Craig Reagan retweeted

The ALS community saw the Nurown AdComm wasn't seeking the truth. We compiled the survival data ourselves & submitted a Citizen's Petition
@FDACBER has delayed it for >160 days with zero response
@SecKennedy @FDA_KyleD @SenRonJohnson @houmanhemmati @BellinaMatthew @BellinaDeb @RonJohnsonWI @realDonaldTrump @RobertKennedyJr @RepAndyHarrisMD @RepGuthrie @RepGusBilirakis @SenatorWicker @lisamurkowski @SenatorCollins

I am confident he’s being serious re AdComs. Thats good for FDA and it’s great for patients. Put drugs on “trial” for everyone to see.
1
2
4
103

AdComms need to be fair & great deference MUST be given to trial PIs in #RareDiseases as no one at FDA or on AdComm has the same expertise.
@US_FDA has repeatedly IGNORED experts with decades of expertise & 1000s of citations when FDA's clinical team has 0 experience with the rare disease.
@FDA_KyleD @FDACommissioner
@FDACBER @SecKennedy
3
155

The FDA’s evidentiary framework was built for large trials and common diseases. ALS is neither.
Rare disease patients deserve advisory committees that understand urgency, totality of evidence, and the cost of delay. The past NurOwn AdComm understood none of this.
When a disease is 100% fatal, “wait for more data” is not a neutral decision. It’s a decision with consequences, costs lives, and is completely unacceptable. @FDA_KyleD @aVoice4ALS @iamalsorg @SecKennedy @houmanhemmati
Jun 11

I follow FDA news and policy, but did not know about the problem of AdComms until today. Thank you to this author for pointing out even more broken bits at FDA that need a cast. Please fix this. @FDA_KyleD, @SecKennedy & @POTUS. @houmanhemmati @peter_mantas @mike98572986 @PeterPitts @SenRonJohnson @SenRickScott @RepHarshbarger
washingtonexaminer.com/op-ed…
6
14
1,351

Jun 11
$qure $clpt
While we all wait for the update on the type b meeting this article shows the complete saga over the last 12-24 months. This amt-130 situation could be made into a 2 hour movie or a Netflix documentary with the insane drama that has occurred. What is even more crazy about this saga is that you have all this drama and this is only the publicly available side of the story. Can you imagine one day when you get the behind the scenes views of Uniqure, Tabrizi/Sung, internal fda members, patients in the trial, it will get much more crazy.
Don’t think I saw this article before, it was on May 5th, one of the better recaps of the entire Uniqure situation that I have seen. Hopefully for the HD community we get an update soon that is considered fair by them. Some of the interesting passages in the article below. Really shows the devastation that Prasad has occurred, history likely will look very bad on Prasad, mainly due to his intense desire to try to bury this program.
“The cost is measured in patient-years - in the people for whom every additional regulatory month is a measurable, irreversible loss of cognitive and motor function, and in the people who will reach the end of their statistical disease horizons before the trial the FDA is now requiring is even completed. Those people exist. They are named. They have families. They have read the same data the FDA read. They have read the same agreement the FDA signed and unsigned. They are asking what changed. They deserve an answer.”
“What the FDA has not addressed publicly is that uniQure used a sham control in approximately 10 patients earlier in the AMT-130 program and then stopped using it, precisely because of ethical concerns about asking patients with a fatal disease to undergo a procedure with no therapeutic benefit. According to a clinical analysis published by chemistry blogger and longtime industry observer Derek Lowe at Science.org, roughly 10% of those original sham-arm patients developed a blood clot during the procedure, which involved 10 to 12 hours of general anesthesia.”
“Bioethics professor Holly Fernandez Lynch of the University of Pennsylvania, asked about the FDA's practice of attacking uniQure on background calls with reporters, said: "The fact that you are sharing information with the press without standing behind it either suggests that you know you should not be talking to the press or that you don't really stand behind your opinion. Why are we debating this in the court of public opinion? The stakes are too high."
“Several other companies have publicly requested adcomm meetings, and at least three have said the FDA initially told them to prepare for a meeting and then retracted that guidance. On the same March 5 background call where the senior FDA official attacked uniQure and singled out Woodcock by name, the official also dismissed the broader pool of outside scientists who serve on FDA advisory panels, saying they "do not do their homework" and may be motivated by financial conflicts of interest. The agency's position is that an advisory committee is unnecessary. The agency's former Acting Commissioner, multiple senators, the rare disease community, and at least three other companies that have requested adcomms believe an advisory committee is precisely what is required.”
“The agency has granted four expedited designations to AMT-130 specifically: Fast Track in 2019, Orphan Drug, RMAT in 2024, and Breakthrough Therapy in 2025. Each designation is supposed to mean the FDA recognizes both the unmet need and the substantial preliminary evidence of effectiveness. Each was granted on the same data the agency now describes as unable to demonstrate "any therapeutic benefit."
davemanuel.com/2026/05/05/fd…
5
5
53
6,806
Bert retweeted

.@chrisaikenmd FDA AdComm for approval of Zyorexa for peds had data showing 11% of kids were d/ced from drug after 2 weeks due to elevated LFTs. Ppl didn't notice because of splitting of diff LFTs. Laughren suggested making it 2nd line, ostensibly b/c of weight gain. Even though it's worse w Seroquel which it wasn't suggested for. At Adcomm Lilly agreed too readily to 2nd line status. But then it never happened.
I have a hypothesis on the mxn.
From memory so hopefully no errors.
Jun 10

Should you check liver enzymes on second generation antipsychotics?
Larger studies, with refined designs, point to a yes for some of them:
psych-partners.com/olanzapin…
#psychiatry #pmhnp
1
1
161

Not surprised at these comments given the issues with rare disease sponsors accessing accelerated approval.
@PharmaPinkSheet
@MaaishaO: Rare Disease Groups Tell US FDA Endpoint, Biomarker, Adcomm Reforms Needed insights.citeline.com/pink-s…
78

Jun 7
The FDA adcomm meeting on Moderna’s mRNA flu vaccine will be virtual.
One thing I miss about in-person meetings, beyond the human connection and the natural flow that comes with being together in one room, is the visual cues when questions arose. Hands went up. Placards flipped. Microphone lights came on.
You got a feel for how many people had questions and whether everyone was getting a chance to speak. Maybe that’s just me, but it felt like an added layer of transparency.
To be fair, virtual meetings probably expand participation. I still prefer a hybrid approach, ideally with the committee, FDA, sponsor, and anyone who wants to attend in person together in the room, while preserving virtual participation options, especially for public speakers and other key participants for whom remote participation may be the only practical option.
#VRBPAC
5
618

Jun 5
Binary for sHTG an overstatement, but overall critical months. But never forget that $IONS has a history of safety surprises that show up only on the label or in AdComm docs. See HAE drug etc.
1
4
802

Jun 2
Wedbush about $ABVX 'upgrade'
Regulatory Risk: Safety signals increase the risk of a potential "black box warning" and may require an FDA Advisory Committee (AdComm) meeting prior to approval
2
1,585


May 27
FDA delays ruling on AstraZeneca’s breast cancer drug after negative adcomm vote fiercebiotech.com/biotech/fd…
1
2
8
3,105
May 27
Don’t get me wrong, I’m happy to see any FDA advisory committee meeting these days.
But it does get under my skin a bit to see another fairly routine COVID strain selection meeting this week while broader public debates around regulatory process, transparency, and surveillance methodology remain largely outside transparent public discussion.
Still, I do think the upcoming Moderna flu vaccine adcomm on June 18 might be a good sign of more to come.
Hopefully the advisory committee process starts to come back to life, considers reforms, and perhaps can evolve into a more nimble public forum that can dedicate a portion of time to broader discussions on pressing regulatory and public health questions alongside its routine agenda items (within any existing procedural constraints), making more efficient use of the expertise already assembled in the room. #VRBPAC
2
1
12
913

May 26
Since 1986, SlideSource has supported over 200 FDA Advisory Committee meetings and produced thousands of effective slides for the pharmaceutical industry. #FDA #AdComm
bit.ly/4bZH2SY

1
2
18
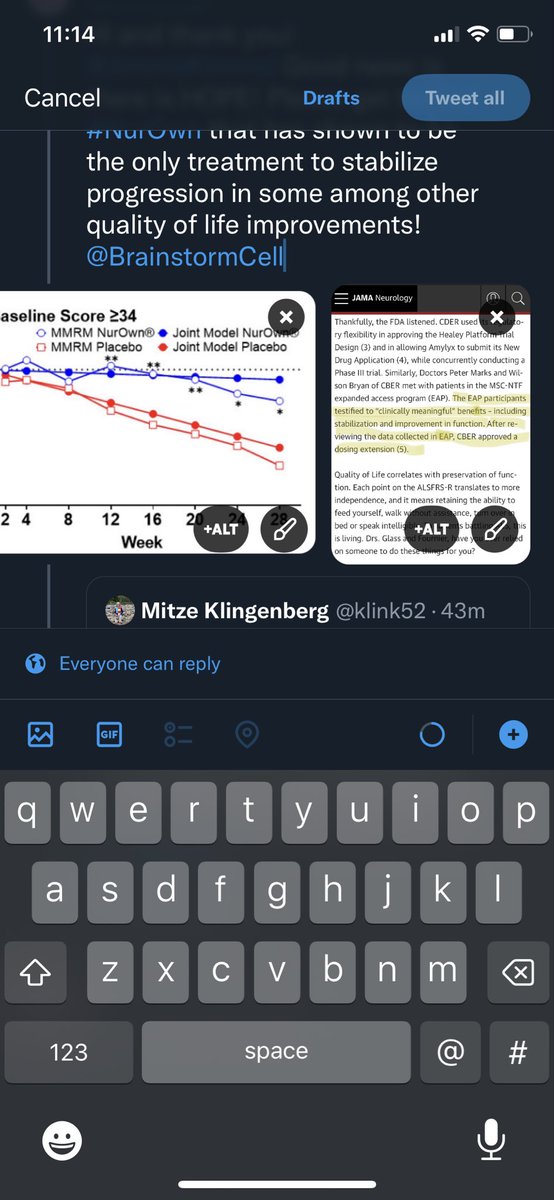
Spot on Dr. and also why I also keep highlighting NurOwn for ALS. There was actually data that showcased a patient whose progression stopped at the adcomm and it was ignored. 5 year survival in the NurOwn EAP is 100% vs. 20% in ALS natural history.

2
2
10
132
May 17
Parts of the Makary FDA postmortem discourse lately have felt a bit like the old Wendy’s commercial:
“WHERE’S THE BEEF?”
The rhetoric is enormous:
chaos, turmoil, habit of overriding scientists, anti-rare disease, goalposts shifting, worst commissioner of all time.
The actual examples? Less enormous. I kept coming back to the same relatively small cluster:
• Moderna mRNA flu vaccine refusal-to-file (unconventional, but ultimately resolved via a split pathway)
• Covid framework/labeling changes
• a handful of rare disease decisions (often without much direct defense of why any specific decision was necessarily wrong on the merits, while largely taking companies at their word regarding prior expectations/guidance – even while making concessions that significant new rare disease guidances/frameworks were advancing)
• staff cuts (largely not Makary’s doing)
• turnover and internal tensions (not entirely surprising during a reform-oriented transition period)
The beefier claims:
• advisory committees:
critics clearly argued that reducing adcomm use weakened transparency, public scientific debate, and procedural legitimacy.
• CNPV:
if you create ultra-fast reviews tied to commissioner discretion and “national priorities,” people are obviously going to worry about politics, favoritism, operational strain, and predictability.
(The flip side: supporters viewed many of these reforms as attempts to address longstanding complaints that FDA had become too slow, too passive, and too unwilling to challenge institutional inertia, while also advancing legitimate national priorities.)
• governing style:
some critics clearly believe FDA legitimacy depends on quieter stewardship, procedural continuity, internal consensus-building, and avoiding highly publicized commissioner-driven interventions.
(Others think FDA needed more visible, reform-oriented leadership willing to challenge institutional norms and inertia.)
Worth noting on the process criticism side: several frameworks did eventually move into draft guidance, formal guidance, and MAPPs.
I think a lot of the postmortem discourse blended together several different things:
• concerns about transparency, strain, and politicization tied to advisory committees and CNPV
• broader governance philosophy disagreements
• a handful of highly visible rejections
• a few overrides reiterated repeatedly
• investor frustration
• broader atmospheric claims that sometimes felt overstated relative to the publicly articulated examples
• intense media amplification (to the point where former CDER director Høeg argued that “the chaos came from the media creating stories about things being chaotic”)
So there’s the beef. Fixins' on the side.

4
1
18
4,934
Beautifully said. Thank you Doc!
The #NurOwn adcomm should become mandatory FDA training on Type II errors and how not to run an advisory committee. It was an embarrassment for the FDA and a devastating slap in the face to the ALS community.
Everything now being discussed around regulatory flexibility, totality of evidence, patient voice, individualized outcomes, and the realities of fatal diseases was ignored in that room.
And the fact that this ALS treatment is still pending after 10 years despite evidence that many ALS patients experienced meaningful benefit in a 100% fatal disease is beyond tragic.
ALS patients do not have the luxury of endless delay. They do not get time back.
Thank you for speaking out about this and pushing for a more modern, compassionate, scientifically balanced regulatory framework.
The FDA Commissioner role is open. This is a pivotal moment for American medicine — & for American patients.
Here’s what I believe the next Commissioner should stand for. Not as a wish list. As a baseline.
🔬 1. BRING BACK THE ADCOMS — AND MAKE THEM COUNT.
Advisory Committee meetings are one of the FDA’s most powerful tools for transparency. They should return in full force. Open. Public. And real.
Patients, doctors, scientists, advocates, & skeptics should all be able to speak. But if you want to speak, you fill out a financial conflict-of-interest form under penalty of perjury — & you read it out loud at the podium before you say another word. Every single person.
And if the issues are complex and the science requires more than one day, then take the time. Don’t cut people off because the schedule says so. The public deserves to see exactly how these decisions are made. Real transparency builds real trust.
⚖️ 2. STOP ASKING ONLY “IS IT SAFE ENOUGH TO APPROVE?” — START ASKING “WHAT HAPPENS IF WE DON’T?”
For rare diseases. For serious conditions with no good options. For patients who don’t have ten years to wait for traditional trials that may never be feasible.
Every regulatory decision carries two risks: the risk of approving something, and the risk of not approving it. Both are real. Both affect real people.
When traditional gold-standard trials aren’t practical, we should still be able to move with urgency — but only when paired with strong post-approval commitments and rigorous safety monitoring. We can give desperate patients a chance without abandoning scientific integrity.
🇺🇸 3. THE FDA’S ONLY CLIENT IS THE AMERICAN PATIENT. FULL STOP.
The FDA exists to serve patients — not outside interests or external pressures of any kind.
It must continue protecting the public from products that carry real, known risks but offer no meaningful clinical benefit.
At the same time, when there is credible evidence that a treatment can help patients with serious conditions, Americans and their physicians should be trusted to make informed decisions once they have complete and honest information about the risks, benefits, and alternatives.
The FDA’s job is to make sure the science is sound and the information is clear. Then let patients and doctors do what’s best for them.
These principles matter because the FDA’s decisions affect every family in this country.
Note: This is a simple social media post and not a massive policy document. The issues are FAR more nuanced, there are challenges and risks with each of the things I said above, and I recognize that. But it's intended to serve as a discussion starter. We must always strive to improve, and we can when we have open debate and dialogue.
1
2
10
624
