
Urologic oncology & epi, focus on #prostatecancer @UCSFcancer @UCSFurology. GU Chief @SFVAMC. All views strictly personal. RT≠E. #🟦
Joined September 2010
- Tweets 11,534
- Following 1,913
- Followers 11,337
- Likes 11,107
1,220 Photos and videos







Pinned Tweet

May 1
Could not be more proud of Jake with his first 3 original songs now streaming! Give him a listen.
Here he is on Spotify:
open.spotify.com/artist/35y9…
and Apple:
music.apple.com/us/artist/ja…
Or Insta, YouTube, and everything else here: jakecoopmusic.com

4
4
23
2,423
Matt Cooperberg retweeted

by Jonathan Fisher, MD, FACC
I am a Jewish physician, and I have never written about that here. I am going to, because of a surgeon I have never met. Emmanuel Moss, chief of cardiac surgery at Montreal’s Jewish General Hospital, is leaving for Atlanta in September.He is one of the few surgeons in Canada routinely performing robotic mitral valve and coronary bypass procedures. People close to him say the deciding factor was not Quebec’s strained healthcare system, which had been strained for years, but a growing sense that he was no longer safe in the city as a Jew.
The hospital he is leaving opened in 1934 with the first official non-discrimination policy of any hospital in Canada. It was founded in response to an era when many Jewish physicians faced discrimination in medical training and hospital appointments. The historical echo is difficult to miss.
When a clinician leaves because of who they are, a health system does not lose a statistic. It loses a specific person who held specific knowledge, relationships, judgment, and expertise developed over decades.
A 2024 survey of Canadian Jewish physicians found that reported antisemitism in hospitals rose from near zero before October 2023 to 39 percent after, and that nearly a third of respondents were considering leaving the country. The association’s chair warned that the consequences could include the loss of hundreds of physicians at a time when the healthcare system can least afford it. That mechanism is not unique to Jews. It is what happens whenever people feel unsafe because of their identity. Experts leave. Communities become poorer in ways that are difficult to measure. Eventually, patients and their families pay the price.
I am writing this as a Jewish physician because this story landed personally. I am writing it as a physician leader because I have spent decades thinking about what allows caring people to do their best work, and what it costs when they cannot. When any clinician feels unsafe because of who they are, something is lost long before they decide to leave.This time, the story touched my own community. That does not make it less relevant to anyone else. It does make it harder for me to stay silent.

89
335
1,379
35,669
Matt Cooperberg retweeted

Even Arab leaders admit it.
Everyone is sharing the Bill Clinton clip where he describes how Yasser Arafat rejected a generous peace offer at Camp David that would have given the Palestinians a state on 96 percent of the West Bank, land swaps, and a capital in East Jerusalem. Clinton says Arafat lied to him and that the Palestinian leadership never actually wanted a two-state solution. They wanted to destroy Israel. It’s a video often shared by people like @VividProwess, and it’s an important one for people to see.
Of course, critics immediately dismiss it. They claim Clinton is biased or he’s pro-Israel. They’ll tell you that you cannot trust the American perspective.
Ok, so let us set that aside.
Now watch this.
In this powerful interview, former Egyptian President Hosni Mubarak, a major Arab leader who was directly involved in negotiations, says exactly the same thing from the Arab side. He talks about the Mena House Conference in Cairo as well as the Camp David negotiations of 1978. All failed because of the Palestinians repeatedly rejecting any offer. The Oslo accords were signed but because Hamas and the Palestinian Islamic Jihad were not involved, they derailed the accords and any chance for peace by initiating 4 years of terrorist suicide attacks in Israel. Then came the second Camp David negotiations in 2000 which Arafat agreed to, then rejected and instead initiated the Second Intifada.
Mubarak explains how the Palestinians refused to even participate in the Mena House conference of 1977. He describes repeated opportunities they were given, including a detailed document that called for Israeli withdrawal from the Samaria, Judea and Gaza, security arrangements during a transitional period, and other major concessions. The Israelis were willing to negotiate on difficult issues like who would control security. The Palestinians, according to Mubarak, kept saying no and wasting chance after chance.
He speaks with clear frustration about how for decades the Palestinian side has rejected peace initiatives and realistic compromises.
The video further shows footage from the PLO representative in 1977, as well as old footage of Egyptian president Sadat who was involved in the Mena House and first Camp David negotiations of 1978.
This perhaps is far more impactful than Clinton’s account because it is not a Western or Israeli voice. It is prominent Arab leaders who lived the negotiations, who represented the broader Arab world, and who had zero incentive to defend Israel.
When leaders from both sides of the table describe the same pattern of Palestinian rejectionism and violence, it becomes much harder to dismiss as bias.
The pattern is clear across decades and across different voices… generous offers, repeated refusals, and continued demands for everything while giving nothing in return.
This is not ancient history. It is the core reason the conflict continues today.
If you value the truth, please share.
278
6,455
14,606
545,021
Matt Cooperberg retweeted

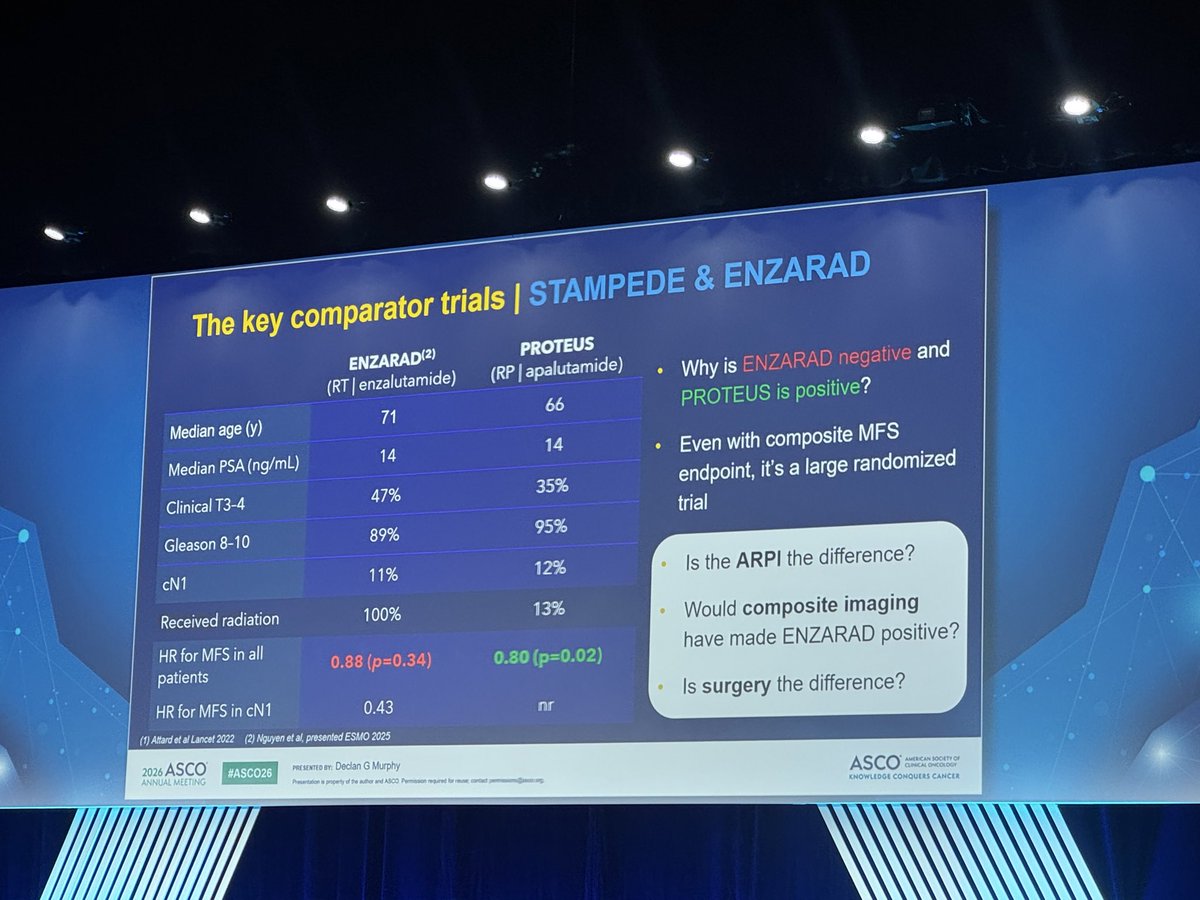
ICYMI - PROTEUS Discussion at #ASCO26. A new journey for high risk prostate cancer patients. Perioperative hormone therapy, space exploration, what is progress, and a bit of Greek mythology throw in @adamkibel_uro youtu.be/7n7PFmpAlVY?si=FeG7…
1
20
47
6,381
Jun 7
WTF
Scientists ejected from diabetes conference for distributing journal reprints - Ars Technica apple.news/AnLaRevwJTWea-llg…
2
1
7
2,718
Matt Cooperberg retweeted

Jun 3
First ever locally injectable immunoactive agent with proven DFS benefit in localized prostate cancer.
Tandem randomized Phase II in surveillance forthcoming.
Origin: Baylor basic science lab (support research!)
thelancet.com/journals/lanon…
1
15
49
5,392
Matt Cooperberg retweeted

A reminder:
People are alive today because somebody funded science.
And while RFK Jr. continues questioning public health institutions, reality remains stubborn: medical research, public health programs, and scientific investment have saved millions of lives. You do not get breakthroughs by ignoring expertise or treating evidence like a political inconvenience.
This week, researchers announced promising results for a novel pancreatic cancer therapy that may dramatically improve survival for one of the deadliest cancers we know. These breakthroughs do not happen accidentally.
They happen because somebody invested in science long before the breakthrough happened. Science is not optional. People’s lives depend on it.
3
49
168
3,533
Matt Cooperberg retweeted

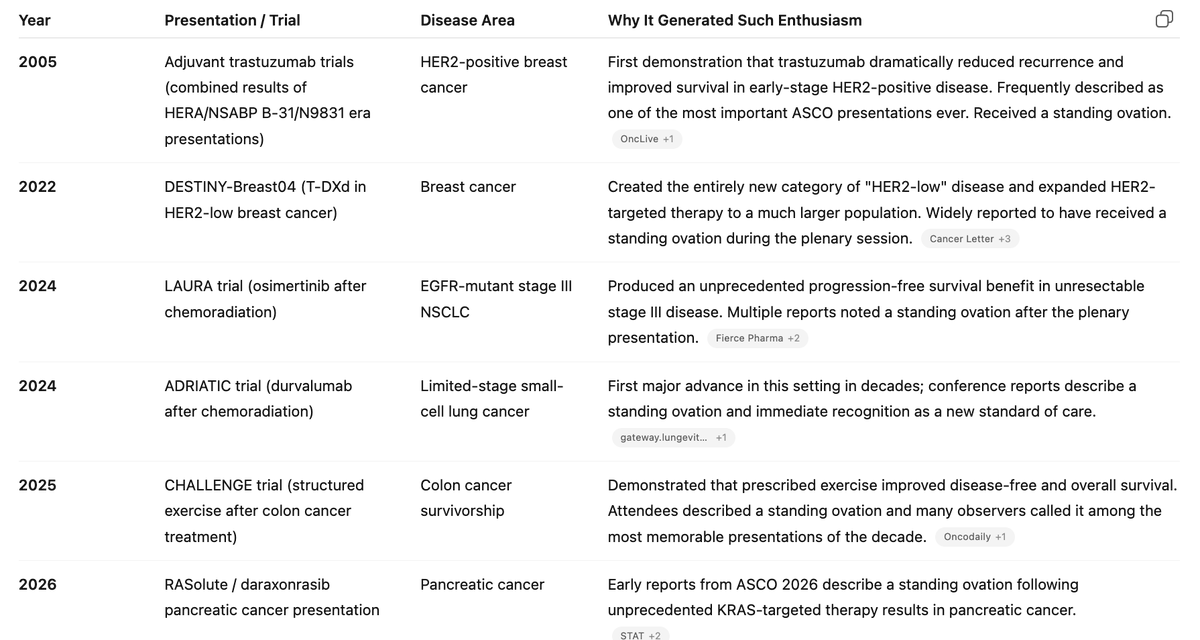
For @ASCO aficionados, there have been questions as to how many standing ovations we have seen. The first I saw was adjuvant Herceptin in 2005. ChatGPT generated the list below for me when prompted for ASCO presentations with standing ovations.

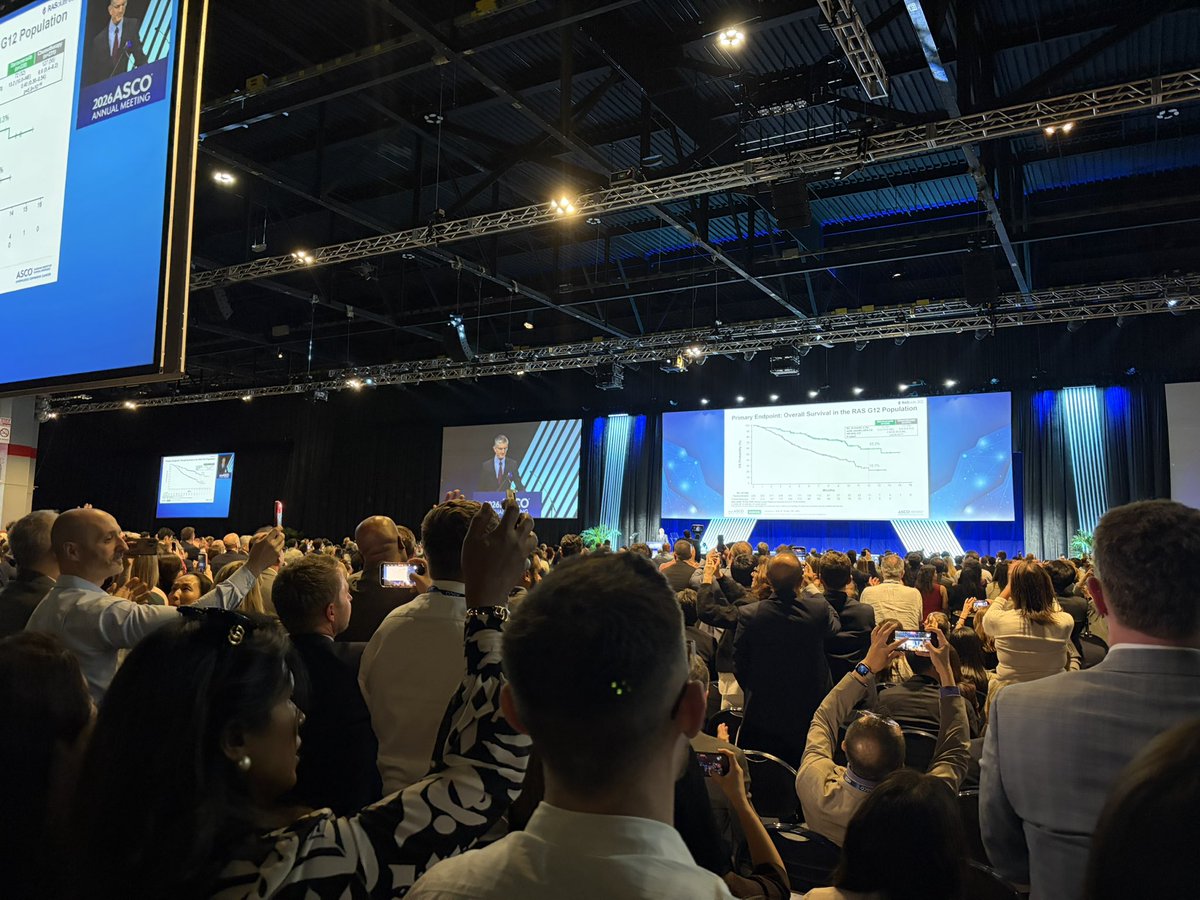
Incredible #ASCO26 moment.
Dr. Brian Wolpin, presenter of the daraxonrasib study, received a standing ovation DURING his talk after he stated the survival benefit for PDAC patients. It was sustained. Cheering. I have never see anything like it in the middle of a talk. $RVMD
7
40
151
25,812
Matt Cooperberg retweeted

May 31
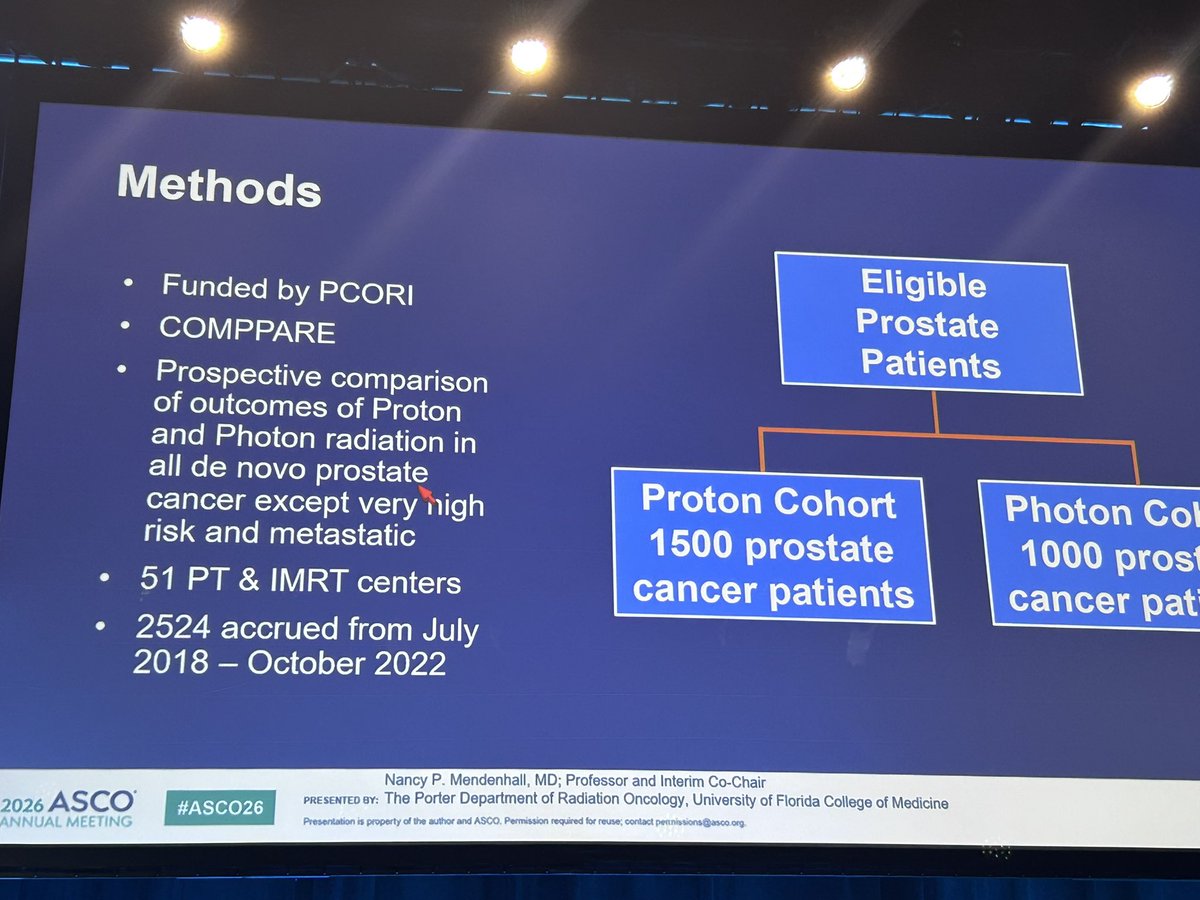
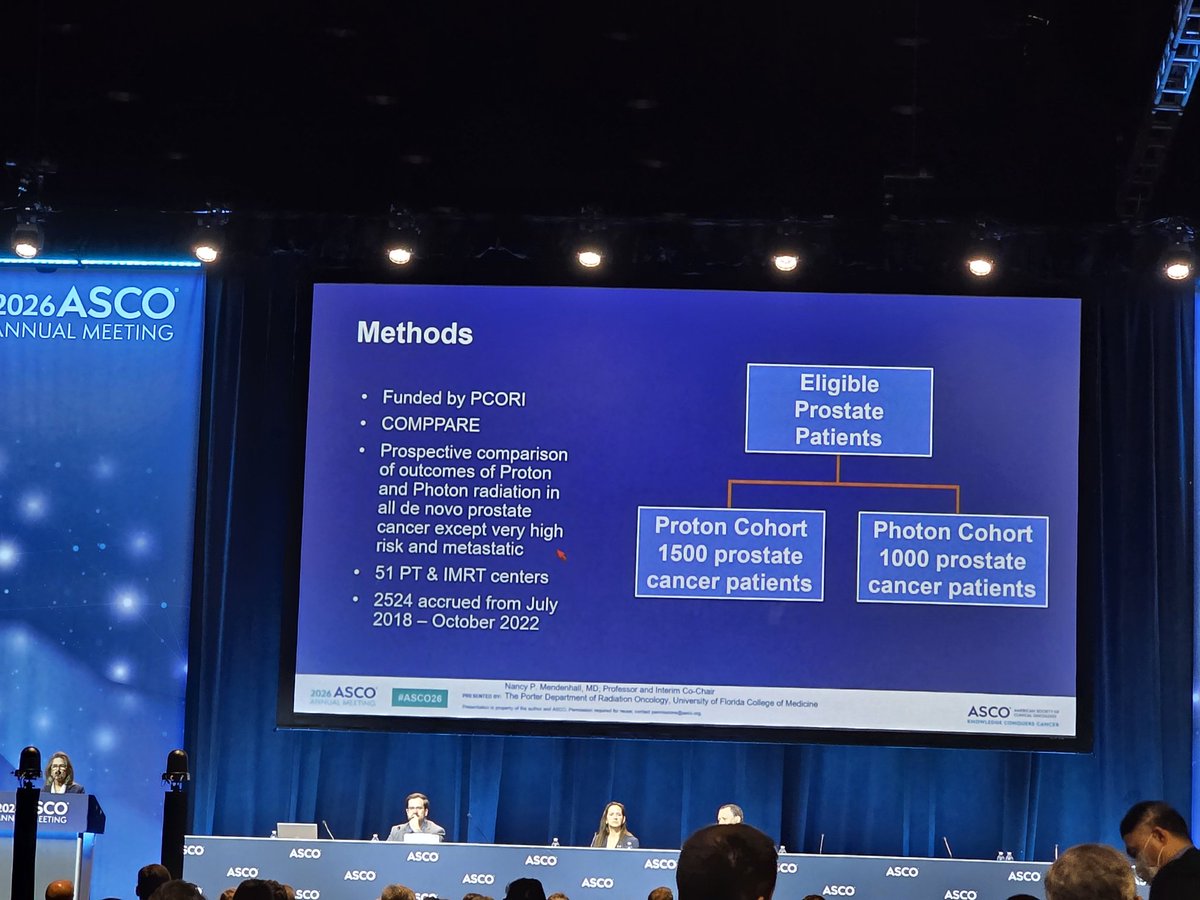
Now we have PARTIQoL and COMPPARE….message is quite clear as to if there is any benefit of protons for localized prostate cancer.
@DrSpratticus @seanmmcbride @TylerSbrt
May 31

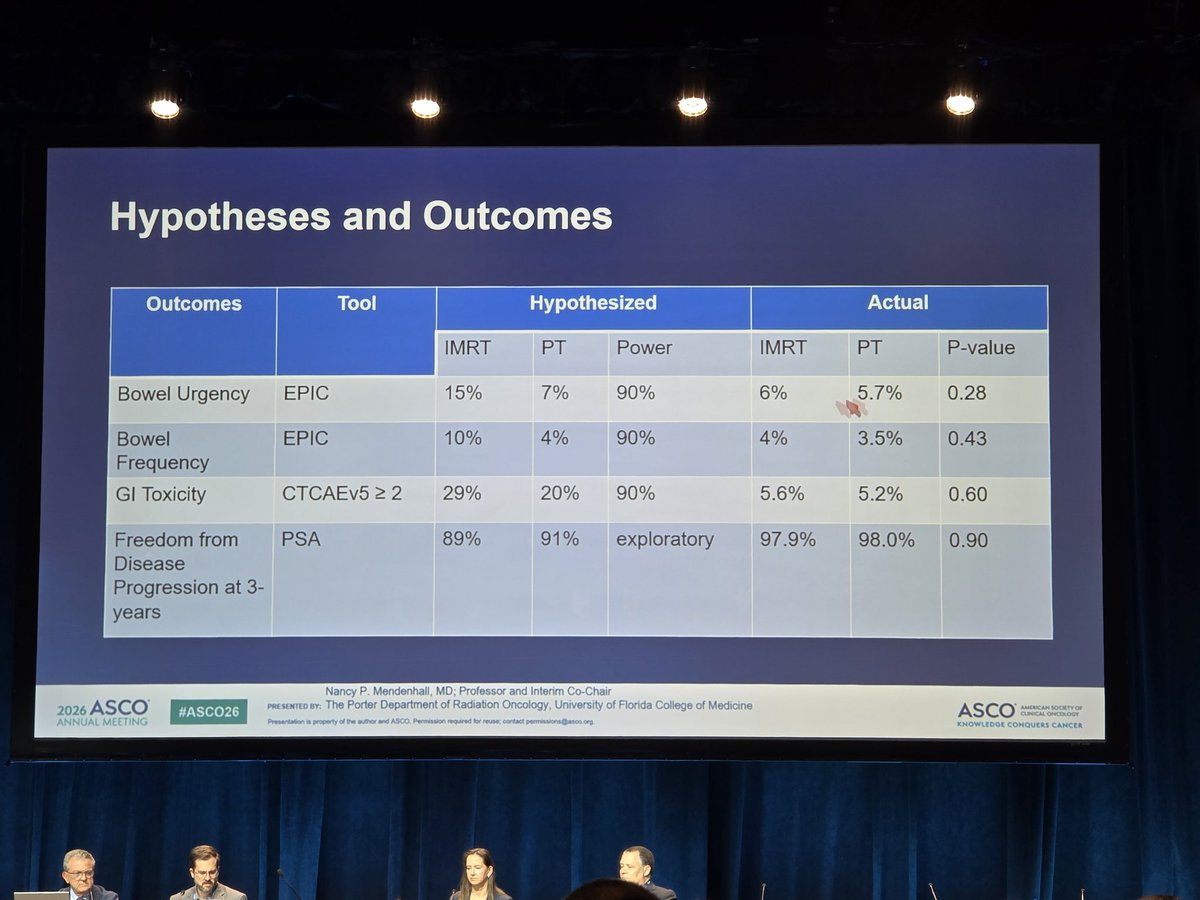
Kicking off the GU Rapid Oral Session at #ASCO26, #NancyMendenhall presents early results from COMPPARE, showing comparable bowel outcomes, grade ≥2 GI toxicity (5.2% vs 5.6%), and 3-year FFBP (98.0% vs 97.9%) in LPC. #ASCO26 #ProstateCancer @ASCO @OncoAlert

3
12
26
10,688
Jun 2
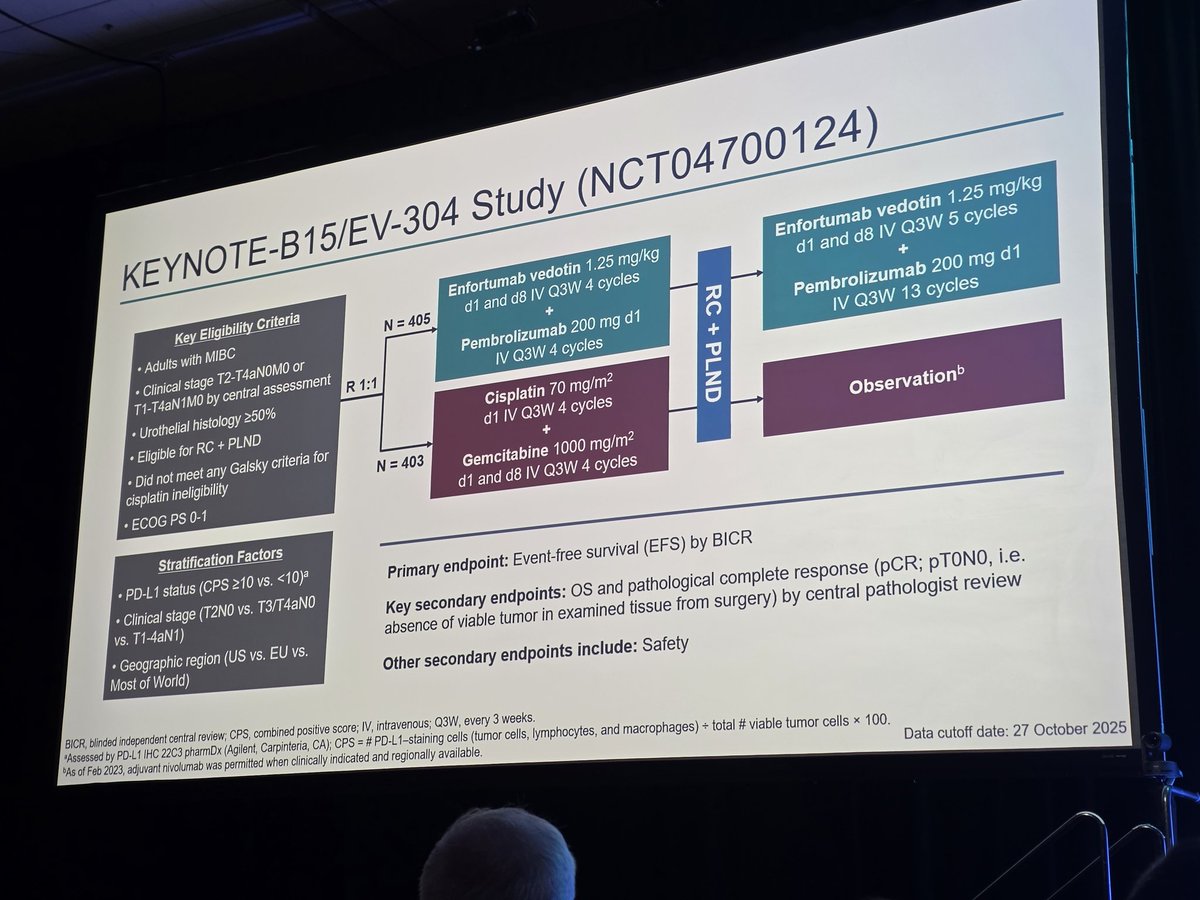
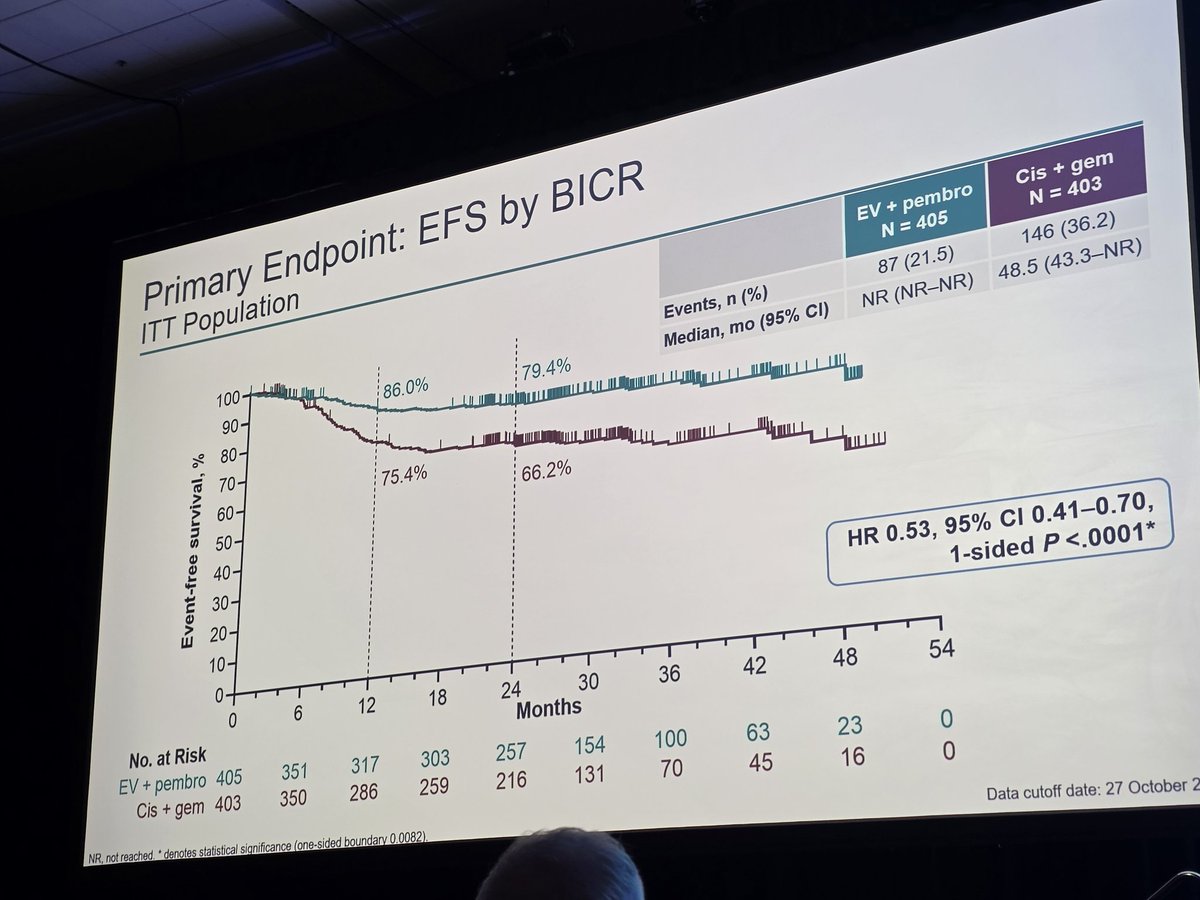
And just like that, an era ended. Neoadj chemo before cystectomy is now a historical footnote #ev304 #keynoteb15 #ASCO26
Feb 27

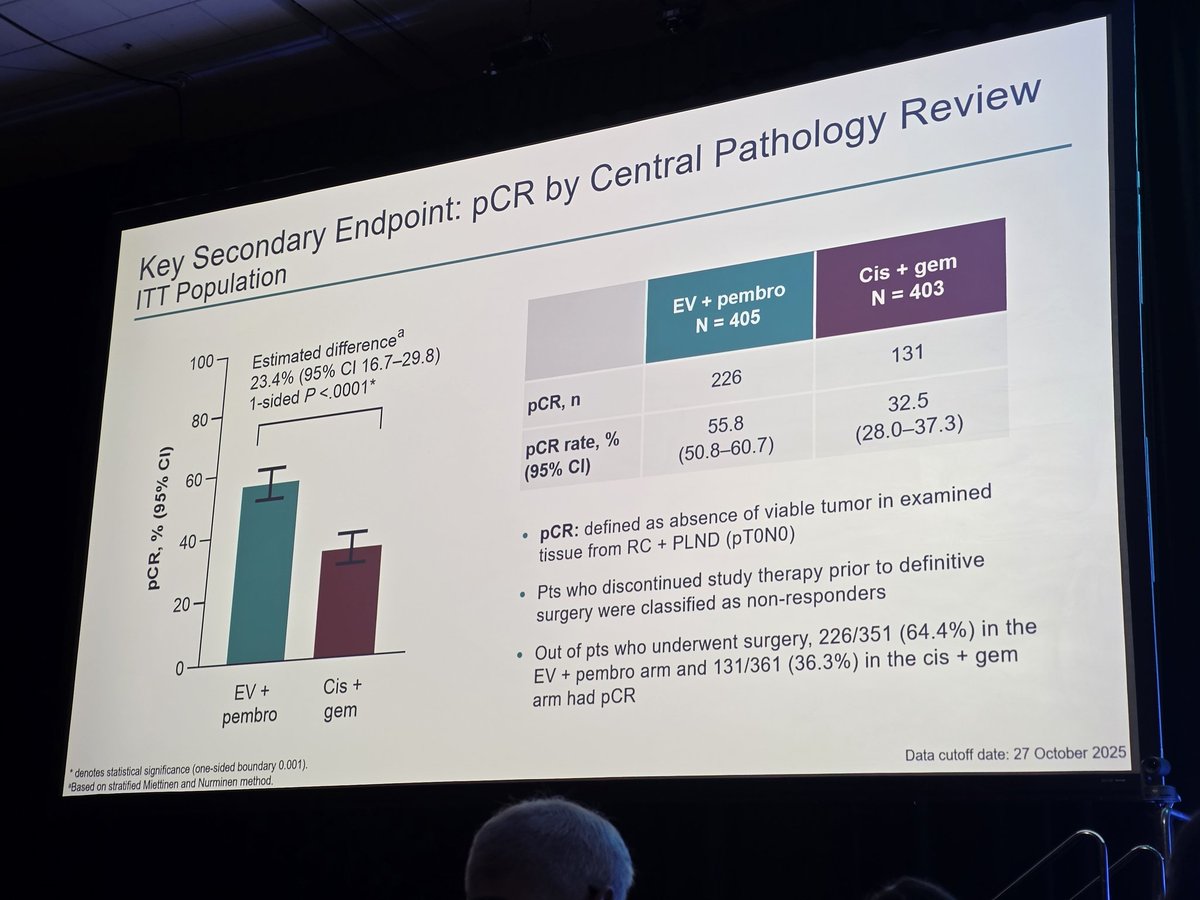
PRACTICE CHANGING: #KEYNOTEB15/EV304- in #MIBC, periop EV/P led to sig EFS (NR v 48.5m, 24m EFS 79.4 v 66.2%, HR0.53; 0.41-0.7), OS (NR v NR, 24m estimated OS 86.9 v 81.3%, HR 0.65; 0.48-0.89), pCR (55.8 v 32.5%) benefit v. neoadj gem/cis, supporting EV/P as SOC in this setting

3
6
33
10,187
Matt Cooperberg retweeted

May 15
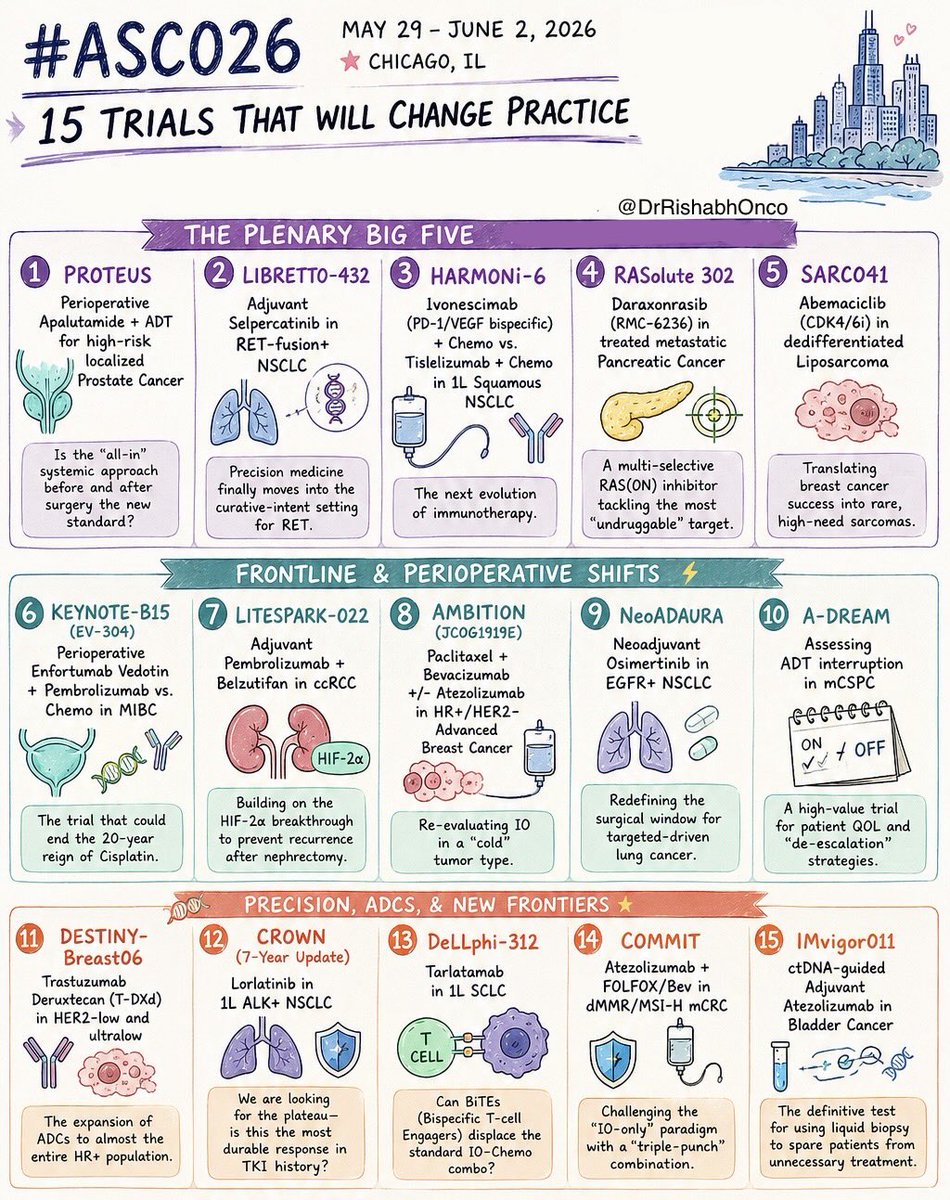
🚨 THE 15 MOST IMPORTANT TRIALS OF #ASCO26
May 29 - June 2 | Chicago
Which trial are you watching most closely?
🌟 PLENARY GAME-CHANGERS
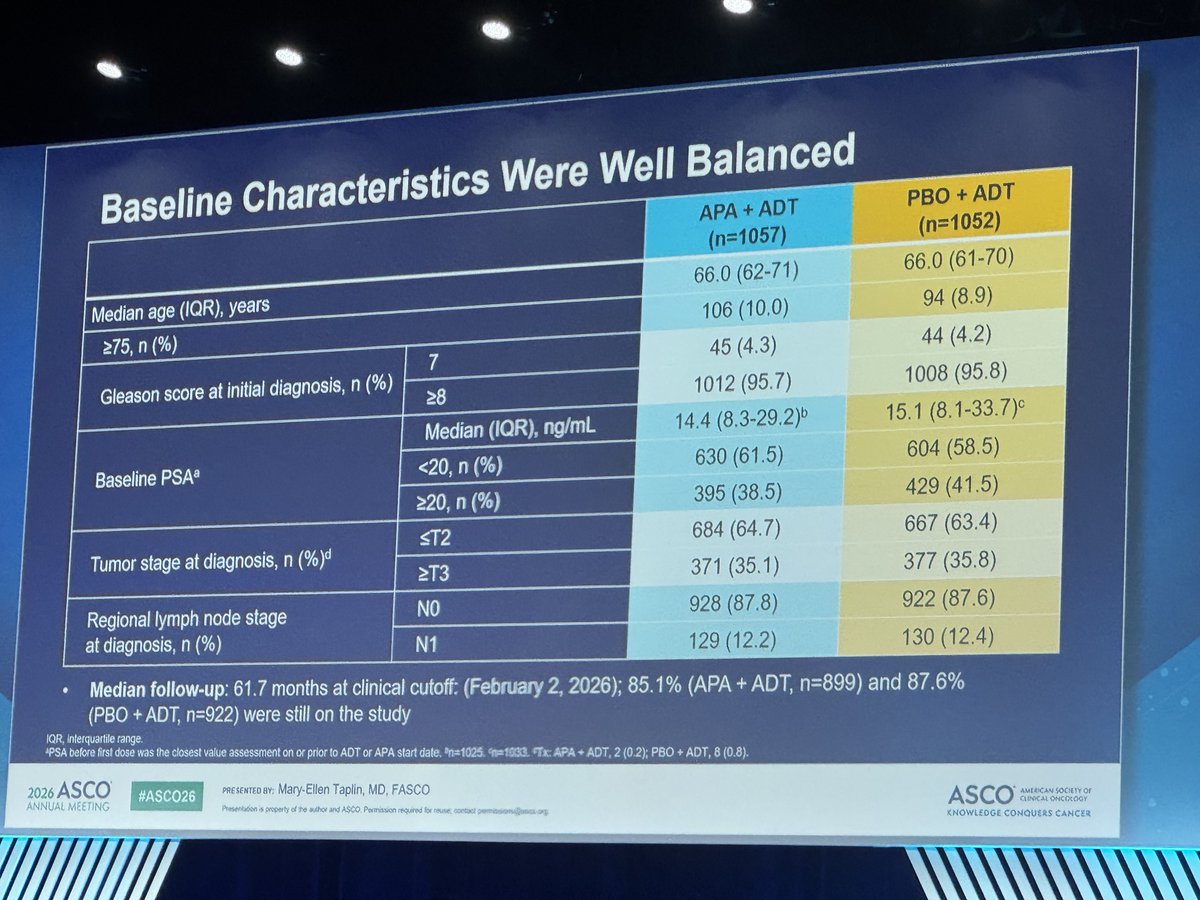
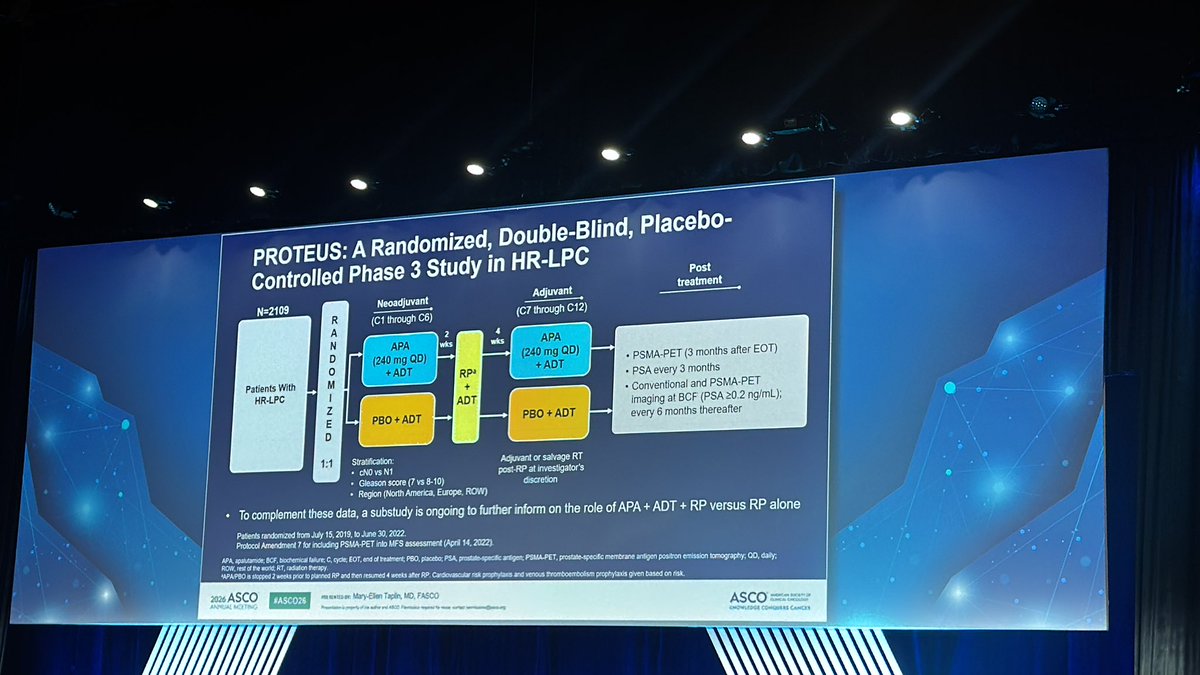
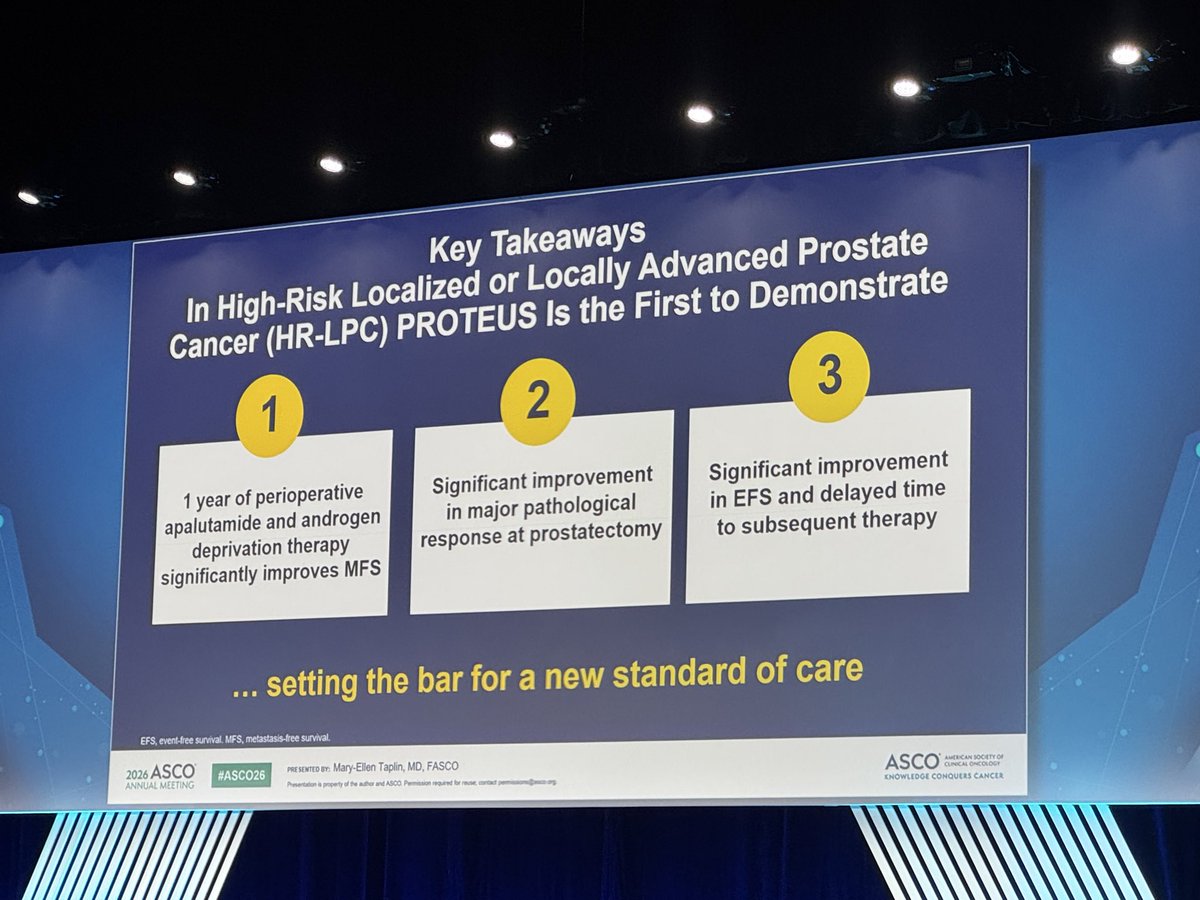
1️⃣ PROTEUS
Perioperative apalutamide ADT in high-risk localized prostate cancer
2️⃣ LIBRETTO-432
Adjuvant selpercatinib in RET NSCLC
3️⃣ HARMONi-6
Ivonescimab chemo vs tislelizumab chemo in squamous NSCLC
4️⃣ RASolute 302
Daraxonrasib (RMC-6236) in metastatic pancreatic cancer
5️⃣ SARC041
Abemaciclib in dedifferentiated liposarcoma
⚡ FRONTLINE & PERIOPERATIVE SHIFTS
6️⃣ KEYNOTE-B15 / EV-304
EV pembrolizumab vs chemo in MIBC
7️⃣ LITESPARK-022
Pembrolizumab belzutifan in adjuvant ccRCC
8️⃣ AMBITION
Paclitaxel/bevacizumab ± atezolizumab in HR breast cancer
9️⃣ NeoADAURA
Neoadjuvant osimertinib in EGFR NSCLC
🔟 A-DREAM
ADT interruption strategies in mCSPC
🧬 PRECISION, ADCs & NEXT-GEN IMMUNOLOGY
1️⃣1️⃣ DESTINY-Breast06
T-DXd expands into HER2-ultralow disease
1️⃣2️⃣ CROWN (7-year update)
Lorlatinib durability in ALK NSCLC
1️⃣3️⃣ DeLLphi-312
Tarlatamab in frontline SCLC
1️⃣4️⃣ COMMIT
Atezolizumab FOLFOX/Bev in MSI-H mCRC
1️⃣5️⃣ IMvigor011
ctDNA-guided adjuvant atezolizumab in bladder cancer
#OncoTwitter #MedTwitter #ASCO26 #CancerResearch @OncoAlert @ASCO @JCOPO_ASCO @OncBrothers
9
160
380
98,672
Matt Cooperberg retweeted

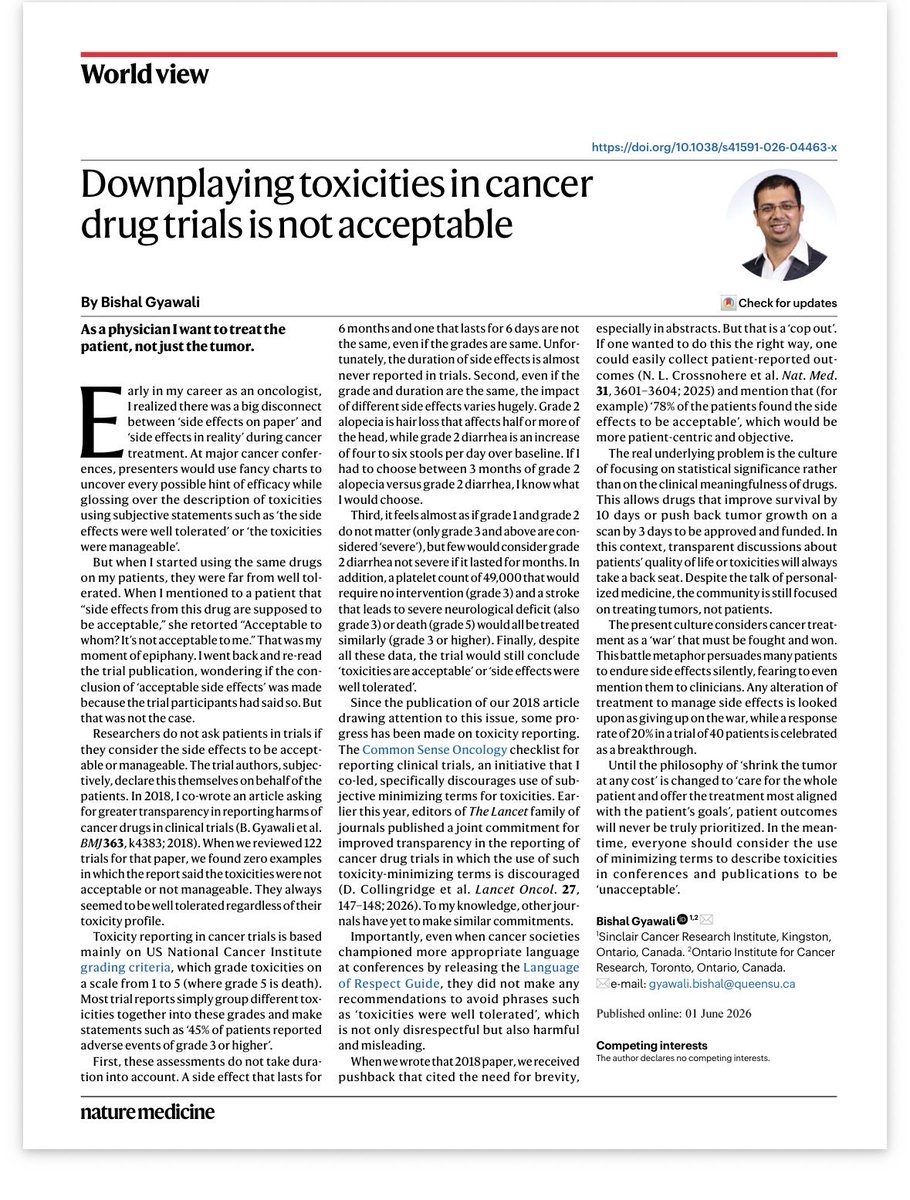
The most important paper of #ASCO26 just dropped in Nature Med! Or any other @asco or @myESMO meetings to be honest. When you hear someone present “the toxicities were acceptable”, please respond “downplaying toxicities is not acceptable”. Thank you @NatureMedicine for publishing this piece.
nature.com/articles/s41591-0…
19
97
397
54,376
Matt Cooperberg retweeted

#ASCO26 GU Oncology Spotlight 🚨
🔬 Abstract 5005 | ARACOG / AFT-47
Cognitive effects of darolutamide vs enzalutamide
Presented by Alicia K. Morgans, MD, MPH, FASCO
@CaPsurvivorship
@OncoAlert
@ASCO
In prostate cancer, we often discuss AR pathway inhibitors through the lens of:
• efficacy
• survival
• disease control
• sequencing
But for many patients, another question is just as important:
➡️ How will this treatment affect how I think, function, and live day to day?
That is why ARACOG is clinically relevant.
🟦 Study design
ARACOG / AFT-47 was a randomized phase II study evaluating cognitive function in patients treated with:
• darolutamide
vs
• enzalutamide
Population included patients with prostate cancer across disease states:
• mHSPC
• mCRPC
• nmCRPC
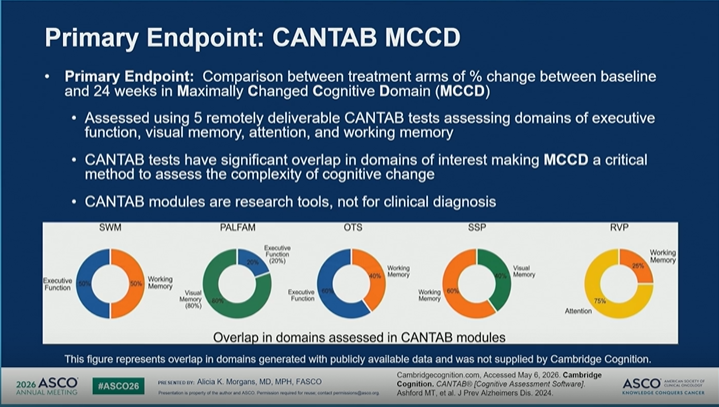
Cognitive outcomes were assessed using remotely deliverable CANTAB modules, evaluating domains such as:
🔹 executive function
🔹 visual memory
🔹 attention
🔹 working memory
🟩 Why this endpoint matters
The primary endpoint was change from baseline to 24 weeks in the maximally changed cognitive domain.
This is important because cognitive change can be subtle.
And in repeated cognitive testing, patients with stable cognition may show a “learning effect” — meaning scores can improve simply because they become familiar with the test.
So stable or declining scores over time may signal a real issue.
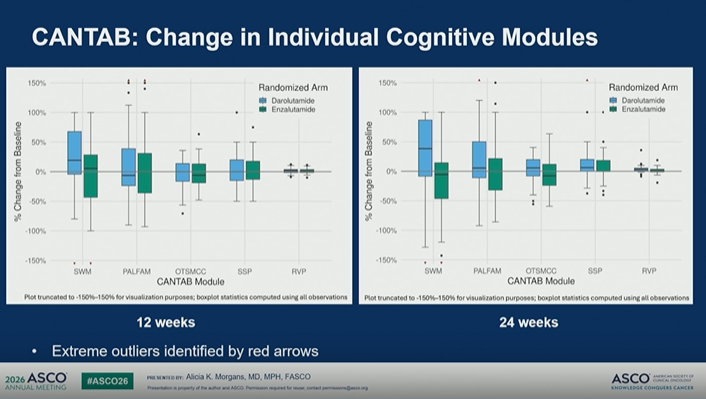
🟨 Key cognitive signal
At 24 weeks, darolutamide-treated patients showed increased median test scores across several domains, consistent with a learning effect and stable function.
Enzalutamide-treated patients had stable to decreased median scores, suggesting potential cognitive decline.
Several CANTAB module differences favored darolutamide at 24 weeks.
🟧 Crossover tells a story
Crossover criteria included:
• ≥30% decline in any CANTAB module
• ≥10-point decline in FACT-Cog
• fall or increased fall risk
• ≥ grade 2 neurologic toxicity
Observed crossovers:
➡️ Enzalutamide → darolutamide: 30 patients
➡️ Darolutamide → enzalutamide: 0 patients
That asymmetry is clinically meaningful.
🟥 My take
This study reminds us that ARPI selection is not only about tumor control.
It is also about:
✓ cognition
✓ falls
✓ neurologic toxicity
✓ daily function
✓ treatment adherence
✓ quality of life
✓ patient preference
For a patient who is older, frail, cognitively vulnerable, working, caregiving, or worried about concentration and memory, these data matter.
The key message:
In prostate cancer, living longer is essential — but preserving cognition and function should be part of the treatment conversation.
#ASCO26 #GUOnc #ProstateCancer #ARPI #Darolutamide #Enzalutamide #Cognition #QualityOfLife #PatientCenteredCare

2
25
36
2,659
Jun 2
Here’s a view of the @McCormick_Place convention hall my guess is 99.9x% of #ASCO26 and other meeting attendees never see. A stone’s throw and a world away! #northerlyisland #beautifulchicago
1
1
12
818
Matt Cooperberg retweeted

Cheers, chills, and a standing ovation when RASolute 302 showed unprecedented survival on daraxonrasib for patients with progressive pancreatic cancer
Seldom do you sense you’re witnessing a historic moment in cancer care but this feels like ras targeting has arrived
#ASCO26
92
1,273
6,504
1,148,590
Jun 2
A couple years ago ASCO was competing w Taylor Swift for Chicago’s attention. At #ASCO26… 🤔🤷♂️

4
782
Matt Cooperberg retweeted

May 31
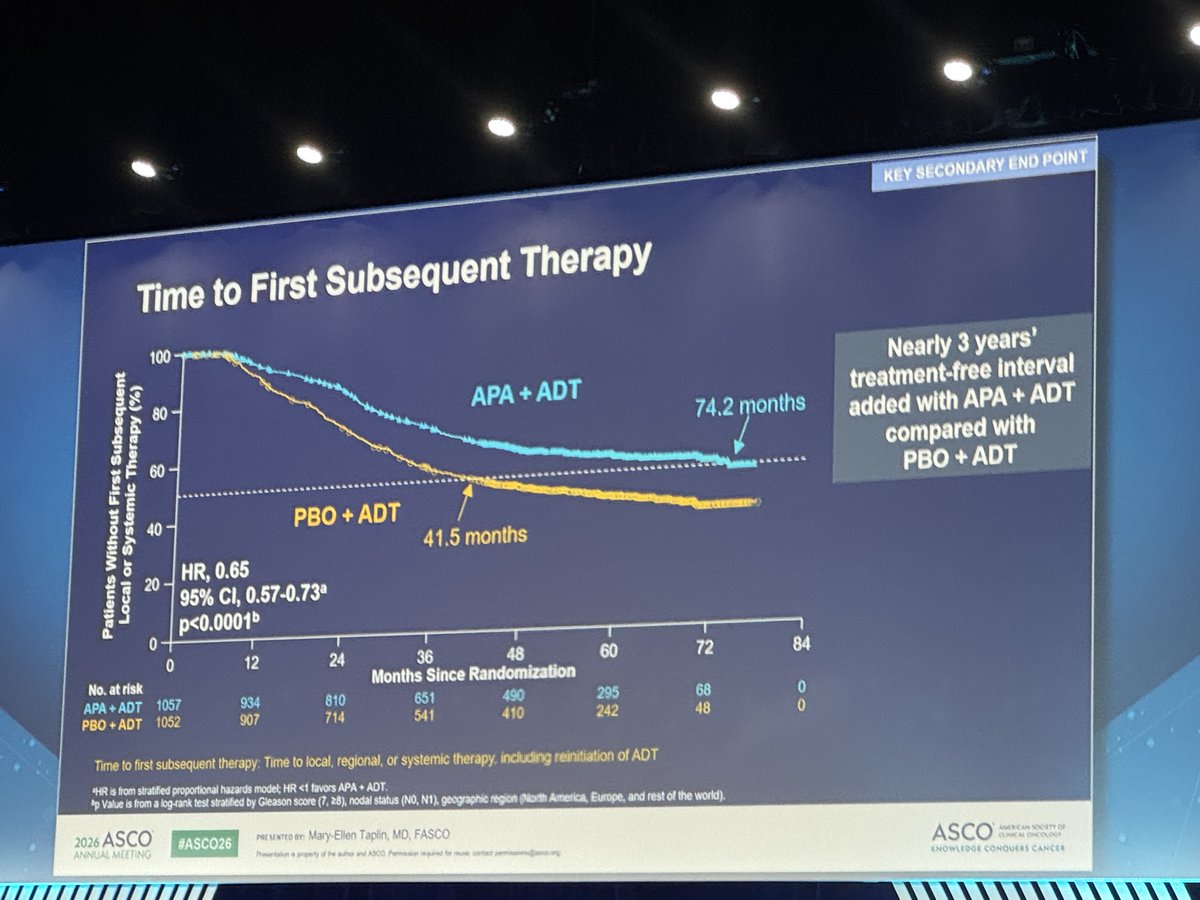
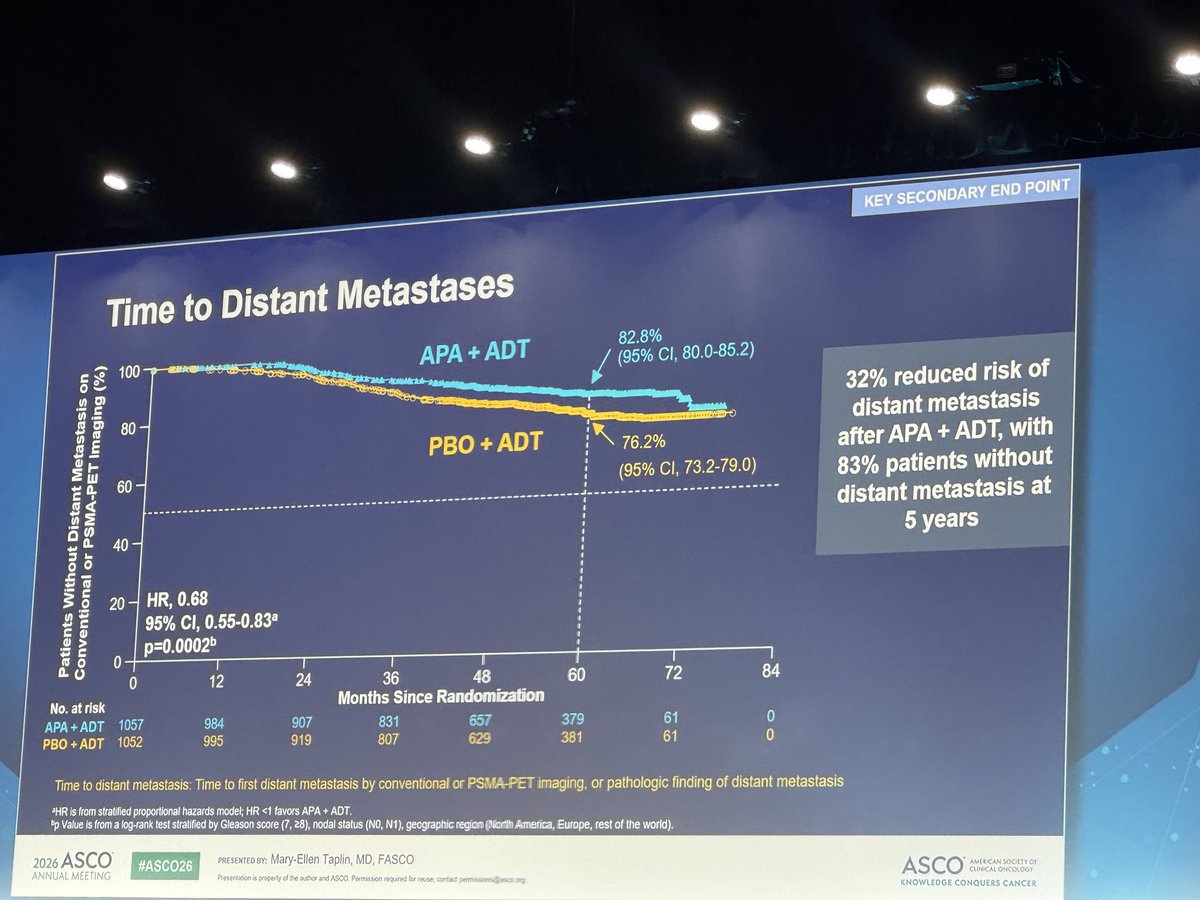
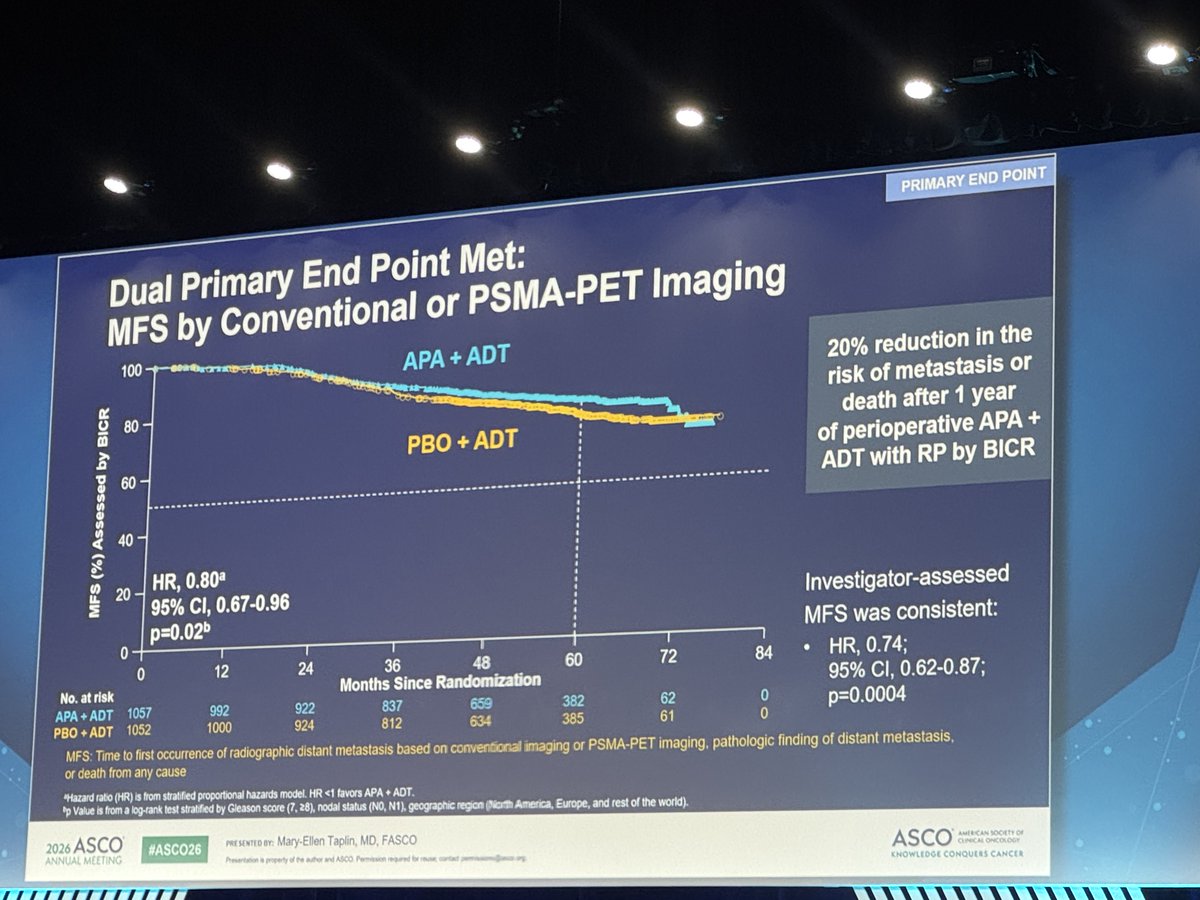
#PROTEUS trial: Neoadjuvant apalutamide and androgen deprivation therapy in high-risk localized #ProstateCancer. Mary-Ellen Taplin, MD @DanaFarber joins @TDorffOnc @cityofhope to discuss the results. Pathologic complete response of five millimeters or less of residual tumor occurred in 9% of the apalutamide arm vs 1% with placebo; favorable residual cancer burden was achieved in 30% vs 11%, with an odds ratio of 3.3. The study showed that metastasis-free survival favored apalutamide with a hazard ratio of 0.8, and patients receiving apalutamide required 30% less postoperative radiation. #WatchNow on UroToday > bit.ly/3RCNnhX #ASCO26
1
7
36
4,026
Matt Cooperberg retweeted
Jun 1
Discussion between expert clinicians and patient advocates on the #OPTIMUM trial, a #JournalClub for patients with #ProstateCancer. @dr_coops @UCSFCancer is joined by experts in the field to discuss the OPTIMUM trial of 1,020 biopsy‑naive men, where microultrasound‑guided biopsy was non‑inferior to MRI‑guided biopsy for detecting Gleason Grade Group ≥2 prostate cancer. Microultrasound offers key practical advantages. #WatchNow to learn more > bit.ly/4b6olxL
3
2
342
Matt Cooperberg retweeted

May 31
No need to buy expensive Proton Machines - a bog standard Linac just as good and much cheaper. Very important results and congratulations to the authors for doing the study.
May 31
#COMPPARE early results: in localized #ProstateCancer, #proton therapy vs #IMRT showed no sig difference in pt-reported bowel urgency/frequency, ≥G2 GI toxicity, or 3-year biochemical control. Longer follow-up needed for late toxicity/long term outcomes #ASCO2026
3
8
38
5,762
Matt Cooperberg retweeted
May 31
Protocol for ADHERE: A randomized controlled trial evaluating a digital exercise intervention with virtual supervised group exercise sessions compared to standard of care for patients receiving ADT for #ProstateCancer. Presentation by @Prof_Nick_James @ICR_London. #ASCO26 written coverage by @RKSayyid @UAUrology > bit.ly/49yup26 @ASCO
1
7
9
475