
Pure science on blue sky (chchatham dot bsky dot social). On X, pushback on the redshift
Joined May 2011
- Tweets 3,924
- Following 3,193
- Followers 1,914
- Likes 3,738
26 Photos and videos



Chris Chatham retweeted

Cheers, chills, and a standing ovation when RASolute 302 showed unprecedented survival on daraxonrasib for patients with progressive pancreatic cancer
Seldom do you sense you’re witnessing a historic moment in cancer care but this feels like ras targeting has arrived
#ASCO26
92
1,273
6,504
1,151,888
Chris Chatham retweeted

Though I'm mostly using twitter for cute animal content at this point, for the remaining scientists on this platform, sharing the first work from my lab published @NatureNeuro (rdcu.be/floYr) and a research briefing for a broader audience (nature.com/articles/s41593-0…). 🧵
8
9
42
9,748
Chris Chatham retweeted

May 22
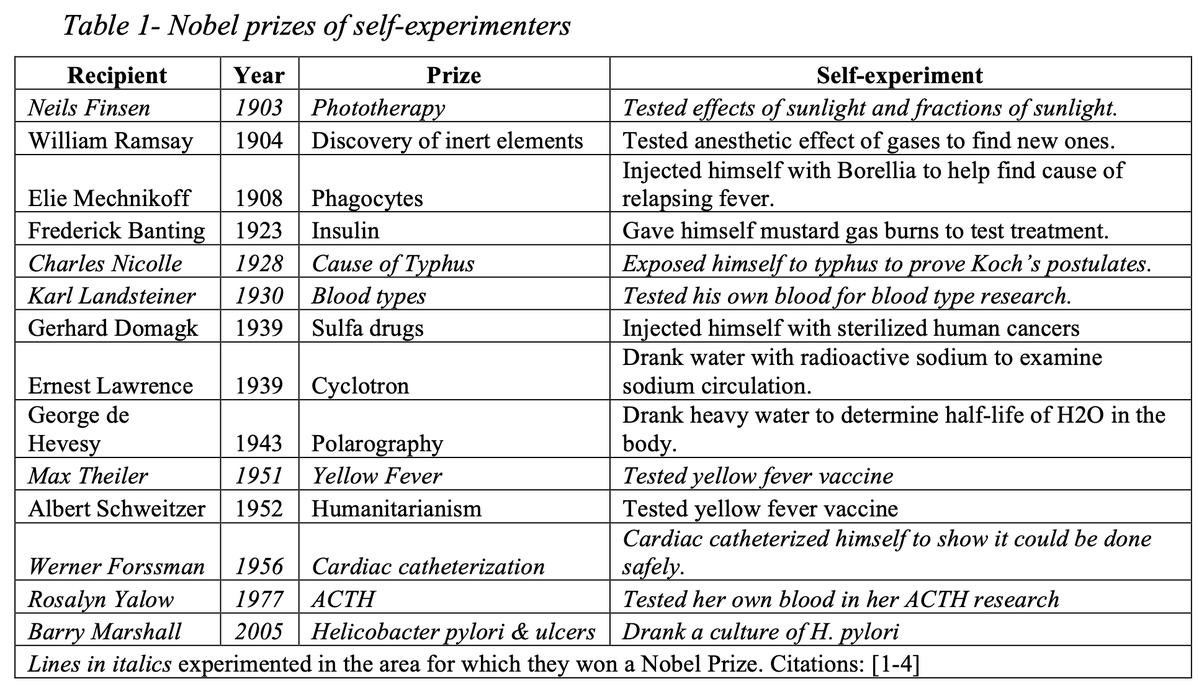
This paper is a goldmine on scientific self-experimentation.
-14 Nobel Prizes have gone to self-experimenters.
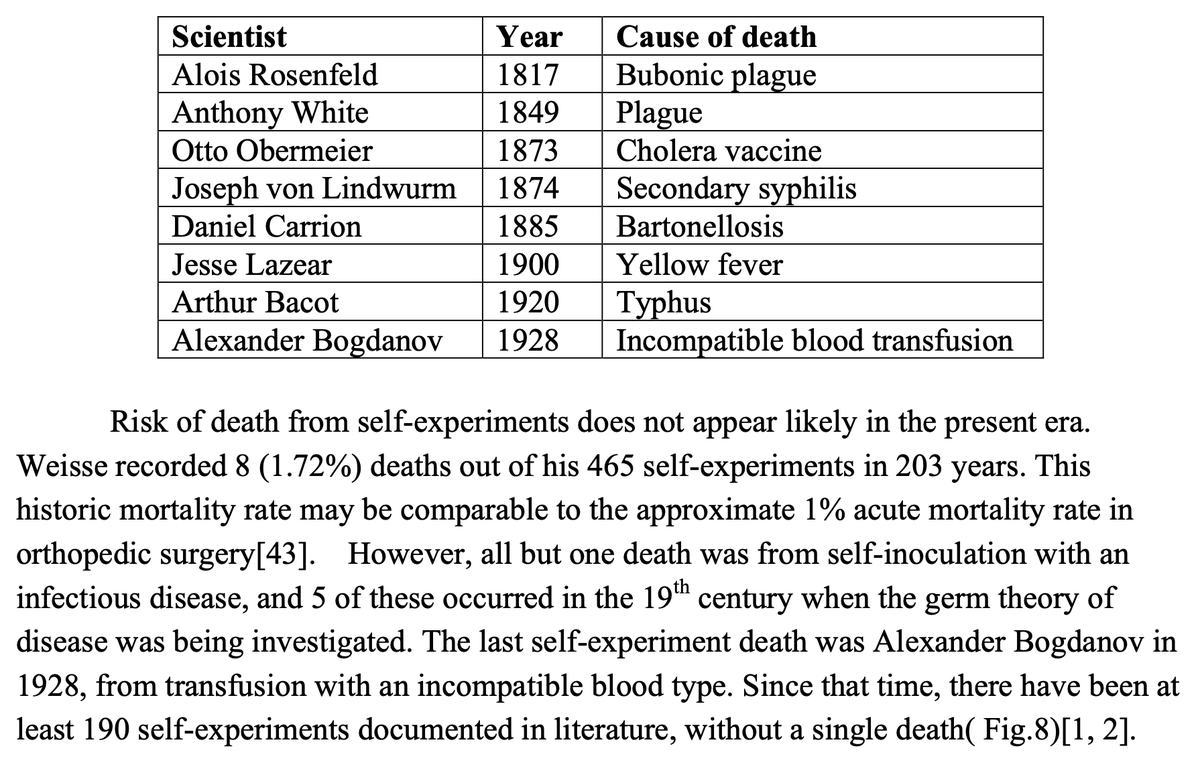
- Of 465 scientific self-experiments documented over a 203-year period, there have been 8 deaths.
- The most recent recorded death from a self-experiment was in 1928, when Alexander Bogdanov injected himself with an incompatible blood type.
- Many universities say that self-experimentation would require IRB approval because it violates "ethical norms for medical research," which is not true; the Nuremberg Principles make an explicit exception for people experimenting on themselves, and the Declaration of Helsinki just says the subject must consent. Also, "there is no law nor regulation identified that requires investigators experimenting on themselves to consult an ethics committee."
- There are lots of recent self-experiments; "In 2014, Philip Kennedy had electrodes implanted into his speech center to further his research on direct brain interfaces. In 2016, Alex Zhavoronkov self tested drugs which his software algorithms identified as likely candidates."

12
108
465
36,261
Chris Chatham retweeted

May 16
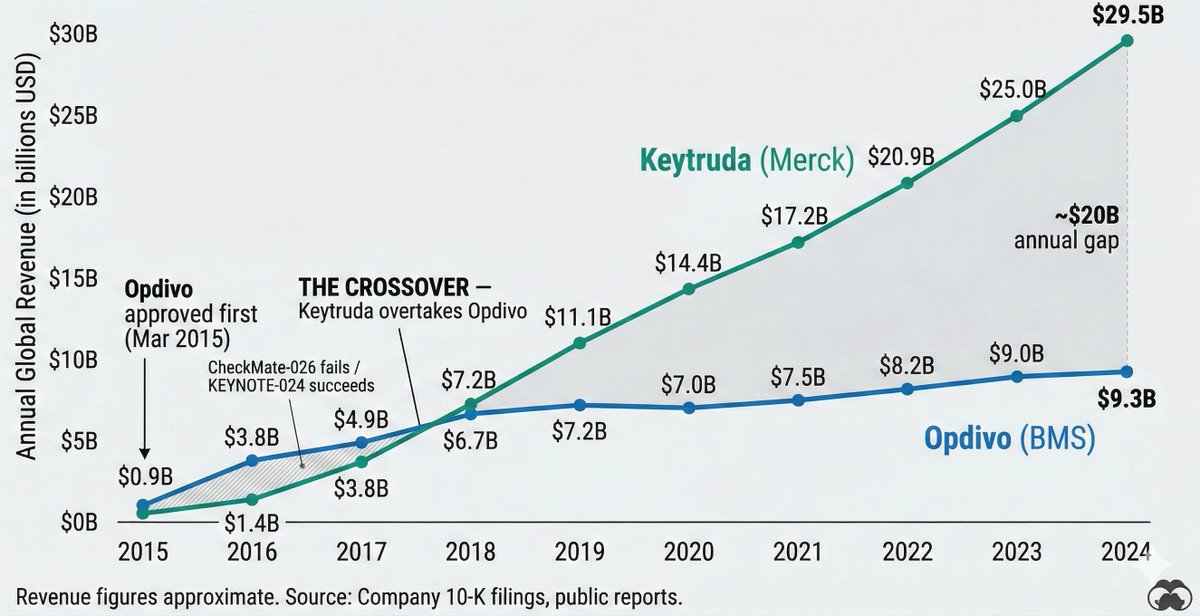
Decisions are everything in biotech, and this is a great experiment to run.
That said, BMS’ decision making around Opdivo is one of the most-written-about case studies on drug development. It is certainly in the training corpus for both models. We need better evals for strategic decision making (something I’ve been thinking about), but hard to do retrospectively without having a training cutoff before an outcome is read out.
May 13

In 2012, two pharma companies faced a defining decision. One chose badly, the other well. If AI can make better decisions than humans, then given the same information it should make the correct choice
But it didn't
Ingenious experiment by @liangc_science via @adamjkucharski
liangchang.substack.com/p/ca…
3
6
72
19,755
Chris Chatham retweeted

May 15
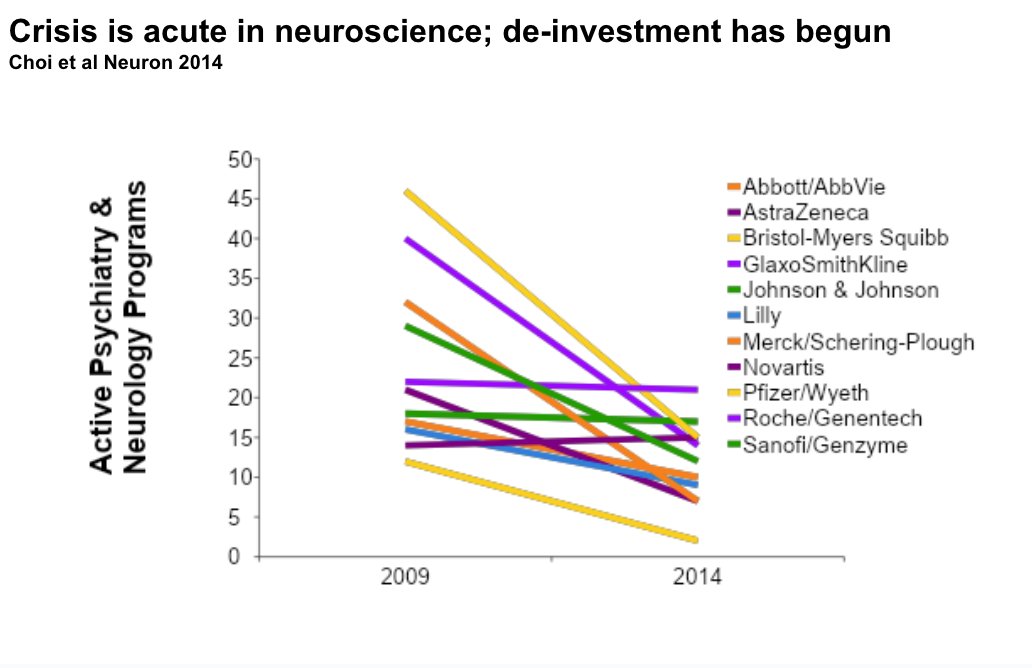
The entire NIH annual budget for neuroscience research - for all scientists across the entire US - is about $3bn a year. And now there are something like a dozen "neolabs" that have all raised O($1bn) within months of being founded, and they are all doing the same thing.

Sources: xAI co-founder Igor Babuschkin plans to raise up to $1B at an up to $5B valuation for a new AI research startup, with General Catalyst possibly leading (Forbes)
(Visit Techmeme dot com for the link and full context!)
13
28
283
78,578
Chris Chatham retweeted

Out today! A truly team effort and one of my favorite lab projects
The data connect NMDA/Grin2A malfunction to dopamine dynamics and related behaviors, and provide a futuristic model to develop and test "course altering" treatments for schizophrenia
nature.com/articles/s41380-0…
2
22
78
6,557
Chris Chatham retweeted

May 11
Yes. This is an essential point, the mangling of which has badly distorted our collective cultural understanding, and it's great to see it in the New York Times.
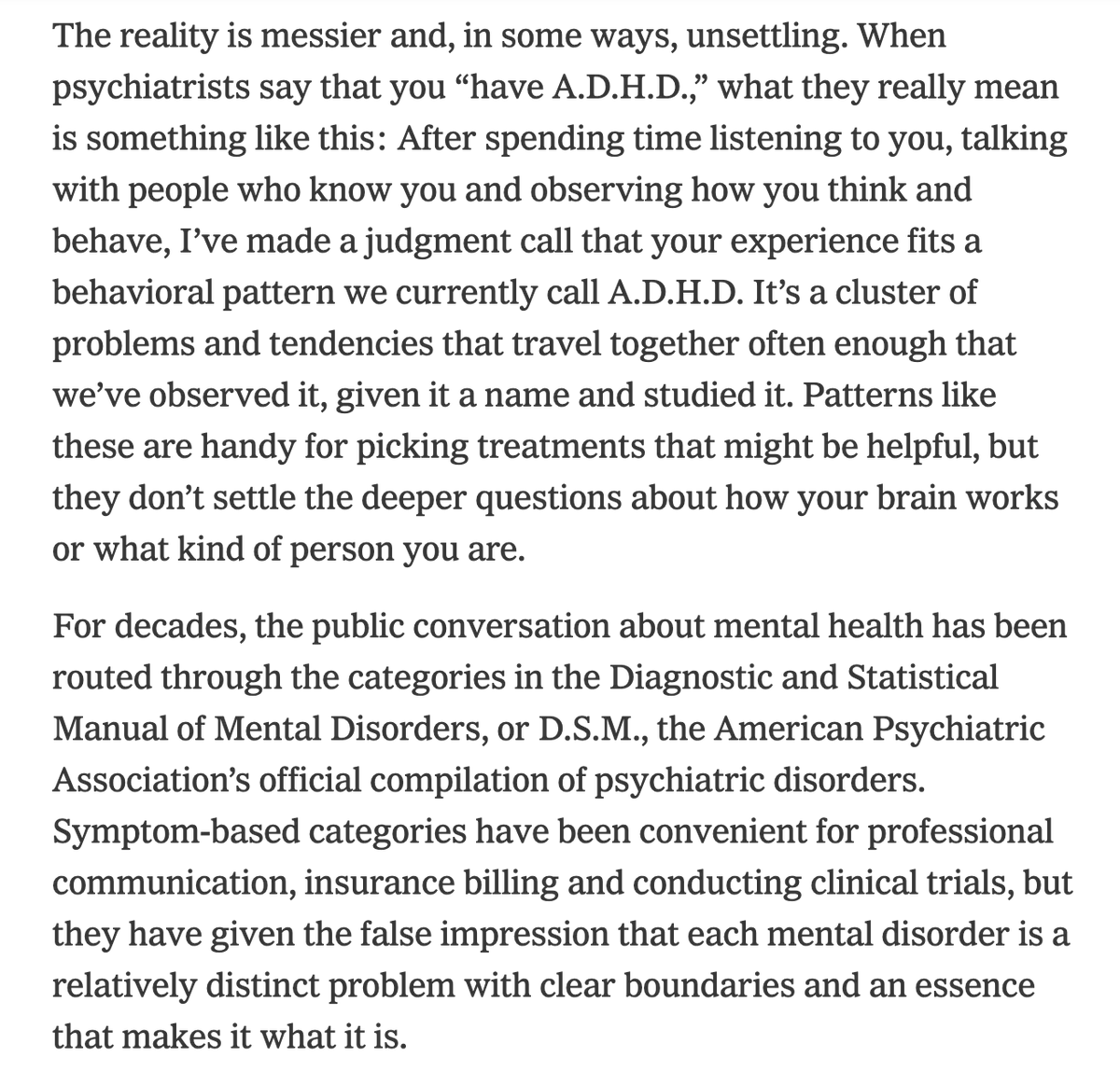

Really nice article about psychiatric diagnosis from today’s New York Times, by Awais Aftab, M.D. @awaisaftab
nytimes.com/2026/05/11/opini…
What's your "real" diagnosis? There isn't one.
13
121
1,434
80,497
Chris Chatham retweeted

Congratulations to Dr. Lindsey Power for leading this important review and practical guide to publication 🎯👇.

New paper in Imaging Neuroscience by Lindsey Power, Sylvain Baillet, et al:
A neuroscientist’s guide to neural burst detection
doi.org/10.1162/IMAG.a.1226

3
18
2,199
Chris Chatham retweeted

Apr 29
I’m excited to share this work from an amazing team @StanfordBrain: @mystrypercy who co-led the study, Zhiyao Gao, Weidong Cai, and Vinod Menon.
nature.com/articles/s41467-0… [2/12]
1
5
32
2,312
Chris Chatham retweeted

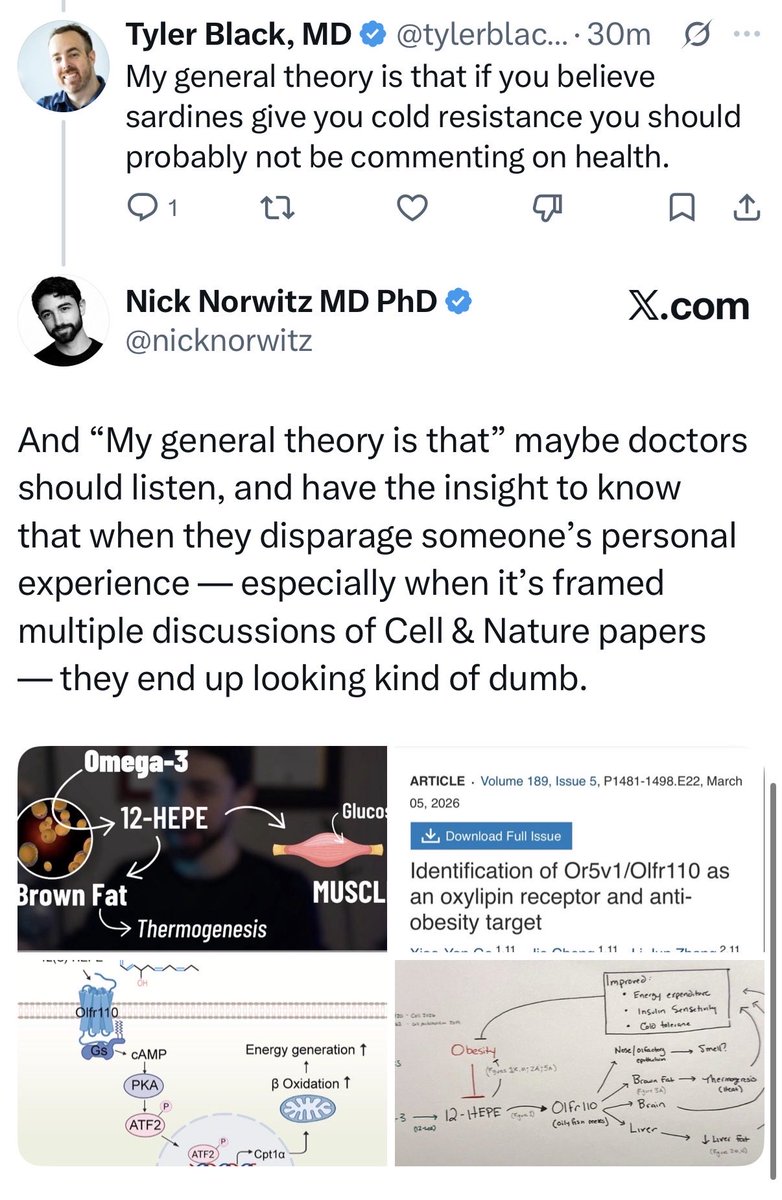
Apr 26
There's a recurring move in wellness discourse: find a real mechanistic paper, collapse the distance between "this pathway exists" and "therefore my month of sardines did the thing I felt," and treat anyone pointing at the gap as anti-science. The gap is the entire discipline.

5
4
60
5,159
Chris Chatham retweeted

“It’s not important how the gunman had the opportunity to transport, store, and use a firearm in an attempted assassination of the POTUS, it’s more important we find ways to blame liberals and justify construction contracts for a building no American voted for or wants.”
6
120
768
23,910
Chris Chatham retweeted

This is the right question. It’s not free. It’s actually R&D funded by a public relations budget funded my other profitable drugs. That’s a luxury available only to profitable companies.

$REGN wins FDA approval for its gene therapy to treat a very rare genetic form of hearing loss. The company is giving away the therapy for free.
OTOF-related hearing loss affects approx. 50 newborns per year, so really rare, but... are there any concerns from other gene therapy makers about a precedent being set whereby an otherwise expensive treatment is given away for free?
3
4
93
20,757
Chris Chatham retweeted

Apr 23
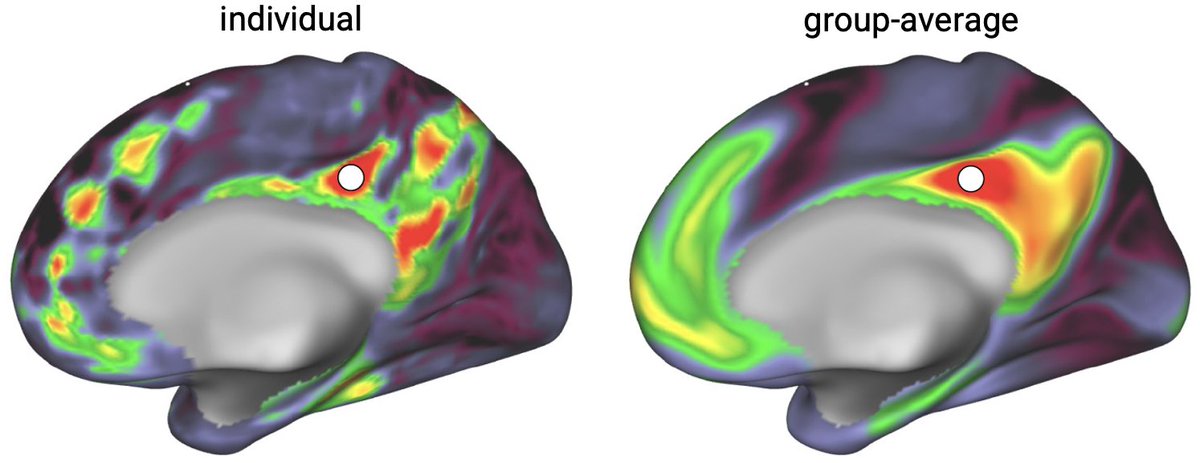
Function & cytoarchitecture don't overlap ... they're orthogonal. Prefrontal cortex is tiled with chains of functional patches mostly known from face processing. Multi-modal parcellations are wrong ... & other insights hidden by group-averaging fMRI data: bsky.app/profile/gordonneuro…
2
35
105
13,111
Chris Chatham retweeted

Apr 24
A monumental moment in medical history: the first gene therapy for genetic hearing loss is now FDA approved. As a former Regeneron scientist, I feel very proud. I had the opportunity to hear about this programme while it was still in development. It’s one of the few programmes that, every time you came across it, you felt the medical breakthrough in your bones and privileged just to be there while it was happening.
At this moment, it’s important that we look 30 years back when researchers mapped a locus on chromosome 2 to congenital deafness in a Lebanese family (pubmed.ncbi.nlm.nih.gov/8789…). They named it DFNB6 (later DFNB9) with no clue about the responsible gene. Three years later, the causal gene came to light: OTOF, encoding a protein called otoferlin (nature.com/articles/ng0499_3…). Seven years after that, in 2006, pioneering work by Christine Petit revealed that otoferlin is a calcium sensor in the inner hair cell membrane, acting as a molecular trigger that converts sound into electric signals that the brain can read (pubmed.ncbi.nlm.nih.gov/1705…). Twenty years fast forward, we now have a successful treatment. Thirty years from discovery to medicine.
OTOF-related deafness is congenital, caused by complete deficiency of otoferlin. In these children, the cochlea is structurally intact, hair cells are there, the mechanics of sound transmission work. It’s just that final step, where hair cells hand off the signal to the auditory nerve through neurotransmitter release, that doesn’t happen. Sound arrives and dies at the synapse. It’s deafness due to a defect in the synapse caused by the absence of a single protein, which is what made this a beautiful, clean target for gene therapy.
The treatment itself is a feat of molecular engineering. OTOF is too large to fit in a single AAV capsid. The team solved this elegantly by delivering the gene in two halves separately, which then get spliced to produce the full functional protein. A single surgical injection into the cochlea, a molecular miracle unfolds. Results from the CHORD trial were striking: of 20 evaluable patients, including children as young as 10 months, 80% showed meaningful hearing improvement, and by 48 weeks, 42% had achieved normal hearing including the ability to hear whispers. Otarmeni is not only the first gene therapy for deafness, it’s also the first dual-AAV therapy to be approved by the FDA.
There are very few things in medicine that come close to giving back a sense like vision, hearing, or touch that a human never had from birth. It’s almost God’s work. A parent witnessing their child who was born deaf hearing their voice for the first time, it’s a joy that no words can describe. Multiply that by the fact that it came from a single injection, a repaired gene, and 30 years of science. We are truly in the golden era of medicine.
Regeneron press release:
investor.regeneron.com/news-…
Below video is from the NEJM publication of CHORD trial (Valayannopoulos et al. NEJM 2025)
nejm.org/doi/full/10.1056/NE…
9
75
263
59,407

Both @NatureMedicine editorials dance around the name. So here it is. Epic.
@HeyEpic's sepsis AI runs in 180 US hospitals. Outside researchers finally tested it. It missed two in three cases. Most alerts fired after doctors had already called sepsis. Still deployed. Nobody had to pull it.
What made that legal is boring and important. The @US_FDA approves medical AI the way it approves a catheter, by showing it resembles an existing product. Drugs have to prove patients do better. Algorithms skipped that step.
Ambient-scribing LLMs walk through the same door next year. Every clinic visit. 10x the scale.
The editorials ask for more studies. The rules never required any.
Apr 22

On the lack of compelling evidence that medical AI is improving patient care, and what to do about it, a @NatureMedicine editorial nature.com/articles/s41591-0…

4
12
46
8,626
Chris Chatham retweeted

The proposed FY2027 budget includes a $5.8B (−12.3%) cut to the NIH. United for Medical Research calculated this could cost ~50,000 jobs and $11.6B in economic activity, with 26 states losing >$100M each. A tragedy for science, patients, and the economy. #NIH
5
65
169
26,740
Chris Chatham retweeted

Apr 22
Absolutely shocking that freezing NIH funds and causing a collapse of trust between universities and NIH, killing active grants and generally creating an environment of chaos and uncertainty resulted in a breakdown of medical and scientific research. 😮
Apr 21

“China is now eating our lunch.”
RFK Jr. warns the U.S. is losing its edge to China in medical research and drug development.
“They got more drugs approved last year.”
“They went from running 3% of clinical trials to running 30%.”
“We are losing scientists, we’re losing our IPs, we’re losing the best researchers.”
“We’re going to lose our biosecurity.”
“We are fast-tracking approvals now in our country at record levels.”
4
46
238
26,907

Apr 23
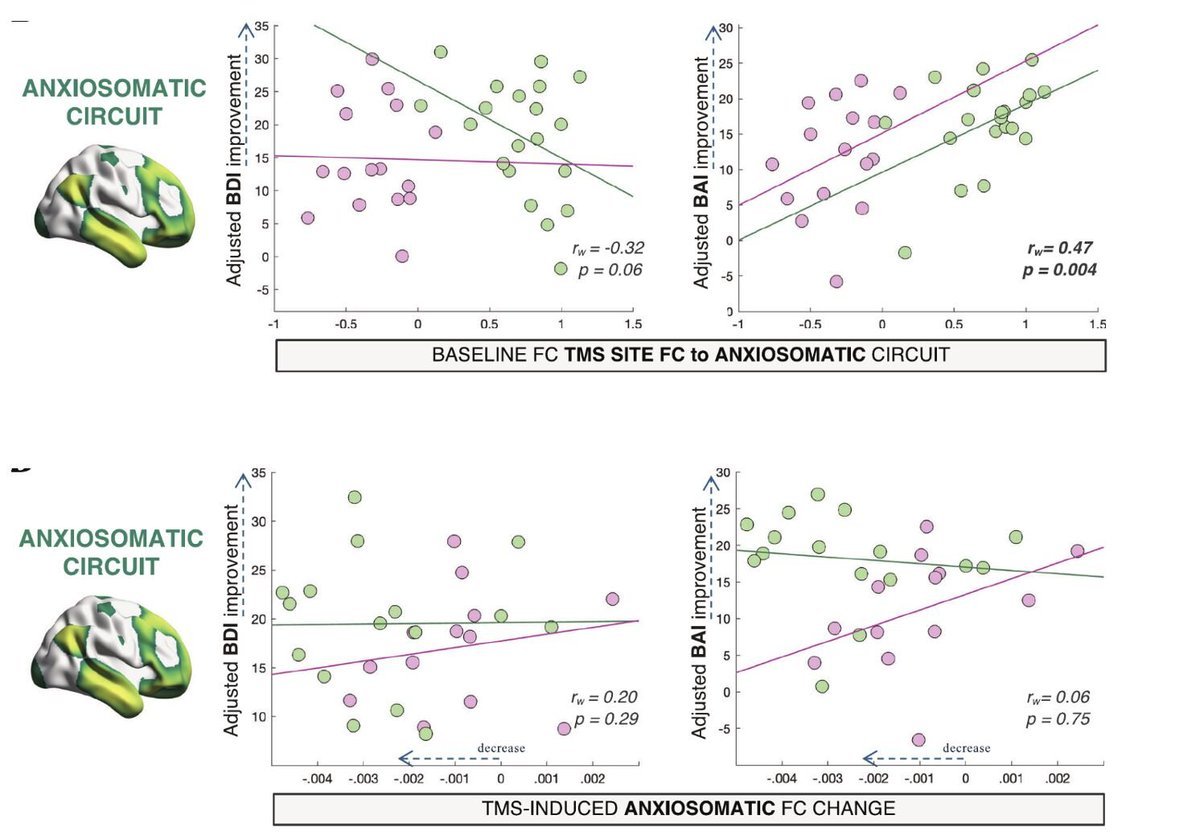
Important work. Also, an opportunity to pedantically note the widespread misuse of “target engagement” to refer to effects that might equally well reflect *off*-target engagement!
Most markers advertised as TE are mislabeled (proximal / distal) (pharmaco)dynamic markers…

We often treat functional connectivity as if it’s an established measure of TMS target engagement. I’m not so sure.
Check out our new paper by Samantha Baldi in @npp_journal on rsfMRI data from a head-to-head TMS trial.
free: rdcu.be/feIya
full: lnkd.in/eSdthbSg
1
269
Chris Chatham retweeted

Apr 21
There are ways to do so, for example through discovery of better biomarkers that could shorten trials or make them more efficient. But most efforts aren't focused on clinical utility in this targeted way, unfortunately. And we still need regulatory reform.
Apr 21

so AI drug discovery sounds great but how's AI going to make clinical trials faster? i'm sure there's a podcast I could listen to about this but can someone just tell me
8
6
52
6,465
Chris Chatham retweeted

Apr 20
Tired of the paperwork to get access to human genomic data from #dbGAP and many other consortia (e.g., #NeMO, #PsychENCODE, #Simons, etc)? I certainly am!
I have a proposal - why we cannot learn from open source licenses and come up with several standard versions of patient consent for research use of data. Labs generating data will work with patients to SELECT proper versions. Then @NIH can establish a process to approve which institutes/PIs have the “certificates” to access ALL data with particular levels of consent.
I guess that will help us avoid months of paperwork to get access to individual datasets?
#HumanGenomicDataSharing
#PatientConsent
#Privacy
2
6
36
4,523