
Practice changing discussions by community oncologists-Rohit Gosain @RoswellPark & Rahul Gosain @WilmotCancer. OwnViews/NoMedAdvice.COI bit.ly/3o9agL3
Joined August 2021
- Tweets 6,673
- Following 494
- Followers 21,446
- Likes 26,618
1,507 Photos and videos






Pinned Tweet

Jun 11
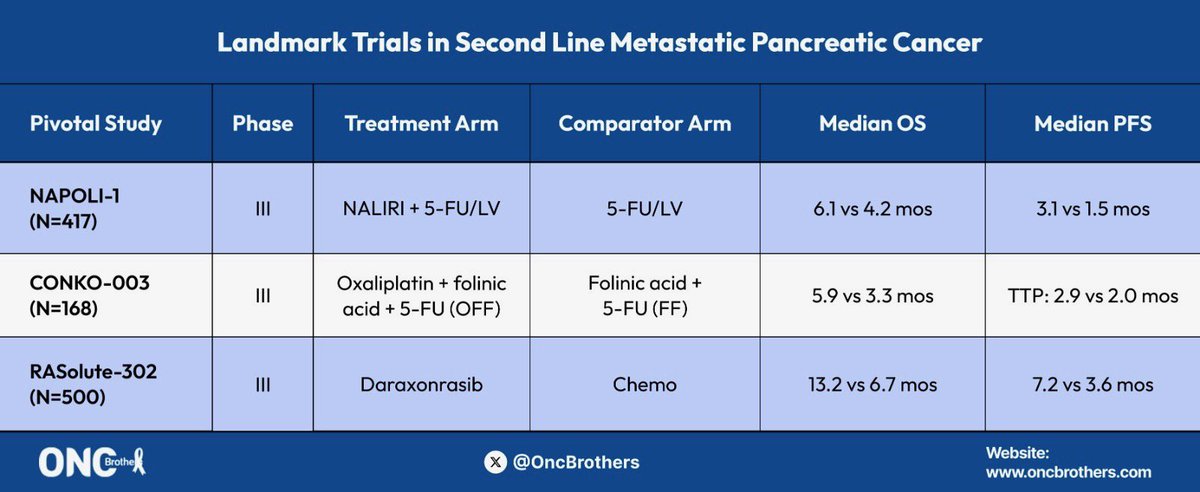
RASOLUTE-302 (GI Conference Highlights) from #ASCO26 w/ #BrianWolpin from @DanaFarber
✅ Other GI studies covered in our next episode w/ @NVijayvergiaMD
Full 🗣️
⭐️ “Oncology Brothers” podcast
⭐️ oncbrothers.com/rasolute-302…
#OncTwitter #MedTwitter #gism @OncUpdates
11
22
5,509
Oncology Brothers retweeted

With Tal-Dara published and concerns about ataxia/ balance disorders lets take a deep dive on GPRC5D ataxia syndrome
-> The first report of a cerebellar syndrome from GPRC5D came from MCARH019 reported by Mailankody et al
-2/17 (12%) Grd 3 cerebellar syndrome
-6.5 and 8.4 mo's after infusion
-was a DLT at 450*10^6
2
5
18
1,413
Oncology Brothers retweeted

My thoughts on new data from EHA. When considered in context of other recently published studies, these results should definitively end the practice of high-dose methotrexate prophylaxis in DLBCL. @JCO_ASCO
ascopubs.org/doi/10.1200/JCO…
2
15
41
6,425
Oncology Brothers retweeted

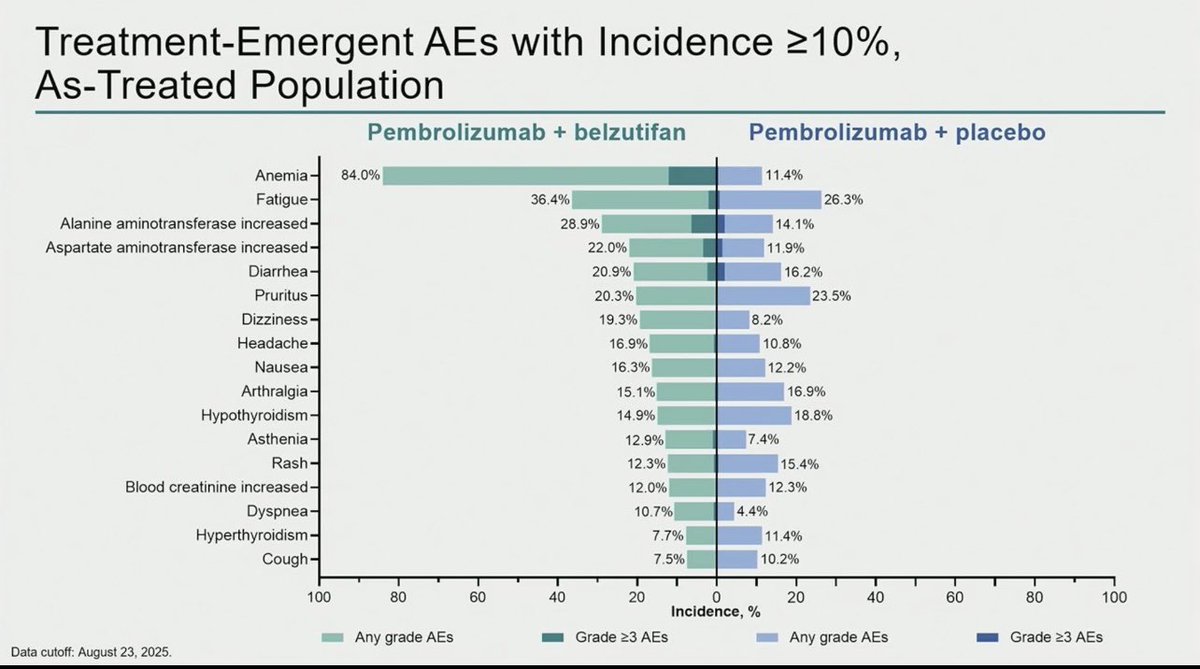
Now that adjuvant pembro plus Belzutifan is approved by @usfda
How will you decide who needs 1 drug vs 2 drugs in adjuvant RCC
pT3 NO clear cell RCC , Fit pt .
What will you u give in adjuvant .
Do vote below and opine 🙂 @OncBrothers @yekeduz_emre @dr_yakupergun @DrChoueiri
39%
Pembro Belzutifan
39%
Pembrolizumab alone
17%
Observation
4%
I don't know
23 votes • 10 hours
3
6
12
1,799
Oncology Brothers retweeted

Just out: presented at #EHA26 and published @NEJM
Randomized trial of 2 talquetamab combinations vs DPd in relapsed myeloma. The Monumental-3 trial.
Both Talq-Dara-Pom and Talq-Dara beat DPd in PFS and OS.
Choice of a Talq combination vs Tec or Tec-Dara in relapsed myeloma will be driven by patient and disease factors and requires significant expertise. Congrats @RobertoMinaMD @PlasmaCellPete @mbeksac56 @paurotero @mvmateos @thanosdimop @RahulBanerjeeMD et al.
nejm.org/doi/full/10.1056/NE…

2
30
91
8,599
Oncology Brothers retweeted

Jun 12
🚨 FDA Approves capivasertib Plus Abiraterone as First Targeted Therapy for PTEN-Deficient Metastatic Hormone-Sensitive Prostate Cancer
Source AstraZeneca
buff.ly/ldFb96p
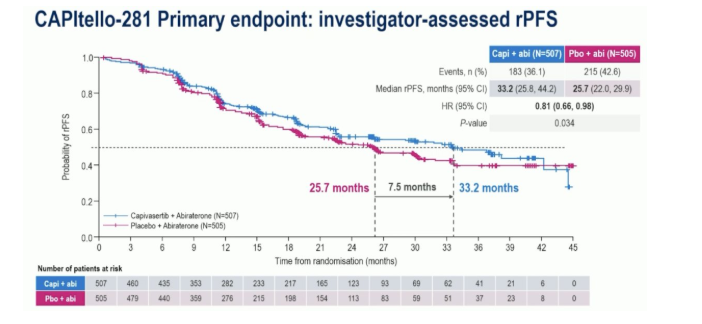
The FDA has approved capivasertib in combination with abiraterone and prednisone as the first targeted therapy for patients with PTEN-deficient metastatic androgen pathway modulation-naïve or sensitive #ProstateCancer . Approval was based on the Phase III CAPItello-281 trial, which demonstrated a 19% reduction in the risk of radiographic progression or death and improved median radiographic progression-free survival by 7.5 months. The decision also highlights the growing importance of biomarker-driven treatment and PTEN testing in advanced prostate cancer.
@montypal @crisbergerot @DrDanielHeng @apolo_andrea @DrChoueiri @PGrivasMDPhD @TiansterZhang @HHammersMD @ravikanesvaran @neerajaiims @amerseburger @sonpavde @drenriquegrande @scserendipity1 @Silke_Gillessen @EfstathiouEleni @tompowles1 @BraunMDPhD @nataliagandur @cdanicas @brian_rini @AOmlin
#OncoAlertAF
@nataliagandur @realbowtiedoc @Onco_Cifu88 @scocmem
3
18
40
3,057
Oncology Brothers retweeted

Jun 12
Just in (again, Friday FDA notices): The @US_FDA
approved Capivasertib (oral AKT inhibitor) for metastatic Hormone-Sensitive prostate Cancer with PTEN deficiency (by IHC; 90% ).
4/30: ODAC voted 7-1 for a favorable benefit-risk profile based on the CAPItello-281 Phase III trial results (HR: 0.81)
astrazeneca.com/media-centre…
Another example of personalized medicine in #oncology
With HIF2 inhibitor Belzutifan approval today (x.com/DrChoueiri/status/2065…), it is a great day for #GU Cancer patients
@OncoAlert @AUC3_Official @DanaFarber_GU @PCFnews @OncBrothers @OncLive

Jun 12

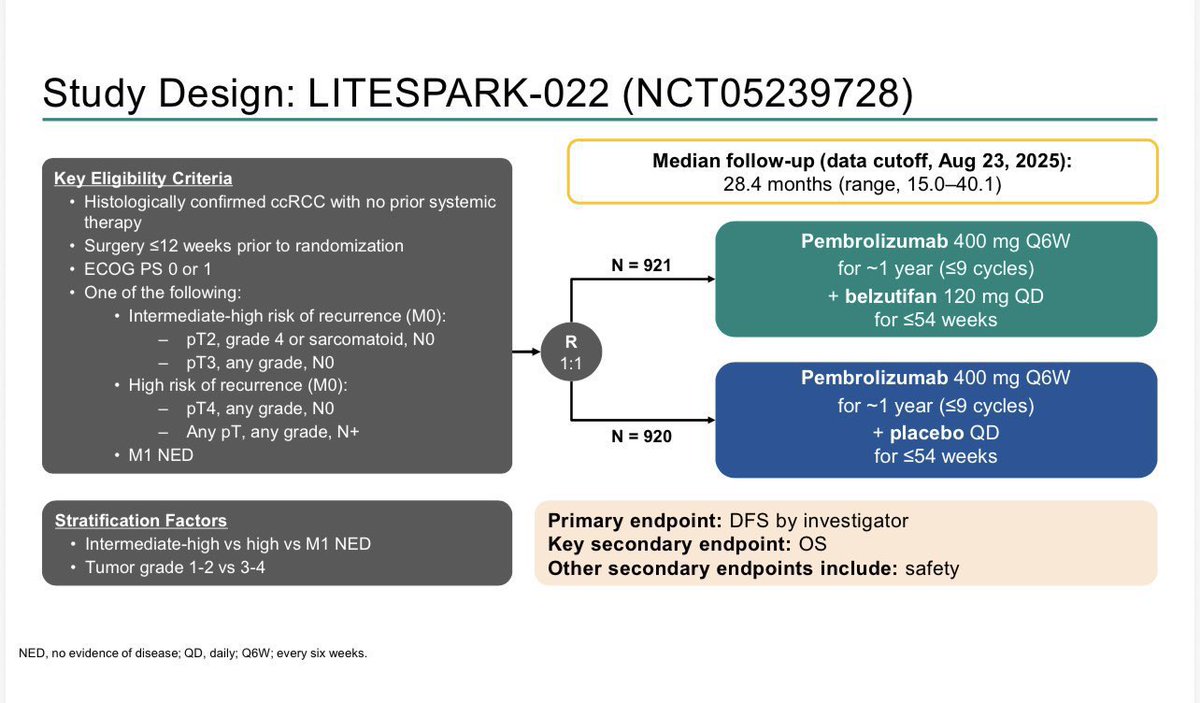
JUST IN: @US_FDA approves combo HIF2 inhibitor Belzutifan PD1 inhibitor Pembrolizumab in adjuvant Kidney Cancer. Approval based on LS022 trial co-led with @tompowles1 presented @ASCO #GU26 adding another approval to @NobelPrize story with @kaelin_lab @DanaFarber @DanaFarber_GU !
Onward ! Great day for patients !
#HIF2 #oncology #labubu
dailynews.ascopubs.org/do/li…
blog.dana-farber.org/insight…


3
32
77
8,954
Jun 12
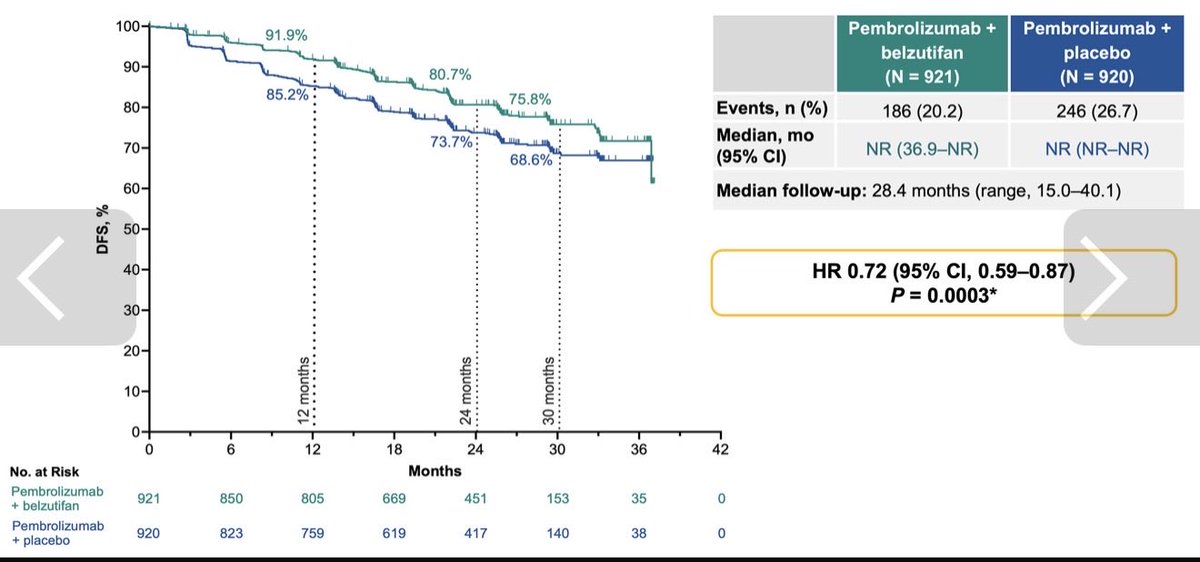
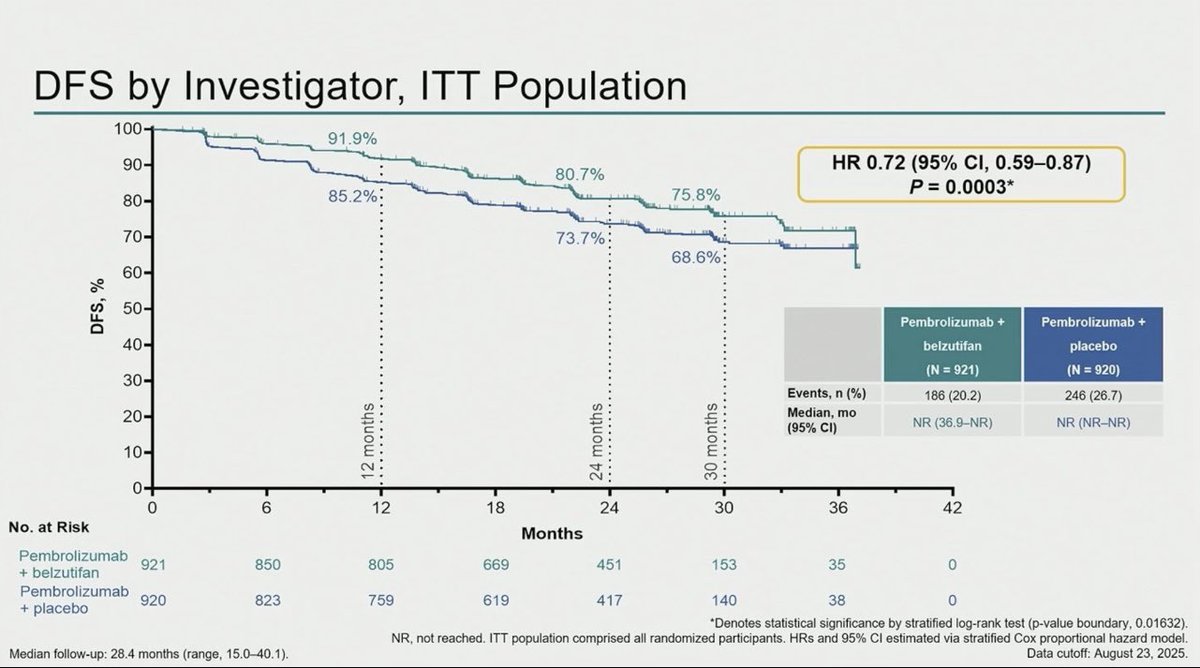
Belzutifan Pembro now @US_FDA ✅ based off LITESPARK-022: PhIII (vs. Pembro) in adj RCC:
- 2.5yrs DFS: 75.8% vs. 68.6% (HR: 0.72)
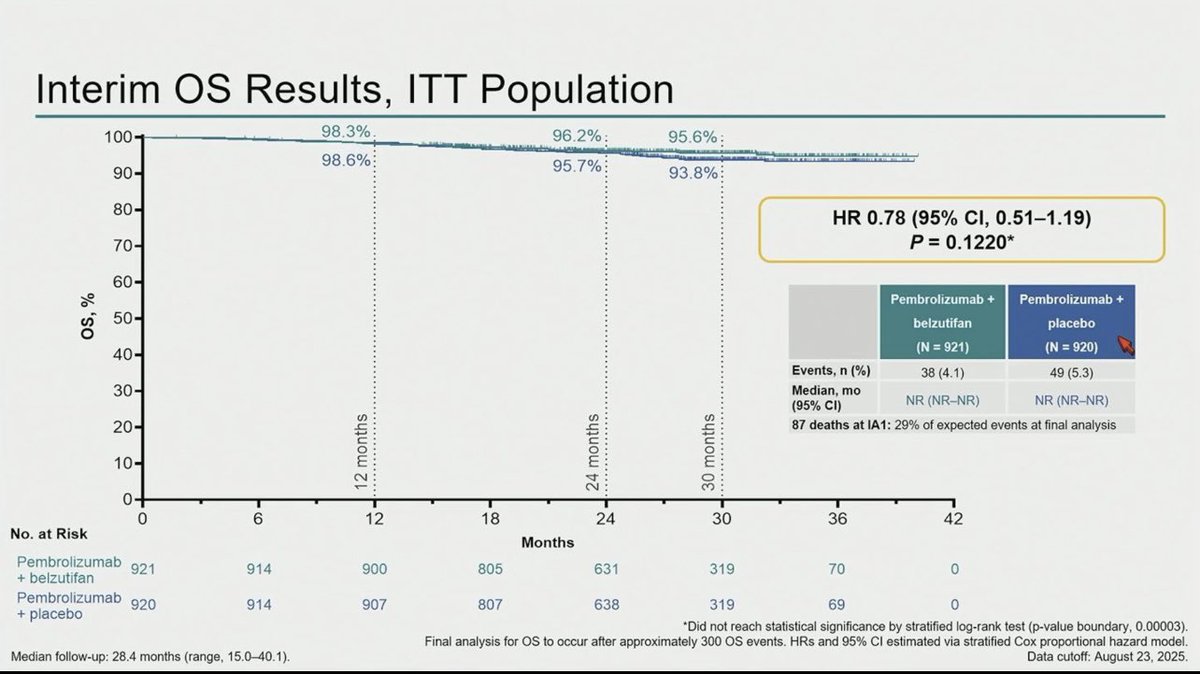
- mOS NR
- 2.5yrs OS: 95.6% vs. 93.8% (HR: 0.78)
- AEs: 42.2% vs. 17.9% w/ Gr ≥ 3
#MedTwitter #gusm #KidneyCancer @OncoAlert
2
33
58
4,333
Jun 12
What were you feeling when you first saw the data? 🤯🤯
#OncTwitter #MedTwitter #MedX #RASolute302 @OncUpdates @OncoAlert
Jun 11

RASOLUTE-302 (GI Conference Highlights) from #ASCO26 w/ #BrianWolpin from @DanaFarber
✅ Other GI studies covered in our next episode w/ @NVijayvergiaMD
Full 🗣️
⭐️ “Oncology Brothers” podcast
⭐️ oncbrothers.com/rasolute-302…
#OncTwitter #MedTwitter #gism @OncUpdates
2
9
16
2,145
Oncology Brothers retweeted

Jun 12
Second-line case question
Metastatic HR−/HER2 breast cancer
1L: T-DXd pertuzumab
Progression after durable disease control
No brain metastases
What would be your preferred 2L treatment?
21%
THP
17%
T-DM1
62%
Tucatinib cape trastzumab
77 votes • Final results
4
3
11
4,076
Oncology Brothers retweeted

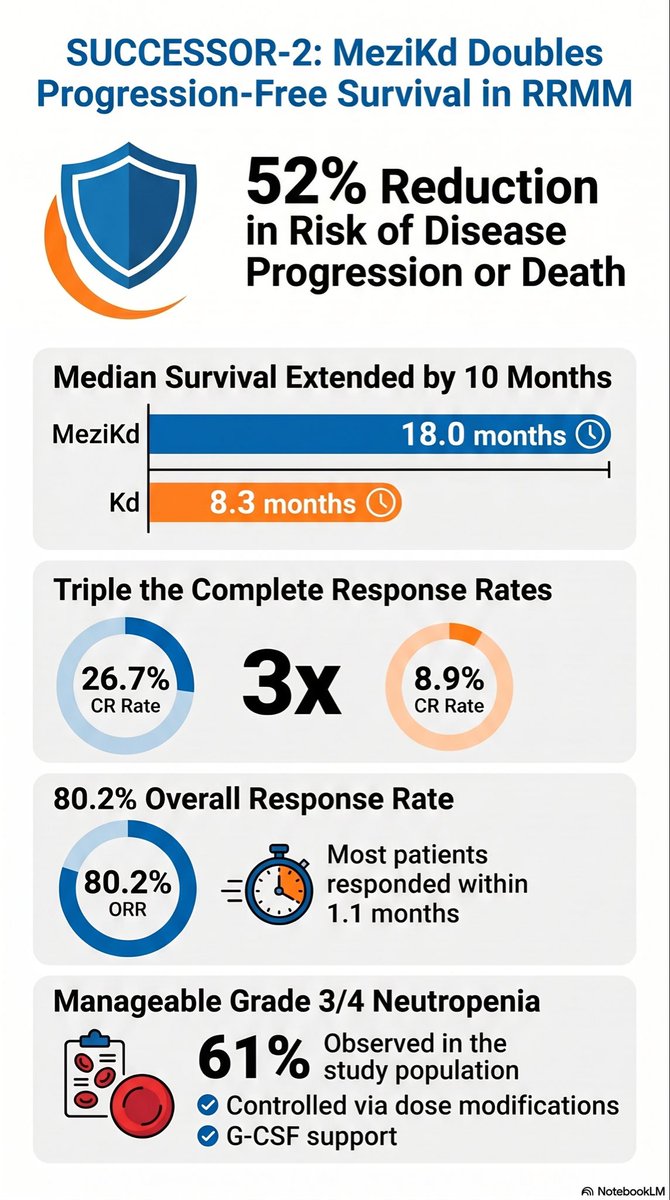
🔹 Is There Still a Place for Mezigdomide in the Modern Myeloma Treatment Landscape?
Let’s see what data we have before we jump to conclusions?
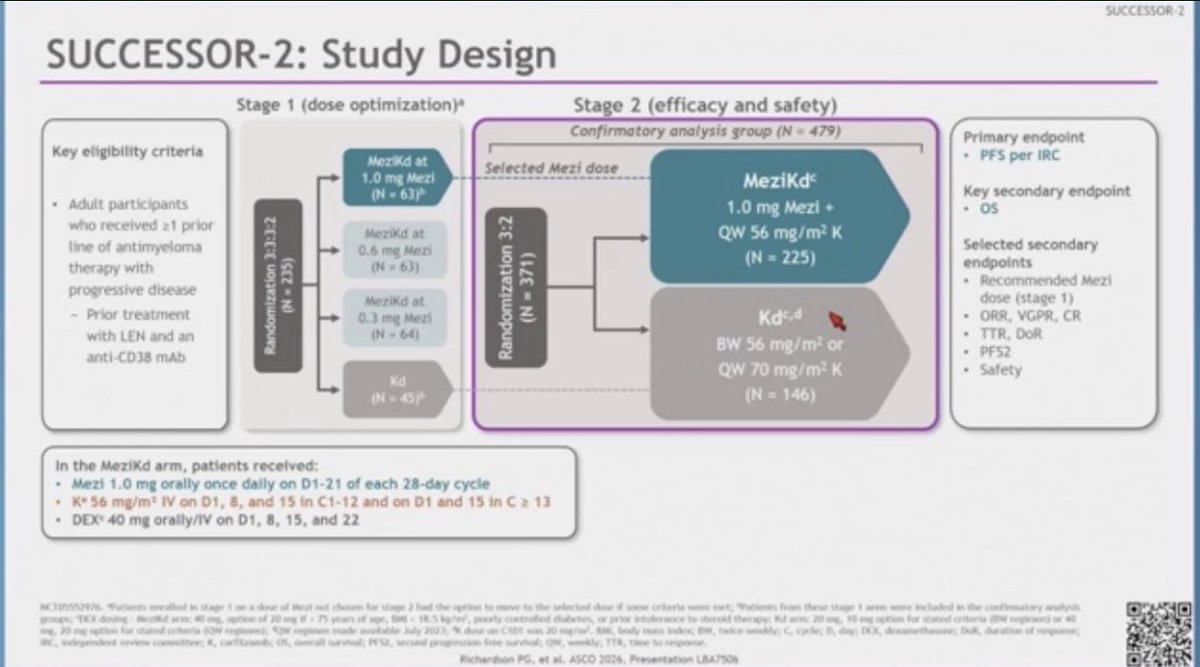
🧵 ASCO 2026 | SUCCESSOR-2: Mezigdomide Kd :
1/🔬 let’s start with the study Design (very Critical)
SUCCESSOR-2 randomized RRMM patients with:
✅ Prior lenalidomide exposure
✅ Prior anti-CD38 monoclonal antibody exposure
✅ ≥1 prior line of therapy
To receive:
🟢 Mezigdomide Carfilzomib Dexamethasone (MeziKd)
vs
⚪ Carfilzomib Dexamethasone (Kd)
Primary endpoint: PFS
#ASCO2026 #MultipleMyeloma #mmsm #USMIRC #MedEd #medtwitter @US_HMC @USMIRCNEWS @MedwatchKate @Larvol @oncodaily
2
9
22
1,900
Oncology Brothers retweeted

Did a fun 5-minute interview with my mentor @apolo_andrea about EV/pembro in bladder cancer oncupdates.com/video-podcast… @OncBrothers @OncUpdates
5
11
1,033
Oncology Brothers retweeted

Jun 11
It’s about time we remove CNS ppx in DLBCL from the NCCN guidelines.
High-Dose Methotrexate as CNS Prophylaxis in Ultra High-Risk Large B-Cell Lymphoma: An International Multicenter Analysis | Journal of Clinical Oncology ascopubs.org/doi/10.1200/JCO…
6
30
133
15,386
Oncology Brothers retweeted

Jun 11
I am not sure about you but those of us first learned Cancer Pharmacology in late 1980s. This is like coolest Sci-Fi stuff-RASolute-302 is a pivotal Phase 3 clinical trial investigating daraxonrasib, a targeted oral inhibitor, for previously treated mPDAC. Don’t wake me up
Jun 11
RASOLUTE-302 (GI Conference Highlights) from #ASCO26 w/ #BrianWolpin from @DanaFarber
✅ Other GI studies covered in our next episode w/ @NVijayvergiaMD
Full 🗣️
⭐️ “Oncology Brothers” podcast
⭐️ oncbrothers.com/rasolute-302…
#OncTwitter #MedTwitter #gism @OncUpdates
1
4
1,317
Oncology Brothers retweeted

Jun 9
I think there are two important messages here.
What is abundantly clear now is that prophylactic tocilizumab reduces the risk of CRS to less than 10%, with most of these cases being grade 1 that can be managed without requiring hospitalization or additional tocilizumab.
Equally important is the substantial cost reduction achieved with the lower, yet fully effective, prophylactic dose, leading to major cost savings for payers


I think 4 mg/kg is a great idea! Really cool concept and work by Hamadeh @szusmani et al looking at this concept…
we need more dose optimization work in this space especially for high-cost supportive care with bsAbs 👏
clinical-lymphoma-myeloma-le…

1
13
47
10,086
Oncology Brothers retweeted

Jun 10
Scalp cooling outcomes in patients receiving trastuzumab deruxtecan for metastatic breast cancer in @ESMO_Open. No benefit of scalp cooling in terms of hair preservation or quality of life.G2 alopecia primary reason for scalp cooling discontinuation. esmoopen.com/article/S2059-7…

1
27
50
25,726
Oncology Brothers retweeted
Jun 10
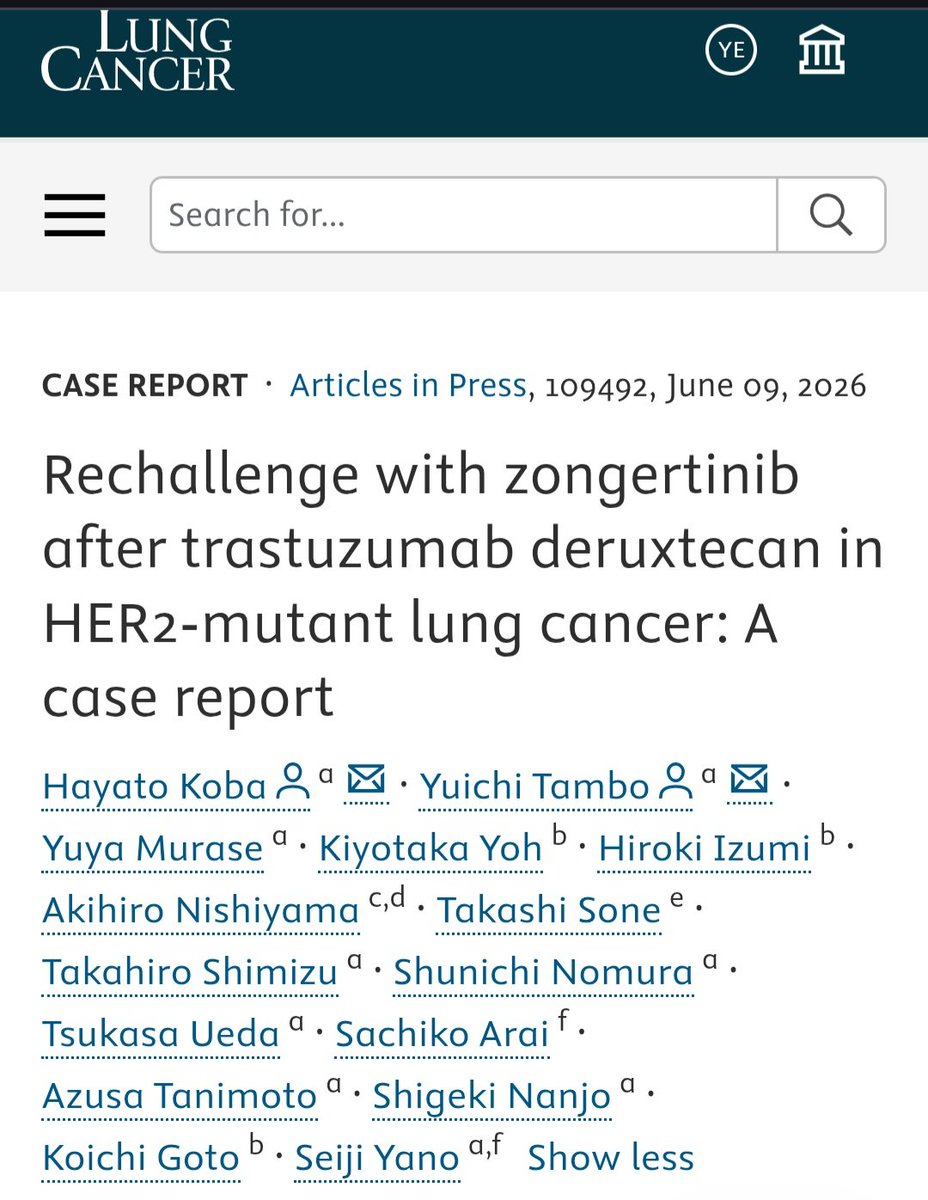
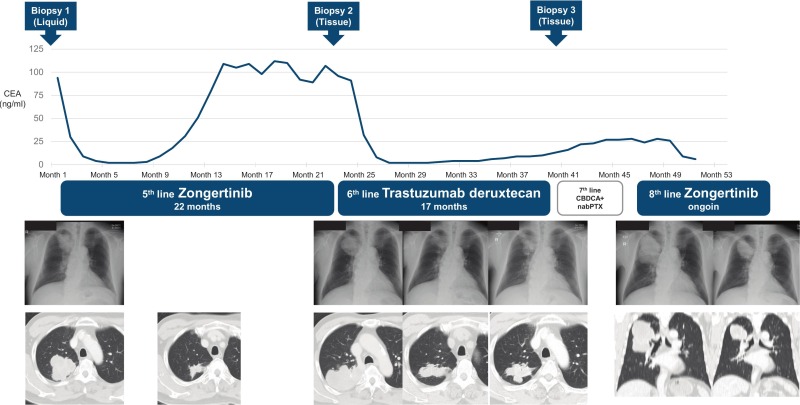
In HER2-mutant NSCLC, this is a highly instructive case.
The target is not fixed; the tumor keeps evolving under treatment pressure.
When serial biopsies show how the phenotype has changed, treatment can sometimes be adapted accordingly, even within the same molecular axis.
Zongertinib → T-DXd → zongertinib rechallenge.
A single case report, but a sharp biology lesson.
The dynamic evolution of the ADC–TKI sequence 👇
lungcancerjournal.info/artic…
9
26
2,877
Oncology Brothers retweeted

I really like this image 🙌🏽

3
26
99
6,351
Oncology Brothers retweeted

Jun 9
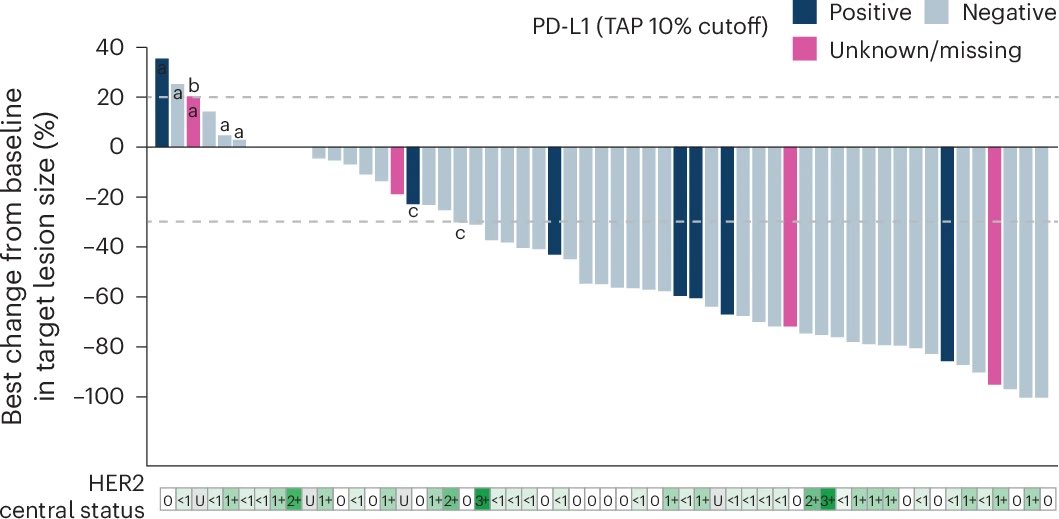
Results of the T-DXd/durva arm of #BEGONIA for 1L mTNBC are now out in @NatureCancer. High efficacy, with ORR 62% and mPFS 12.6 months. Strikingly, deep responses observed even in HER2-0 (null) dz, reminding that IHC is a poorly predictive ADC biomarker. nature.com/articles/s43018-0…
4
38
134
11,132
Oncology Brothers retweeted

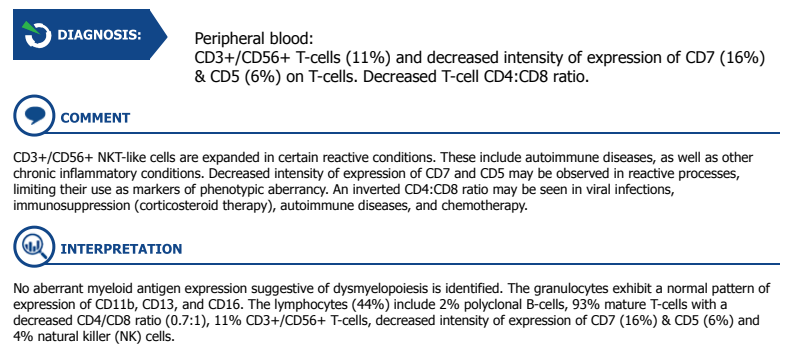
Need some help decoding this flow
83 MM pt on single agent Dara-no M spike doign well.
no recent infection
Mild persistent abs lymphocytosis for 6 months. around 5-6 k
Hb and plt ok. No rash. No auto immune dz.
is this T LGL?
Could this be from Dara ?
6
1
7
4,097