
- Tweets 11,530
- Following 536
- Followers 5,937
- Likes 21,957












ALT A extreme close-up macro photograph of a Castor Bean Tick (Ixodes ricinus) perched on the edge of a vibrant green leaf. The small, reddish-brown arachnid is in a "questing" pose, clinging to the vegetation with its rear legs while extending its front legs outward into the air to detect a host. The background is softly blurred with natural green foliage, making the sharp details of the tick's body stand out.
ALT Female Banded Demoiselle

ALT Nurser Web Spider with egg sac

ALT Green-veined White butterfly

ALT Male Thick-legged Flower Beetle on a flower
ALT Side on macro shot of a green tiger beetle, a metallic green beetle with flashes of pink, and cream spots.




ALT Springtails can range in shape from the elongate entomobryomorphs to the rotund, globular symphypleonans. Macro-photography reveals details of the eyes, hairs, and patterns which are often crucial for identifying springtails to species level. Image credit: Tim Jonas, photographer.
ALT Close up face shot of a jumping spider, revealing the large, round anterior eyes. The spider is mainly black with orange on the tips of the legs and a few short, white hairs.


ALT Hairy Rove Beetle - Creophilus maxillosus. A 2cm rove beetle with distinctive pattern of creamy grey hairs on an otherwise dark body, shiny black thorax.
ALT Hairy Rove Beetle - Creophilus maxillosus. A 2cm rove beetle with distinctive pattern of creamy grey hairs on an otherwise dark body, shiny black thorax.
ALT Macro photo of Platybunus pinetorum, a well marked harvestman with a wide, brown ocularium, orange and dark black marking on the body and long white tubercles on the pedipalps.

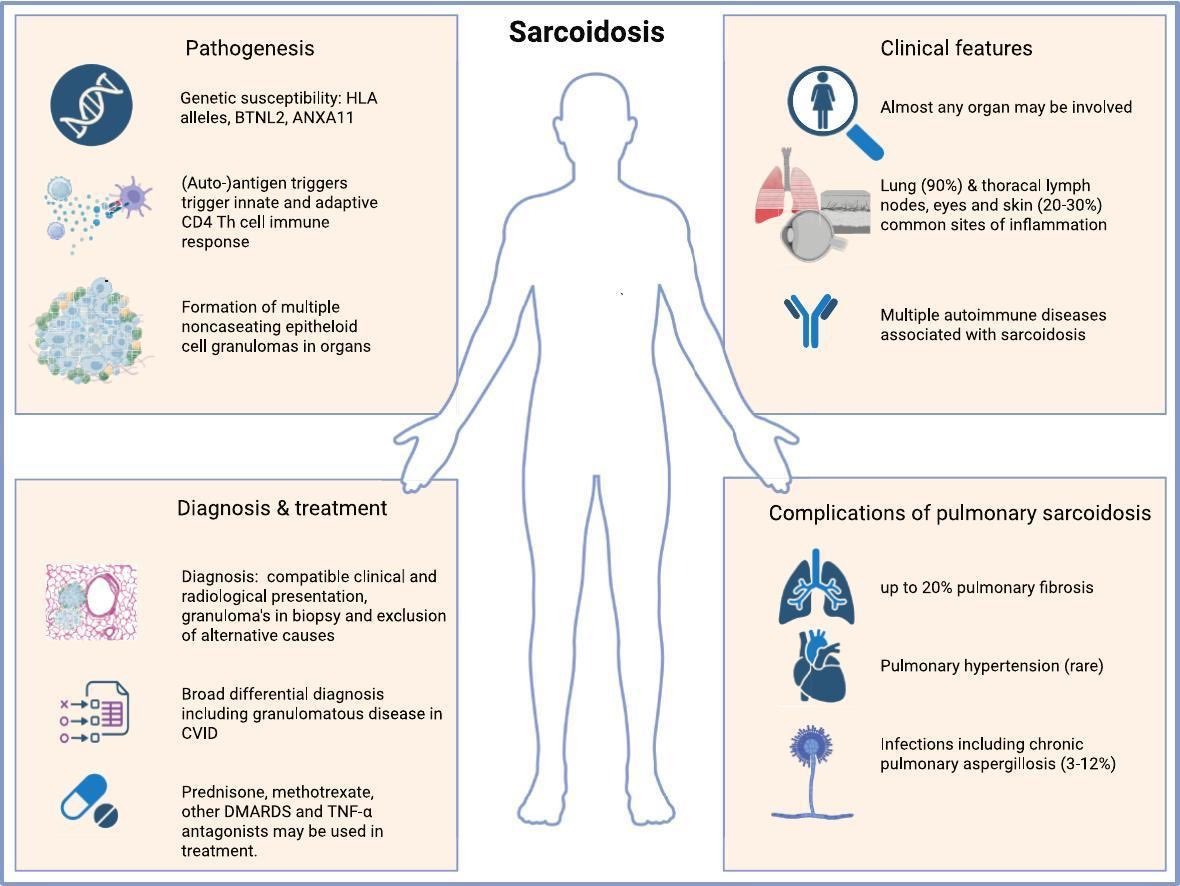
ALT Miedema J, Nunes H, Dalm VASH, Judson MA, Spagnolo P. Sarcoidosis: Disease mechanisms, diagnostic pathway and treatment. Autoimmun Rev. 2026 Mar;25(3):103993. doi: 10.1016/j.autrev.2026.103993. Epub 2026 Feb 4. PMID: 41651390.




ALT Macro shot of a harvestman (Rilaena triangularis), a speckled brown arachnid with proportionally large eyes on top of a single fused body.



ALT Something I haven't done much this year is get out and properly look for springtails, but I'm giving a talk on them in a couple a weeks so decided to grab the camera and find some inspiration. Plenty to be found in the woods up the hills of north Sheffield, including these eyeless Protaphorura aurantiaca springtails.

ALT Continuing the winter macro theme with a pot worm (Enchytraeid). Smaller cousins of the earthworm, these semi translucent worms are fantastic contributors to soil health. The tiny white blobs you can see inside are part of that process, revealing how the decaying organic matter, fungi and bacteria they've eaten are broken down and returned to the soil.

ALT Ptenothrix atra, a 'vary rare' pink/purple springtail - that I tend to find quite a lot...

ALT Another from this afternoon's walk in the woods. It's a 2-3mm Dicyrtomina saundersi, one of the globular springtails and probably the most common one I find.


ALT Close-up of an insect with iridescent, scale-like patterns covering its body and large compound eyes. Jumping bristletail, Dilta sp. (c) Tim Jonas 2023

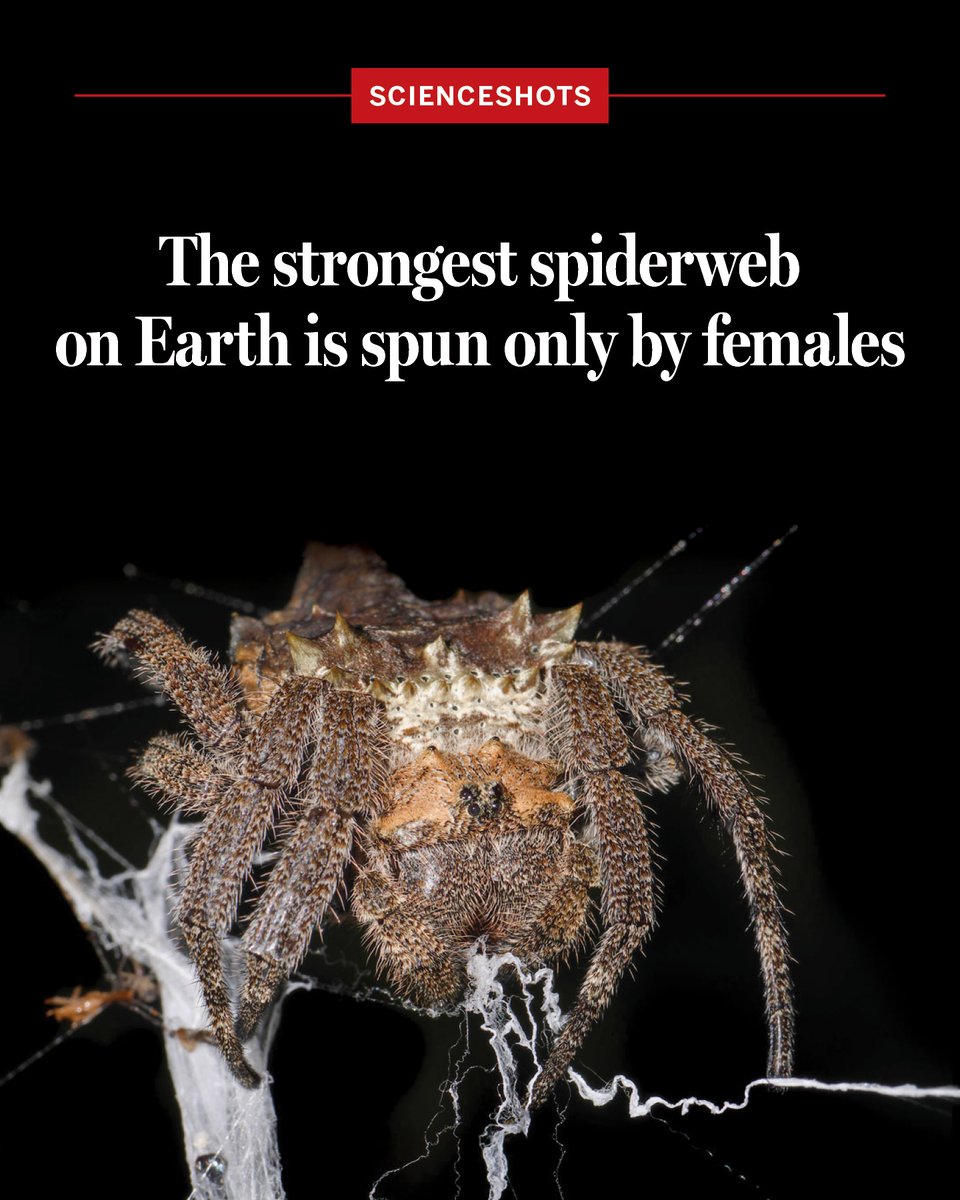
ALT The strongest spiderweb on Earth is spun only by females