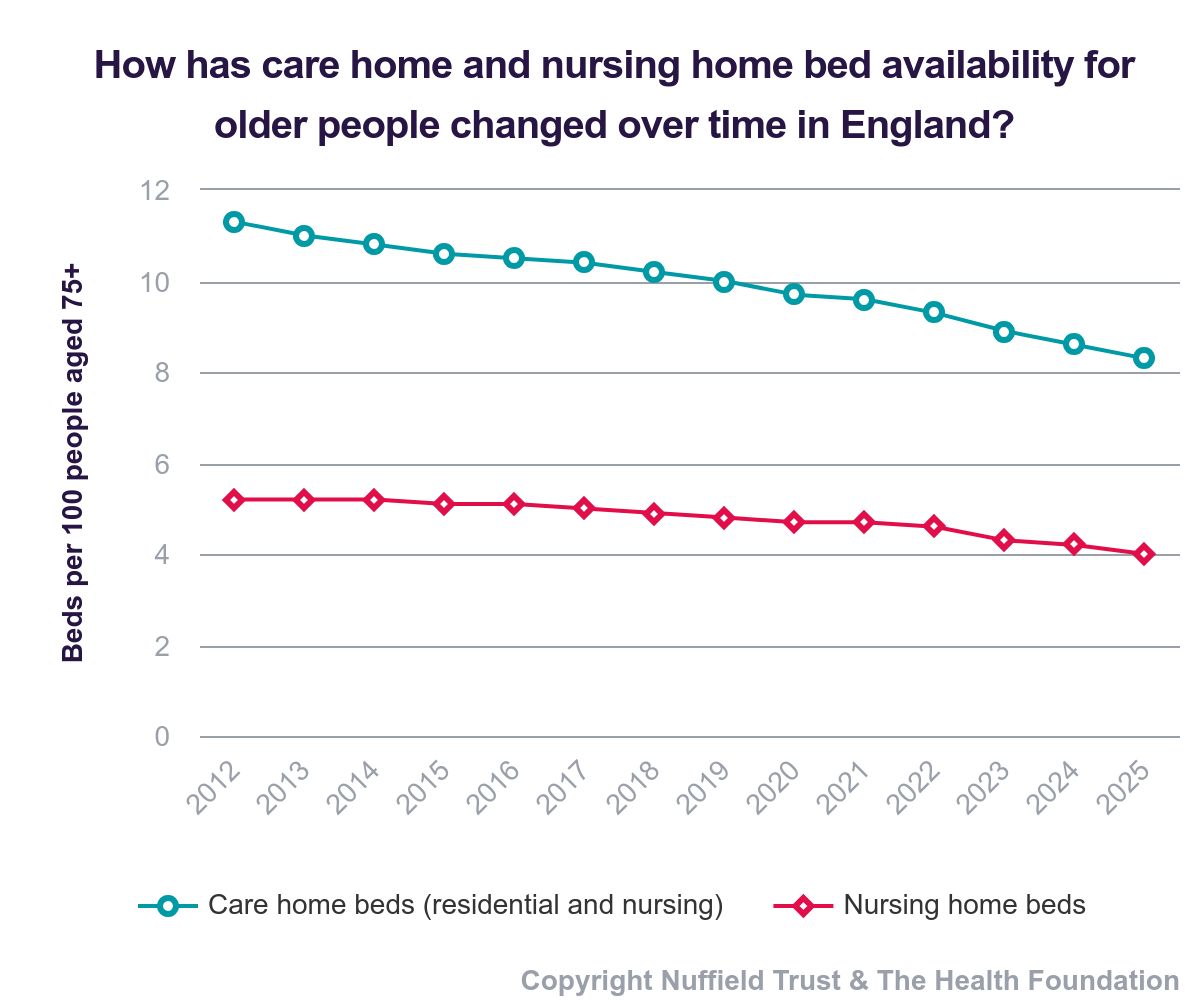
ALT Chart showing the trend in the number of care home beds and nursing home beds in England per 100 people aged over 75, between 2012 and 2025. There has been a 26% decline in the number of care home beds ad 23% decline in the number of nursing home beds. Follow the link in our post for more analysis.
6
236
309
16,628
Rob Calvert retweeted
May 7
Please considering supporting me as I take part in the Bike4TUF Challenge which will see us cycle from Newcastle to Glasgow via Edinburgh in 3 days. ~400km with 3,400m of climb.
justgiving.com/page/robert-c…
1
2
11
797