
Jan 11
➰Why is Sodium Bicarbonate injection used in acute metabolic acidosis & emergencies?
🤹Rapid buffering of excess H⁺ ions:-
Sodium bicarbonate dissociates → HCO₃⁻ binds H⁺ → forms H₂CO₃ → CO₂ H₂O
🌀Quick rise in blood pH (life-saving when pH < 7.1)
🤹Restores cardiovascular function:-
Severe acidosis ↓ myocardial contractility & ↓ response to catecholamines
🌀Bicarbonate improves cardiac output & BP
🤹Stabilizes dangerous hyperkalemia:-
Acidosis shifts K⁺ out of cells
🌀Correcting pH drives K⁺ back intracellularly, reducing arrhythmia risk
🤹Essential in specific emergencies:-
🌀 Cardiac arrest (prolonged CPR)
🌀 Severe metabolic acidosis with shock
🌀TCA overdose (alkalinizes blood)
🌀 Severe hyperkalemia with ECG changes
🌀Certain poisonings (salicylates, methanol, ethylene glycol)
🤹Important caveat:-
♨️Not routine for all acidosis → may cause:
🪬Paradoxical intracellular acidosis
🪬Volume overload, hypernatremia
🪬Hypocalcemia, ↓ oxygen release (left shift)
🤹Golden rule:
🌀Treat the cause first (sepsis, DKA, renal failure).
🌀Use bicarbonate only when acidosis itself is immediately life-threatening.
#EmergencyMedicine #MetabolicAcidosis #CriticalCare #AcidBaseBalance #Hyperkalemia #Pharmacology #MedicalPearls #KriMeeraHC
1
6
456

30 Aug 2025
Last, but not least... #respiratoryalkalosis...🥵
To read more: surgicalpizza.org/critical-c…
#spbites 🍕 #surgicalpizza #acidbasebalance #ACS #CriticalCare #emergencysurgery #trauma #surgery #education #MedTwitter #MedEd

1
3
423

24 Aug 2025
@Ahmedata7777 Vomiting causes hypokalemic metabolic alkalosis due to HCl loss, raising pH & prompting K excretion. Diarrhea causes hypokalemic metabolic acidosis from HCO3- loss, lowering pH & depleting K . #MedicalScience #AcidBaseBalance
2
931
23 Aug 2025
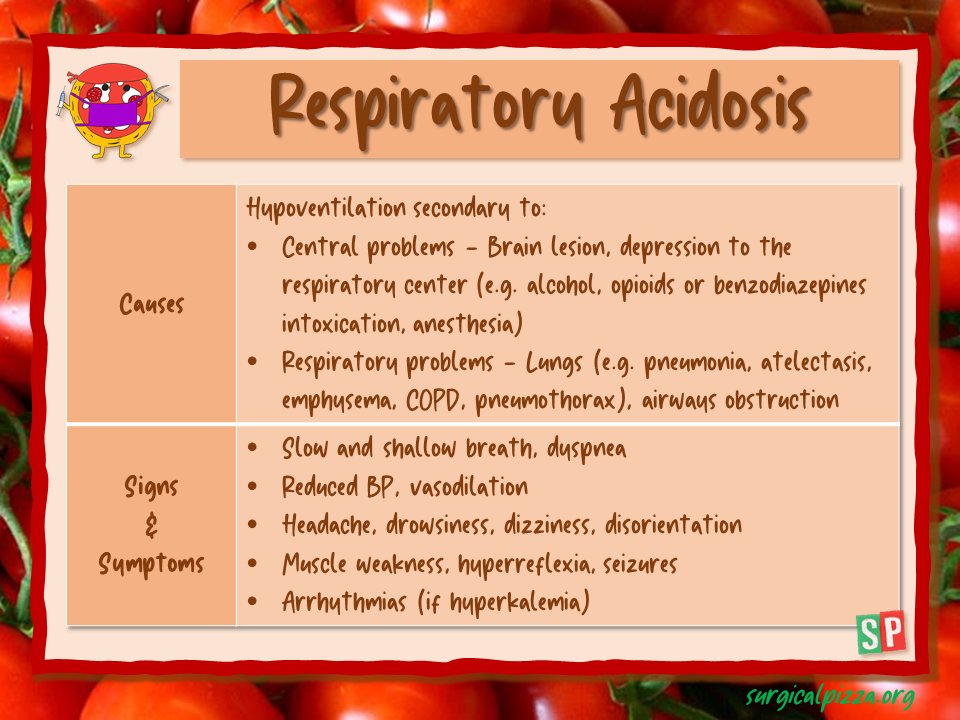
#respiratoryacidosis...😷 Causes, signs & symptoms...
To read more: surgicalpizza.org/critical-c…
#spbites 🍕 #surgicalpizza #ACS #CriticalCare #trauma #emergencysurgery #acidbasebalance #surgery #education #MedTwitter
1
3
472
10 Aug 2025
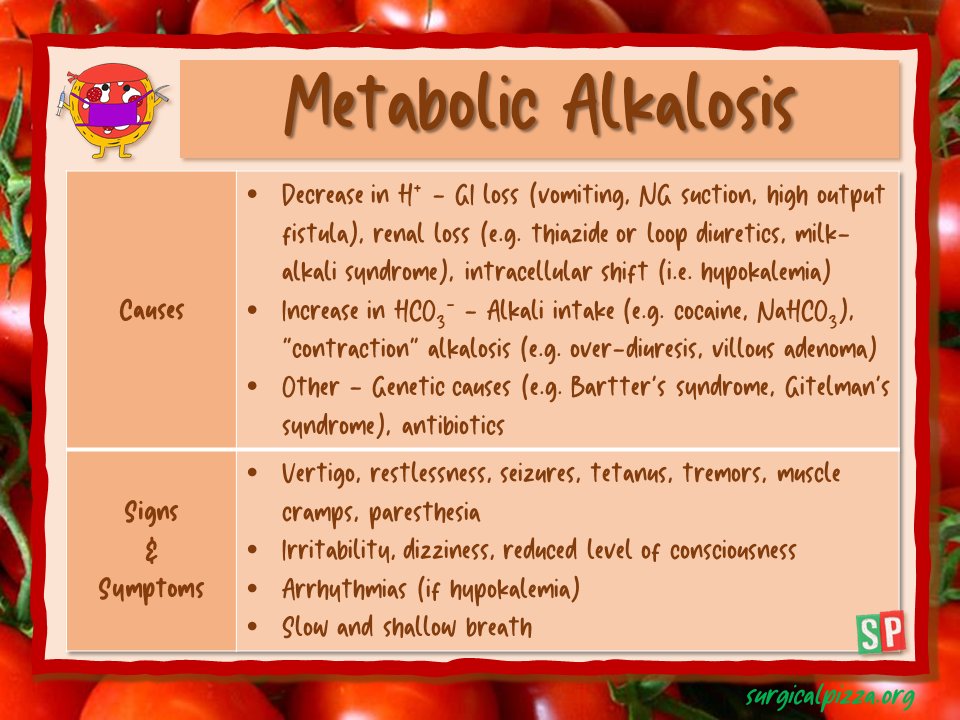
#metabolicalkalosis...🔋
To read more: surgicalpizza.org/critical-c…
#surgicalpizza #spbites 🍕 #acidbasebalance #criticalcare #trauma #emergencysurgery #surgery #ACS #education #MedEd
3
4
557
4 Aug 2025
Let's talk about #MetabolicAcidosis...🧪
To read more: surgicalpizza.org/critical-c…
#surgicalpizza #spbites 🍕 #acidbasebalance #CriticalCare #ACS #emergencysurgery #trauma #Surgery #education #MedEd

4
4
452
19 Jul 2025
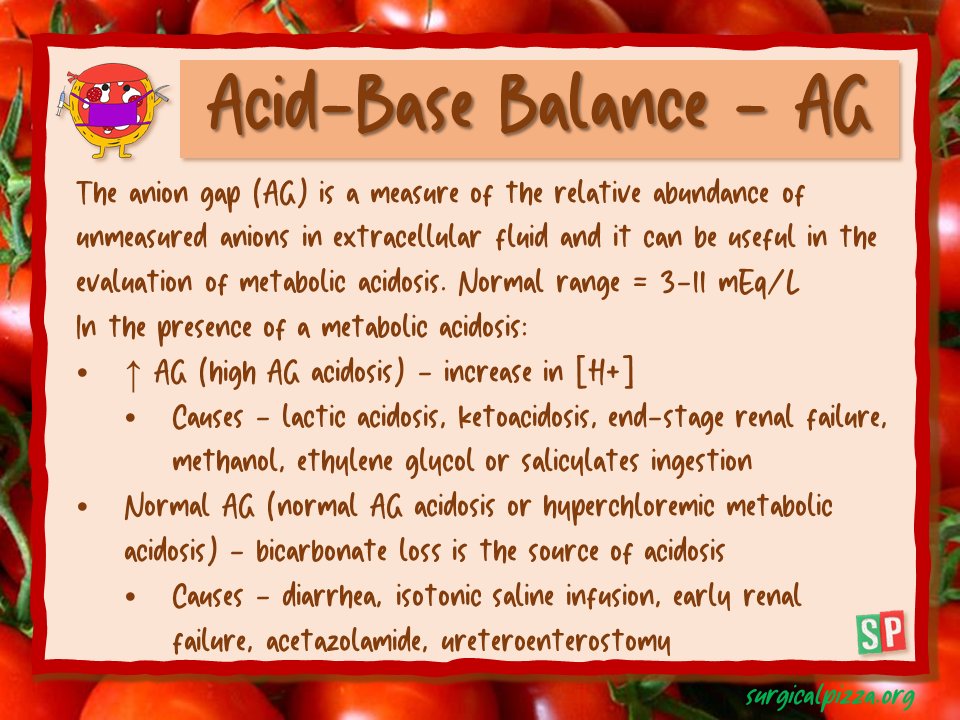
...and the anion gap? 🤯
To know more: surgicalpizza.org/critical-c…
#spbites 🍕 #surgicalpizza #ACS #surgery #criticalcare #acidbasebalance #trauma #ABGInterpretation #education #MedEd #MedTwitter
1
2
1,086
5 Jul 2025
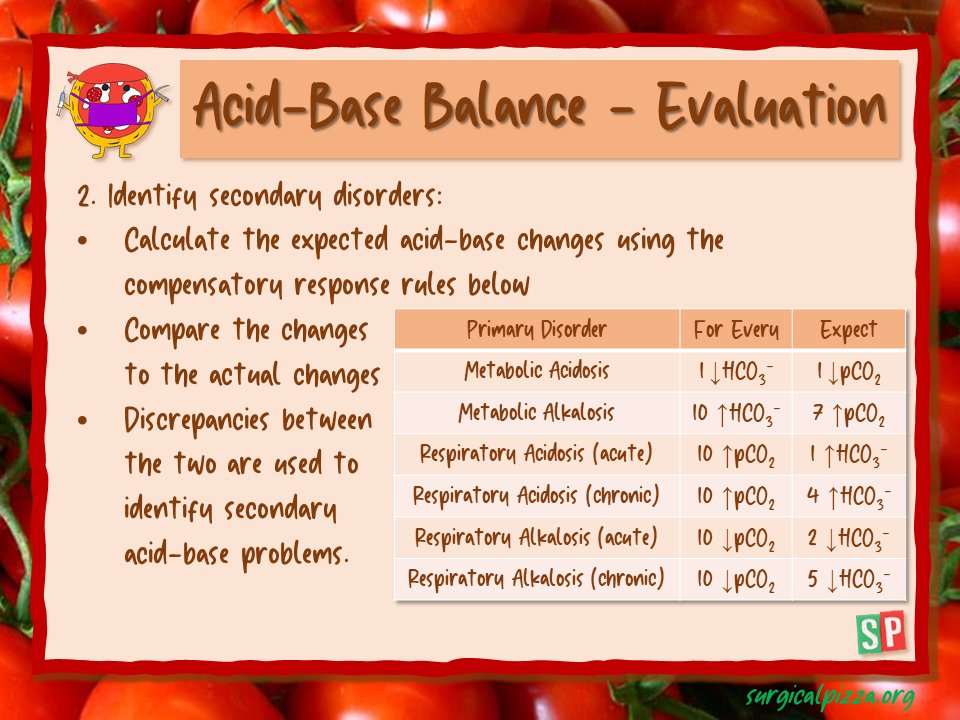
...and what about a second problem??? 😱
To read more: surgicalpizza.org/critical-c…
#spbites 🍕 #surgicalpizza #acidbasebalance #acidebase #surgery #ACS #criticalcare #SCC #emergencysurgery #SurgicalEducation #MedTwitter #meded
1
2
435
28 Jun 2025
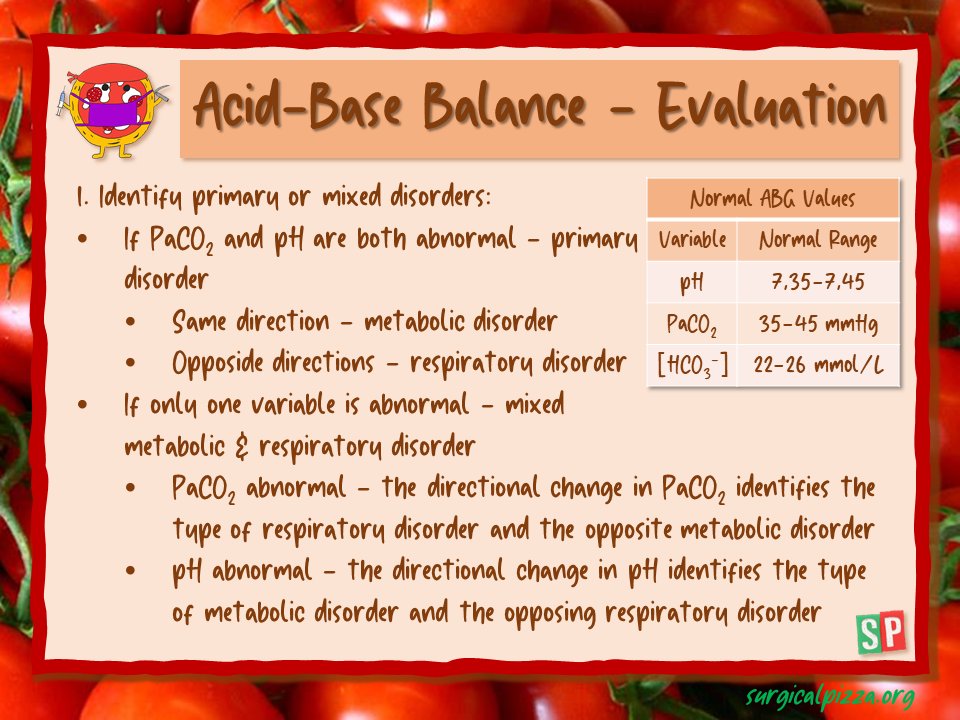
How to identify the #acidbasebalance disorder...🧐
To read more: surgicalpizza.org/critical-c…
#spbites 🍕 #surgicalpizza #ACS #CriticalCare #surgery #trauma #emergencysurgery #education #MedTwitter #MedEd
4
488

27 Jun 2025
💡 Acid Base Homeostasis: Stewart Approach at the Bedside 🛏️
🔹 The Stewart Approach
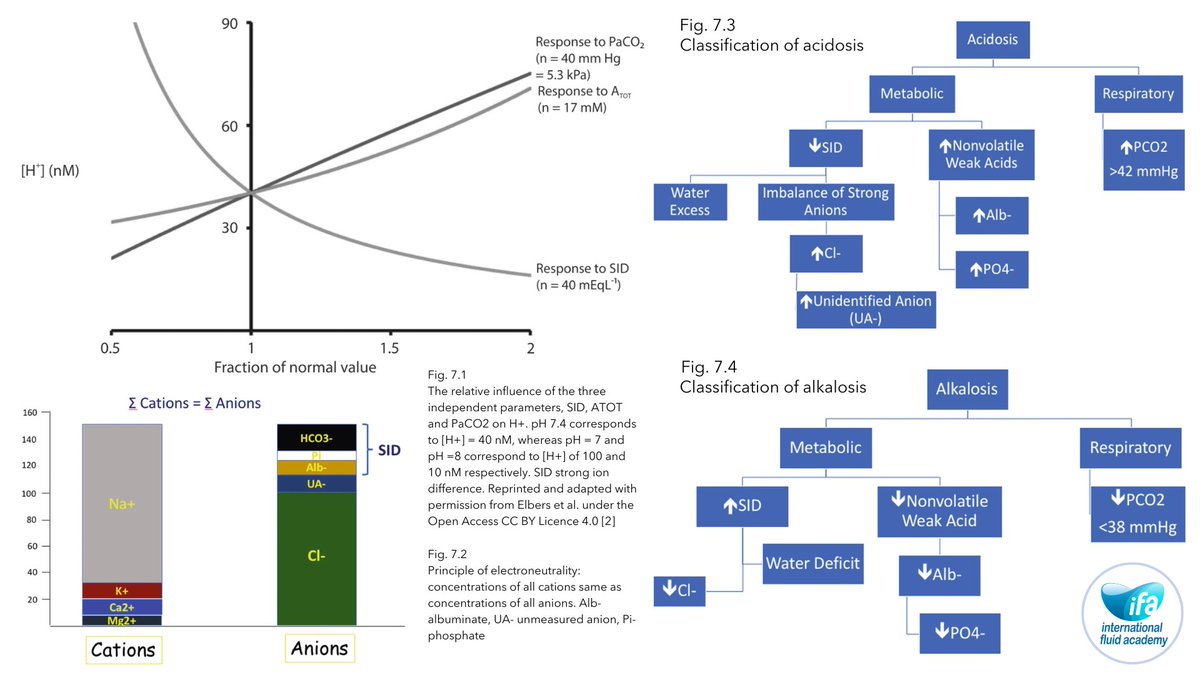
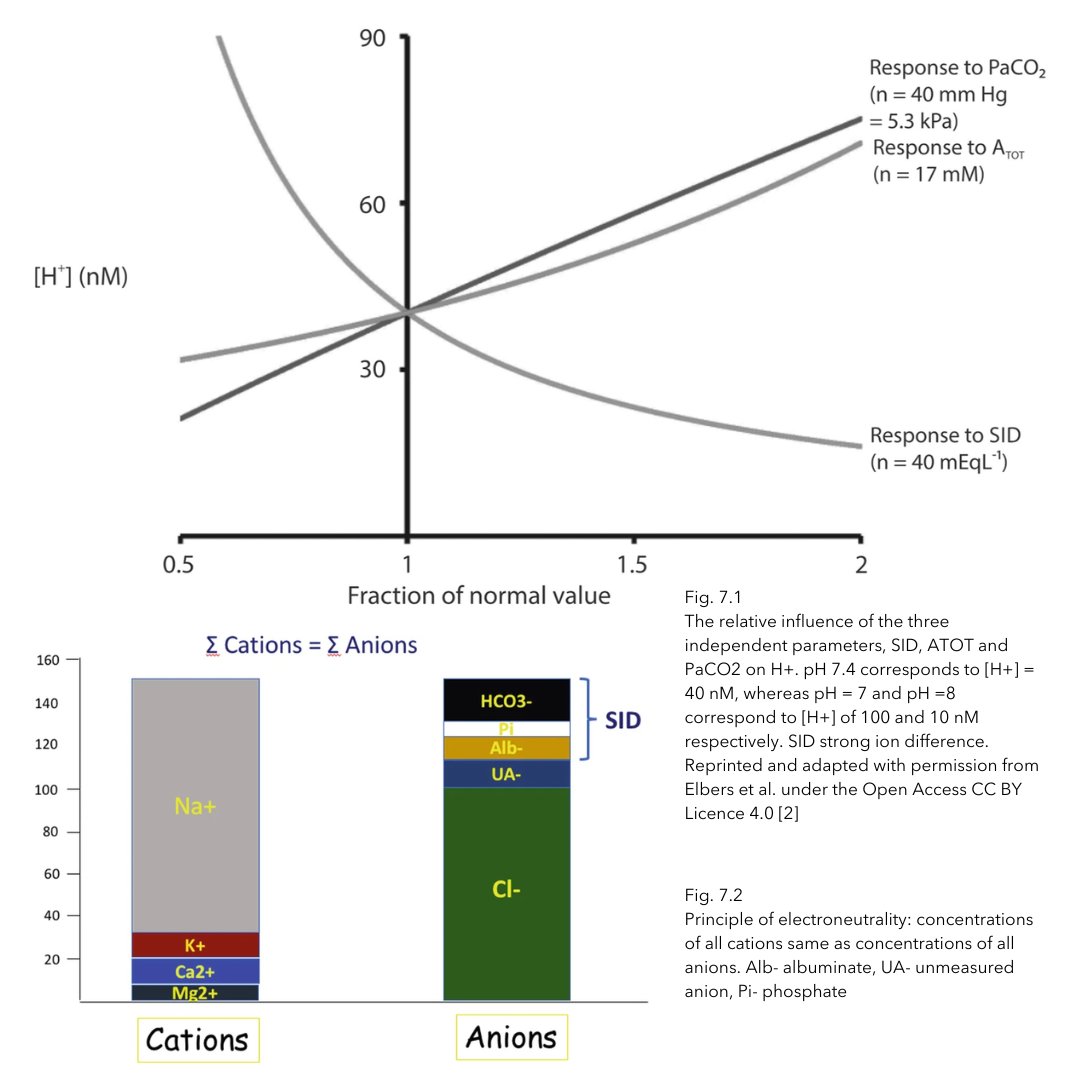
The Stewart approach to acid-base balance offers a modern and increasingly adopted framework in intensive care medicine. Unlike the traditional view, it posits that bicarbonate (HCO₃⁻) is not an independent variable influencing pH. Instead, Stewart emphasizes three key independent variables that govern hydrogen ion concentration—and thus pH—in any solution, including plasma (Fig. 7.1).
Importantly, the Stewart and Henderson-Hasselbalch equations are not contradictory; they are mathematically compatible. Stewart’s method simply provides a more comprehensive, mechanistic understanding of acid-base disturbances.
🔹 Physicochemical Perspective
At the core of Stewart’s method lies the principle of electroneutrality: the total concentration of plasma cations must equal that of anions to maintain electrical neutrality. This balance is visually represented in the Gamblegram (Fig. 7.2), a tool that aids in interpreting complex electrolyte shifts from a physicochemical viewpoint.
🔹 Stewart at Bedside: Fencl-Stewart Approach
To make the Stewart model clinically practical, Fencl and Leith introduced a simplified bedside method. By analyzing plasma concentrations of the independent variables, clinicians can gain direct insight into the pathophysiology of acid-base disorders.
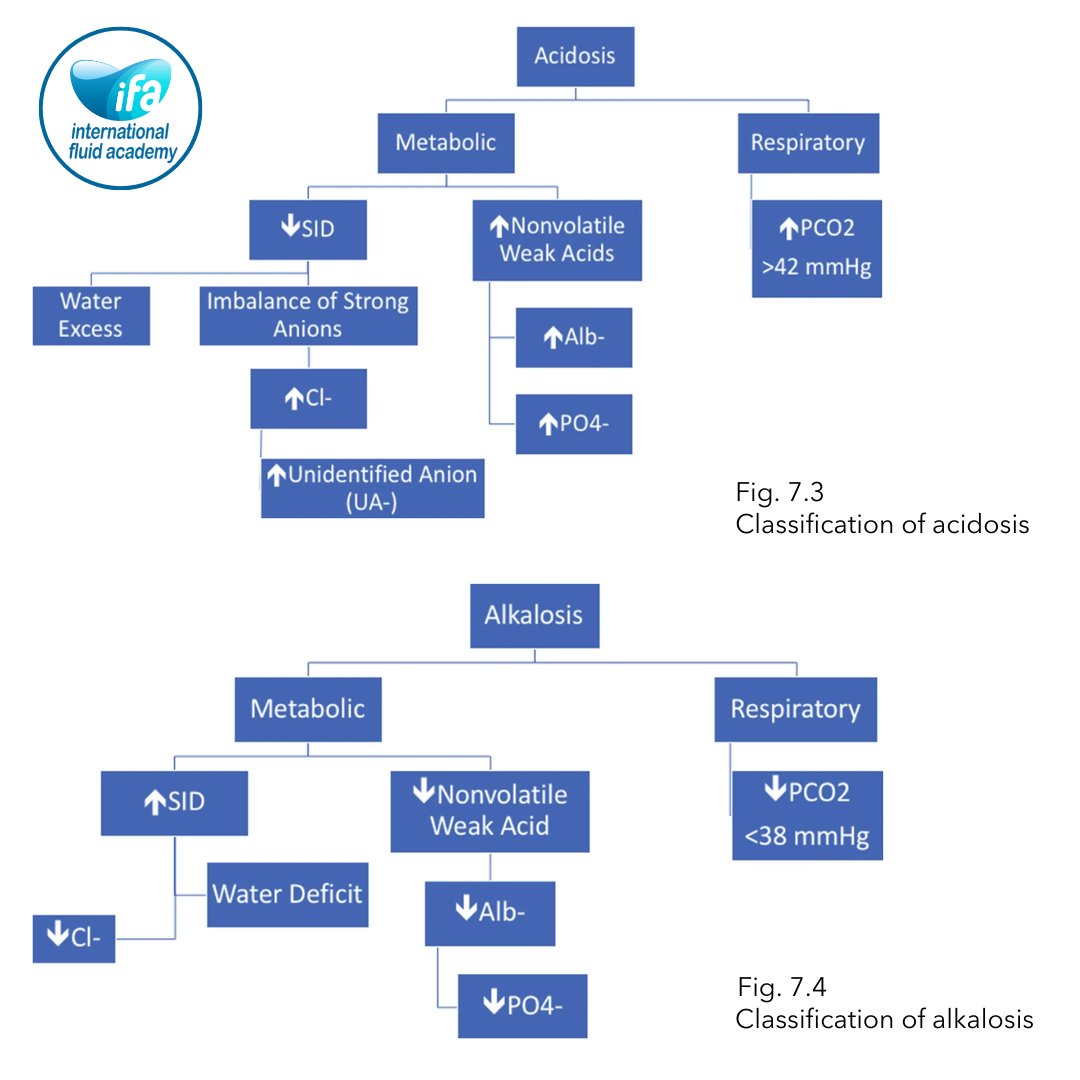
Using this method, causes of acidosis (pH < 7.38) are categorized as shown in Fig. 7.3, and alkalosis (pH > 7.42) in Fig. 7.4—offering a structured and reproducible diagnostic framework for bedside use.
🩺 Unlock these concepts and more on our Members Portal, where you’ll find in-depth content, bedside applications, and exclusive resources designed for healthcare professionals.
🔗 Join now and advance your expertise in fluid management and critical care: fluidacademy.mn.co/posts/rat…
#AcidBaseBalance #StewartApproach #CriticalCare #FluidManagement #MedicalEducation
64
194
9,645
31 May 2025
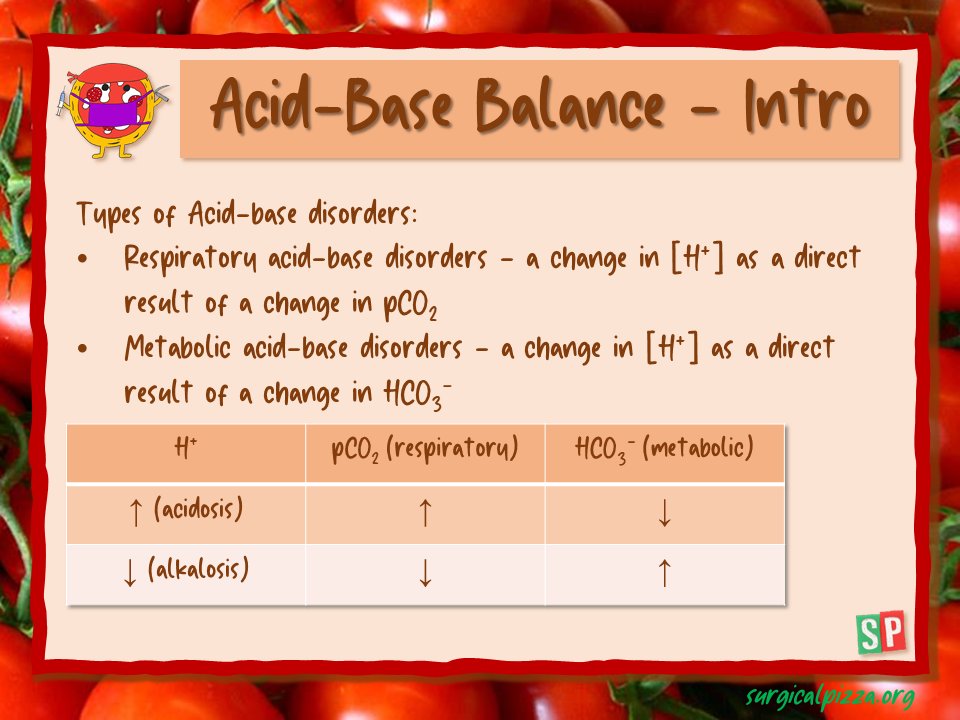
What kind of acid-base disorders can we find? 🔋🧪
To read more: surgicalpizza.org/critical-c…
#spbites 🍕 #acidbasebalance #criticalcare #SCC #ACS #trauma #education #surgery #MedEd #MedTwitter
1
2
630
25 May 2025
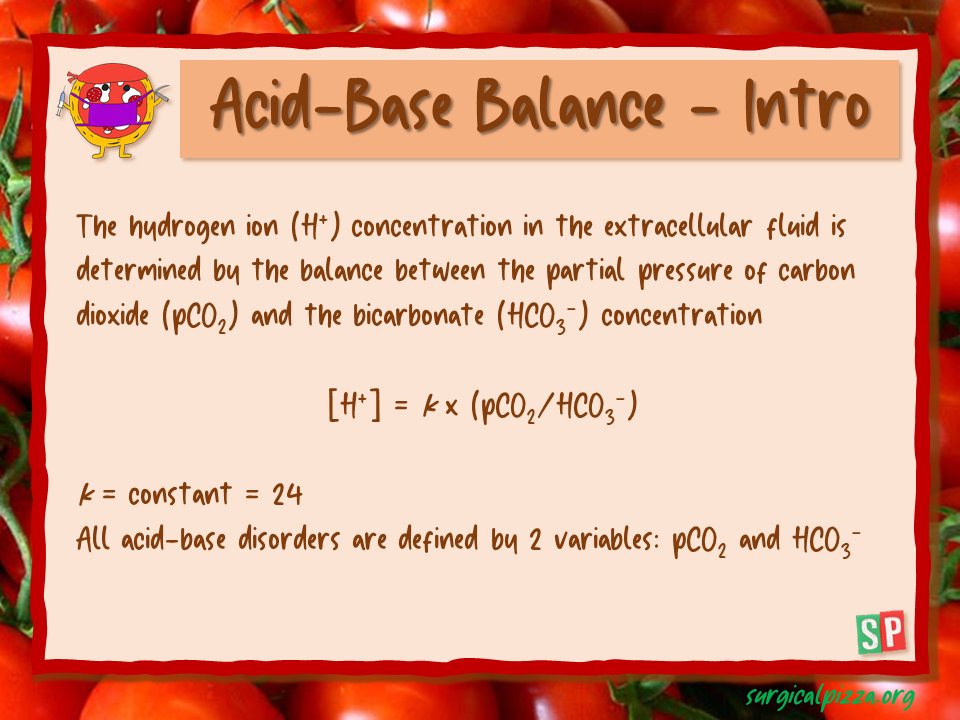
Acid-base balance... what is it?!...🤔
To learn more: surgicalpizza.org/critical-c…
#spbites 🍕 #acidbasebalance #SCC #ACS #trauma #EGS #education #criticalcare #MedEd #MedTwitter
2
6
1,593

28 Mar 2025
Acid Meets Buffer: Who Wins in the ICU?
“Understanding buffering of metabolic acidosis in the critically ill – and keeping our minds OPEN!”
Metabolic acidosis is no stranger to the ICU ⚠️. Whether it’s from sepsis 🦠, AKI 🧬, shock 🚨, or large-volume saline resuscitation 💧, it’s our daily bread and butter. But what determines the clinical impact of an acidotic hit?
Not just the amount of acid, but the buffering capacity (β) of the extracellular fluid (ECF) ⚖️. Let’s dive into the beautiful complexity of this often-underappreciated concept 🧠.
#AcidBaseBalance #CriticalCare #MetabolicAcidosis #PhysiologyFirst
2
5
7
655
19 Feb 2025
🔬 Balanced Solutions: Choice of Buffer 💧
Buffered solutions are commonly used in medical settings to help maintain acid–base balance in patients.
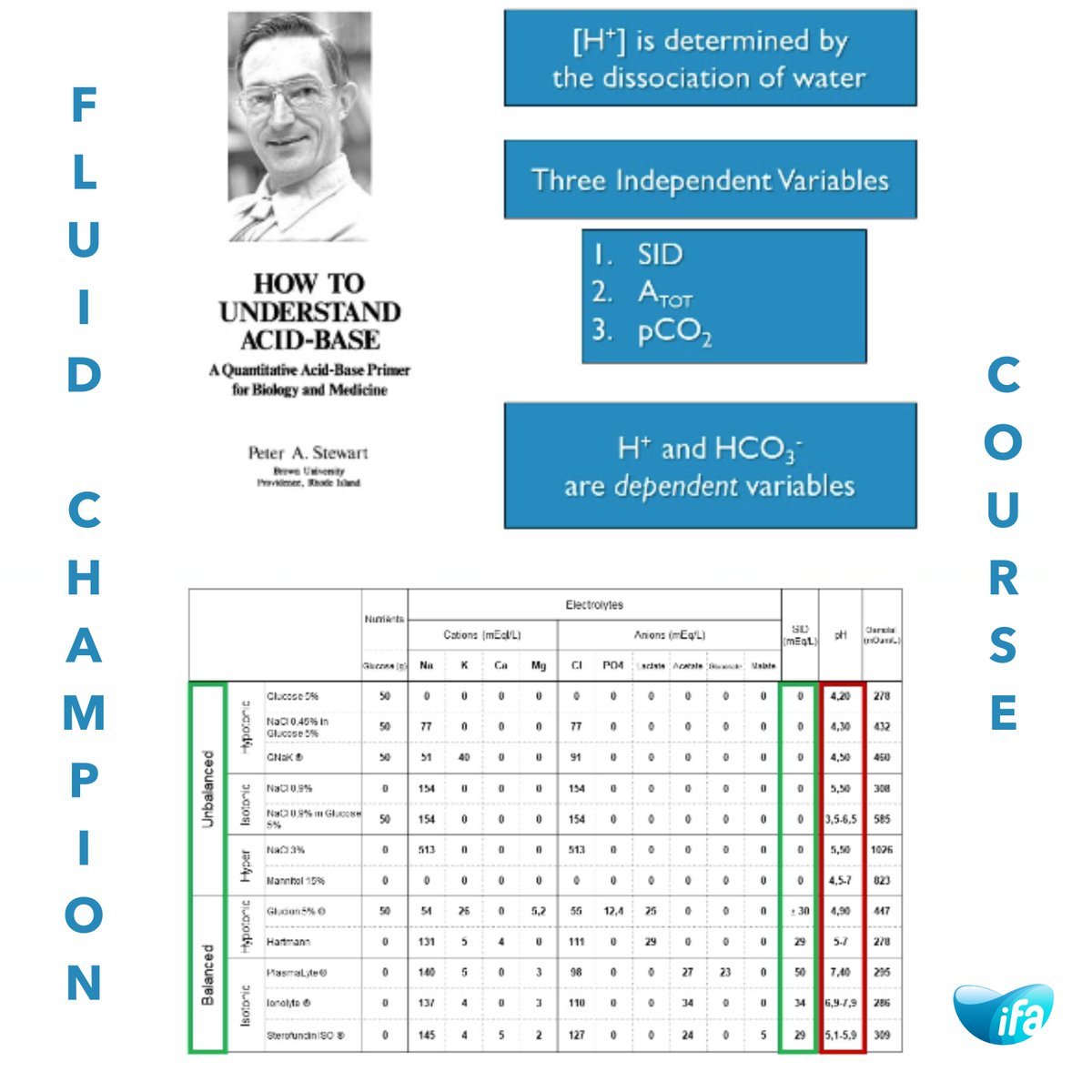
The choice of buffer can impact the effectiveness and safety of the solution. The ideal solution to maintain pH should have a strong ion difference (SID) of around 24–28 mmol/L, whereas abnormal saline has a SID of zero and hereby can induce hyperchloremic metabolic acidosis. Lactate, malate, acetate, gluconate and pyruvate are all potential buffer choices for balanced solutions (Figure). The selection of a particular buffer is influenced by several factors, including pH, the desired buffering capacity and the safety profile of the buffer.
🔹 Buffered/Balanced Crystalloids
Buffered/balanced crystalloids are designed to mimic the composition of human plasma. The key differences between 0.9% NaCl and buffered/balanced crystalloid solutions are the presence of physiological or near-physiological amounts of chloride, a nearly physiological SID and also the presence of additional anions, such as lactate, acetate, malate and gluconate. These anions act as physiological buffers by generating bicarbonate on metabolism. Despite physiological similarities of these solutions to human plasma, presently there is no ideal balanced or physiologically “normal” crystalloid (Table 24.1).
📊 Want to know which buffer to use and when? Get the full details inside our members' portal!
🔗 fluidacademy.mn.co/posts/rat…
#FluidManagement #BalancedSolutions #AcidBaseBalance #CriticalCare #IVFluids #ICU #Anesthesia #FOAMed

38
81
4,942
16 Jan 2025
💡 Acid Base Homeostasis: Stewart Approach at the Bedside 🛏️
🔹 The Stewart Approach
The Stewart approach to acid-base balance is a fascinating method that is increasingly being used by the medical community and especially intensive care physicians. One of the key concepts of the new Stewart approach is that bicarbonate, or HCO3−, does not play any role in acid-base balance as opposed to the traditional and still generally used approach. Interestingly, Stewart does not deny the value of the Henderson Hasselbalch equation.
This implies that both approaches are mathematically compatible and that the Stewart approach may provide the overall and bigger picture. According to the Stewart approach, there are only three independent variables that determine the concentration of H and thus pH in any fluid, including plasma (Fig. 7.1).
🔹 Physicochemical Perspective
Principle of electroneutrality states that concentration of all cations in plasma must be equal to the concentration of all anions to maintain the electrical equilibrium, as can be seen in the Gamblegram below (Fig. 7.2).
🔹 Stewart at Bedside: Fencl-Stewart Approach
Fencl and Leith proposed a simplified approach to Stewart’s physicochemical concept by determining the plasma values of independent variables and getting direct insight into the mechanism of acid base abnormality [2].
Fencl-Stewart: Putting It All Together - causes of acidosis (pH < 7.38) can be re-classified and are depicted in Fig. 7.3. Causes of alkalosis (pH > 7.42) can be classified as shown in Fig. 7.4, following Fencl and Stewart approach.
🩺 Unlock these concepts and more on our Members Portal, where you'll find detailed insights, practical applications, and exclusive educational resources tailored for healthcare professionals.
🔗 Join now and elevate your expertise in fluid management and critical care: fluidacademy.mn.co/posts/rat…
#AcidBaseBalance #StewartApproach #CriticalCare #FluidManagement #MedicalEducation
58
176
9,034
15 Jan 2025
🔬 Acid-Base Homeostasis: Traditional Approach 🔬
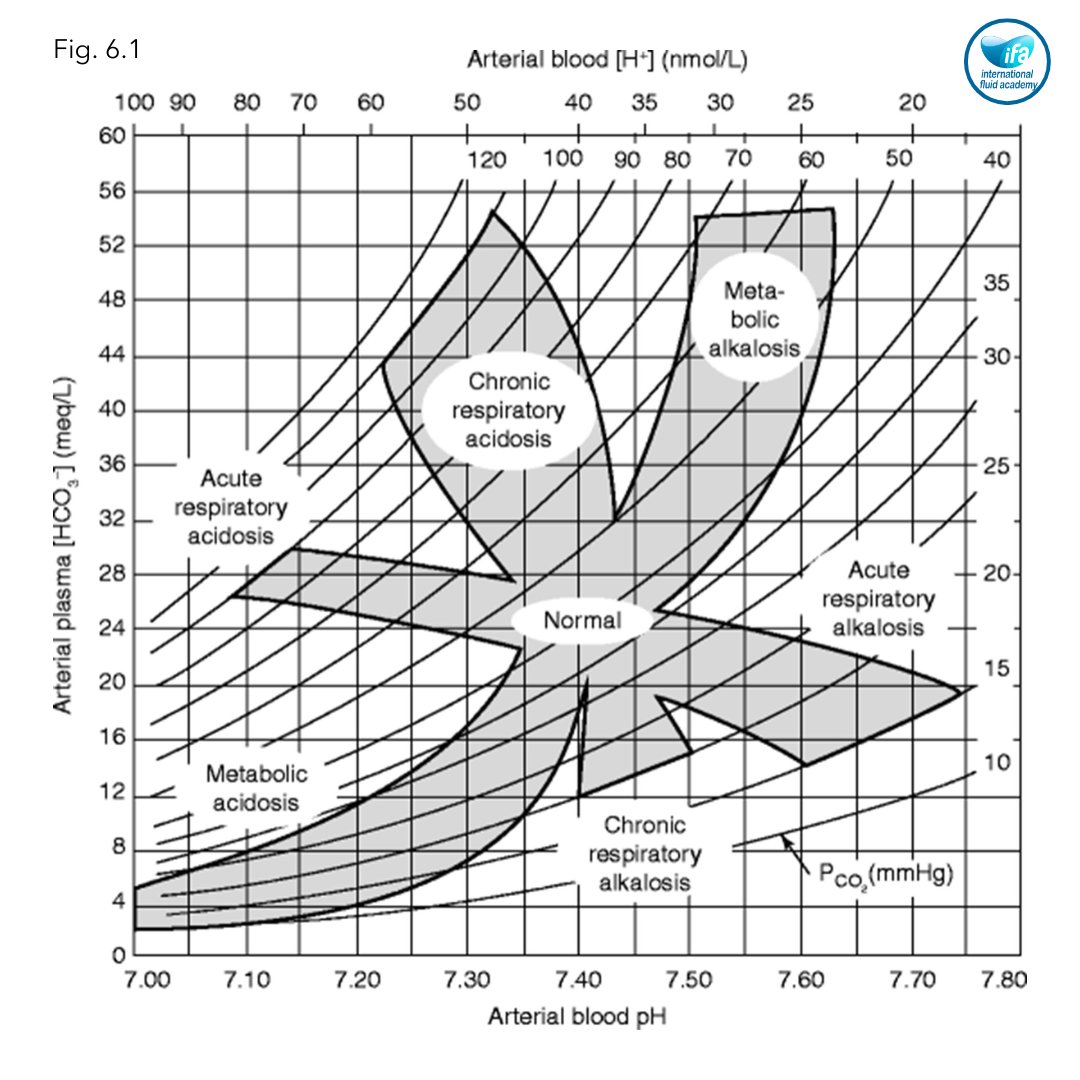
🔹 Acid-base disorders are a common occurrence in critically ill patients, and it is crucial to approach them systematically. There are different methods of interpreting acid-base disorders, including the traditional approach, Stewart's physiochemical approach, and Siggaard-Anderson's base excess approach, as shown in Fig. 6.1.
🔹 Acid-Base Homeostasis
Traditional approach is based on the Henderson–Hasselbalch equation, which states that: pH = pK log10 ([HCO3−]/[0.03 × (PaCO2)]) (pK denotes the acid dissociation constant, [HCO3−] is the bicarbonate ion concentration in plasma in mmol/L and PaCO2 is the partial pressure of CO2 in mmHg). Simplistically, according to the traditional approach, [H ] concentration is proportional to [PaCO2]/[HCO3−]. An acid–base disorder is called “respiratory” when changes in [H ] ion concentration is primarily because of [PaCO2] and “metabolic” when changes in [H ] ion concentration is attributed to variation in [HCO3−].
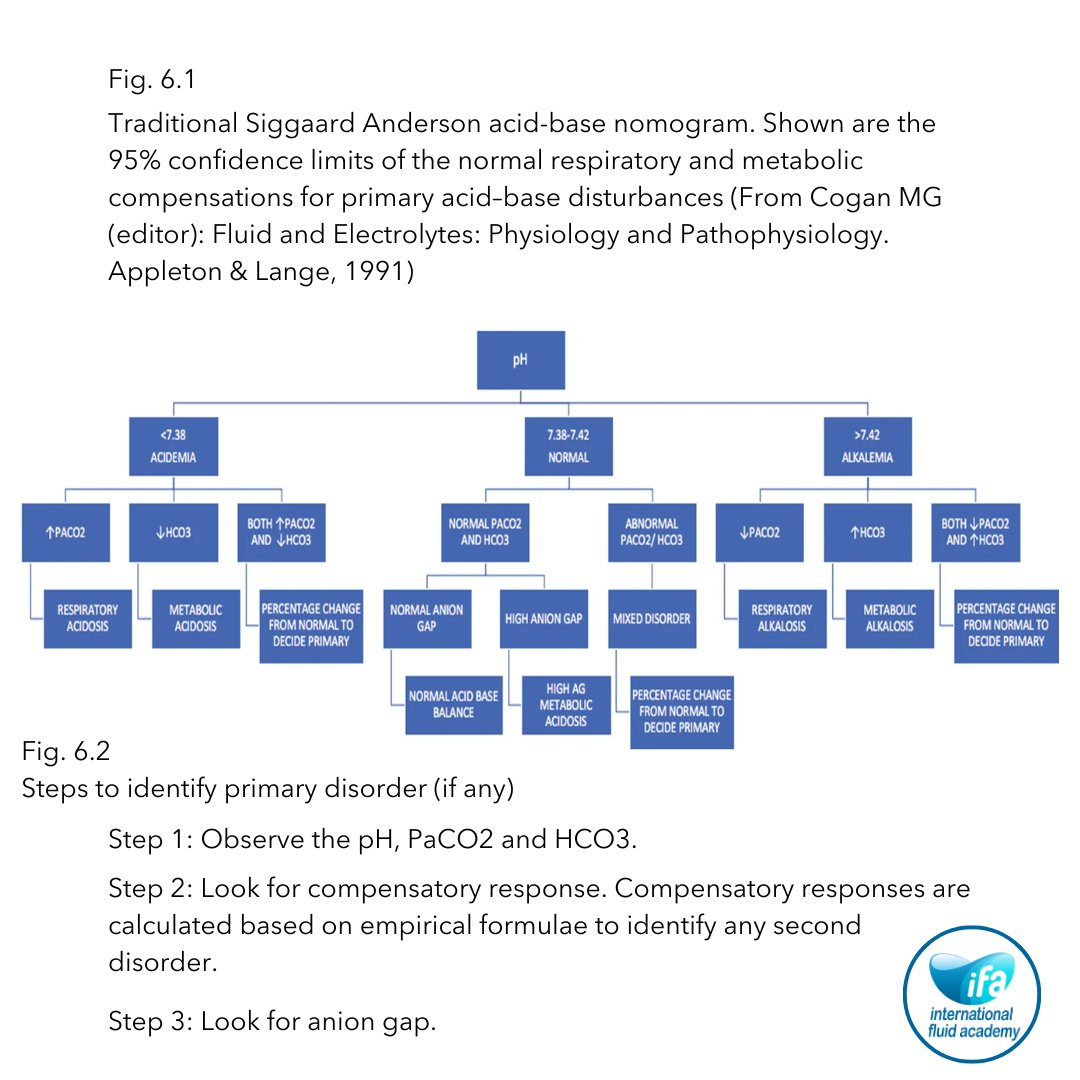
🔹 Step 1: Observe the pH, PaCO2 and HCO3.
🔹 Step 2: Look for compensatory response.
🔹 Step 3: Look for anion gap.
For a comprehensive and systematic understanding of acid-base disorders, including detailed step-by-step approaches, join the Academy.
🔎 Discover all details on our members platform!
🔗 fluidacademy.mn.co/posts/rat…
Fig. 6.1 Traditional Siggaard Anderson acid-base nomogram. Shown are the 95% confidence limits of the normal respiratory and metabolic compensations for primary acid–base disturbances (From Cogan MG (editor): Fluid and Electrolytes: Physiology and Pathophysiology. Appleton & Lange, 1991)
Fig. 6.2 Steps to identify primary disorder (if any)
#CriticalCare #AcidBaseBalance #FluidManagement #MedicalEducation #JoinNow
53
147
8,722
31 Oct 2024
🎃 This Halloween, let’s appreciate the science behind our “life-giving potions” and remember the magic healthcare professionals bring to fluid management every day! 🎃
💡 Join us for the 5th lesson of our Fluid Champion Course, Understanding Strong Ion Difference in IV Fluids!
In this session, Dr. Niels Van Regenmortel explores the strong ion difference (SID) in IV fluids, clarifying common misconceptions and highlighting how pH and chloride levels impact acid-base balance. Based on the principles of Peter Stewart, this lecture offers healthcare professionals a scientific framework to make informed decisions between balanced and unbalanced IV solutions—ultimately elevating patient care. 💉🏥
📅 Ready to enhance your fluid knowledge? Sign up now! 🙌👇
fluidacademy.mn.co/spaces/15…
#FluidChampionCourse #FluidManagement #CriticalCare #AcidBaseBalance #HealthcareEducation #PatientCare #IVFluids
6
19
1,874

27 Sep 2024
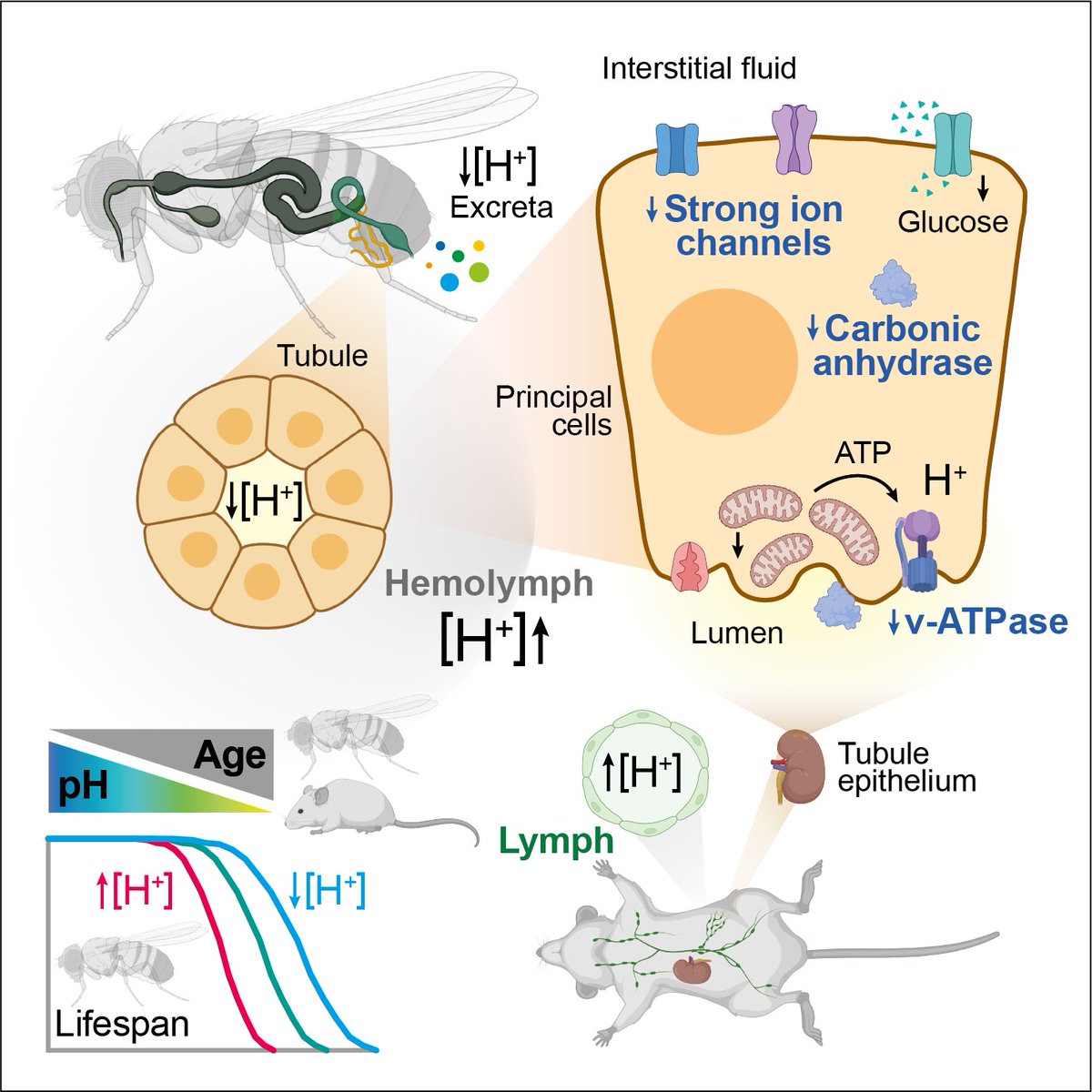
Using a powerful combination of #Drosophila and #mouse models, we investigate physiological #pH during #aging, and propose loss of #AcidBaseBalance as a novel #HallmarkOfAging
1
1
9
950
24 Aug 2024
⚙️🤖Diving into Continuous Renal Replacement Therapy (CRRT) & Its Complications 🚑
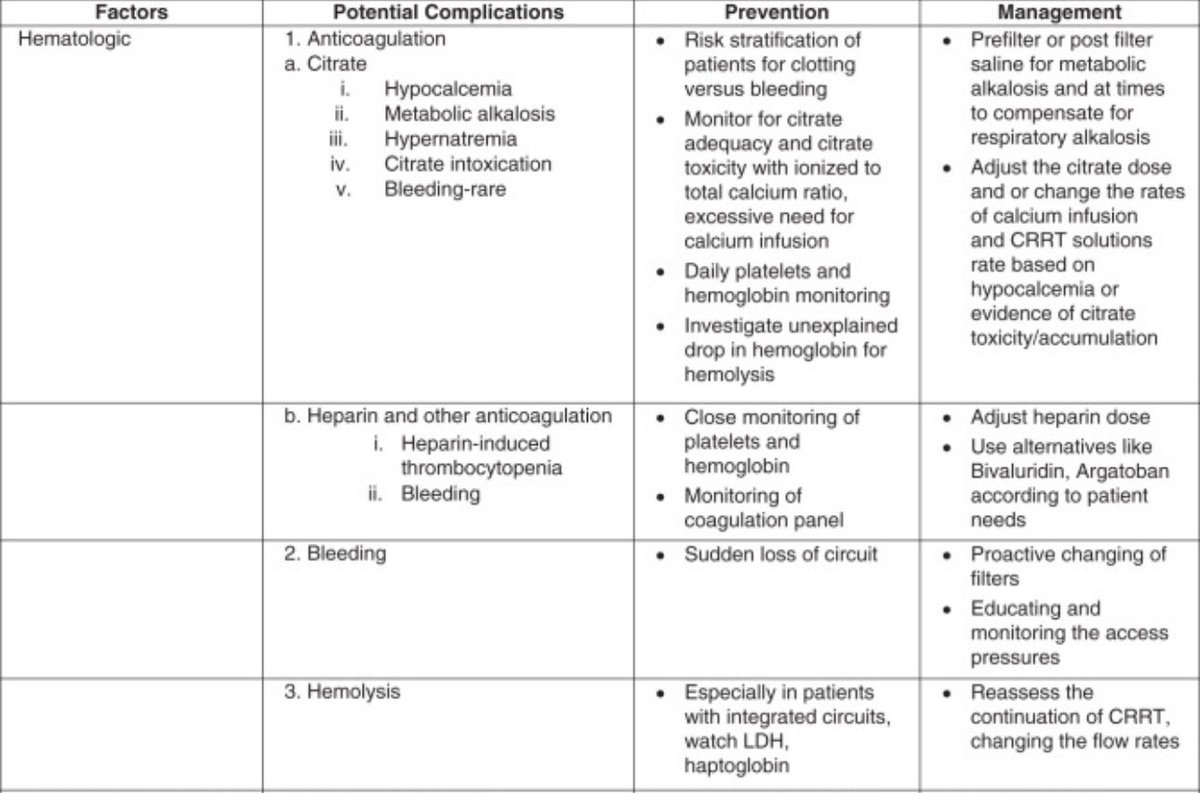
🚨Managing Hematologic Complications in CRRT 💉
🔬 Understanding Hematologic Impact
Continuous Renal Replacement Therapy (CRRT) doesn’t just cleanse the blood—it also has significant effects on blood components, which can lead to a host of hematologic complications. These issues, if not carefully managed, can undermine the benefits of CRRT and even harm the patient.
🩸 Key Hematologic Complications
1.Anemia: CRRT can contribute to anemia by removing red blood cells (RBCs) during filtration and through blood loss associated with frequent circuit changes. Anemia in critically ill patients can exacerbate hypoxia and worsen overall outcomes, making it essential to monitor and manage hemoglobin levels closely.
2.Platelet Dysfunction: The interaction of blood with the extracorporeal circuit can lead to platelet activation and consumption, increasing the risk of bleeding. This is particularly concerning in patients who are already at risk for bleeding or are receiving anticoagulation therapy as part of CRRT.
3.Coagulopathy: CRRT can affect the delicate balance of coagulation, either by causing excessive clotting (due to inadequate anticoagulation) or by contributing to bleeding (due to anticoagulation or platelet dysfunction). Managing this balance is critical to prevent both thrombosis and hemorrhage.
4.Dilutional Coagulopathy: The continuous nature of CRRT can lead to dilution of clotting factors, especially if large volumes of replacement fluids are used. This can impair the body’s ability to form clots, increasing bleeding risk.
💡 Strategies for Managing Hematologic Complications
•Blood Product Administration: Regular monitoring of hemoglobin and platelet counts is essential. Transfusions of RBCs or platelets may be necessary to manage anemia or thrombocytopenia. However, transfusions should be carefully considered to avoid fluid overload and transfusion-related complications.
•Adjusting Anticoagulation: Tailoring anticoagulation protocols to the individual patient’s needs can help prevent both clotting and bleeding. Options like regional citrate anticoagulation can minimize systemic anticoagulation effects, reducing bleeding risk.
•Monitoring Coagulation Status: Frequent assessment of coagulation parameters, such as PT, APTT, and fibrinogen levels, is vital. Adjusting therapy based on these parameters can help maintain the right balance between clotting and bleeding.
•Replacement Therapy: In cases of dilutional coagulopathy, administering clotting factors (e.g., fresh frozen plasma or cryoprecipitate) may be necessary. This helps to replenish the body’s clotting ability and reduce bleeding risk.
🚀 What’s Next: Navigating Electrolyte Disturbances
In the final part of this series, we’ll focus on the intricacies of managing electrolyte imbalances during CRRT. From hypokalemia to hypercalcemia, we’ll cover how to keep electrolytes in check and ensure the therapy is both safe and effective. Don’t miss this crucial discussion!
#CRRT #ICU #CriticalCare #Hematology #Nephrology #PatientSafety #Anemia #Platelets #Coagulopathy #CRRT #ICU #CriticalCare #VascularAccess #Nephrology #PatientSafety #Hemodialysis #CatheterCare #CriticalCare #AcidBaseBalance #AKI #Physiology #pocus #ICU #citrate #dialytrauma #vascularaccess #pocus #Nephrocriticalcare #CRRT #RRT #complication #patientsafetyfirst
#NerdyMedicine #MedX #MedEducation #Medtwitter #FOAM #FOAMed #FOAMcc #EDIC #FFICM #FICM #FCICM #IDCCM #IFCCM #CTCCM #criticalcarereviews @CritCareReviews @nephrocc
23 Aug 2024

⚙️🤖Diving into Continuous Renal Replacement Therapy (CRRT) & Its Complications 🚑
—> PART 3
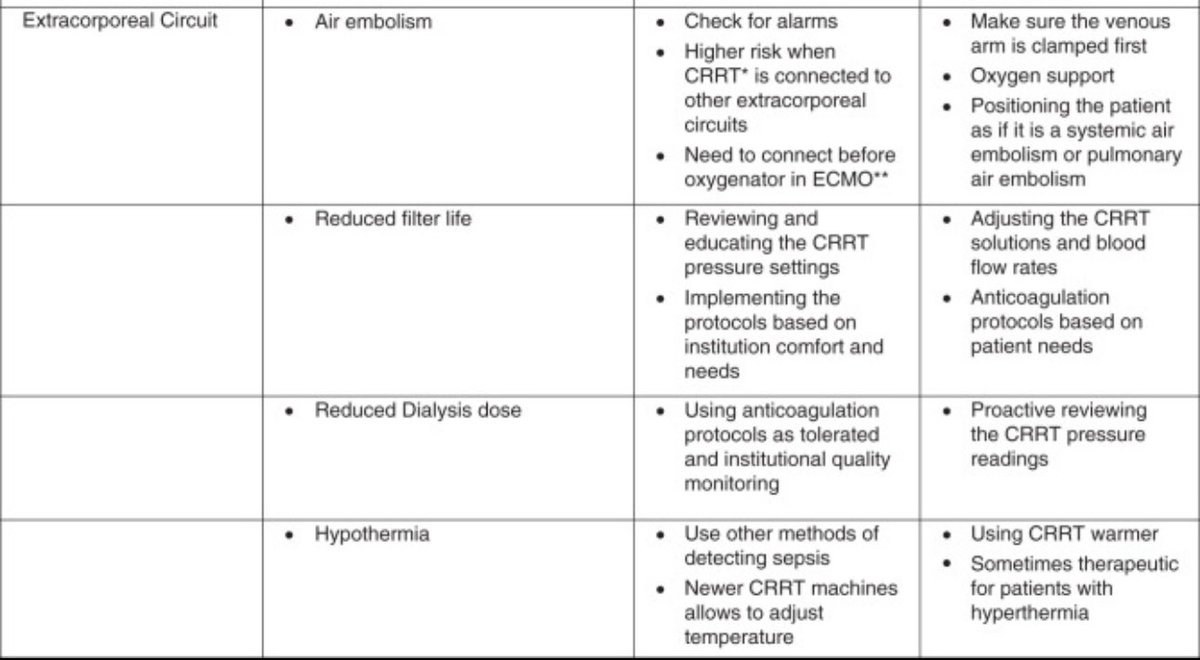
🎙️Tackling Extracorporeal Circuit Complications in CRRT 🧩
🔄 The Role of the Extracorporeal Circuit
The extracorporeal circuit is the lifeline of Continuous Renal Replacement Therapy (CRRT). It’s where blood is purified, toxins are removed, and fluids are balanced. But like any complex system, it’s prone to issues that can jeopardize therapy and patient safety.
🔧 Common Circuit Complications
1.Clotting in the Circuit: Clots can form in the circuit due to inadequate anticoagulation, slowing or stopping blood flow. This not only interrupts therapy but can also damage the circuit components. Filter clotting is particularly problematic, as it requires frequent filter changes, leading to therapy downtime and increased costs.
2.Filter Failure: Filters can fail for several reasons, including clotting, air bubbles, or excessive pressure. A failed filter means the circuit can’t properly remove waste or fluids, leading to ineffective therapy. Repeated filter failure is a red flag for underlying issues that need addressing, like anticoagulation protocols or circuit setup.
3.Air Embolism: Although rare, air can enter the circuit and cause an air embolism, which is potentially life-threatening. This can occur due to improper priming of the circuit, loose connections, or air leaks. An air embolism can lead to cardiovascular collapse, requiring immediate intervention.
4.Pressure Alarms: High or low-pressure alarms indicate issues within the circuit, such as obstructions, clotting, or kinks in the tubing. These alarms are not just annoying—they’re critical safety alerts that must be addressed promptly to avoid therapy interruption or patient harm.
🛠️ Solutions and Best Practices
•Optimizing Anticoagulation: Balancing anticoagulation to prevent clotting while minimizing bleeding risks is key. Regular monitoring and adjusting anticoagulant doses based on clotting times (like APTT) can help maintain circuit patency.
•Filter Care: Ensure proper filter priming and handle with care to avoid damage. Regularly monitor filter pressures and replace the filter promptly if clotting is suspected. Some centers use citrate anticoagulation, which can reduce filter clotting rates.
•Air Detection: Use air detectors in the circuit and ensure all connections are secure. Proper circuit priming and vigilance in checking for air bubbles can help prevent air embolism. In the event of air entry, follow emergency protocols immediately.
•Pressure Monitoring: Regularly check the circuit for kinks or obstructions and address any pressure alarms without delay. Understanding the cause of pressure changes can prevent bigger issues down the line.
🚀 Coming Up: Hematologic Complications
In the next installment, we’ll explore how CRRT affects blood components and what we can do to manage these hematologic challenges. We’ll delve into issues like anemia, platelet dysfunction, and more. Stay tuned for a deep dive into blood management in CRRT!
#CRRT #ICU #CriticalCare #Nephrology #Extracorporeal #PatientSafety #Hemodialysis #FilterCare #AirEmbolism
#CriticalCare #AcidBaseBalance #AKI #Physiology #pocus #ICU #citrate #dialytrauma #vascularaccess #pocus #Nephrocriticalcare #CRRT #RRT #complication #patientsafetyfirst
#NerdyMedicine #MedX #MedEducation #Medtwitter #FOAM #FOAMed #FOAMcc #EDIC #FFICM #FICM #FCICM #IDCCM #IFCCM #CTCCM #criticalcarereviews @CritCareReviews @nephrocc
3
7
5,289
23 Aug 2024
⚙️🤖Diving into Continuous Renal Replacement Therapy (CRRT) & Its Complications 🚑
—> PART 3
🎙️Tackling Extracorporeal Circuit Complications in CRRT 🧩
🔄 The Role of the Extracorporeal Circuit
The extracorporeal circuit is the lifeline of Continuous Renal Replacement Therapy (CRRT). It’s where blood is purified, toxins are removed, and fluids are balanced. But like any complex system, it’s prone to issues that can jeopardize therapy and patient safety.
🔧 Common Circuit Complications
1.Clotting in the Circuit: Clots can form in the circuit due to inadequate anticoagulation, slowing or stopping blood flow. This not only interrupts therapy but can also damage the circuit components. Filter clotting is particularly problematic, as it requires frequent filter changes, leading to therapy downtime and increased costs.
2.Filter Failure: Filters can fail for several reasons, including clotting, air bubbles, or excessive pressure. A failed filter means the circuit can’t properly remove waste or fluids, leading to ineffective therapy. Repeated filter failure is a red flag for underlying issues that need addressing, like anticoagulation protocols or circuit setup.
3.Air Embolism: Although rare, air can enter the circuit and cause an air embolism, which is potentially life-threatening. This can occur due to improper priming of the circuit, loose connections, or air leaks. An air embolism can lead to cardiovascular collapse, requiring immediate intervention.
4.Pressure Alarms: High or low-pressure alarms indicate issues within the circuit, such as obstructions, clotting, or kinks in the tubing. These alarms are not just annoying—they’re critical safety alerts that must be addressed promptly to avoid therapy interruption or patient harm.
🛠️ Solutions and Best Practices
•Optimizing Anticoagulation: Balancing anticoagulation to prevent clotting while minimizing bleeding risks is key. Regular monitoring and adjusting anticoagulant doses based on clotting times (like APTT) can help maintain circuit patency.
•Filter Care: Ensure proper filter priming and handle with care to avoid damage. Regularly monitor filter pressures and replace the filter promptly if clotting is suspected. Some centers use citrate anticoagulation, which can reduce filter clotting rates.
•Air Detection: Use air detectors in the circuit and ensure all connections are secure. Proper circuit priming and vigilance in checking for air bubbles can help prevent air embolism. In the event of air entry, follow emergency protocols immediately.
•Pressure Monitoring: Regularly check the circuit for kinks or obstructions and address any pressure alarms without delay. Understanding the cause of pressure changes can prevent bigger issues down the line.
🚀 Coming Up: Hematologic Complications
In the next installment, we’ll explore how CRRT affects blood components and what we can do to manage these hematologic challenges. We’ll delve into issues like anemia, platelet dysfunction, and more. Stay tuned for a deep dive into blood management in CRRT!
#CRRT #ICU #CriticalCare #Nephrology #Extracorporeal #PatientSafety #Hemodialysis #FilterCare #AirEmbolism
#CriticalCare #AcidBaseBalance #AKI #Physiology #pocus #ICU #citrate #dialytrauma #vascularaccess #pocus #Nephrocriticalcare #CRRT #RRT #complication #patientsafetyfirst
#NerdyMedicine #MedX #MedEducation #Medtwitter #FOAM #FOAMed #FOAMcc #EDIC #FFICM #FICM #FCICM #IDCCM #IFCCM #CTCCM #criticalcarereviews @CritCareReviews @nephrocc
21 Aug 2024
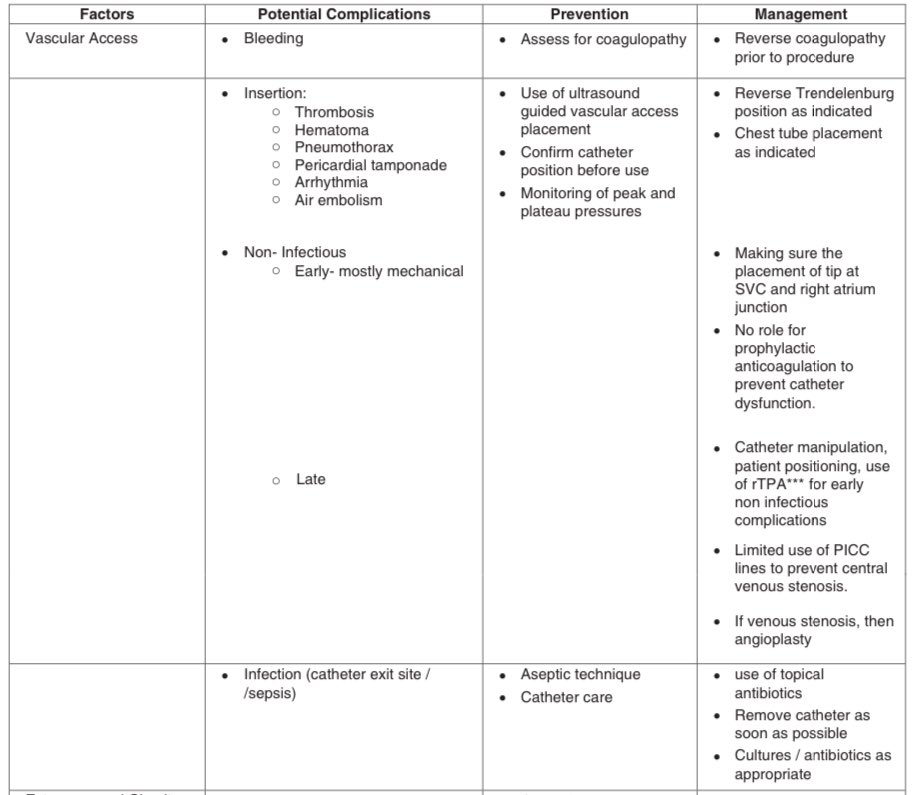
🗺️🗾🧭Navigating Vascular💉🩸 Access Issues in Continuous Renal Replacement Therapy (CRRT) 🔄- PART 2
🔍 Why Vascular Access Matters
When it comes to CRRT, the first hurdle is getting—and keeping—reliable vascular access. Without it, the therapy can’t happen, and the patient’s condition can deteriorate rapidly. But it’s not just about sticking a catheter in and calling it a day. Vascular access in critically ill patients is a whole other beast, with complications lurking at every turn.
🔑 Common Challenges
1.Catheter Placement: Getting the catheter into the right vein is easier said than done, especially in patients with challenging anatomy or prior vascular access issues. Misplaced catheters can lead to poor blood flow, increasing the risk of clotting or inadequate therapy.
2.Infection Risks: Catheters provide a direct route for bacteria to enter the bloodstream, making infection a top concern. Central line-associated bloodstream infections (CLABSIs) are a serious complication that can prolong ICU stays and increase mortality.
3.Catheter Occlusion: Blood clots or fibrin sheaths can form around the catheter, leading to blockages that disrupt CRRT. This not only halts the therapy but also risks embolism if clots dislodge.
4.Mechanical Complications: Kinks, dislodgements, or even catheter breakage can occur, particularly if the catheter is not properly secured or if the patient moves frequently. These issues can lead to therapy interruptions and necessitate re-insertion.
💡 Strategies for Success
•Ultrasound-Guided Insertion: Utilizing ultrasound can improve the accuracy of catheter placement, reduce insertion-related complications, and increase first-attempt success rates.
•Aseptic Technique: Rigorous adherence to aseptic techniques during insertion and maintenance can minimize infection risks. This includes proper hand hygiene, use of full barrier precautions, and regular dressing changes.
•Regular Monitoring: Frequent checks for signs of infection, occlusion, or displacement are crucial. Regular flushing of the catheter with saline can help prevent clot formation.
•Patient Positioning: Positioning the patient to minimize movement around the catheter site can reduce the risk of mechanical complications. Securement devices can also help keep the catheter in place.
🚀 Up Next: Extracorporeal Circuit Complications
Stay tuned for Part 3, where we’ll dive into the challenges and solutions related to the extracorporeal circuit, including clotting, filter failure, and more. This is where things get really technical, so don’t miss out!
#CRRT #ICU #CriticalCare #VascularAccess #Nephrology #PatientSafety #Hemodialysis #CatheterCare #CriticalCare #AcidBaseBalance #AKI #Physiology #pocus #ICU #citrate #dialytrauma #vascularaccess #pocus #Nephrocriticalcare #CRRT #RRT #complication #patientsafetyfirst
#NerdyMedicine #MedX #MedEducation #Medtwitter #FOAM #FOAMed #FOAMcc #EDIC #FFICM #FICM #FCICM #IDCCM #IFCCM #CTCCM #criticalcarereviews @CritCareReviews @nephrocc

2
5
1,362