
Primary Care Physician | Educator | ASCVD, 🫀Failure, Diabetes | Addicted to 🏃♂️ 🏏 &🏌🏼♂️ Follows Jesus, loves family, tweets≠medical advice @RACGP
Joined September 2015
- Tweets 1,957
- Following 226
- Followers 3,127
- Likes 1,203
717 Photos and videos


Pinned Tweet

31 Jan 2025
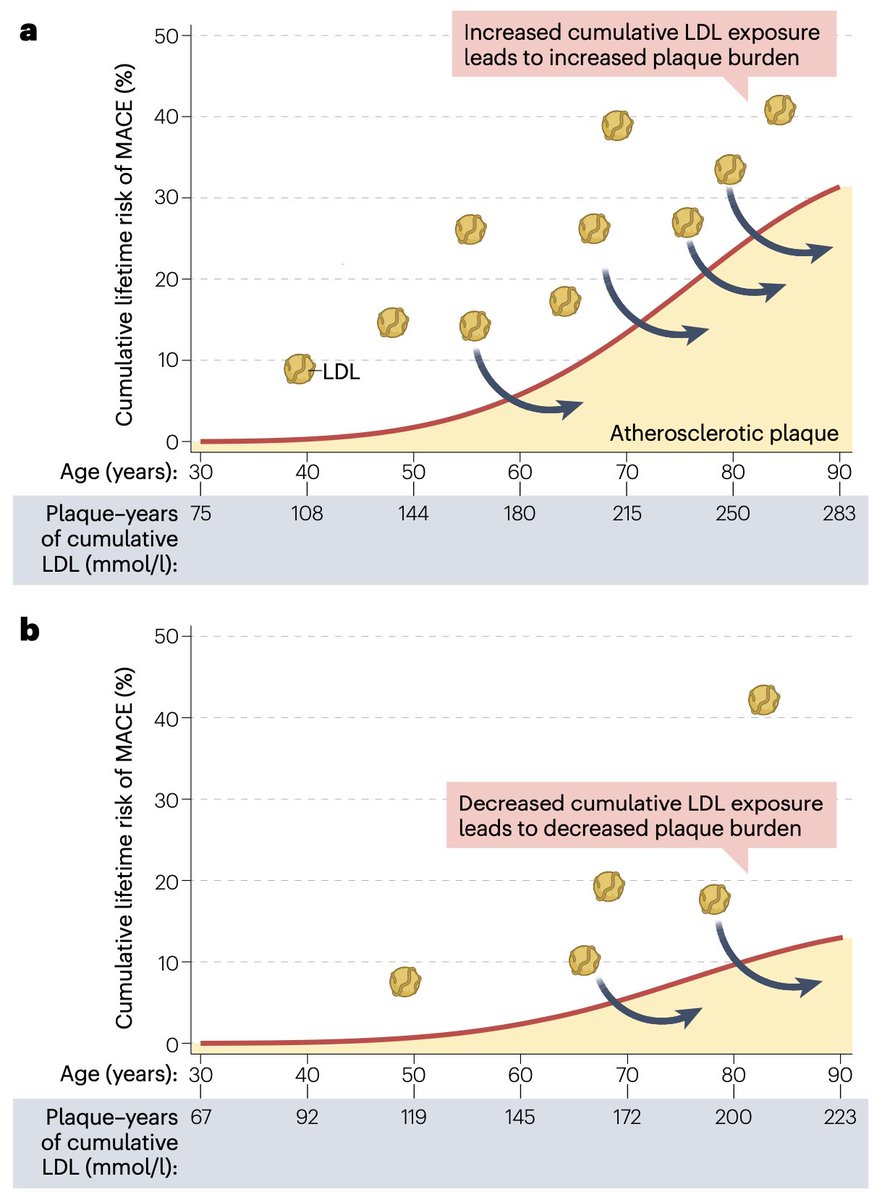
The LDL Cumulative Exposure Hypothesis
The longer your arteries are exposed to high LDL-C, the ⬆️ the risk of atherosclerosis. 📈
🔬 Early & sustained LDL lowering = lifelong CV benefit.
🔗 nature.com/articles/s41569-0…
#CardioTwitter #MedTwitter #FOAMed #MedED @ACCinTouch @escardio @atheroaussie @society_eas
16
92
303
48,502
Dr Rob 🫀🩺 🇦🇺 retweeted

Apr 11
👉 We spend decades arguing about how low to push LDL-C
👆 Almost no one asks the obvious question:
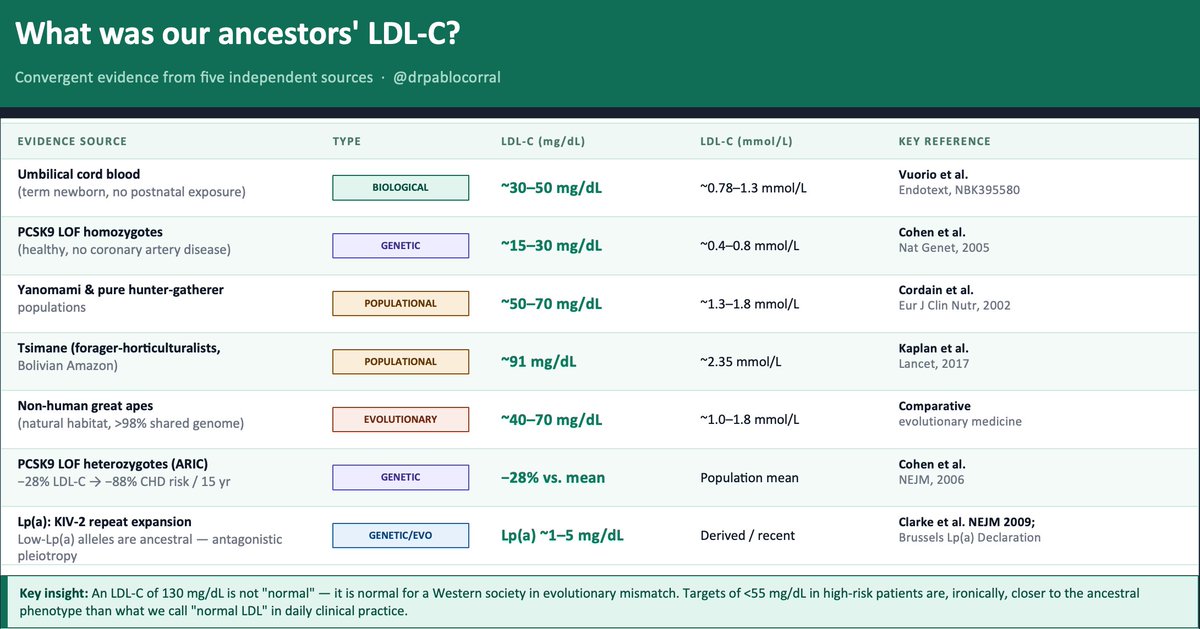
🤔 How much LDL-C did our ancestors actually have?
The evidence exists — five independent lines, all converging on the same uncomfortable answer.
1️⃣ The term newborn. Before any dietary or metabolic influence, a healthy neonate arrives with LDL-C of ~30–50 mg/dL. That is the LDLR operating without environmental interference. Everything that rises after birth is acquired.
2️⃣ The Tsimane (Kaplan et al., Lancet 2017) — forager-horticulturalists of the Bolivian Amazon — have a LDL-C between 70 to 90 mg/dL and the lowest prevalence of coronary atherosclerosis ever recorded in any human population. Five times less than the U.S. in adults over 75. And their LDL is rising as roads and processed food arrive.
3️⃣ PCSK9 loss-of-function variants. African American carriers of nonsense mutations (Y142X/C679X, ~2% frequency): −28% LDL-C and −88% CHD risk over 15 years (Cohen et al., NEJM 2006). Homozygous LOF carriers live with LDL-C of ~15–30 mg/dL. Perfectly healthy. Nature already ran the trial.
4️⃣ Evolutionary genetics. Recent positive selection signals exist on gain-of-function PCSK9 variants that raise LDL-C — likely adaptive in food-scarce ancestral environments. Modern hypercholesterolemia is not "normal." It is an ancestral survival advantage turned pathological by evolutionary mismatch.
5️⃣ Great apes in natural habitat: ~40–70 mg/dL LDL-C. Same genome. Different environment.
👆 Bonus — Lp(a). The KIV-2 repeat expansion that raises Lp(a) is a derived, recent variant. Low-Lp(a) alleles are ancestral. Elevated Lp(a) is a textbook antagonistic pleiotropy signal — possibly protective against bleeding early in life, atherogenic over decades
📍The convergent estimate: ancestral LDL-C was ~30–70 mg/dL.
📍An LDL-C of 130 mg/dL is not "normal." It is normal for a Western society in evolutionary mismatch. Targets of <55 mg/dL in high-risk patients — which still feel aggressive to many clinicians — are, ironically, closer to the ancestral phenotype than what we call "normal LDL" in daily practice.
🤔 The question is not "is it safe to lower LDL this much?"
The question is: why did we let it rise this high?
@society_eas
@nationallipid
25
89
355
75,609
Dr Rob 🫀🩺 🇦🇺 retweeted
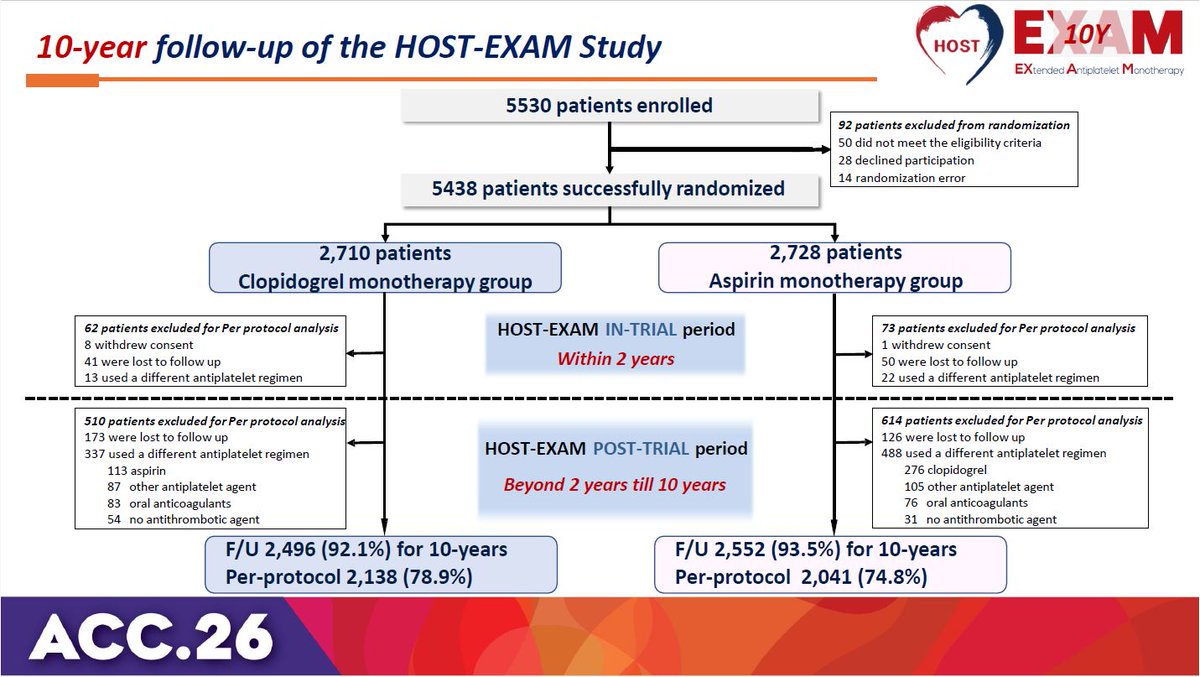
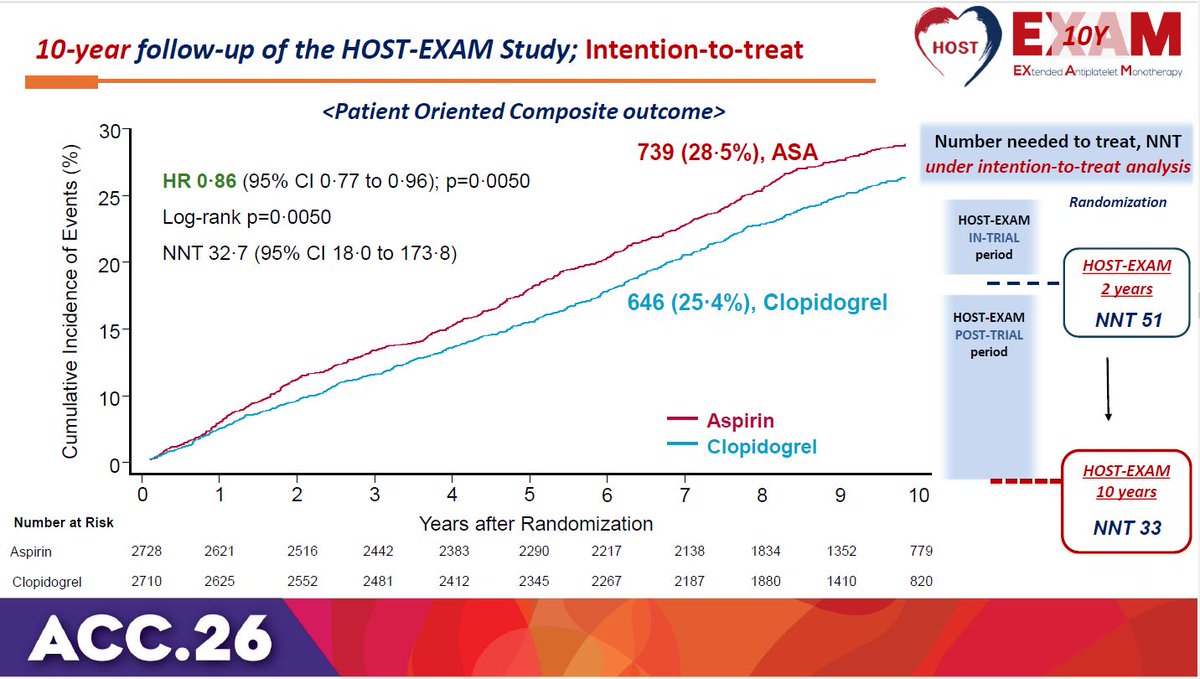
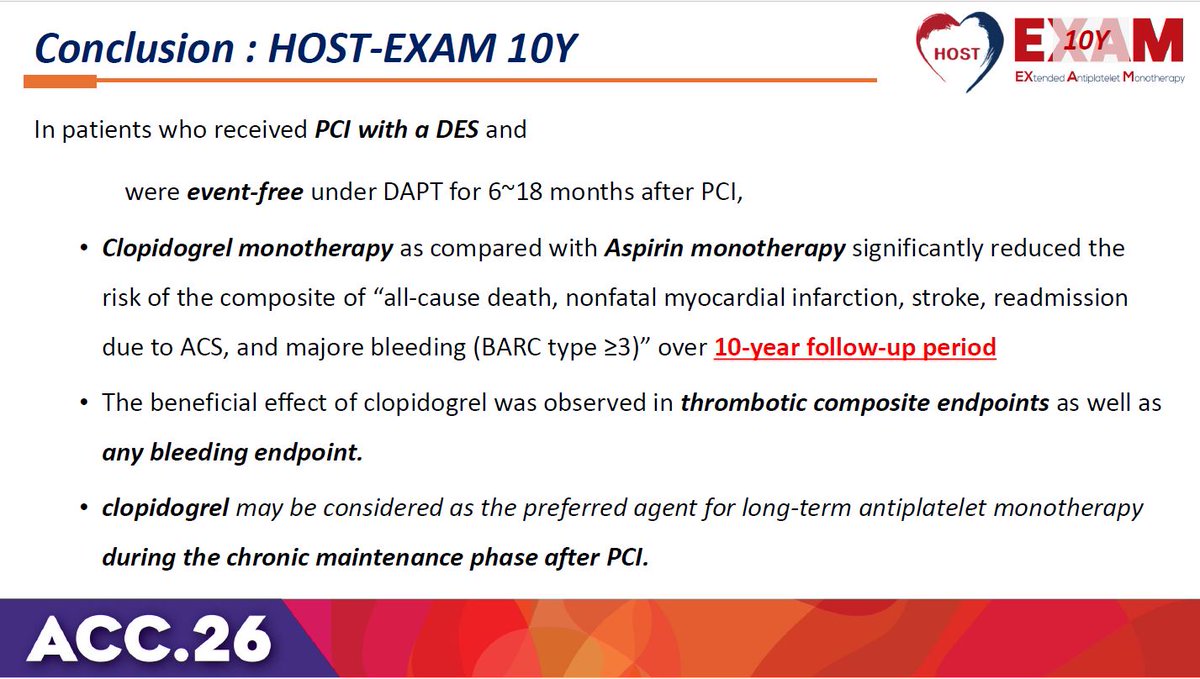
HOST-EXAM trial 10-year results: Clopidogrel monotherapy is superior to aspirin for chronic maintenance after PCI, significantly reducing both thrombotic and bleeding events. #ACC26 View slides here: clinicaltrialresults.org/wp-…

5
173
435
31,846
Dr Rob 🫀🩺 🇦🇺 retweeted
PCSK9 inhibitors transformed secondary prevention—
but what about primary prevention?
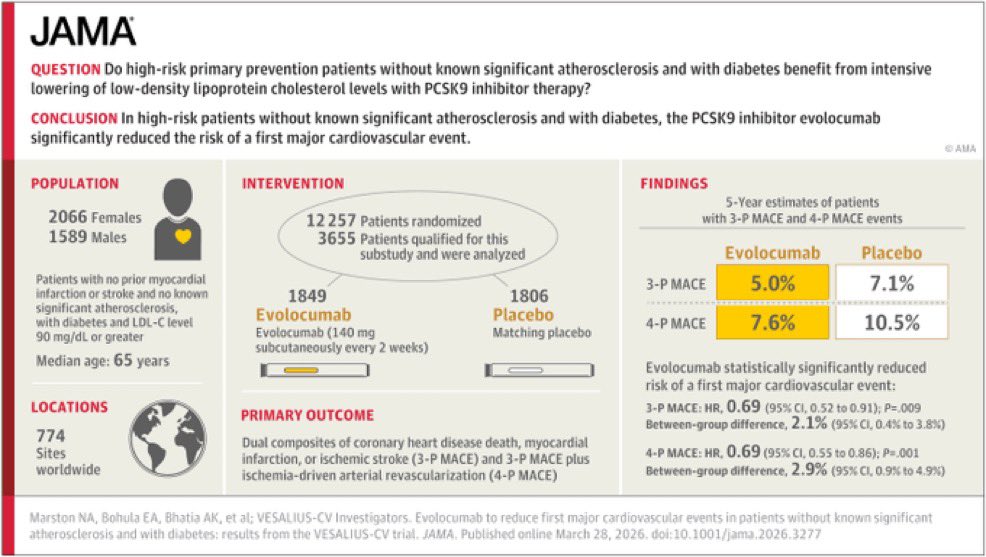
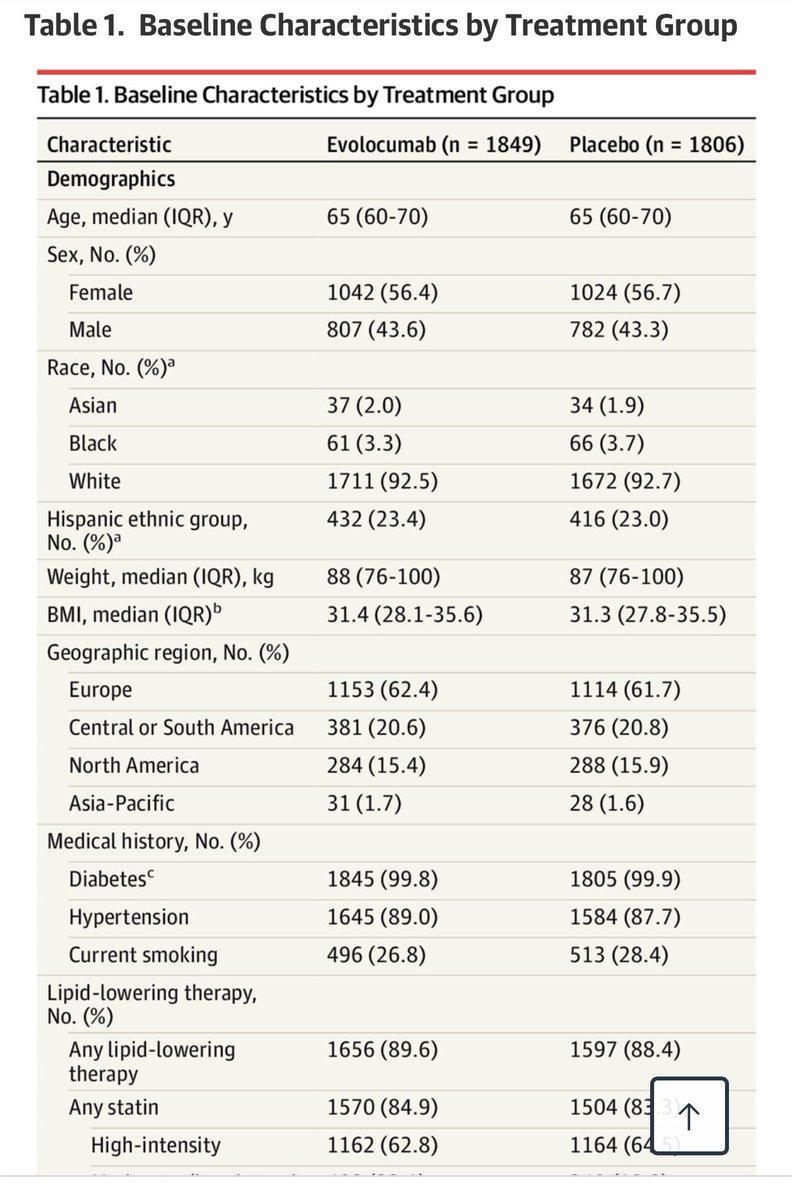
#VESALIUS-CV evaluates evolocumab in patients without established ASCVD.
Could this expand who we treat—and when?
➡️ Key results: evolocumab⤵️ CV events in this high risk primary prevention study!
56% 💃🏻
92% White
#ACC26 #Lipids #CvPrev @JAMACardio
📎 jamanetwork.com/journals/jam…


6
38
137
27,286
Dr Rob 🫀🩺 🇦🇺 retweeted
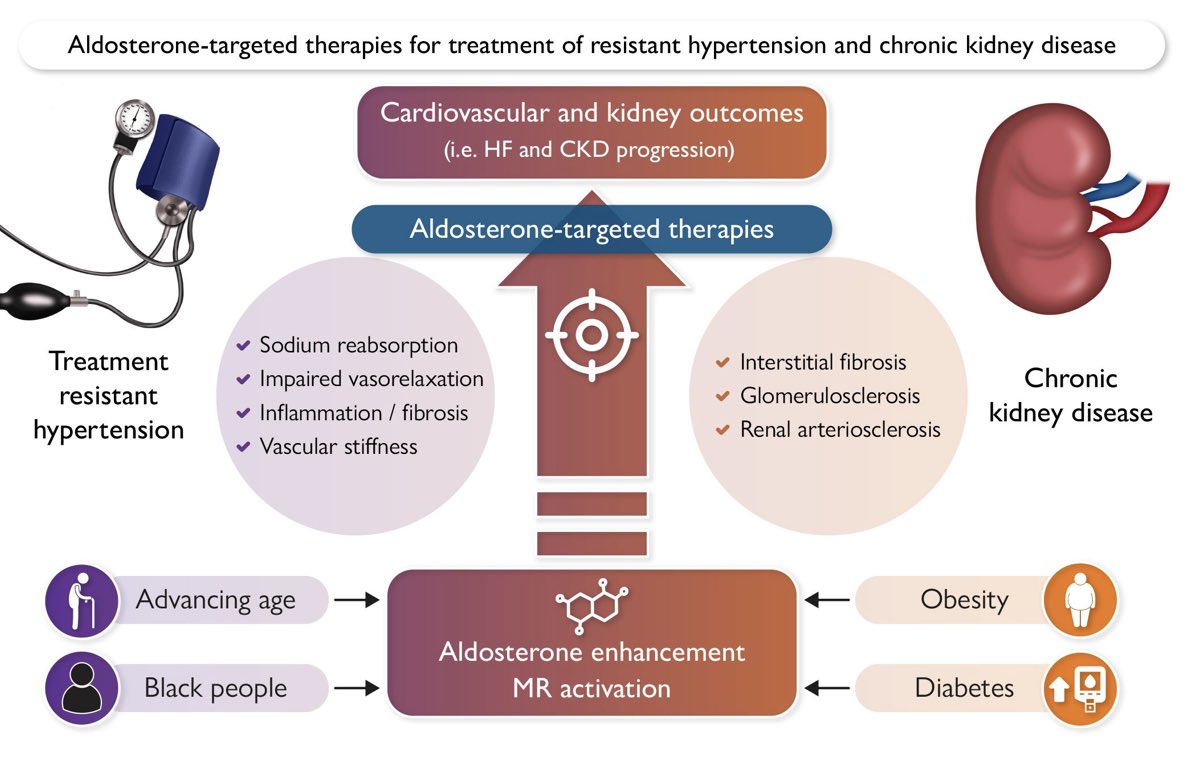
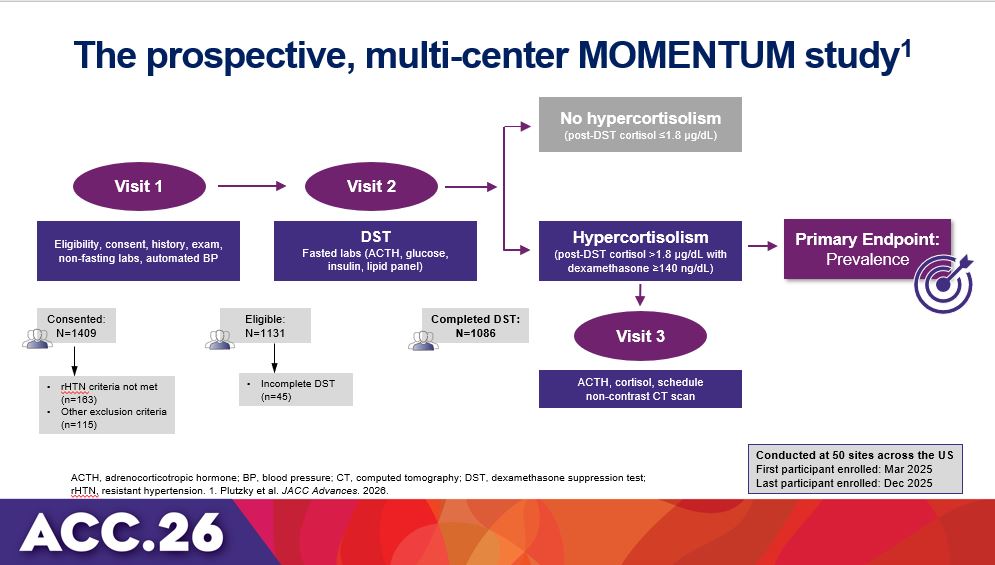
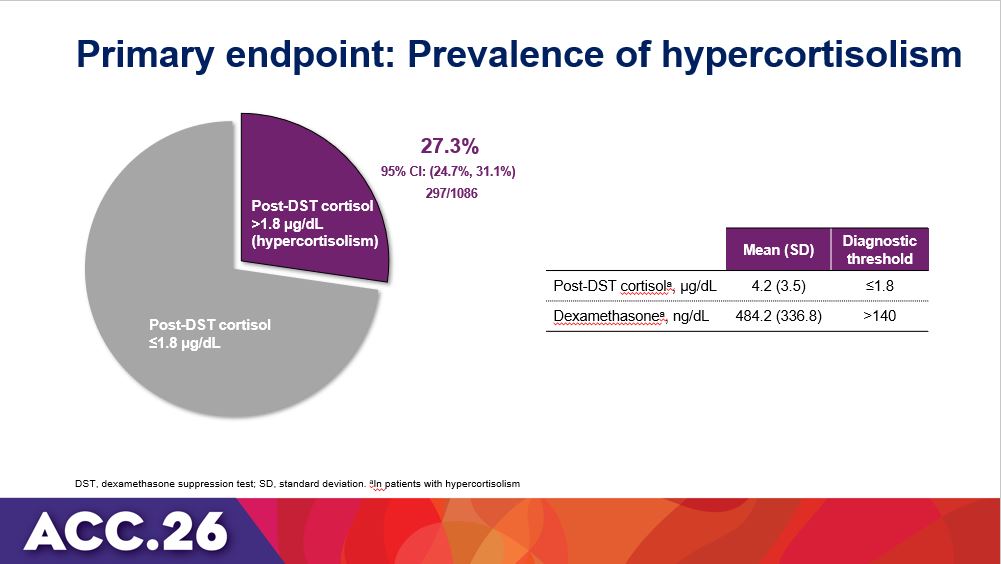
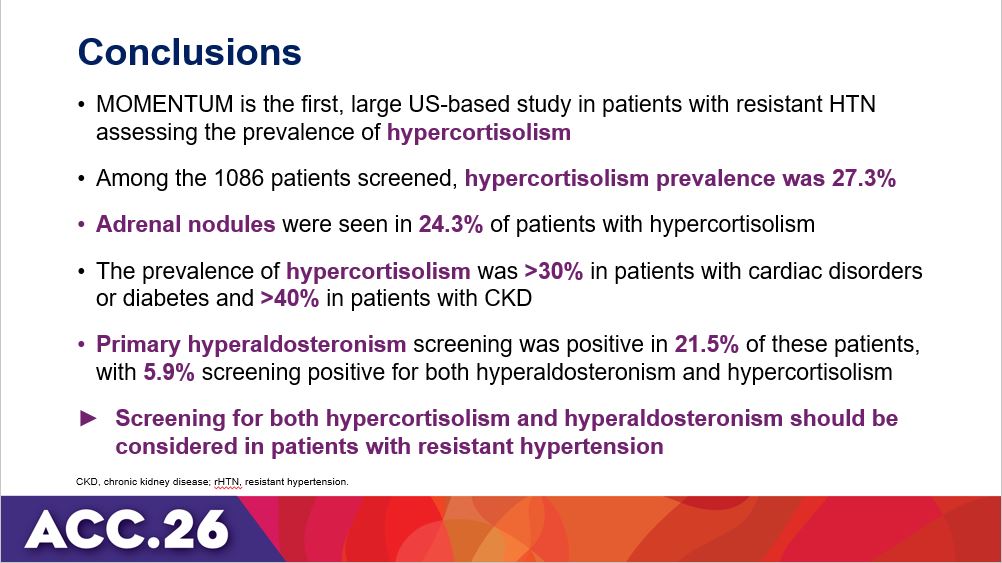
MOMENTUM study revealed high prevalence of hypercortisolism & hyperaldosteronism in U.S. resistant HTN patients, suggesting the importance of screening for both. #ACC26 View Slides Here: clinicaltrialresults.org/wp-…

2
47
123
18,379
Dr Rob 🫀🩺 🇦🇺 retweeted
Mar 14
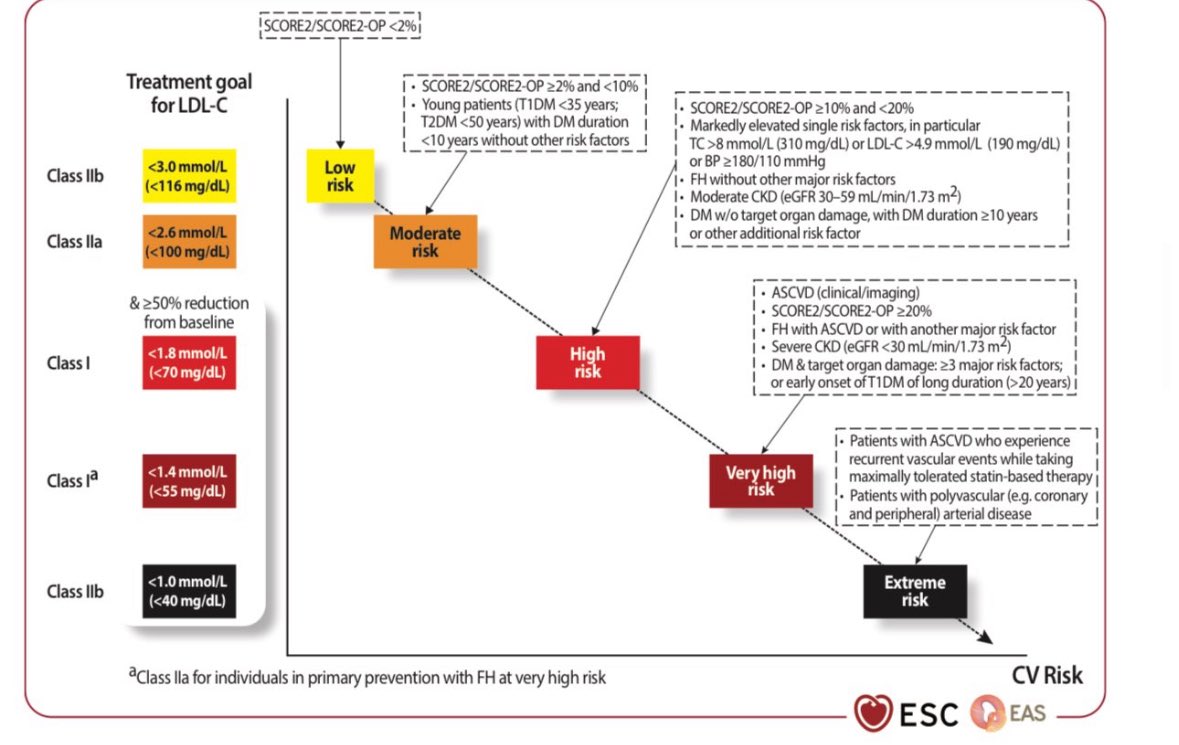
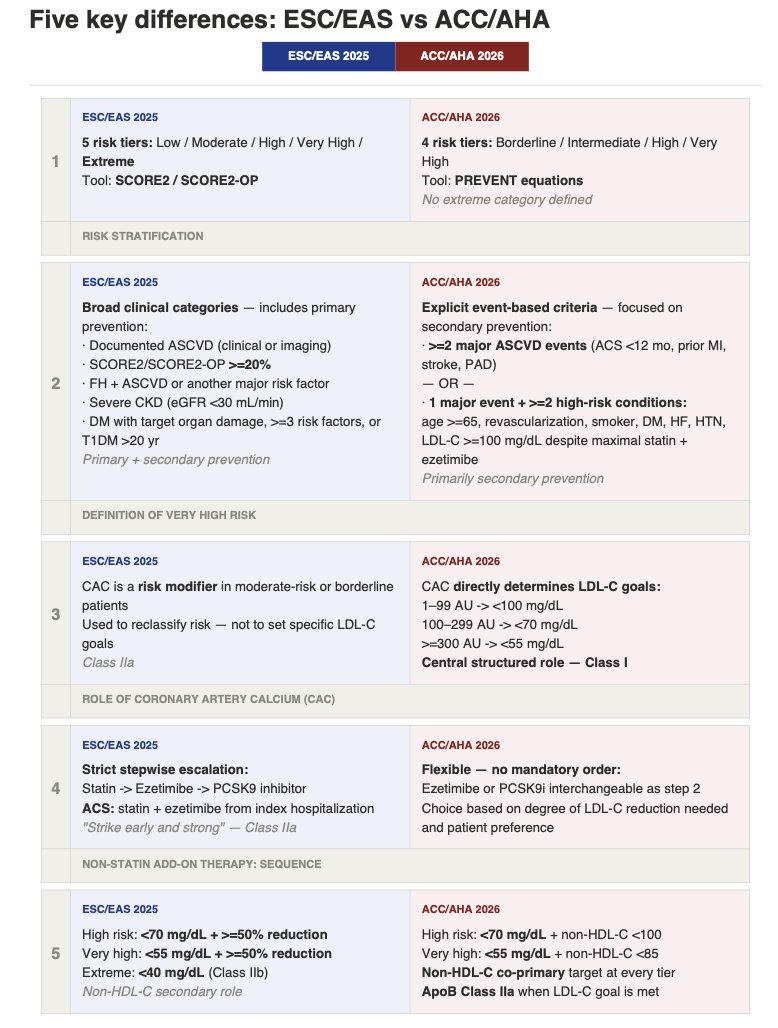
🇪🇺ESC/EAS (2025) vs 🇺🇲ACC/AHA (2026):
👉 Where They Differ—and Where They Converge
1️⃣ Risk stratification
2️⃣ Definition of very high risk
3️⃣ Role of coronary artery calcium (CAC)
4️⃣ Non-statin add-on therapy
5️⃣ LDL-C treatment goals
@society_eas
@escardio
@LipidJournal
@ATHjournal
@ACCinTouch
@American_Heart
8
75
216
12,599
Dr Rob 🫀🩺 🇦🇺 retweeted
Feb 23
🤔“Statins add 4 days”
❌No
💔They prevent heart attacks for decades
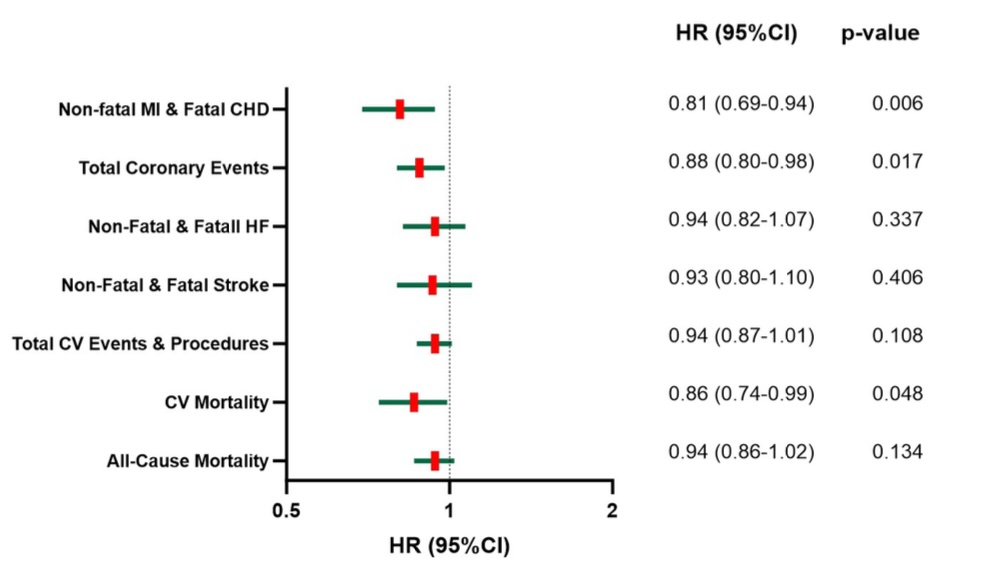
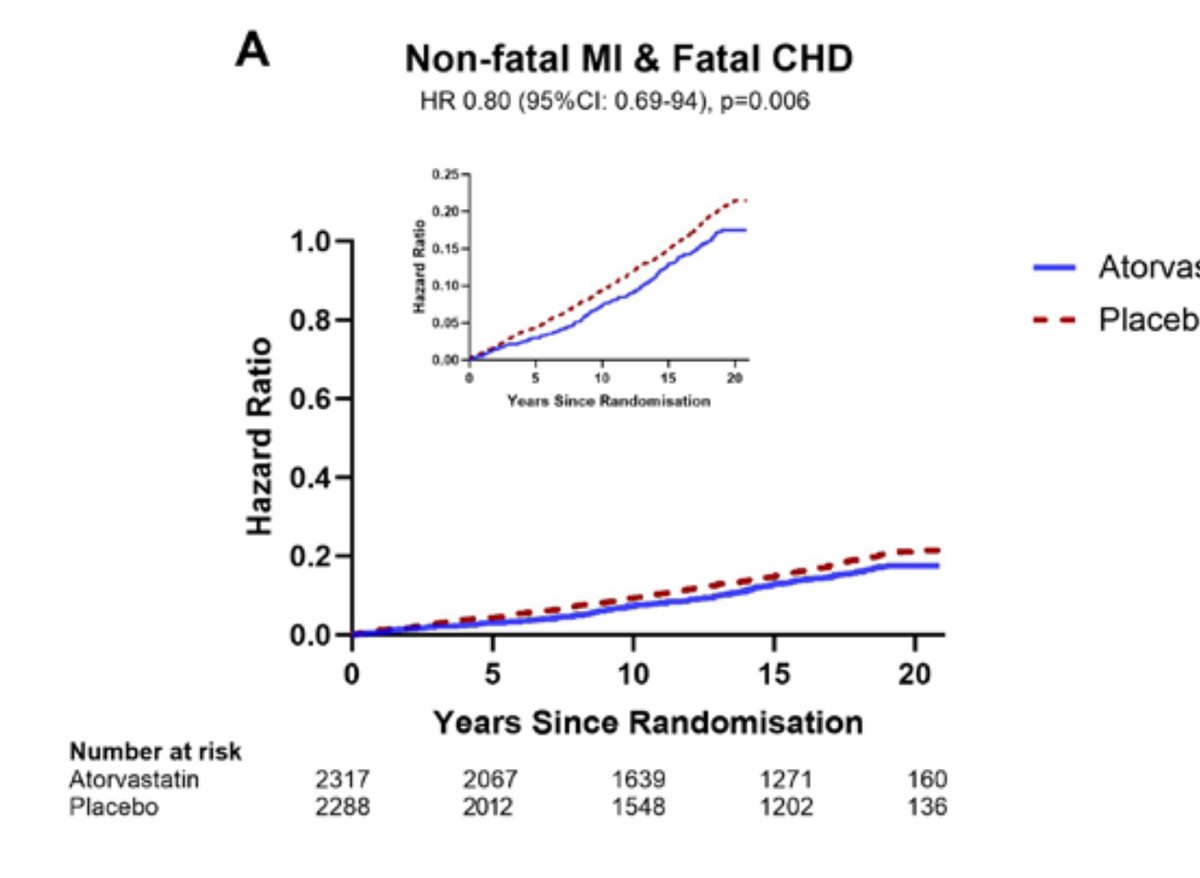
👉ASCOT-Legacy, 20-year follow-up
• ↓ MI fatal CHD: 19%
• ↓ Total coronary events: 12%
• ↓ CV mortality: 14%
👆And the lower the achieved LDL during the trial, the lower the long-term risk:
Every 1 mmol/L LDL reduction →
31% less MI/CHD
34% less CV death
👉The original RCT lasted 3.3 years
👉The benefit persisted 20 years
📍That’s not “4 days”
📍That’s altering the natural history of atherosclerosis
📍If you truncate survival curves at 4 years, you’ll measure days
📍If you follow patients for decades, you’ll measure prevented infarctions and lives saved
🔗Open Access heart.bmj.com/content/111/16…
@society_eas
@mmamas1973
@DrMarthaGulati
@Drlipid
@ethanjweiss
@purviparwani
@BarteltLab
23
72
236
32,214
Dr Rob 🫀🩺 🇦🇺 retweeted
Jan 26
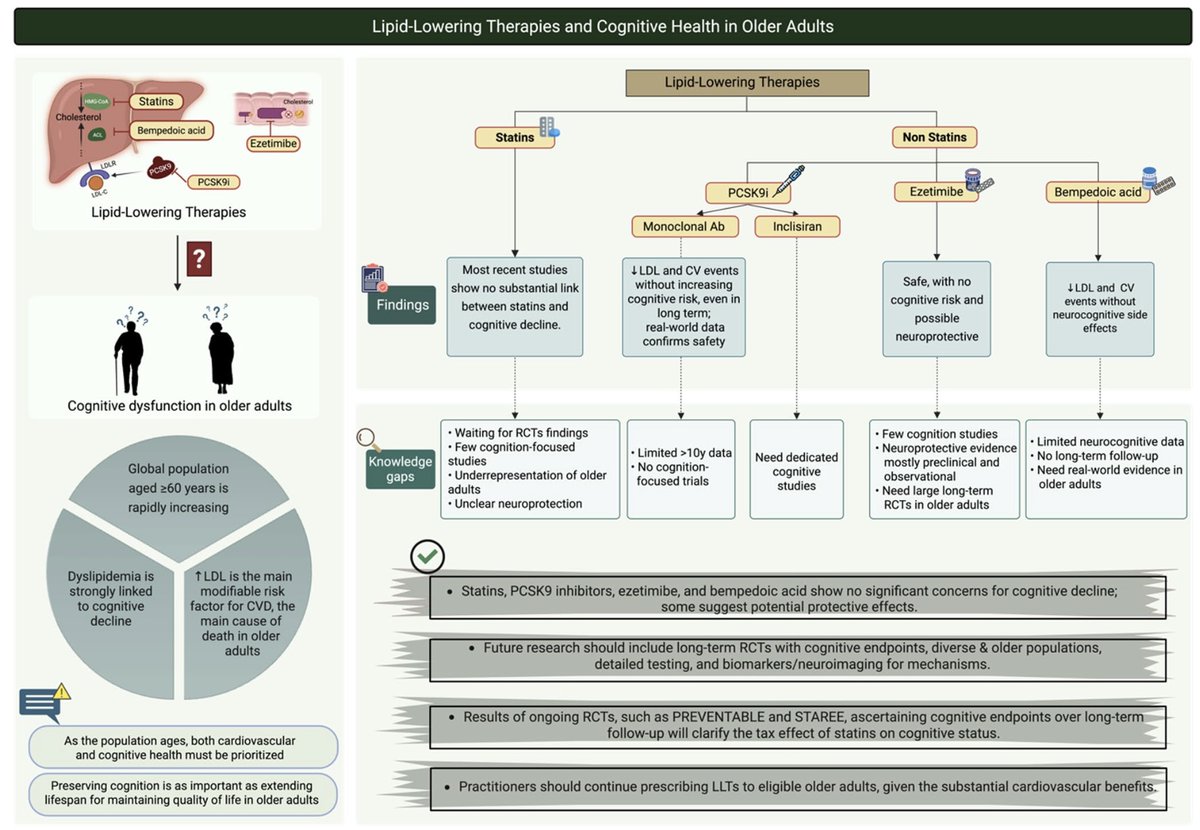
👉 Lipid-Lowering Therapy and Cognition: Evidence vs Myth
1️⃣ Elevated LDL-C remains the leading modifiable risk factor for cardiovascular disease and a major contributor to global mortality.
2️⃣ Concerns about cognitive adverse effects of lipid-lowering therapies (LLTs), particularly statins, are largely driven by early case reports rather than robust clinical evidence.
3️⃣ Observational studies and randomized trials consistently show no significant association between statin use and cognitive decline, with some data suggesting potential protective effects against dementia.
4️⃣ Major randomized trials (HPS, PROSPER, HOPE-3) found no difference in cognitive outcomes between statin-treated and placebo groups.
5️⃣ PCSK9 inhibitors (evolocumab, alirocumab) demonstrate neurocognitive safety, even with very low LDL-C levels and long-term exposure.
6️⃣ Ezetimibe and bempedoic acid show neutral neurocognitive profiles, with emerging signals of possible neuroprotective effects.
📍 Current data support a clear conclusion:
👆 Lowering LDL-C improves cardiovascular outcomes without meaningful cognitive harm.
👆 The real knowledge gap is not safety, but understanding whether lipid-lowering therapies might also confer long-term neuroprotection.
📍 Take-home message:
Fear of cognitive decline should not justify therapeutic inertia. The price of untreated LDL-C is cardiovascular disease—not cognitive impairment.
🔗 link.springer.com/article/10…
2
25
117
5,571

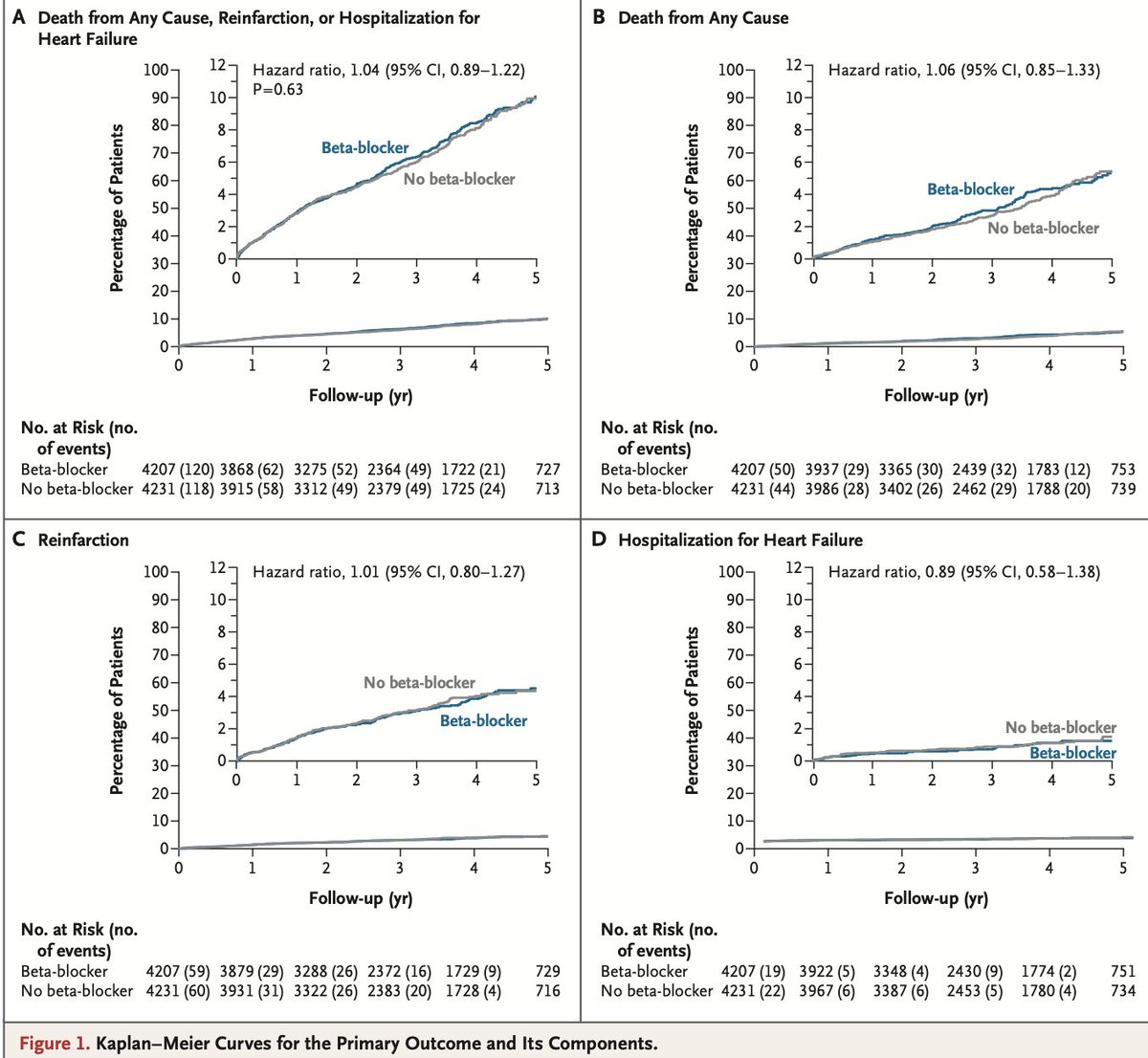
Presented at #AHA25:
In a meta-analysis of 17,801 patients with myocardial infarction and preserved LVEF (≥50%), beta-blockers did not reduce death, MI, or heart failure over a median 3.6 years of follow-up. Full results: nej.md/43U5Ppo
@AHAScience
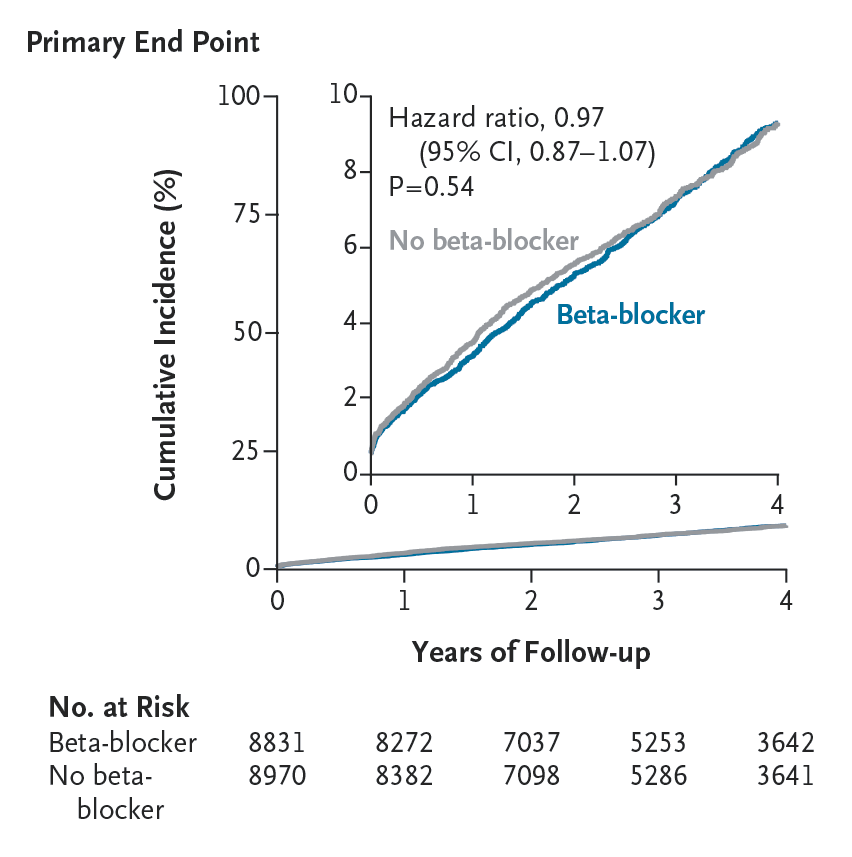
ALT Kaplan–Meier curves of the cumulative incidence of death from any cause, myocardial infarction, or heart failure (the composite primary end point).
7
231
571
98,730
Dr Rob 🫀🩺 🇦🇺 retweeted

9 Nov 2025
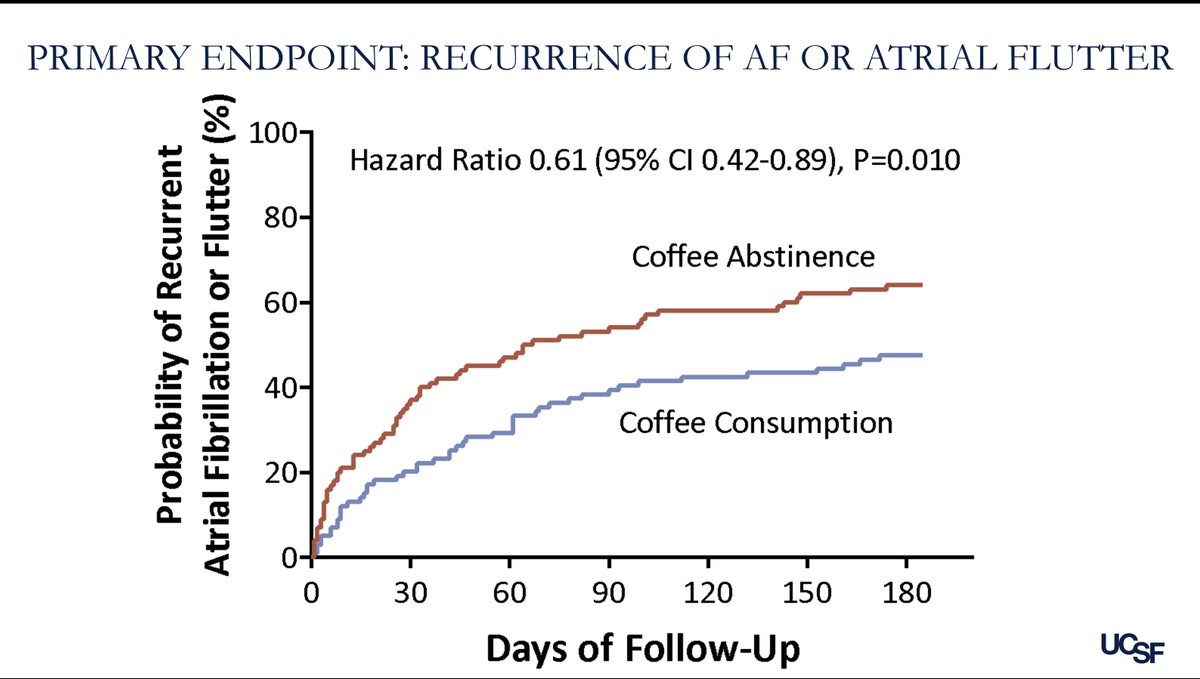
DECAF trial: continued consumption of caffeinated coffee was associated with a 39% lower risk of AF/AFL recurrence at 6 months after cardioversion vs. abstinence from coffee. View the slides here: clinicaltrialresults.org/wp-…

16
85
311
317,786
9 Nov 2025
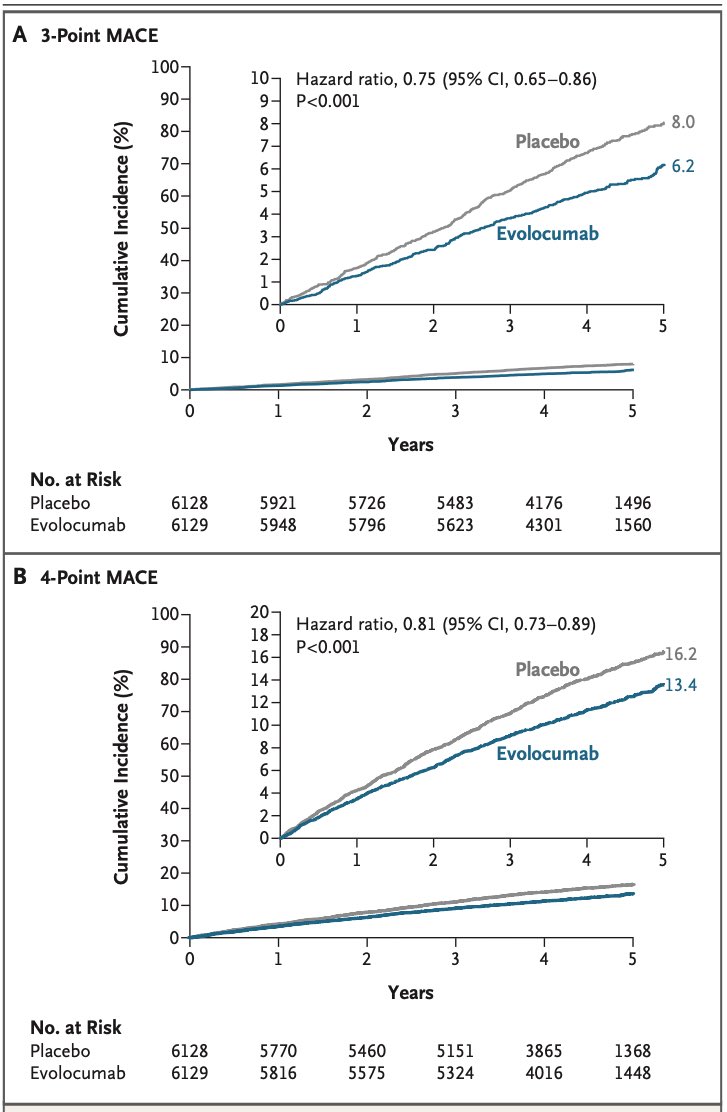
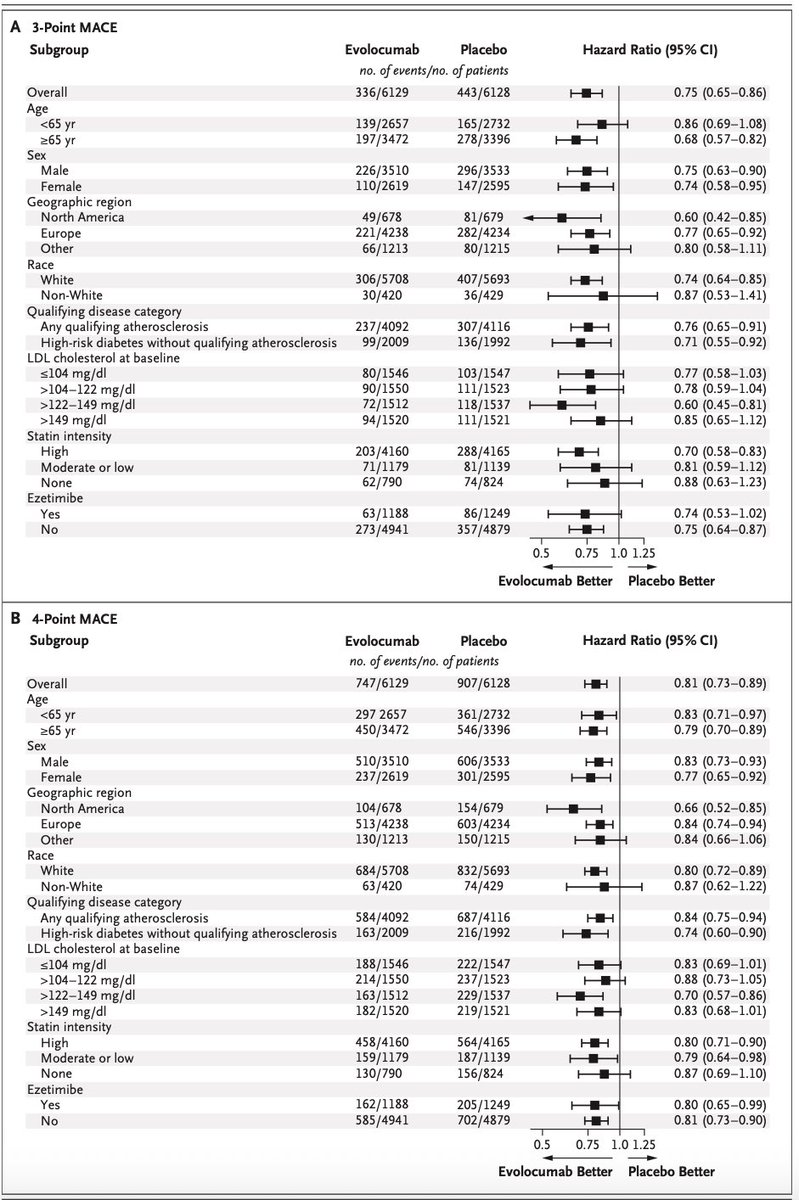
VESALIUS-CV: Expanding the reach of PCSK9 inhibition!
In >12,000 pts without prior MI or stroke but with ASCVD or diabetes, evolocumab (140 mg q2w) cut major CV events vs placebo over 4.6 yrs.
🩸 3-point MACE: 6.2% vs 8.0% → HR 0.75 (95% CI 0.65–0.86)
🫀 4-point MACE: 13.4% vs 16.2% → HR 0.81 (95% CI 0.73–0.89)
🎯 Benefit without new safety concerns.
✅ Take-home: PCSK9 inhibition isn’t just for secondary prevention.
Evolocumab prevented first CV events in high-risk patients - redefining “primary prevention” in the atherosclerotic era.
#MedED #FOAMed #Cardiotwitter #Medtwitter
@ehj_ed @ACCinTouch @JACCJournals @escardio @society_eas @ATHjournal
1
4
391
Dr Rob 🫀🩺 🇦🇺 retweeted

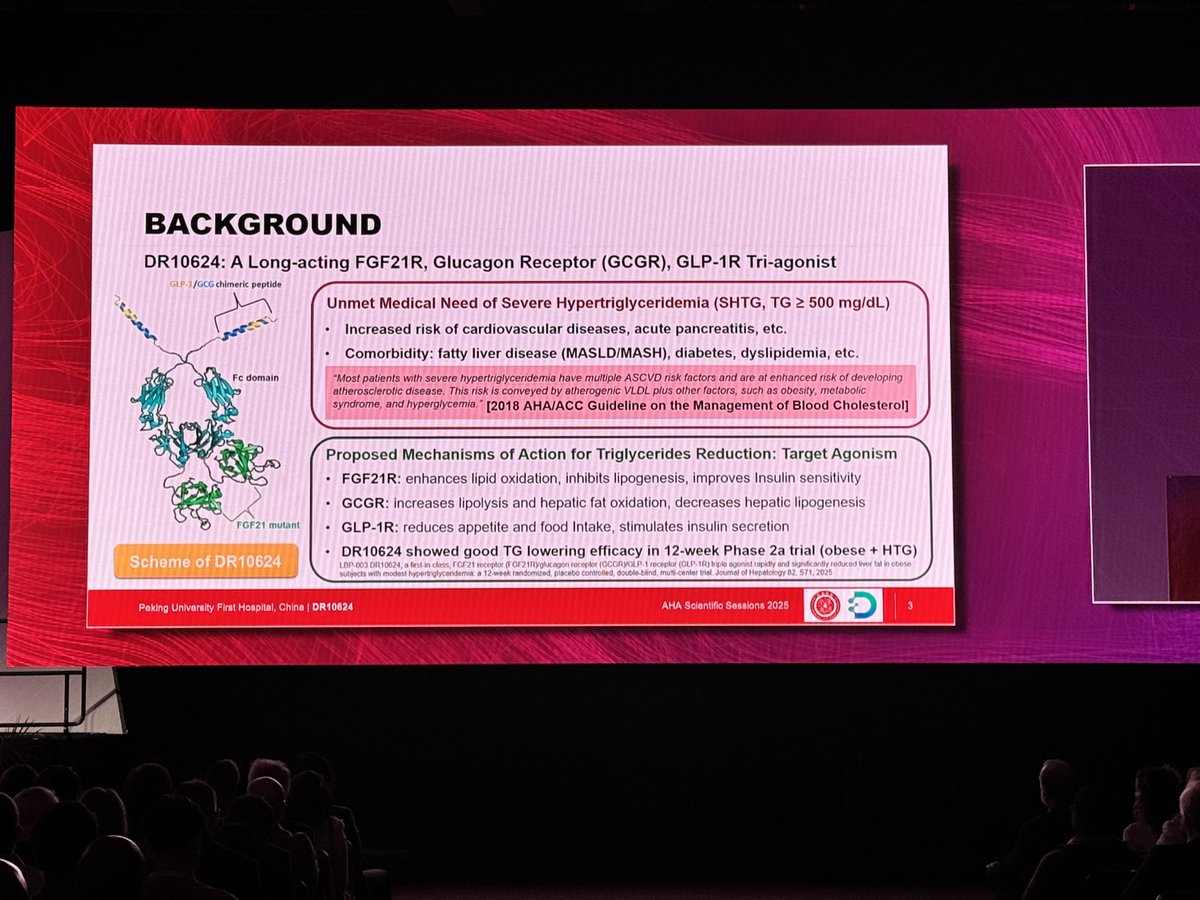
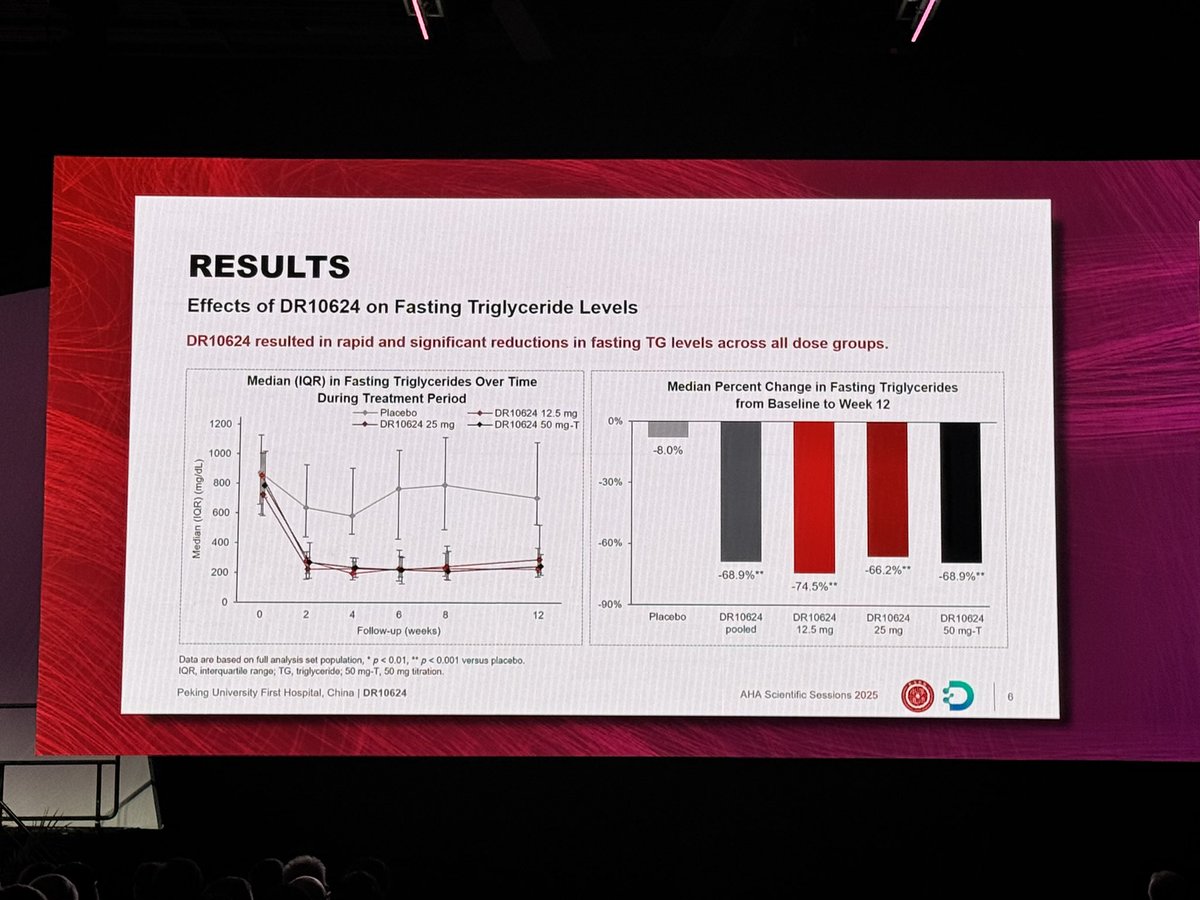
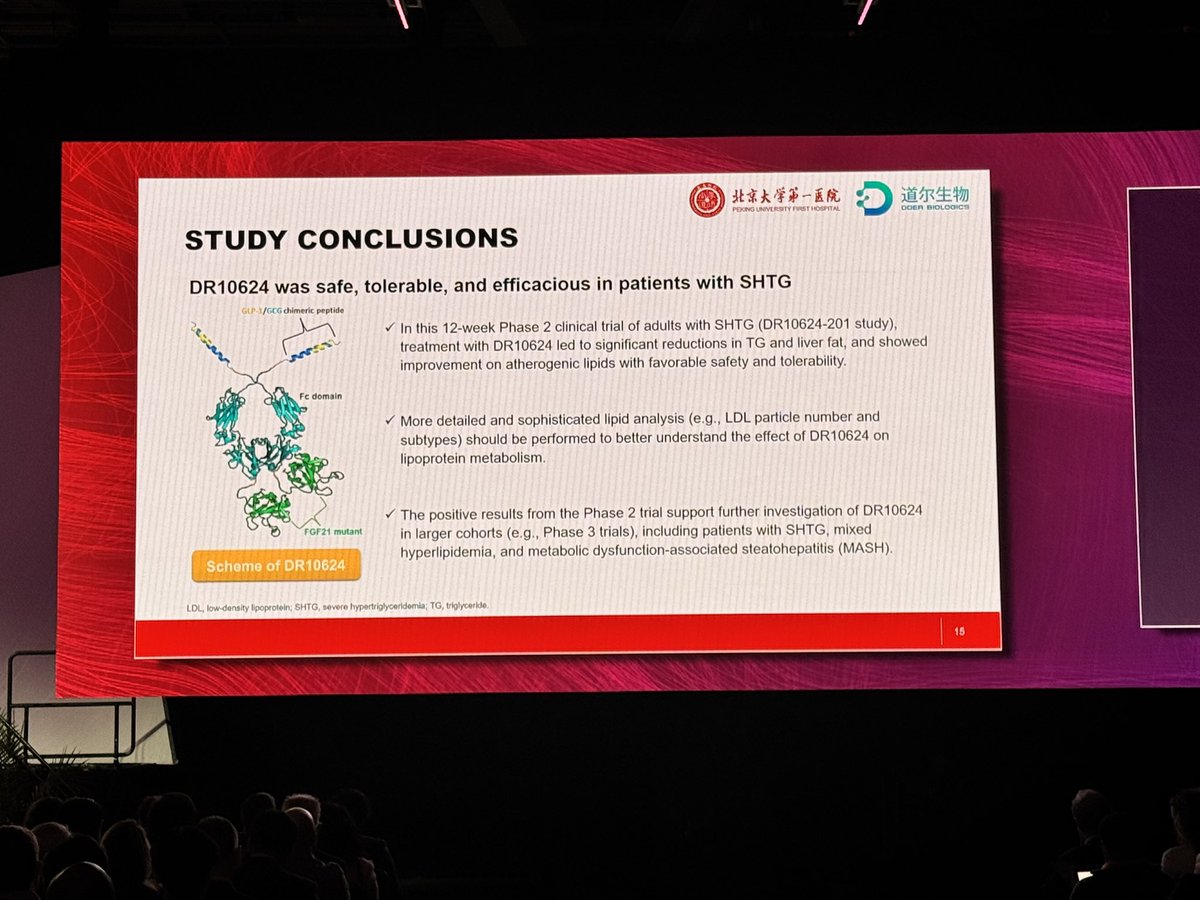
8 Nov 2025
First in Class triple agonist targeting FGF21 triple glucagonreceptor, GLP1R TG, Lipids & liver fat:
Phase 2, 12 week trial
♥️ 1/2 women enrolled
📍Primary endpoint: change in TG: reduced in all groups
📍⤵️ Non HDL and TChol
📍⤵️ Liver fat content: <5%
📍⤴️ insulin sensitivity
📍 Safe, tolerable Phase 2 trial
✨Metabolic improvements!
#AHA25 #CVprev #LBCT #Cardiotwitter

2
23
108
7,545
Dr Rob 🫀🩺 🇦🇺 retweeted

21 Oct 2025
New Residual Risk Score!
Now you can calculate almost immediately the 10-year risk of your patient who has prior ASCVD
The risk calculator is free online & outperforms existing risk assessment algorithms:
jacc.org/doi/abs/10.1016/j.j…

14 Oct 2025

In a new study, researchers from @BrighamWomens and colleagues developed a personalized model to predict risk of subsequent cardiovascular events. The study is published in @JACCJournals.
Read more: massgeneralbrigham.org/en/ab… @SamiaMoraMD
4
61
173
23,832
Dr Rob 🫀🩺 🇦🇺 retweeted

8 Oct 2025
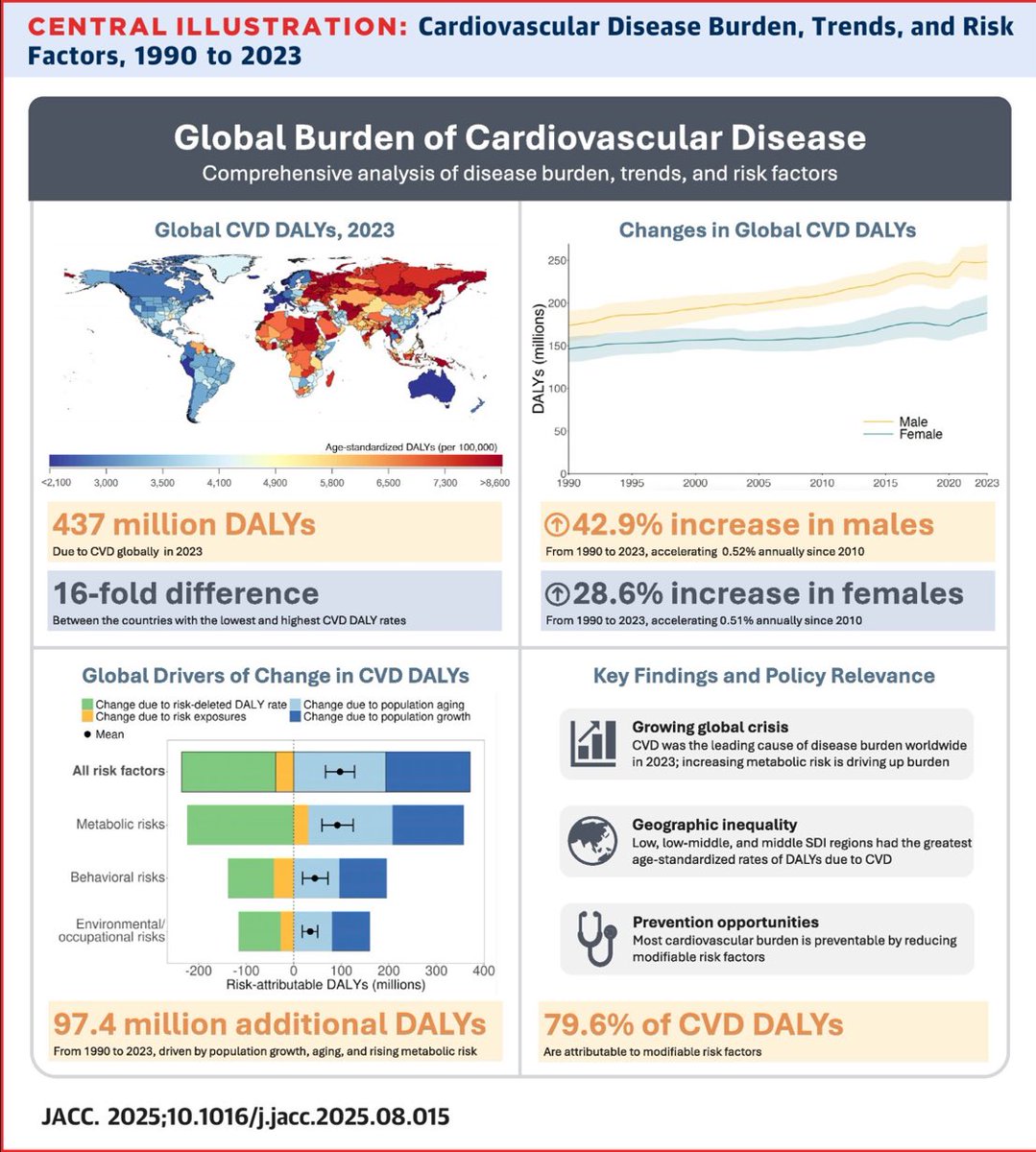
Most Updated Global Burden of Cardiovascular Disease now out in @JACCJournals
80% (!) of CV disease burden is attributable to modifiable RFs
Top modifiable risks in 2023:
⚠️ High systolic BP
⚠️ Dietary risks
⚠️ High LDL cholesterol
⚠️ Air pollution
🔗 jacc.org/doi/10.1016/j.jacc.…
3
63
155
10,639
Dr Rob 🫀🩺 🇦🇺 retweeted

2 Oct 2025

1
72
240
15,993
16 Sep 2025
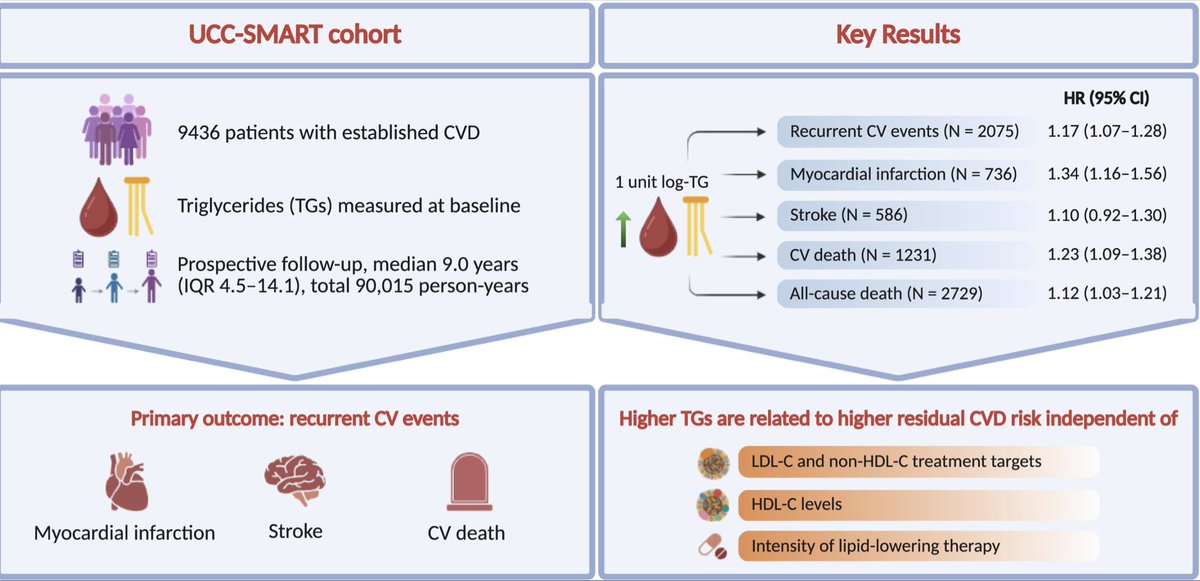
🔺 Triglycerides: The Hidden Residual Risk in CVD 🫀💥
📊 In 9,436 pts with established CVD (9y FU), elevated TGs = ↑ recurrent events, CV death & mortality.
⚠️ TG risk persisted despite reaching LDL-C/non-HDL-C targets & across LLT intensity.
👉 TRLs are key drivers of residual risk - lifestyle & new TG-targeted therapies needed.
#MedED #FOAMed #Cardiotwitter #Medtwitter
@escardio @society_eas @ATHjournal
1
2
6
412
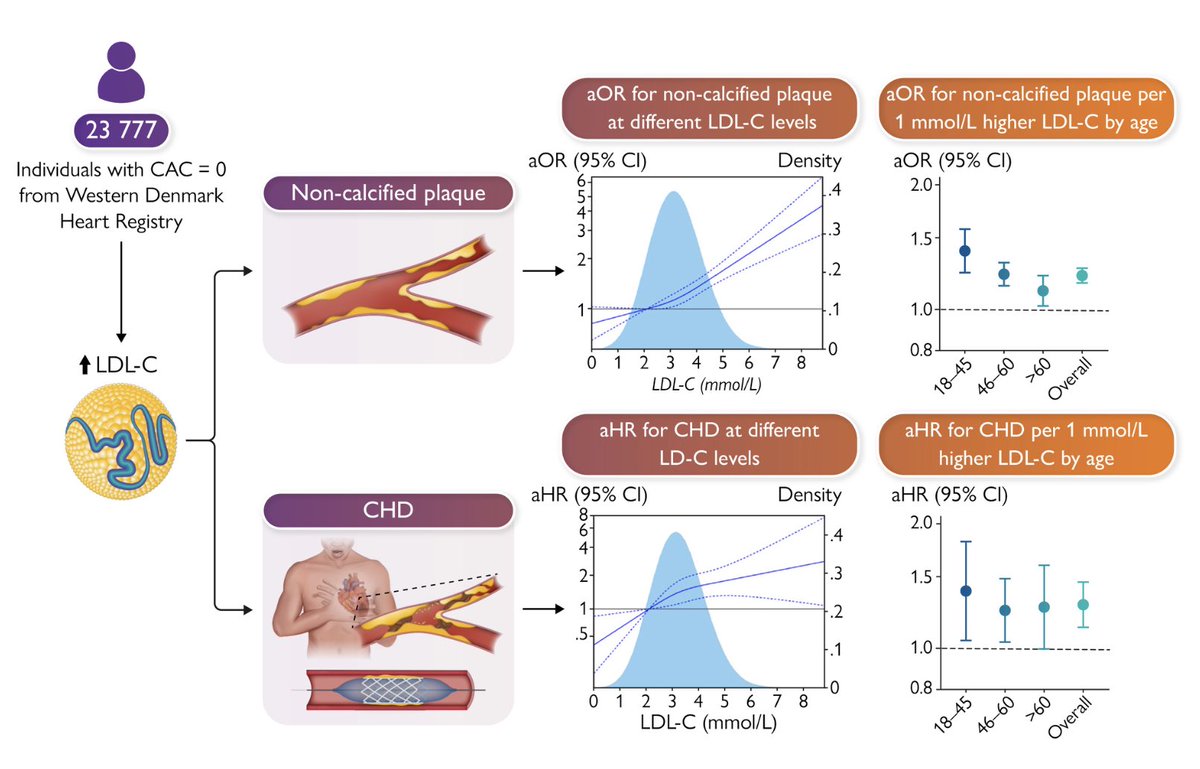
13 Sep 2025
🧬🫀 The CARDIA study
Shows that cumulative exposure to apoB & LDL particles in young adults strongly predicts later ASCVD.
👉 No “safe” LDL threshold identified - risk keeps falling the lower & longer LDL/apoB is controlled.
Early prevention = lifelong protection.
🔗 academic.oup.com/eurheartj/a…
#MedED #FOAMed #Cardiotwitter #Medtwitter
@ehj_ed @escardio
2
5
23
1,363
11 Sep 2025
🧬🫀 Adipose tissue isn’t just bystander 👉🏼 it’s a driver of atherosclerosis.
🔥 Perivascular adipose tissue (PVAT) dysfunction fuels endothelial injury, inflammation & plaques.
💊 Targeting adipose health (e.g. SGLT2i, PPARγ) gives CV benefits beyond glucose/lipid control.
📊 Risk models must include adipose phenotyping → precision CV care.
#MedED #FOAMed #Cardiotwitter #Medtwitter
@escardio @society_eas @ATHjournal

2
187
11 Sep 2025
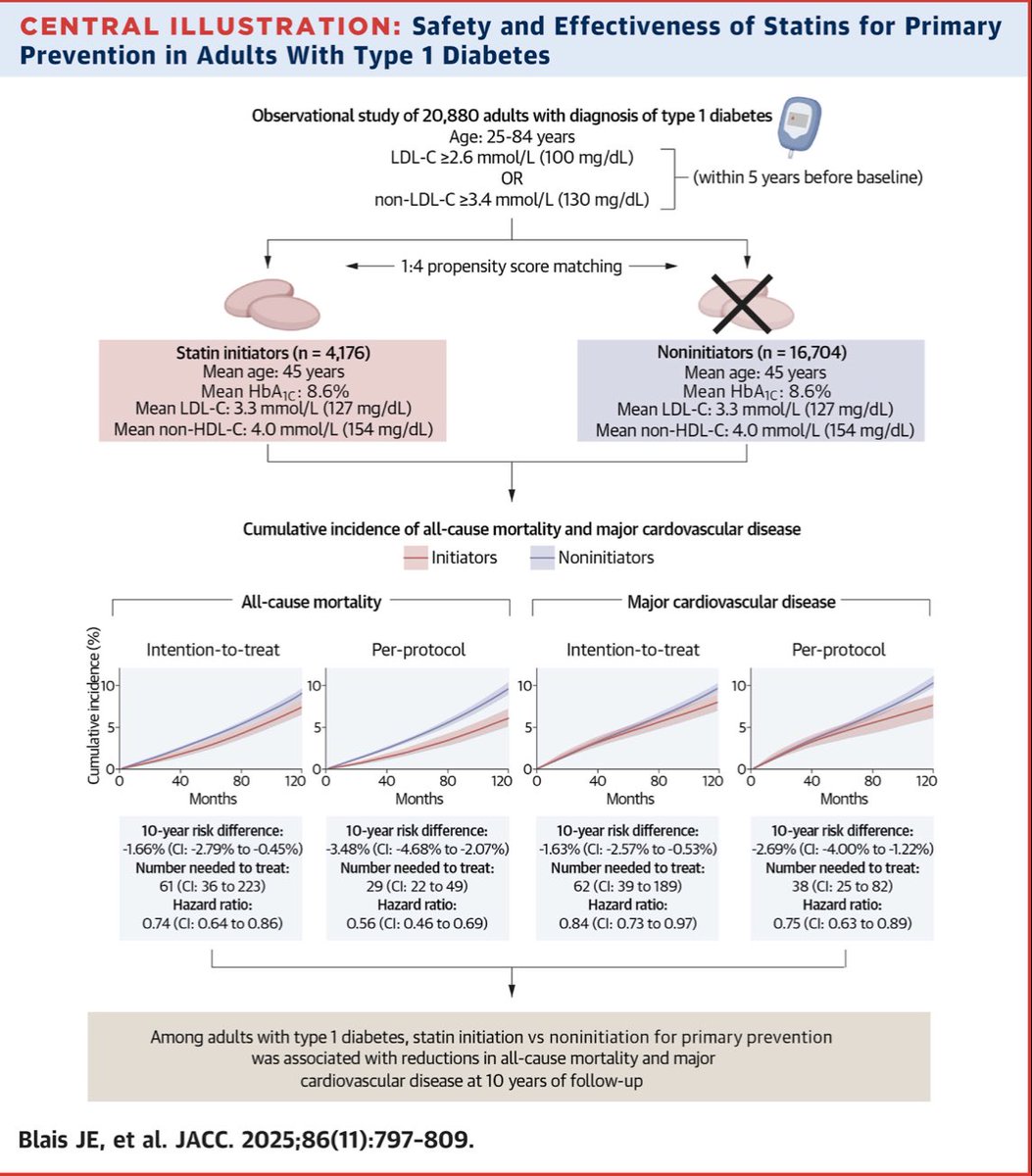
🧑⚕️💊 New evidence in type 1 diabetes - an emulation study
Statin initiation was linked to lower 10-yr all-cause mortality & major CVD in >20k UK adults 🇬🇧
✅ Benefits strongest in women, ≥40y, high LDL-C, higher CV risk
⚠️ Very low adverse effects (slight ↑ liver dysfunction, no ↑ myopathy)
🔗 jacc.org/doi/10.1016/j.jacc.…
#MedED #FOAMed #Cardiotwitter #MedTwitter @ACCinTouch @JACCJournals
1
5
316
Dr Rob 🫀🩺 🇦🇺 retweeted

31 Aug 2025
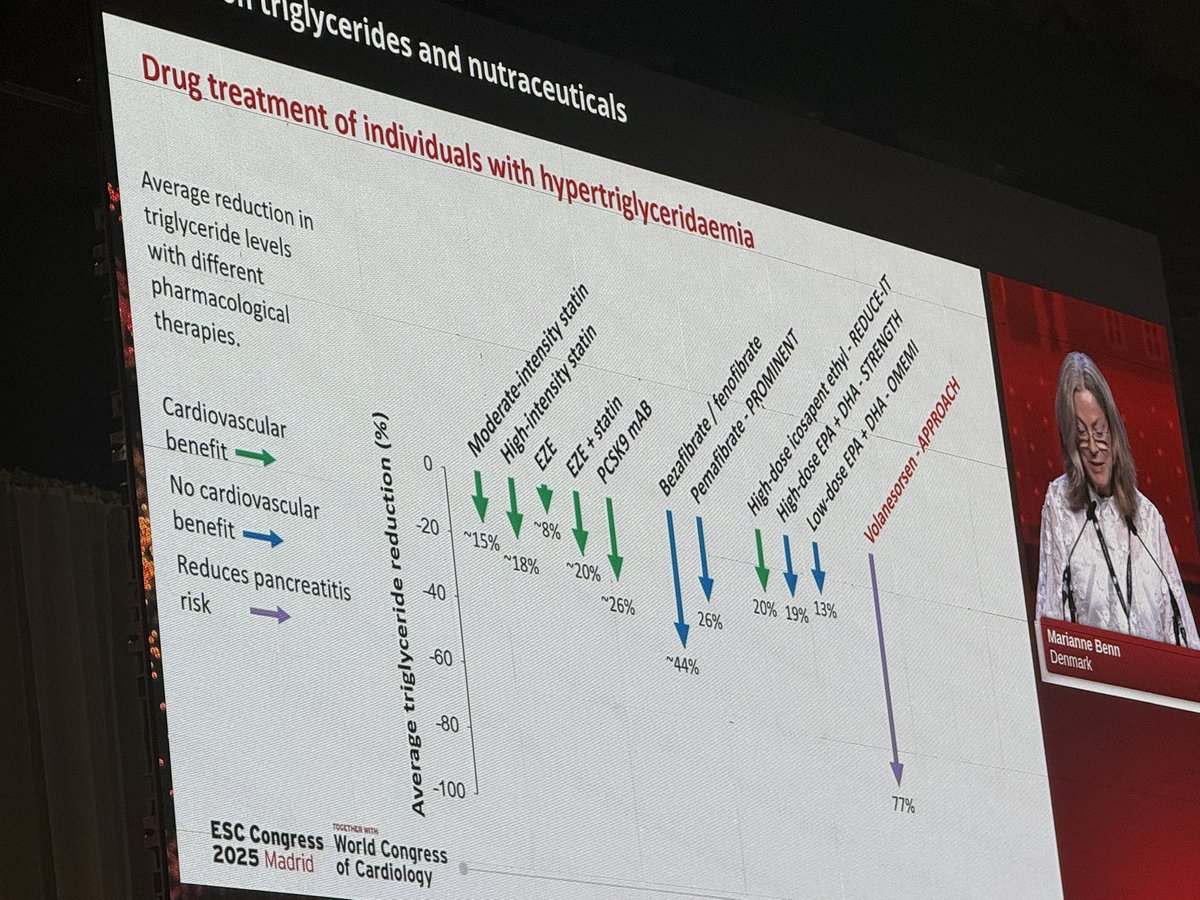
Some great slides from #Guidelines discussion on triglycerides reduction.
Check them out.
📉 Not all TG-lowering therapies equal CV benefit.
•Statins: ↓TG 15–26% ✅ CV benefit
•Fibrates: ↓TG ~26% ❌ no clear CV benefit
•High-dose icosapent ethyl (EPA): ↓TG 20% ✅ CV benefit (REDUCE-IT)
•Volanesorsen: ↓TG 77% ✅ pancreatitis risk reduction
#ESCCongress #Lipidology #CardioTwitter

4
74
285
26,682
Dr Rob 🫀🩺 🇦🇺 retweeted

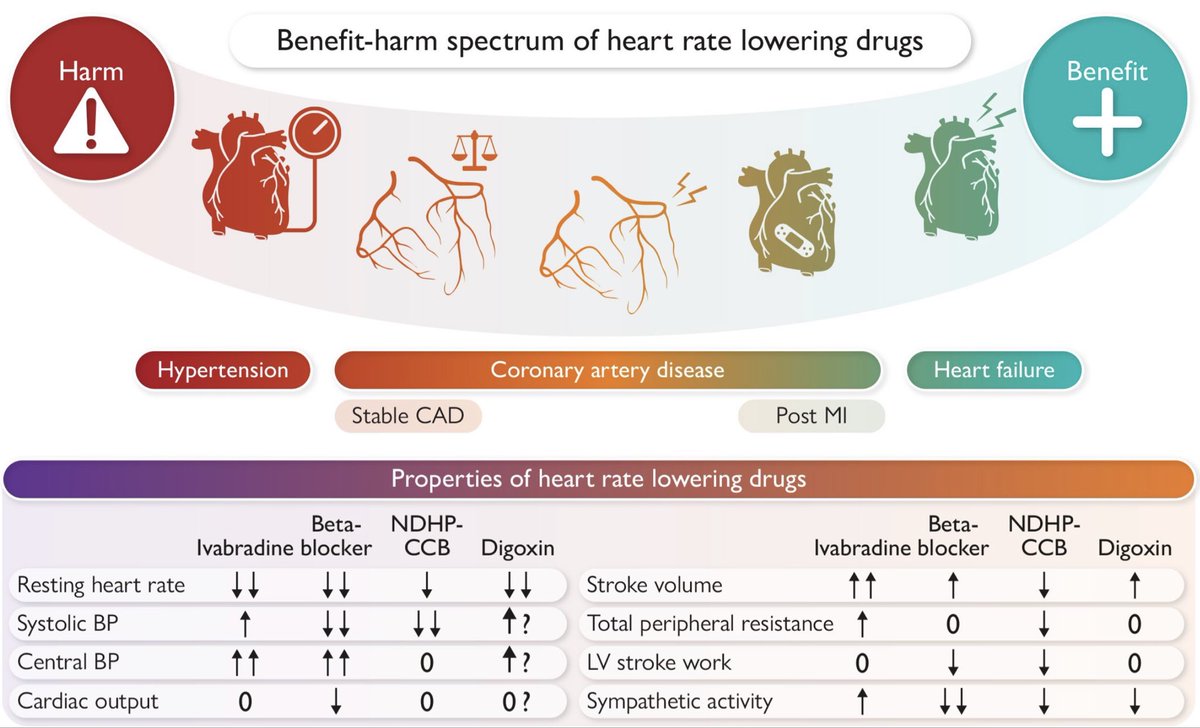
30 Aug 2025
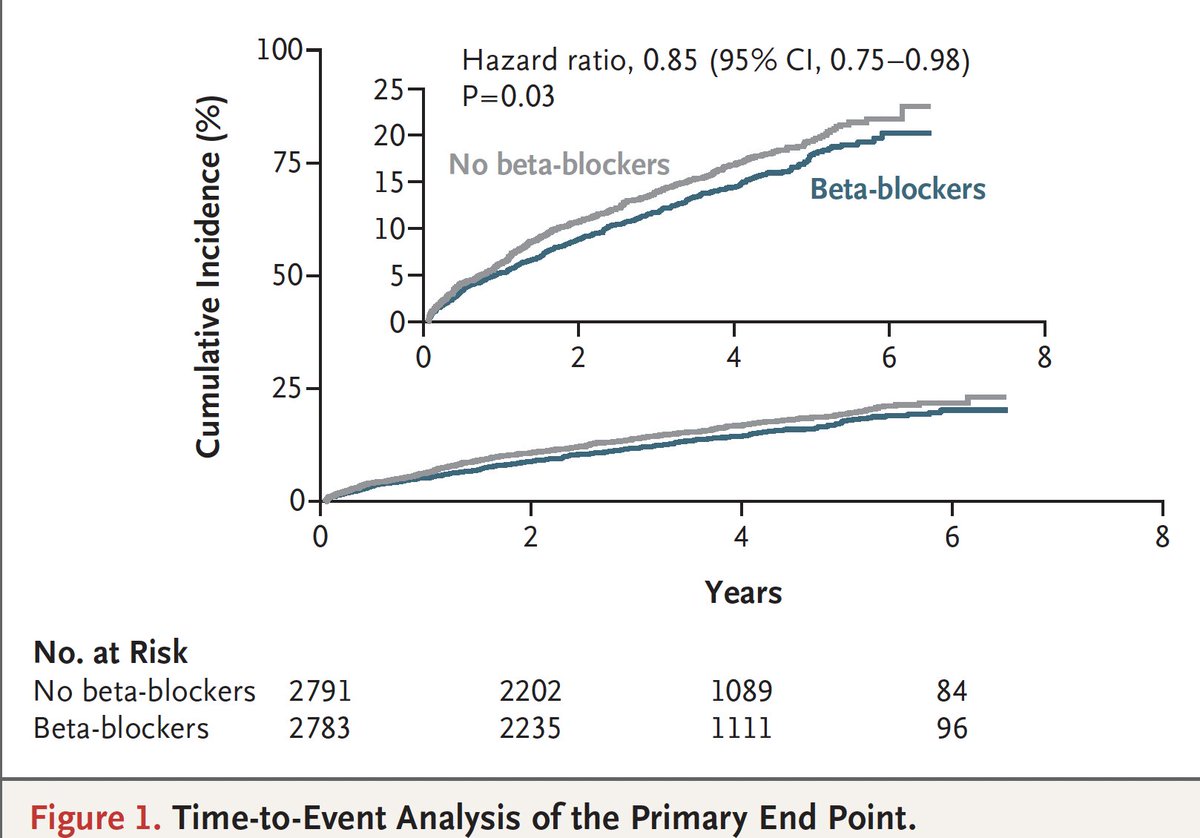
Beta blockers were routinely given to patients after a heart attack. 2 new randomized trials show conflicting results for patients with an ejection fraction of >40% #ESC2025 @NEJM
nejm.org/doi/full/10.1056/NE…
nejm.org/doi/full/10.1056/NE…
9
70
287
48,597