
co-founder @bzinfocoalition, BIND survivor, dysautonomia, cancer, disabled
Joined October 2018
- Tweets 36,931
- Following 586
- Followers 4,060
- Likes 110,983
1,969 Photos and videos






jc retweeted

List of top New York heroes:
1. Firefighters during 9/11
2. Jalen Brunson
40
1,986
36,093
334,301
jc retweeted

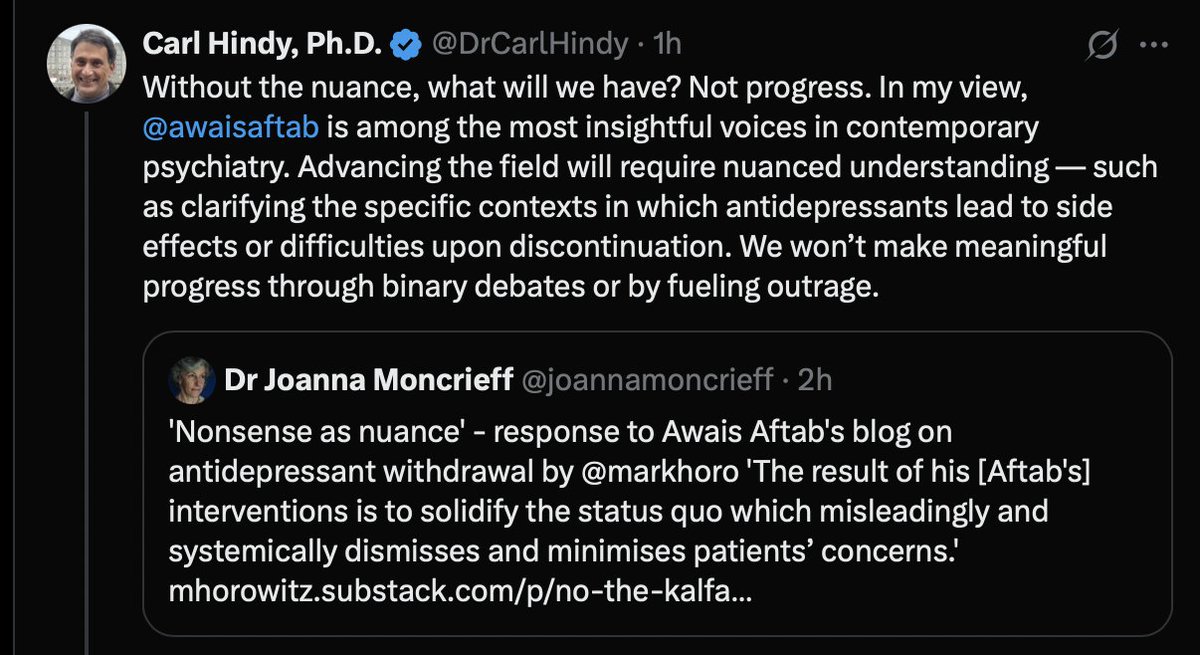
I do think this is true. I agree that there are lots of holes that further research would be very welcome to fill. But the fact that so much professional energy is being used to deny or minimise the issue or blame patients rather than trying to get to the bottom of what is happening and work on solutions (possible without perfect knowledge!) harms the credibility of psychiatry further and undermines faith that patients have in the specialty. The quicker it moves past to minimisation to constructive action the quicker it will re-build it reputation.
11h

The longer the denial of psychiatric drug harm and withdrawal injuries goes on
It becomes crystal clear biomedical psychiatry is all about protecting the status quo and avoiding accountability.
If there was any concerns for patients safety and wellbeing seriously addressing the horrific harms would be a priority.
2
9
15
800

Jun 13
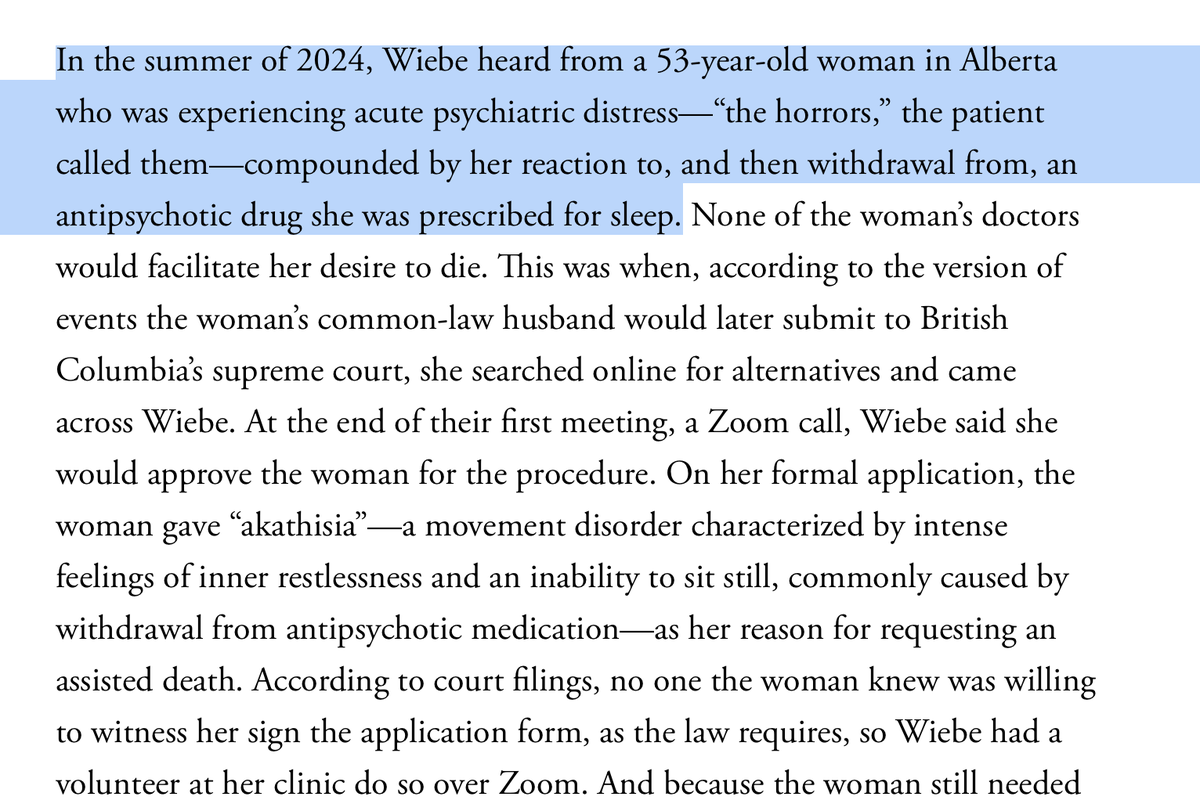
I don’t know if the drugs caused her to kill her children. I know that they *could* have and that should be looked into. I also know it’s not going to be explored responsibly because psychiatry has successfully minimized that their drugs can create horrific outcomes like this.
Jun 11

Postpartum mom Lindsay Clancy killed 3 kids with 'extreme atrocity and cruelty' - using common household item, prosecutors say trib.al/oiaDGIm

14
16
116
13,008
jc retweeted

I'm pleased to share that two abstracts have been accepted for poster presentation at the July 2026 Dysautonomia International Annual Conference in Houston.
• Autonomic-Dominant Symptom Phenotype in Benzodiazepine Withdrawal
• Distributed Autonomic Dysregulation Across Benzodiazepine Withdrawal Phenotypes
Looking forward to sharing these clinical observations and discussing them with patients, clinicians, and researchers at the conference.
3
3
168
jc retweeted

Jun 12
Involuntary commitment is more likely if you're Indigenous, immigrant, lower-income... seeing any trends here? robwipond.substack.com/p/who… My latest at PsychForce.Report
3
13
23
632
jc retweeted

Jo Watson of @dropthedisorder and I have just launched the Critical Counsellor collective:
If you are a counsellor, psychotherapist, clinical psychologist or trainee who questions the increasing medicalising and pathologising of human distress, come join us!
More to follow....
facebook.com/groups/13173204…

4
10
39
1,725
jc retweeted

Jun 12
I've spoken to hundreds of people tapering off SSRIs, benzos, antipsychotics.
Not one of them was warned this could happen when they started.
51
44
342
43,281
jc retweeted

Jun 11
“Social class narcissism linked to anti-psychiatry conspiracy theories.”
This article:
• pathologizes people who think highly of themselves as narcissists
• turns the overmedicaalization debate into a class war
• implies questioning psychiatrists is anti-psychiatry
Let’s not forget that healthy, positive self-esteem protects mental health and that is not a conspiracy theory.

18
9
45
4,155
jc retweeted

Jun 8
What I think about when I see psychiatrists on social media debating semantics and deftly diverting attention, as someone whose life has been profoundly affected by psychiatric drug harm. 🧵 (1/9)

1
14
50
5,555
jc retweeted

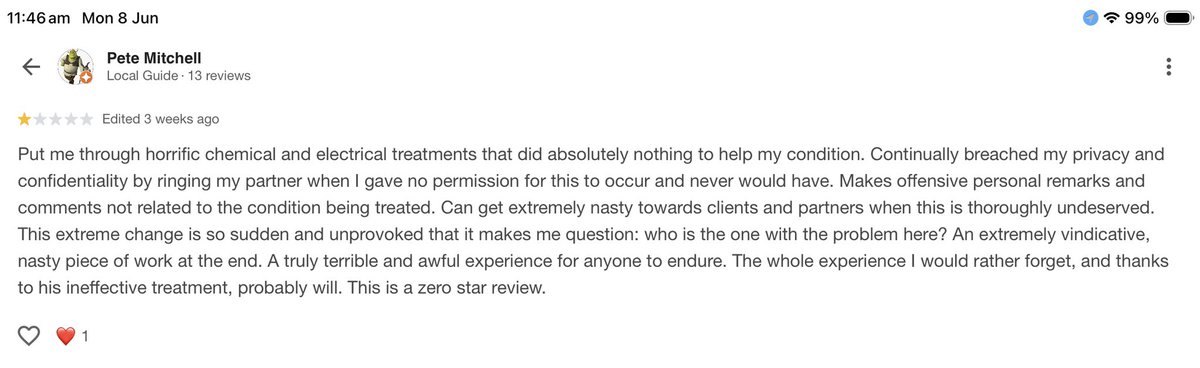
Dr Murray Walters Patient Review. Why doesn’t this surprise me.
1
6
13
576
jc retweeted

Jun 6
My friend had ALS. He joined a trial and was immediately worse after taking the medicine. He told the researchers. They said it could not be from the medicine but that if he didnt want to be in the trial, he could stop.
He stopped. His departure was not mentioned in the trial data.
Another friend worked at Stanford when they were doing trials on Ambien. One elderly woman in the trial kept removing her clothes and was sleepwalking around at night naked.
He was part of the research team, and he told the other researchers that this drug was not safe; if that woman had not been in the sleep lab with him, she could have gotten hurt or in trouble.
They fired him. Not just from the trial, but from Stanford. He was later told that if the trial is not successful, then Stanford won't be asked to do clinical trials and will lose millions of dollars. Another school will get that money instead of Stanford. This is one reason why many universities can't tell the truth. That truth costs them money.
Jun 6

Just received this: this is how vaccine trials are done:
my son had a friend who volunteered for the Emory trials when he was 18 and in high school. Trial would have been ~2019-2020. He became gravely ill after getting vaccinated, thought he was going to die. He contacted the researchers, they told him it could not have been from vaccine, then he was ghosted by the researchers. It’s my understanding he never finished the trials because they stopped communicating with him."
60
684
3,571
162,891
jc retweeted
Jun 5
I wonder when he’ll figure out they’re the same people at different stages of “treatment”?
7
32
109
4,504
jc retweeted
When people hear the mocking, defensive responses of psychiatrists on this platform to patient reports about harm from psychiatric drugs and withdrawal it can be demoralising and lead people to feel hopeless that things will ever change. But I lecture to hundreds of prescribers each month and on the ground people are much more reasonable and less ideological and defensive than the psychiatrists on here. I just leave some responses from last week from GPs in the UK as examples



12
28
108
5,261
jc retweeted
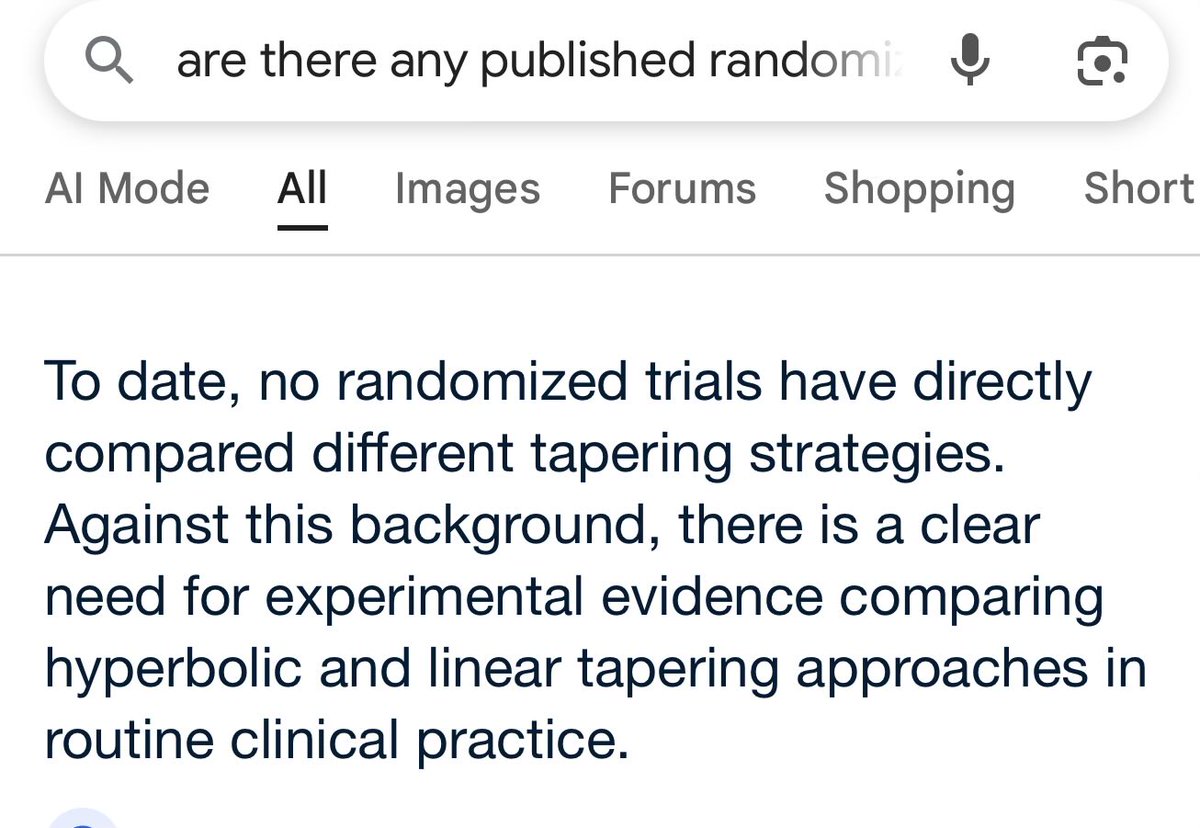
I think there is an odd misconception that hyperbolic tapering means 'everyone needs to spend 3 years tapering off their drugs.' Not true - this is a strawman argument.
Of course some people can taper off with no problem in a few weeks.
Hyperbolic tapering is drawing attention to the shape of the pharmacological road - it is hyperbolic. You can do a hyperbolic taper in 4 weeks (or in 6 months or in 3 years).
A sensible application of the principle is to do a small test dose reduction to see how someone responds. If that is tolerable you could always speed up. If 10% is fine, try 15%, etc.
What is baffling is people who are so virulently against this approach are therefore against the precautionary principle. Who says let's get everyone to jump off buildings and only if they get into trouble will we bother building stairs?
Psychopharmacology boosters on this platform love to paint me as a fiery radical (always amusing to my friends who know what a risk-averse, nervous, four-eyes little geek that I am) : seems somewhat odd when I am advocating for a method of tapering that is slower and more cautious to avoid harm.
It's a bit like driving: if you go too slowly you can always speed up. But if you go too fast and crash (see protracted withdrawal ) it can often be too late to hit the brakes (not always).
So advocating a cautious hyperbolic tapering approach as default is not condemning everybody to years- long tapering, it means taking a cautious approach that can be adapted. Most doctors would do the same for their families (and many have contacted me to get advice to do so).
The risk of a too slow taper (unnecessary exposure to low dose medication) is generally outweighed by the risk of a too quick taper (the possibility of severe and prolonged withdrawal effects which can sometimes be debilitating).
Jun 5

In the absence of RCTs, we should be up front that we don't know what works best for the individual, go with something reasonable for most (hyperbolic for most is a huge mistake that will keep them on the drug for far too long, cold turkey for most is an awful idea that will give far too many unpleasant/disabling side effects), and then adjust from there.
12
11
61
8,596
jc retweeted

Jun 5
I was in the die hard “I can’t live without these” crowd for decades. To go from that to absolutely disabled by them was a turnaround that was very hard for me to accept. But it became impossible to deny over time.
1
4
20
393
jc retweeted
What a dangerous and outrageous statement! Just because your personal experience and 100,000s of others aligns with basic pharmacology and increasing numbers of cohort studies we should not act on that! We need to do what we've always done because to do otherwise would be to admit we have been doing things wrongly for decades. And saving face is more important than helping people avoid harm. Shame on you for suggesting otherwise!
1
6
35
587
jc retweeted
Yes 'science'. Unless there are randomised controlled trials we just need to sit around and do whatever we've done, no matter how many people get hurt. That's how science works. There is no hierarchy of evidence to examine. We should not examine cohort studies that compared different tapering techniques, studies which examine rate of tapering and relapse, and we should ignore fundamental principles of pharmacology, and common sense. I love learning about science!

There is no “tapering science”. It is based on conjecture and clinical experience. No randomized trials comparing methods, without a way to know which patients will respond to what. Just guesswork, which is fine, but it’s not science. I’m glad you found the right help.
13
19
89
10,124
jc retweeted

In my career as a psychologist I am unable to recall any one person whose quality of life improved from prescription psychiatric medications. Yet I am haunted by the consistent stream of clients entering my center whose quality of life & health has been negatively impacted.
20
56
308
10,181