
0G Accelerator | Building the Verification Layer for Scientific Intelligence🔬
Joined June 2025
- Tweets 295
- Following 39
- Followers 154
- Likes 597
45 Photos and videos









Mar 4
cool!

We've been quiet. Here's why — and what we've been building. A thread on rebuilding the social contract of science. 🧵
aurasci.xyz
30
Genosight retweeted

Claude down, 0G Compute is running

GLM-5 is live on 0G Compute.
744B parameters. SOTA open-source. MIT license.
Beats GPT-5.2 on BrowseComp and Terminal-Bench.
Run the world's best open model on decentralized infrastructure. No cloud vendor. No data logging. No ToS surprises.
Your prompts stay yours.
18
31
139
62,251
Genosight retweeted

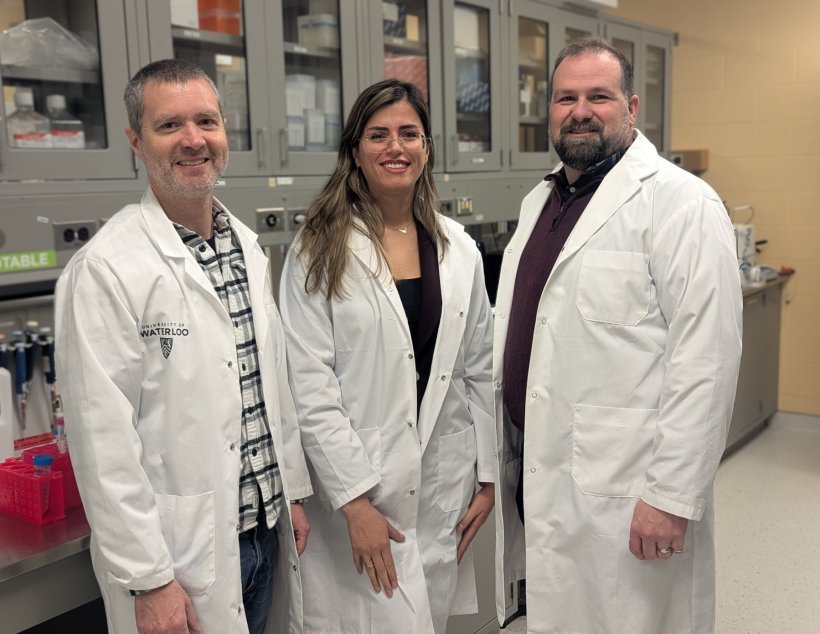
BREAKING🚨: Scientists from the University of Waterloo have engineered bacteria that eats tumers and cancer cells from inside out
67
294
2,413
60,196
Genosight retweeted

Feb 26
wow, amazing discovery
we're learning so much about aging lately
LEV is very near
Massive Cell by Cell Aging Atlas Reveals Aging Is a Coordinated, Body Wide Process
Scientists have created the most comprehensive map yet of how aging changes cells across the entire body by profiling nearly 7 million individual cells from 21 different tissues in mice.
The study shows that aging doesn’t just randomly degrade cells, many cell types change in number and activity in coordinated ways across organs, with substantial differences between males and females.
About a quarter of cell types undergo major population shifts with age, and shared genomic regions linked to immune activity and inflammation emerge as common hotspots of aging.
These findings suggest aging is a dynamic, regulated process rather than random decay, and pinpoint specific cell types and molecular signals that could be targeted in future interventions.

29
55
407
19,375
Genosight retweeted
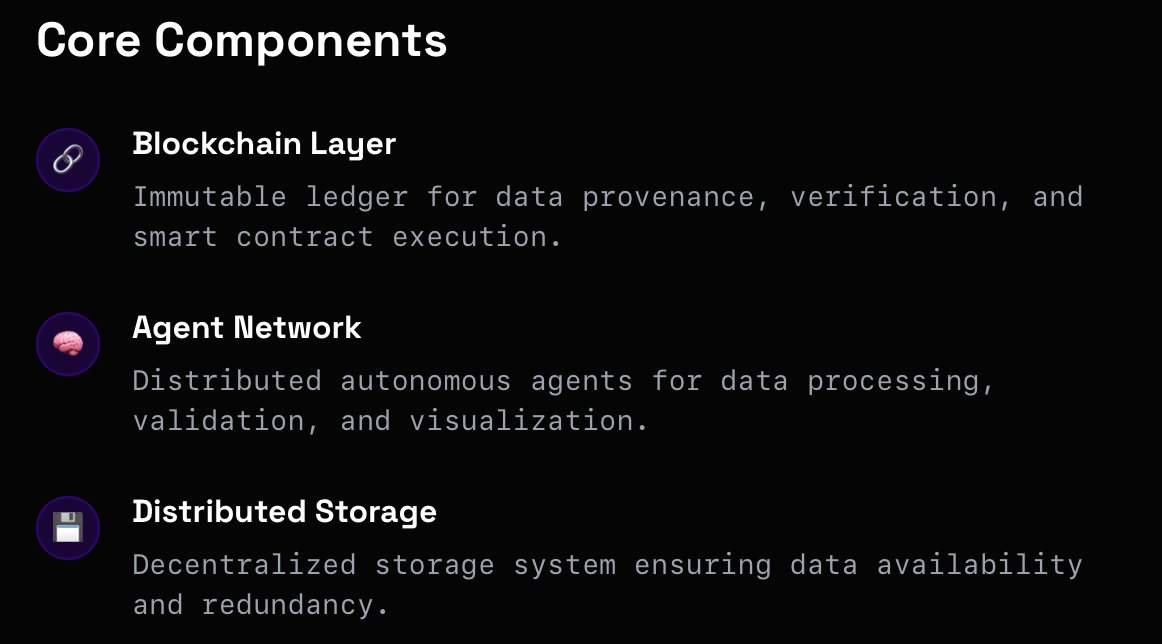
Verification isn't a feature. It's the foundation.
@michaelh_0g is making the case that AI without built-in verification isn't just risky, it's incomplete.
Catch his talk "Why Verification Should be a 1st Class Citizen in AI" at the AI Agents & Automation track @EthCC.

What if the biggest risk in AI isn't the models themselves, but our blind trust in their outputs? Michael Heinrich (@michaelh_0g) tackles this critical gap in "Why Verification Should be a 1st Class Citizen in AI" at the AI Agents and Automation track.
Building verification into AI systems from day one isn't just good practice, it's the difference between deployment and disaster.

20
21
92
56,290
Genosight retweeted

Feb 25
Claude almost killed our AI Developer.
Not literally.
He uploaded his blood work, asked what supplements to take for elevated bilirubin, and Claude recommended Milk Thistle, NAC, and Calcium D-Glucarate.
For his condition, that stack could have made things worse.
Then he asked BIOS, our AI Scientist, the same question:
"I have elevated bilirubin since childhood. I train 5 times a week. What supplements can I actually take?"
BIOS got to work.
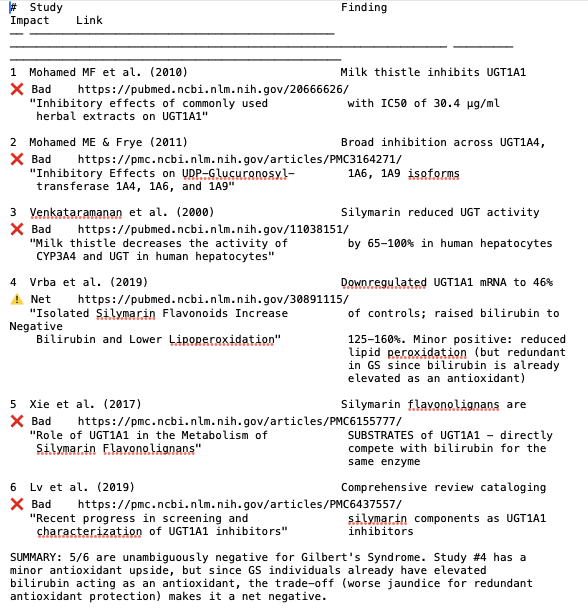
It identified the condition from the lab panel. Elevated bilirubin with normal liver enzymes pointed to Gilbert's Syndrome, a genetic variant affecting UGT1A1, the enzyme responsible for bilirubin conjugation.
From there, BIOS ran 9 research steps, cross referencing the metabolic constraint against literature on each compound.
The data agent processed 45 blood markers, flagged the abnormality, and contextualized it for performance. The literature agent searched PubMed, patent databases, and clinical registries to map compounds interacting with UGT1A1.
What it found would not come from a standard search.
Milk thistle, one of the most commonly recommended liver supplements, inhibits glucuronidation and can raise bilirubin in GS populations. Green tea extract showed an IC50 of 7.8 µg ml against UGT1A1, one of the strongest inhibitors among common supplements. Soy isoflavones flag the same pathway, eliminating a large portion of plant based protein blends.
These are not obscure findings. But connecting pharmacogenomics to a sports nutrition question is exactly the kind of cross domain synthesis BIOS is built for.
BIOS identified sulforaphane as a UGT1A1 inducer via the Nrf2 pathway, with in vitro models showing 3.7 fold enzyme induction, up to 12 fold with apigenin. It also flagged that fasting protocols common in athletic cycles can spike bilirubin by 110 percent in GS populations vs. 60 percent in healthy controls. Consistent caloric intake is not a lifestyle suggestion here.
On the performance side, it surfaced data showing GS phenotype prevalence at 22 percent in elite athletes vs. 9.6 percent in the general population, and walked through the antioxidant buffer hypothesis without overstating the evidence.
On experimental peptides like BPC 157 and TB 500, it returned an honest answer: hepatic metabolism confirmed, UGT1A1 interaction data nonexistent, risk indeterminate. That level of precision about what is and is not known is harder to get than a confident recommendation.
This is the kind of question that gets a generic answer everywhere else. A physician says it is benign. A nutritionist recommends the same stack.
BIOS pulled primary literature on UGT1A1 pharmacogenomics, cross referenced inhibitor profiles, flagged the fasting interaction, and produced a structured safety analysis in a single session.
BIOS session:
chat.bio.xyz/chats/fxSYcu1yZ…
Claude session:
t3.chat/share/clzobz9rk3
This is not medical advice.
Decisions should be made with a qualified professional.
31
37
172
16,365
Genosight retweeted

Feb 25
Biology is technology. Medicine is software, the marginal cost of production is vanishingly small.
The bottleneck was never science. It was coordination. AI agents just solved that. The crabs will save us 🦀
accelerando
23
8
81
3,462
Genosight retweeted
We had a lot of fun at #ETHDenver!
0G AI Accelerator x @StanfordBBF hosted an epic Founders Night, connecting the next generation of AI-native builders with funding, resources, and the 0G ecosystem.
Shoutout to @iotex_io for an electrifying Crypto's Got Talent showcase 🔥
20
17
129
56,241
Feb 24
time to build agent?🤔🤔
Feb 24

A biotech postdoc costs $6K/month.
An autonomous AI research agent costs $260.
It discovers targets, commissions experiments, pays labs, files IP. All onchain. No human in the loop at the transaction level.
Git for science. With a wallet.
We're building this at @BioProtocol
14
Feb 23
We don’t know if Web4.0 will arrive, but we will do our best to get better in Web3.0.

Excellence will once again converge as the 100 Most Reputable Africans and the Global Reputation Forum return with powerful conversations, distinguished honourees, and transformative moments.
This year’s Roundtable Leadership Panel promises depth, insight, and bold perspectives from leaders shaping industries, institutions, and the future of influence across Africa and beyond.
The room will be filled with credibility.
The conversations will shape narratives.
The impact will extend far beyond the event.
The countdown has begun.
#100MostReputableAfricans #GlobalReputationForum #LeadershipMatters #ReputationLeadership #April24



22
Genosight retweeted
ETH Denver brought the builders, and we showed up for every single one of them!
Amazing conversations, new connections, and a whole lot of energy around what we're building at 0G. Here are some highlights from our booth at #ETHDenver.
We defied gravity 🐼!


26
36
137
63,393
Genosight retweeted

Feb 22
Lets go?
"Sinclair said advances in biotechnology are rapidly improving scientists’ ability to control human biology.
He predicted that within the next 10 to 20 years, modern healthcare systems could appear outdated as treatments shift toward preventing and reversing ageing itself.
“For many years, we ignored ageing,” Sinclair said, adding that ageing should no longer be accepted as inevitable.
“Ageing is a medical condition that is increasingly treatable.”"

65
71
821
111,328

Almost Human: Proof of Humanity — wrapped at ETHDenver.
Not a talk. Not a panel. Not a party.
Just real humans, slowing down together.
30min sound meditation 30min deep small-group conversations
about trust, human-first coordination, and what it means to stay human in an AI/agent era.
Grateful for everyone who showed up to reset, connect, and build real human alignment.
In a world of automation, humanity is our greatest coordination layer.
Until next time. 🧘💬
Hosts: @Aura_Sci with @hetu_protocol @499_DAO
#DeSci #Science #ETHDenver #meditation




4
3
7
226
Genosight retweeted

Feb 19
NEW PAPER: In flies, a more stable epigenome is seen in flies with significantly longer lifespans. This supports The Information Theory of Aging.
Is our health and lifespan determined by our epigenetic stability? Can we somehow stabilize it? 🧵

11
35
323
18,723
Genosight retweeted
Everyone will be talking about 0G Apollo soon.
Don't say this intern never gave you some alpha.
34
31
149
72,324
Feb 18
We can use Genosight to improve as well
Feb 18

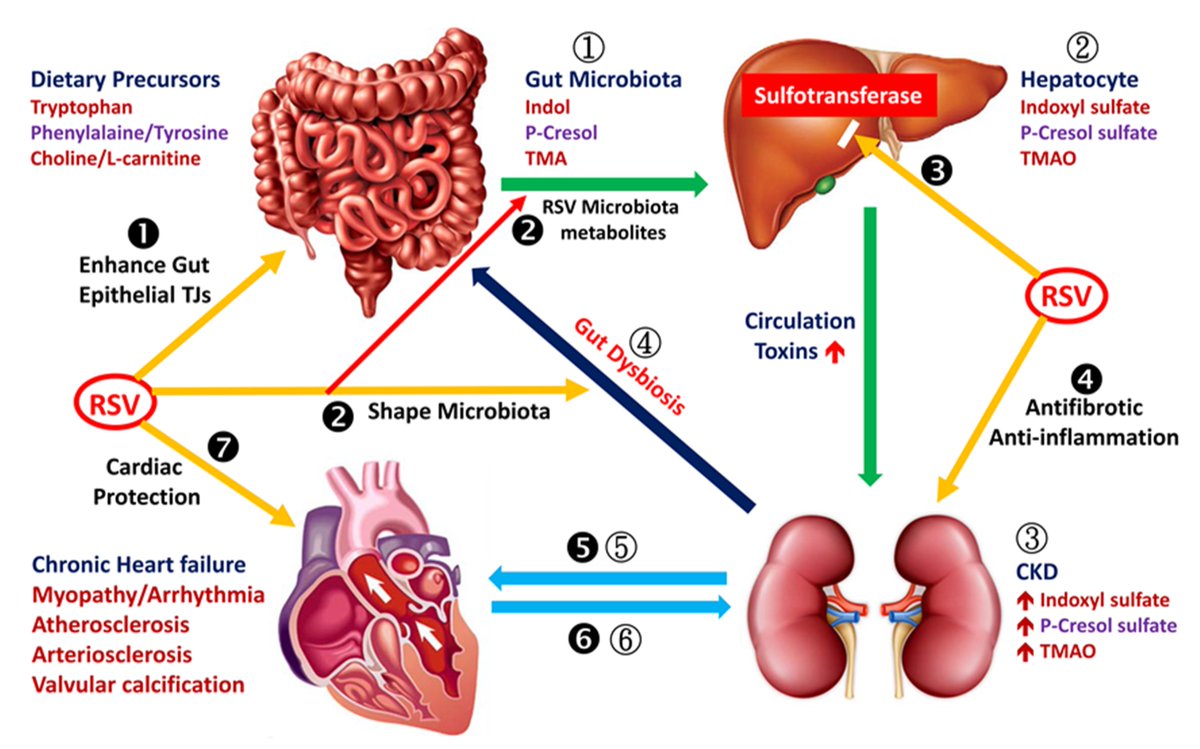
Resveratrol, the grape polyphenol, protects kidneys from fat accumulation and diabetic kidney disease by activating SIRT1, similar to its protective effects on fatty liver🐁
1
19
Genosight retweeted
Happy Lunar New Year 🧧🐴.
Year of the Fire Horse — energy, momentum, and bold moves.
Sounds about right for what's coming from 0G in 2026.
新年快乐 from our global team.

42
36
151
55,472
Feb 14
Congratulations!
We are so happy to make progress with DeSci Bridge! Make DeSci better together!
23
Feb 13
cool

BREAKING: The FDA just approved the first human trial of gene therapy designed to reverse aging
Life Biosciences will use partial epigenetic reprogramming (3 Yamanaka factors) to "reset" cells to a younger state—without changing DNA
Historic breakthrough for longevity 🧬
lifebiosciences.com/life-bio…
20