
he/him • Cardiologist • The 🫀 is my passion! #cardiotwitter #echofirst private account, not only work related tweets! Sometimes silly :3
Joined June 2023
- Tweets 9,425
- Following 1,081
- Followers 915
- Likes 70,085
347 Photos and videos











Pinned Tweet

23 Jun 2023
High sensitivity-cardiac #Troponin I and high sensitivity-cardiac Troponin T provide comparable diagnostic information regarding exercise-induced myocardial #ischemia. Overall, their diagnostic accuracy seems moderate.
#hsTroponin #Cardiology #Biomarker sciencedirect.com/science/ar…
2
29
11,312
Dr. Sou retweeted

💥 Answer these 3 questions before tomorrow's #ASEchoJC!
Q1. Which echocardiographic feature is MOST characteristic of the arrhythmic #MVP phenotype ⚡️?
#EchoFirst @HeartToProve @PWesslyMD @LucySafi
🧵(1/3)
21%
Isolated P2 prolapse
79%
Bileaflet prolapse MAD
0%
MV annular calcification
0%
Small central MR jet
39 votes • Final results
2
13
24
4,542

In a new blog post, Dr. Michelle Kittleson writes that clinical decisions should be driven by the patient’s medical needs, not by physician concerns about their status, expectations, or perceptions.
Read “Very Important Patients”: voices.nejm.org/doi/full/10.…
ALT NEJM Voices graphic with a quote from Michelle Kittleson, M.D., about evaluating medical interventions, emphasizing emotions and motivations. Colorful border at the top.
5
16
59
9,774

Posted With permission.
Male, age 94, retired surgeon, lean, walks daily.
Asymptomatic, brought in by visiting worried daughter who lives in North America.
BP 150/70(he confirms is accurate)
LDL 170
HbA1C 7.1, FBS 124
Refusing any treatment
Poll in 🧵
If I insist he’ll comply
3%
Insist on BP Rx
0%
BP & Metformin
8%
BP, Metformin, statin
89%
Let him be!
36 votes • Final results
9
3
16
7,400
May 19
Very hard!
May 16

Sadly, kids today will never know how hard this intro goes man...
1
37
@twj1974 this complication is not about you fixing it to show it in a meeting later, this is about saving a patient, patients die from complications…
Profound teaching! #EuroPCR
@PCRonline

1
3
14
1,262
May 12
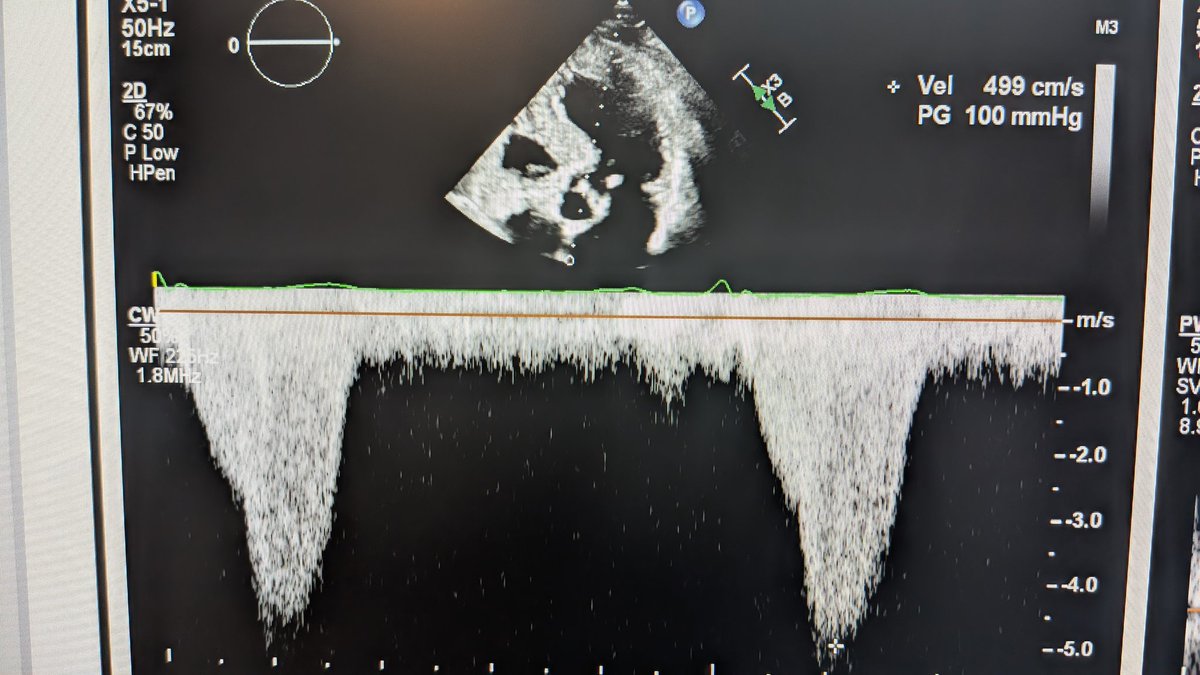
Austin flint

Can you connect this echo finding to a classic auscultatory sign?
1
11
840
Dr. Sou retweeted

⚠️ Low BP in HFrEF — should it stop us from using GDMT? Data says: probably not.
From COPERNICUS, PARADIGM-HF, RALES/EMPHASIS-HF & DAPA-HF:
✅ Carvedilol beneficial even at SBP 85–95 mmHg
✅ Sacubitril/Valsartan consistent across all BP strata
✅ MRA & SGLT2i similarly effective in low BP groups
Low SBP is a reason to be careful — not a reason to stop. 💡
#HeartFailure26 #HF2026 #HFrEF #GDMT #Cardiology

3
58
159
7,874
Dr. Sou retweeted

📚🤖 Congratulations.
We finally industrialized fake science.
And apparently… we even peer-review it now.
Basically AI is doing what human do ( 😁 ). Fake it til you make it.
We will need AI to vet what AI did in science.
This Lancet audit analyzed:
👉 2.5 million biomedical papers
👉 125 million references
And found something absolutely spectacular:
Thousands of completely fabricated citations inside peer-reviewed biomedical literature.
Not “slightly wrong.”
Not “formatting issues.”
I mean:
👉 studies that literally do not exist.
And the trend is exploding.
📈 Fabricated-reference rate:
~4 per 10,000 papers in 2023
→ ~57 per 10,000 papers by 2026
That’s a >12-fold increase.
But here’s the funniest part.
These fake citations were:
✅ correctly formatted
✅ scientifically plausible
✅ assigned to real researchers
✅ with believable publication years
Basically:
AI became the world’s most confident pathological liar.
And peer review apparently responded with:
👉 “Looks academic enough to me.”
One masterpiece highlighted in the paper:
A surgical oncology article had:
18 fabricated references out of 30.
SIXTY (60%) PERCENT !!!!!!!!!.
At that point it’s not a bibliography anymore.
It’s speculative fiction with DOI formatting.
Even better
A rheumatology biomarker paper cited:
👉 a nematode worm study
Which honestly feels spiritually accurate for some biomarker papers.
The deeper problem
Medicine runs on citation chains.
Paper → review → meta-analysis → guideline → clinical decision.
So when fake citations enter the system:
we are no longer practicing evidence-based medicine.
We are practicing:
👉 autocomplete-based medicine.
And let’s be honest
This didn’t happen because AI is evil.
It happened because:
👉 productivity became more important than verification
👉 publication became more important than understanding
👉 quantity became more important than truth
AI simply exposed the system.
My favorite line in the paper (basically)
Most fabricated references:
👉 looked perfectly real
👉 survived peer review
👉 received no publisher action
98.4% remained untouched.
Translation
The system is currently optimized for: ❌ publication velocity
—not— ✅ epistemological integrity
My take
We are entering a dangerous phase of science: plausible knowledge inflation
Where papers increasingly sound scientific… without guaranteeing that the underlying evidence even exists.
Bottom line
The future of scientific publishing may depend less on:
👉 generating content
and much more on:
👉 verifying reality
⚡ Because once fake references become scalable…
fake certainty becomes scalable too.
One more thing: REAL EXPERTS (HUMAN) WILL BE EVEN MORE NEEDED AND BECOME EVEN MORE CENTRAL IN THE MANAGEMENT OF SCIENCE.
#AI #Science #ResearchIntegrity #MedicalPublishing #LLM #EvidenceBasedMedicine #AcademicMedicine #PeerReview

6
8
14
1,950
May 9
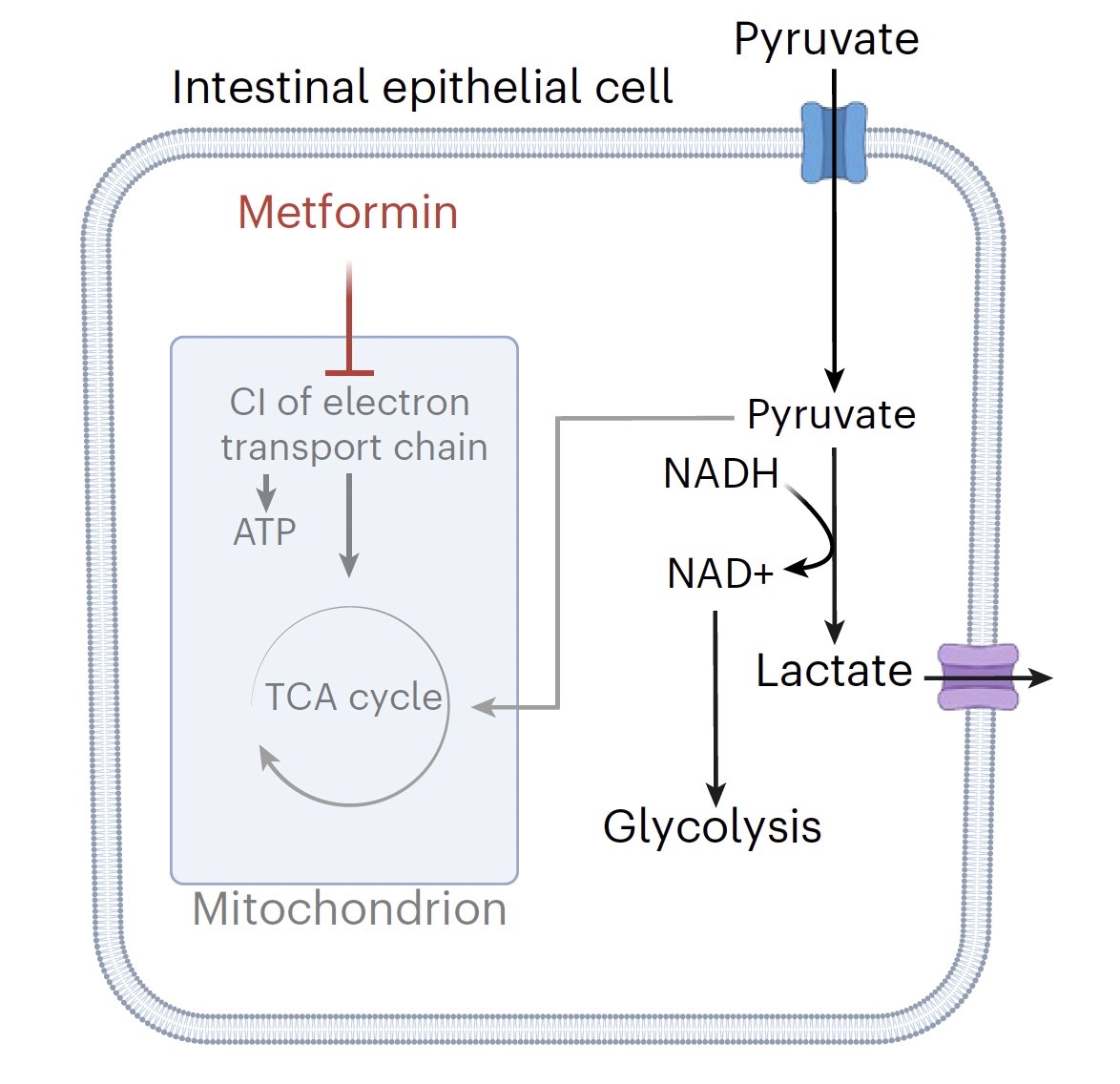
Now, this explains the side effects 😉
May 8

Metformin, one of the most commonly prescribed drugs, was thought to work via the liver. Check that. It's primarily through the gut. @NatMetabolism
nature.com/articles/s42255-0…
337
Dr. Sou retweeted

May 8
Metformin, one of the most commonly prescribed drugs, was thought to work via the liver. Check that. It's primarily through the gut. @NatMetabolism
nature.com/articles/s42255-0…
13
241
769
54,089
Dr. Sou retweeted
May 6
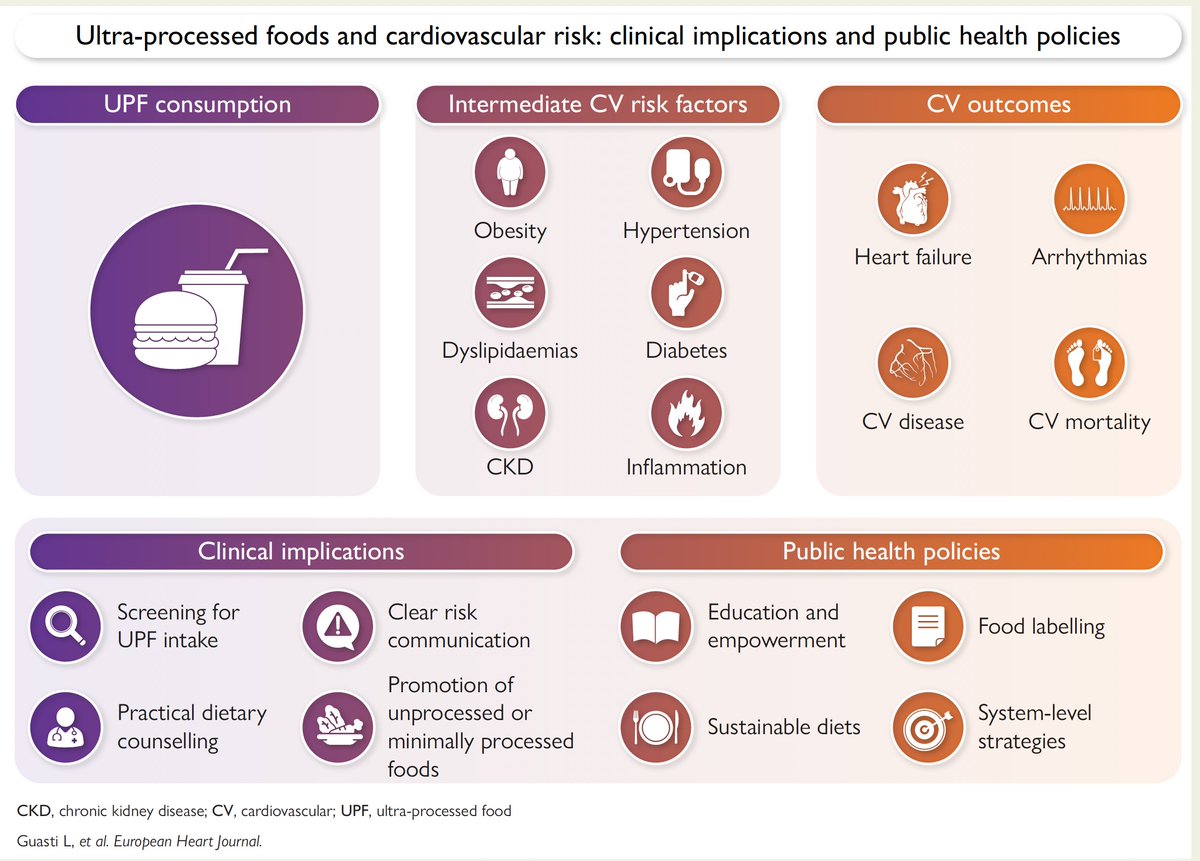
A consensus statement from @escardio today to limit intake of ultraprocessed foods for reduced risk of heart disease
academic.oup.com/eurheartj/a…
5
31
118
19,449
May 8
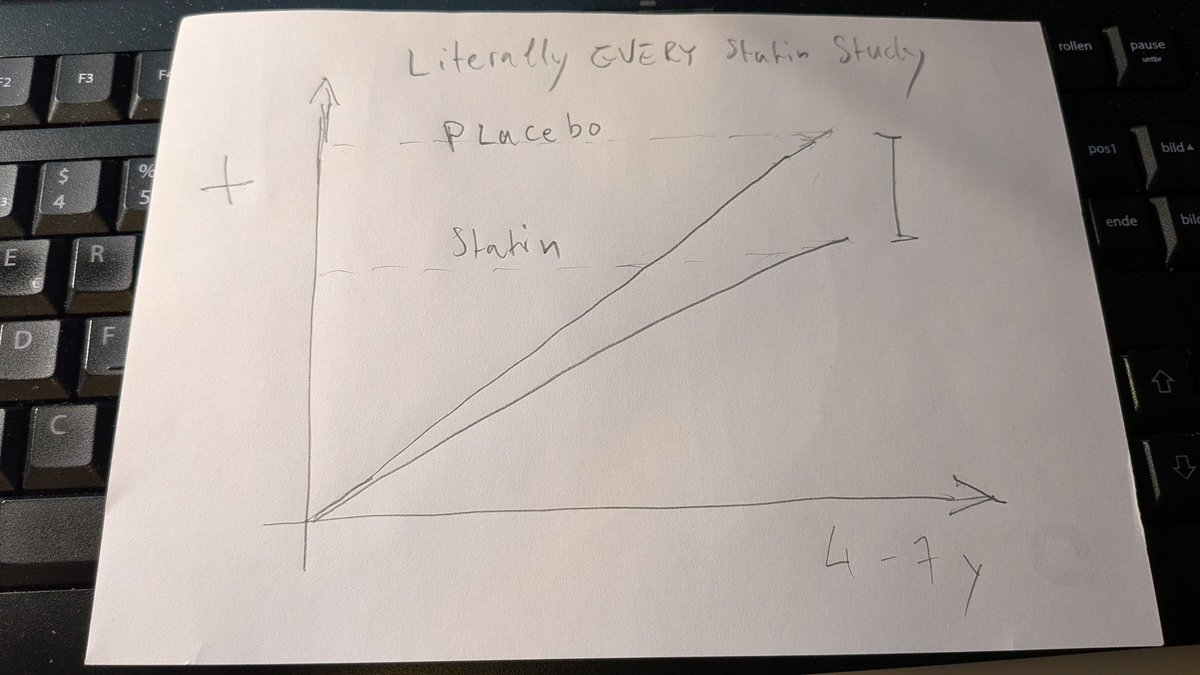
Please listen to actual cardiologists.
For 30 years, statin trials have repeatedly shown the same thing: after ~4–7 years, mortality was higher in the placebo group than in the statin group.
Every. Single. Time.
My sketch 👇🏻
May 7

5 things you need to know about statins medications according to a confused pharmacist! (1) #CardioTwitter #MedTwitter
9
5
36
11,675
Dr. Sou retweeted

50 plus slides of what you already know the word “alignment” = 15 million per hospital and the illusion of a “Strategy” … #cmgsays
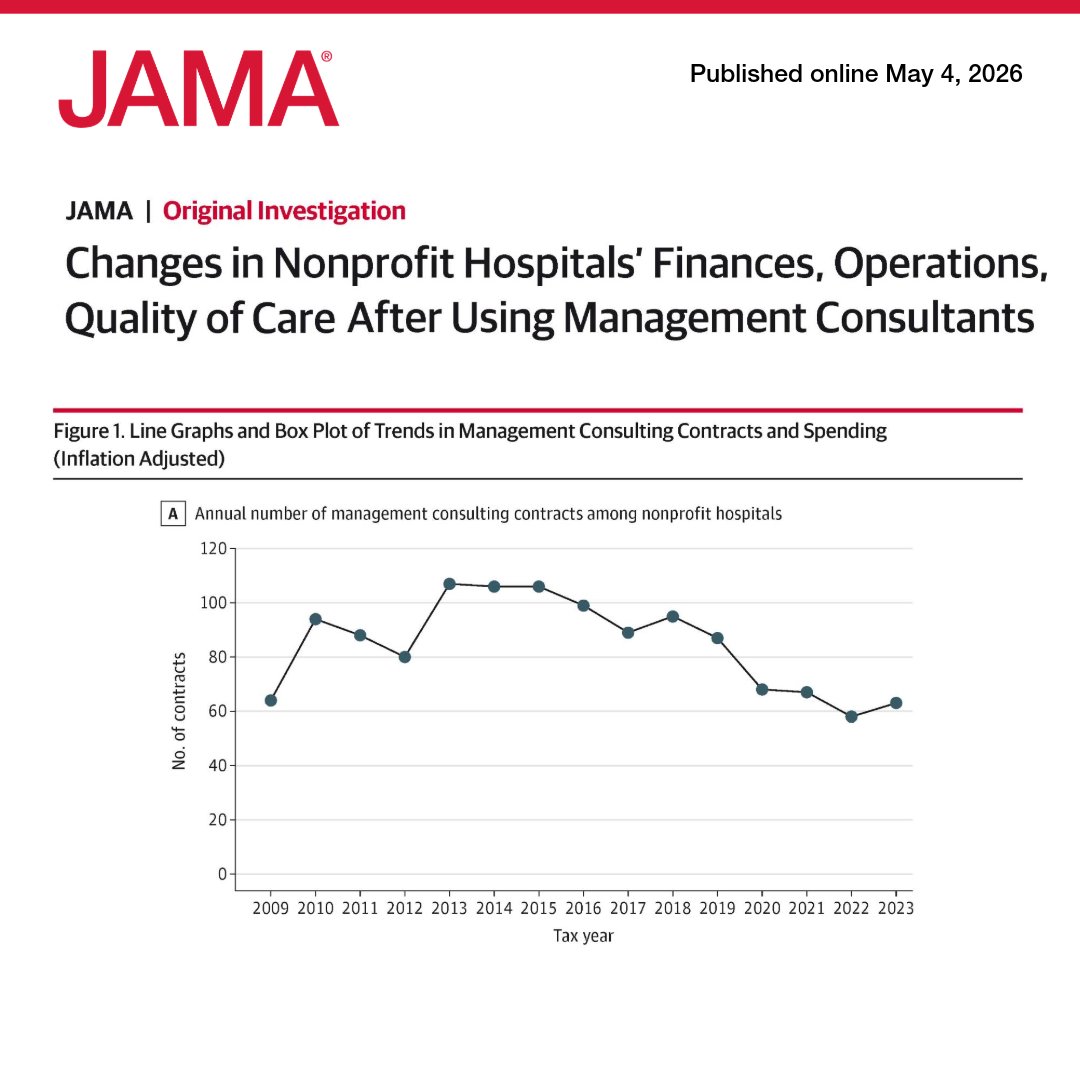
May 4

US nonprofit hospitals spent $7.8 billion on management consultants from 2009 to 2023, but contracts were not associated with meaningful changes in finance, operations, or quality of care. 🧵
ja.ma/4d46zfq
10
23
117
14,625
Dr. Sou retweeted

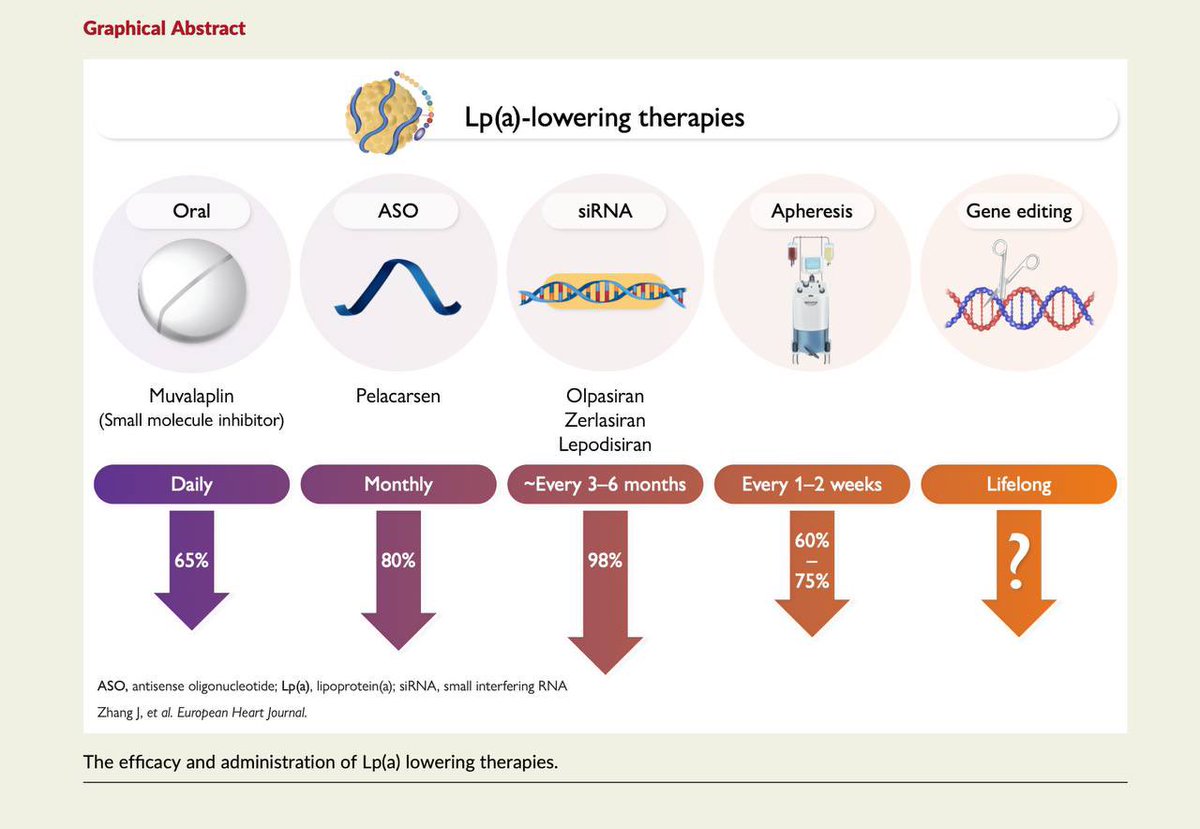
Lp(a) risk factor, unaffected by lifestyle/statins
New drugs:🧬
• Pela (ASO): ~80%⤵️'26
• Olpa (siRNA): 71-101%⤵️'26
• Lepo (siRNA): 94%⤵️ ↔️1.5y 1x💉
• Muva (oral): 86% Lp(a)⤵️
⚠️ Very low Lp(a) may ⬆️T2D
Until trials: 📏 Lp(a) once, ⬇️ LDL, 👀
📎 academic.oup.com/eurheartj/a…
5
43
130
12,217
Dr. Sou retweeted

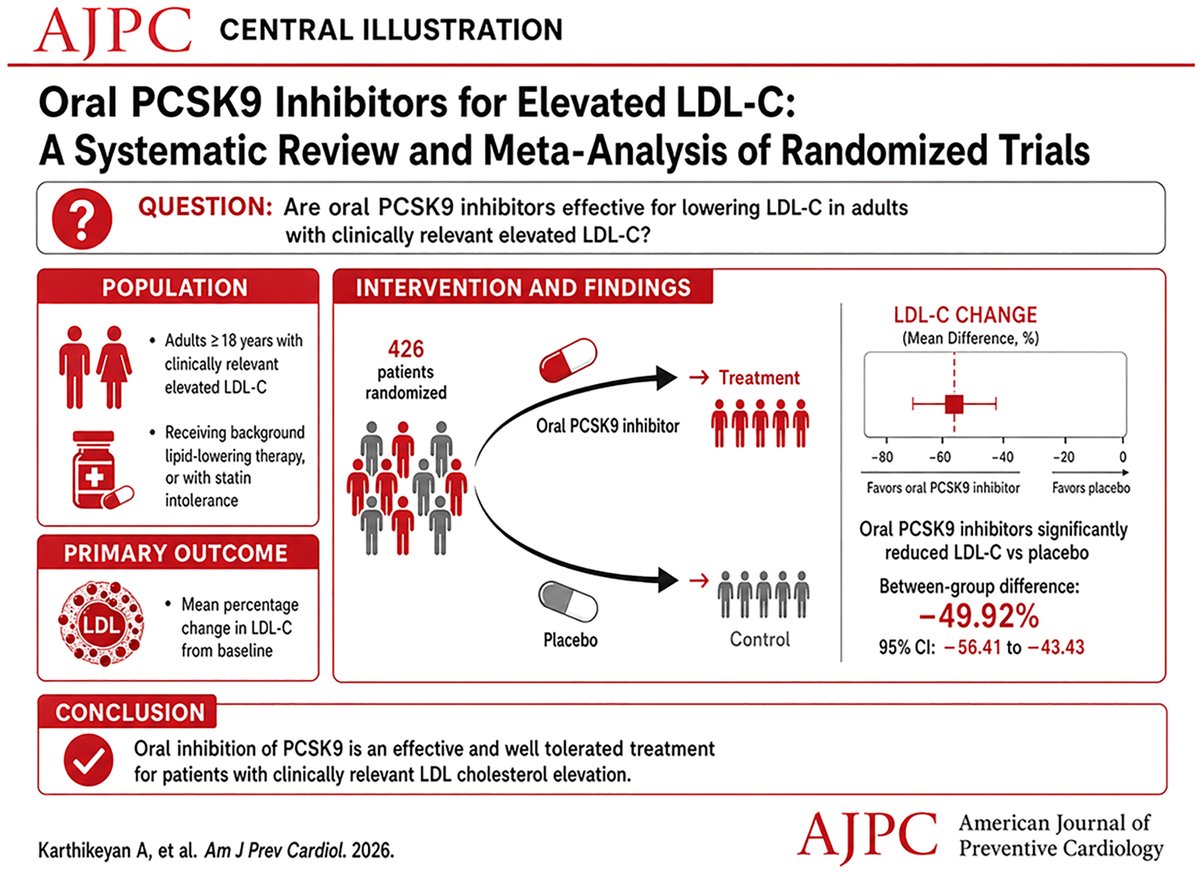
👉 Oral PCSK9 Inhibition: High-Efficacy Lipid Lowering Moves to the Oral Era
📍 Randomized evidence shows substantial LDL-C reduction (~50%) with oral PCSK9 inhibitors vs placebo
📍 Consistent effects across atherogenic parameters:
ApoB ↓ ~40–50%
Non-HDL-C ↓ ~45%
Lp(a) ↓ ~15–25%
📍 Safety profile comparable to placebo, including:
No excess adverse events
No signal for diabetes within available follow-up
1️⃣ MK-0616 (Enlicitide): Phase 3–Level Evidence
👆 LDL-C reduction ~60% at dose-aligned analyses
👆 ApoB reduction ~50%, supporting particle-level impact
👆 Minimal heterogeneity at consistent dosing
👆 Concordant reductions in non-HDL-C and Lp(a)
Pharmacodynamic profile:
👆 Tight coupling between LDL-C and ApoB reduction
👆 Consistent effect across study designs when exposure is standardized
2️⃣ AZD0780 (Laroprovstat): Mechanistic and Clinical Signal
Demonstrates significant LDL-C lowering in randomized trials
👆 LDL-C reduction ~50%
👆 Directionally consistent reductions in ApoB and other lipid parameters
👆 Contributes to reproducibility of oral PCSK9 pathway inhibition
Pharmacological attributes:
👆 Oral delivery with measurable systemic effect
👆 Supports class-level biological validity
📍 Integrated Lipid Effects
LDL-C reduction parallels ApoB lowering, consistent with enhanced clearance of ApoB-containing particles
Non-HDL-C reduction reflects broad impact on atherogenic lipoproteins
Lp(a) lowering is present but quantitatively smaller, aligning with partial LDL receptor–mediated clearance
📍 Conclusion
Oral PCSK9 inhibition achieves high-intensity lipid lowering with consistent effects across atherogenic markers and a favorable short-term safety profile.
👆 Next step: demonstration of cardiovascular outcomes to define its role in risk reduction strategies.
🔓 Open Access
🔗sciencedirect.com/science/ar…
@society_eas
@nationallipid
6
50
163
10,450
May 5
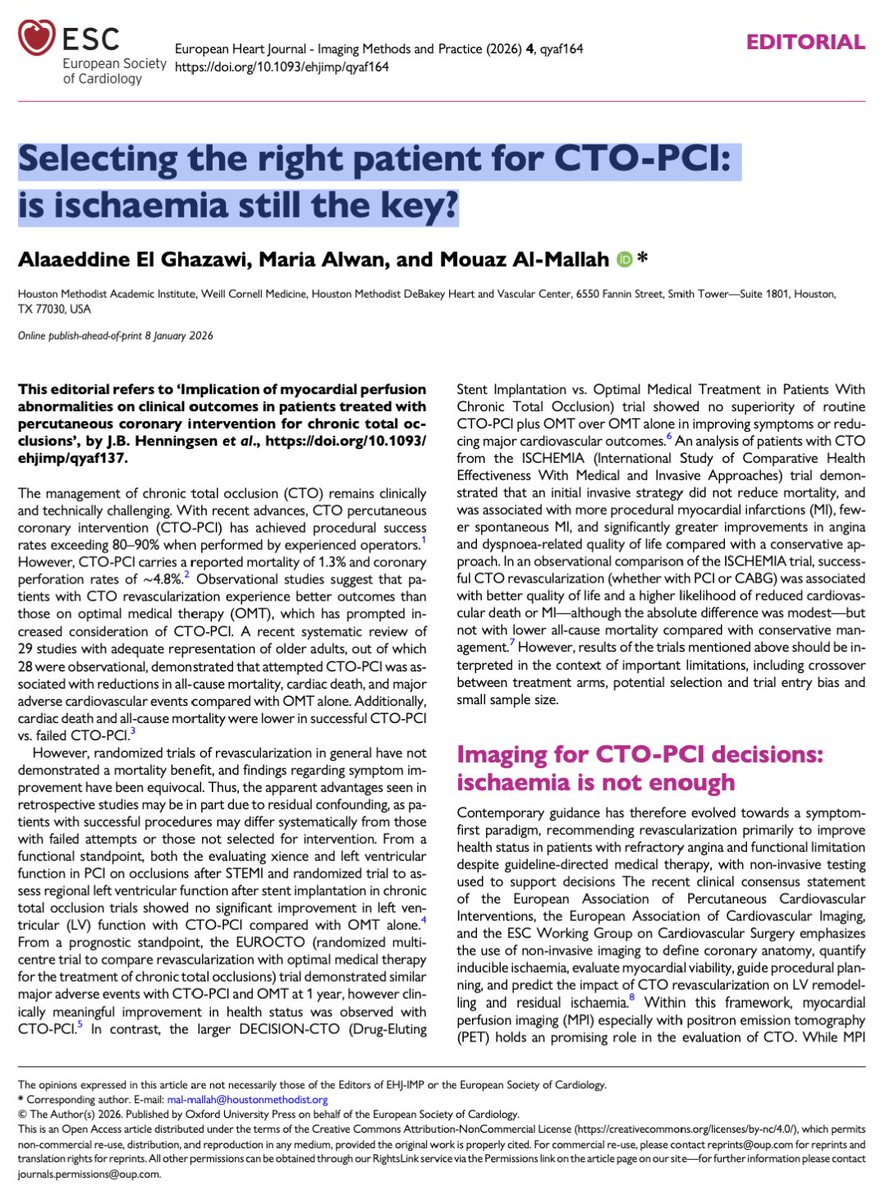
Dr. Cadematiri's final thought: If your indication for CTO-PCI is: “there is ischaemia” You’re already outdated.
The future is brutally simple: No symptoms → think twice
Symptoms → act Because in modern cardiology: The most important endpoint is not the image. It’s the patient!

🫀⚠️ We’ve been selecting patients for revascularization… wrong.
👉 ischemia = treat... not really?
For years the rule was simple:
👉 find ischaemia
👉 fix the artery
But what if ischaemia is NOT the key?
This editorial on CTO-PCI says something uncomfortable:
👉 Ischaemia does NOT predict outcomes.
Even when:
👉 ≥10% ischaemic burden
👉 PET or SPECT proven
There was:
❌ no reduction in death
❌ no reduction in hard events
So what actually improves?
👉 Symptoms.
👉 Quality of life.
That’s it.
Let that sink in.
We are:
👉 opening complex CTOs
👉 taking procedural risks
👉 chasing ischaemia
But:
⚠️ Ischaemia is NOT driving prognosis.
The real paradigm shift
From: ❌ Ischaemia-driven cardiology
To: 👉 Patient-driven cardiology
The new selection logic:
👉 refractory angina
👉 functional limitation
👉 patient suffering
FIRST.
Imaging?
Still crucial—but:
👉 as a SUPPORT tool, not the decision-maker
Even the paper states it clearly:
👉 Ischaemia alone is an insufficient arbiter for revascularization
And there’s a deeper problem
We love measurable things:
👉 % ischaemia
👉 flow reserve
👉 perfusion maps
But we ignore:
👉 symptoms
👉 daily function
👉 real patient experience
My take
This is the same cognitive error we see everywhere:
👉 We treat numbers
instead of
👉 treating patients
Final thought
If your indication for CTO-PCI is:
👉 “there is ischaemia”
You’re already outdated.
The future is brutally simple:
👉 No symptoms → think twice
👉 Symptoms → act
⚡ Because in modern cardiology:
The most important endpoint is not the image.
It’s the patient.
#Cardiology #CTO #PCI #Ischaemia #Imaging #PrecisionMedicine #CardiacCT #CardiacPET
2
9
1,746
May 3
Honestly, AR, along with TR, is the most challenging valvular lesion to quantify. This will be so helpful!

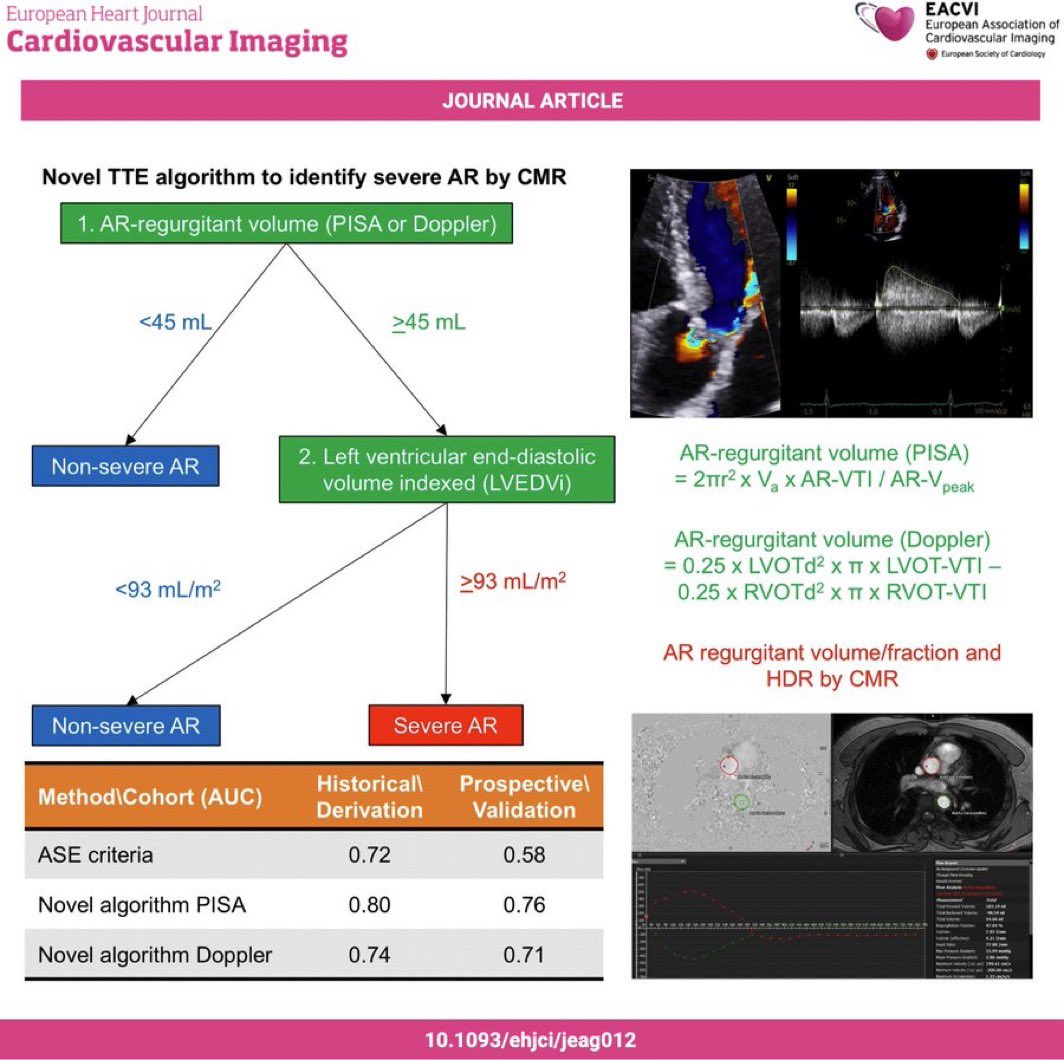
🫀 Grading severe aortic regurgitation — time to upgrade our TTE approach.
ASE criteria alone show an AUC of only 0.58 on prospective validation. This novel 2-step algorithm, benchmarked against CMR, does better:
1️⃣ AR regurgitant volume ≥ 45 mL (PISA or Doppler)
2️⃣ LVEDVi ≥ 93 mL/m²
→ Both met? Severe AR. AUC up to 0.76 with PISA method.
Simple. Reproducible. CMR-validated.
EHJ Cardiovascular Imaging — doi: 10.1093/ehjci/jeag012
#Cardiology #Echocardiography #AorticRegurgitation #ValvularHeartDisease #CMR #CardioTwitter #MedTwitter #EACVI
2
6
40
7,585
Dr. Sou retweeted
🫀 Grading severe aortic regurgitation — time to upgrade our TTE approach.
ASE criteria alone show an AUC of only 0.58 on prospective validation. This novel 2-step algorithm, benchmarked against CMR, does better:
1️⃣ AR regurgitant volume ≥ 45 mL (PISA or Doppler)
2️⃣ LVEDVi ≥ 93 mL/m²
→ Both met? Severe AR. AUC up to 0.76 with PISA method.
Simple. Reproducible. CMR-validated.
EHJ Cardiovascular Imaging — doi: 10.1093/ehjci/jeag012
#Cardiology #Echocardiography #AorticRegurgitation #ValvularHeartDisease #CMR #CardioTwitter #MedTwitter #EACVI
1
33
90
13,922
May 3
This is actually ground breaking.
As far as I know there was NO screening recommendation for CV disease. There are many for cancer but this one is the first recommendation for CV reduction 👏🏻
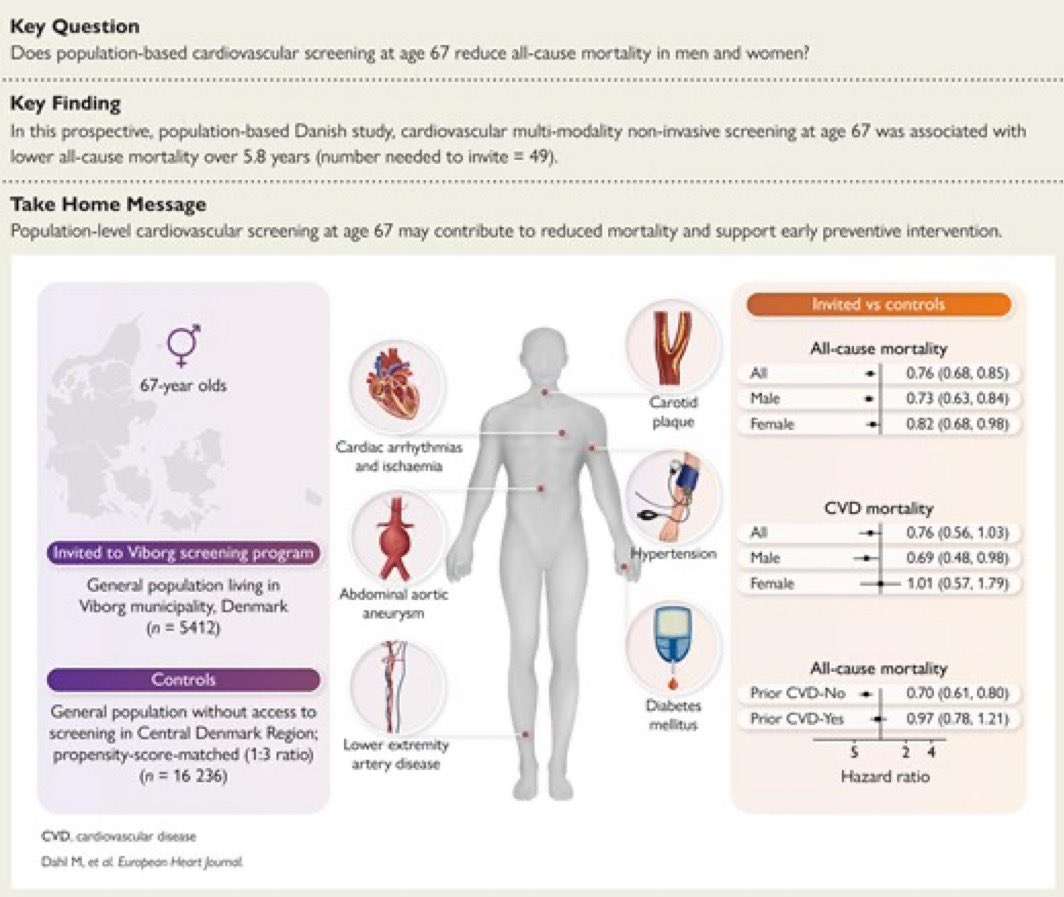
🫀 Cardiovascular screening at age 67 saves lives.
A Danish prospective study (n = 21,648) shows that non-invasive multimodal screening is associated with a 24% reduction in all-cause mortality over 5.8 years.
📊 Hazard ratio: 0.76 (CI 0.68–0.85)
👥 Number needed to invite to save 1 life: 49
✅ ECG, aortic ultrasound, carotid arteries, lower limbs, BP, diabetes screening…
One comprehensive check. Right age. Real impact.
➡️ Benefit strongest in men (HR 0.73) and those without prior CVD (HR 0.70).
Time to rethink population-level prevention? 🧵
Dahl M. et al. — European Heart Journal
#Cardiology #CardiovascularHealth #Prevention #Screening #CVD #HeartHealth #PublicHealth #Cardio #EHJ #EuropeanHeartJournal #MedTwitter #MedX #Cardiotwitter
1
1
317