
Mar 24
The agitation, apathy, and depression your Alzheimer's patients show aren't random — new JCP research links distinct behavioral symptom clusters to specific brain regions, and all of them predict loss of daily function.
Abstract ----->
Objective: Neuropsychiatric symptoms (NPS) constitute a major challenge in Alzheimer disease (AD). We applied a component-based symptom paradigm by deriving Neuropsychiatric Inventory Questionnaire (NPI-Q) clusters and evaluating their longitudinal associations with regional brain volumes and functional outcomes (instrumental activities of daily living, activities of daily living [ADLs]).
Methods: Participants with AD (N=111) were from the Ontario Neurodegenerative Disease Research Initiative. NPS were assessed using the NPI-Q. Symptom clusters were identified via principal components analysis at baseline. Magnetic resonance imaging–derived volumes for 34 cortical and 9 subcortical regions were obtained annually over 3 years. Longitudinal associations between NPS clusters and functional outcomes were examined using linear mixed-effects models adjusting for age, sex, Montreal Cognitive Assessment (MoCA), education, visit number, and cholinesterase inhibitor use.
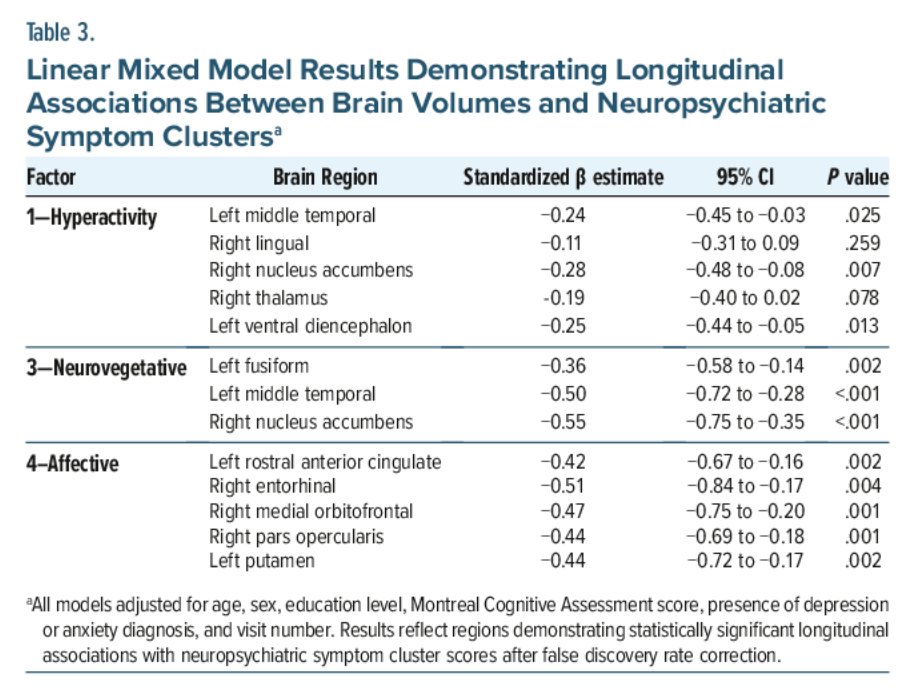
Results: Four clusters explained 62% of variance: hyperactivity (disinhibition, irritability, motor disturbance, agitation), psychosis (hallucinations, delusions, euphoria), neurovegetative (apathy, appetite), and affective (depression, anxiety, nighttime behavior). The hyperactivity cluster was associated with the left middle temporal (β=–0.24, P=.025) and right nucleus accumbens (β=–0.28, P=.007). The neurovegetative cluster was associated with the left middle temporal (β=–0.50, P<.001) and right nucleus accumbens (β=–0.55, P<.001). The affective cluster showed the strongest associations with the left rostral anterior cingulate (β=–0.42, P=.002) and right medial orbitofrontal cortex (β=–0.47, P=.001). All clusters predicted iADL outcomes; clusters 1, 3, and 4 also predicted ADL outcomes. Greater NPS burden, male sex, age, lower MoCA, and later visits predicted worse function.
Conclusion: NPS in AD separate into hyperactivity, psychosis, neurovegetative, and affective clusters, supporting a cluster-based paradigm linking co-occurring behavioral symptoms with brain structure and functional decline.
#AlzheimersDisease #Dementia #NeuropsychiatricSymptoms #GeriatricPsychiatry #Neuroscience #BrainStructure #ClinicalPsychiatry #JCP #MentalHealth #Psychiatry
4
24
1,227

Feb 18
This dude probably changed her diapers and helped her with using the toilet. Anyone who thinks this is sexual in any way has the brainstructure of a pedophile.
5
181

Feb 8
Its not sham, im not into it. People toh like it. It depends on the brainstructure. Most of there features apoeal to the lizard in you. Higher form of humans go for resource signalling.
1
1
49

How has the human brain evolved over time?
Tune in to Science Hour now to explore brain structure, mental development & the history of psychiatry.
Listen back: ow.ly/LLoV50XWpWV
#PsychiatryHistory #ScienceHour #BrainStructure
4
6
132

wot if i told u…
vat altho possibly some conditions are innate in some people, vey can also be contingent/epigenetic and hence its a very real possibility u contingently ended up in the attraction basin of the adhd mindstate-brainstructure equilibrium electron level due to said mindrape and calhoun u r a helpless frog boiling in tha water of ur society n environemt, a raped-mouse Beautiful One and in another world u r extraverted and social and embedded in a community in real life and barely look at screens an hour a week but the only difference is circumstance bc u dont have (and also do have) free will???
16 Sep 2025

do i have adhd or am i just addicted to an infinite flow of hypertuned dopamine release inducing content such that anything else pales in comparison
1
2
304

#Cognitivebehavioraltherapy can #alter #brainstructure and #boost #graymatter volume, study shows
A study of 30 depressed patients found therapy alters brain areas responsible for emotion processing, an effect similar to what is seen with medication. scitechupdates.com/cognitive…
14
17
277

24 Aug 2025
SA News #Thread | How Excessive Screen Time Affects Your Brain Health
1. Structural Brain Changes in Children
Research shows that preschoolers (ages 3–5) who spend over one hour per day on screens (without parental involvement) exhibit reduced white matter development, impacting cognitive and language abilities.
#EarlyDevelopment #BrainStructure #WhiteMatter #ChildHealth

17
608
829
5,373
19 Jun 2025
#Heading a #SoccerBall can cause subtle changes in #BrainStructure and chemistry, even without concussion or symptoms, highlighting the need to assess long-term effects on player health. doi.org/g9qpcc medicalxpress.com/news/2025-…
1
4
7
1,424

12 May 2025
Now published in the European Journal of Pain, this study reveals that (posttraumatic) #stress impacts #brainstructure differently in people with #chronicpain vs pain-free controls.
Key regions: putamen, insula, and middle cingulate.
doi.org/10.1002/ejp.70034
2
4
250


To understand if CYP with #ARFID symptoms indeed exhibit differences in #BrainStructure relative to CYP not presenting with ARFID symptoms, an international group of researchers led by Dr Michelle Sader analysed brain scans.
Read the blog to learn more. bit.ly/3Wbh4pF
2
349

2 Feb 2025
To understand if CYP with #ARFID symptoms indeed exhibit differences in #BrainStructure relative to CYP not presenting with ARFID symptoms, an international group of researchers led by Dr Michelle Sader analysed brain scans.
Read the blog to learn more. bit.ly/3Wbh4pF
1
1
157

23 Jan 2025
Hideo Kojima présente Brain Structure, l'épisode 1 du podcast doublé en français est dispo ⬇️
youtu.be/d_6GeHzE3UM
#brainstructure #podcast #KojimaProductions
2
2
5
200

21 Dec 2024
Changes to our brainstructure through wireless exposure. Taste and smell is also affected and may even differ from day to day!
1
9
15 Dec 2024
Not just the jab, also the wireless exposure from Smartphone antennas that are literally gnawing away at our brainstructure, resulting in a partial lobotomy. Many people who are electrosensitive have been going through hell in the last 3 years because of this.
3
135

9 Dec 2024
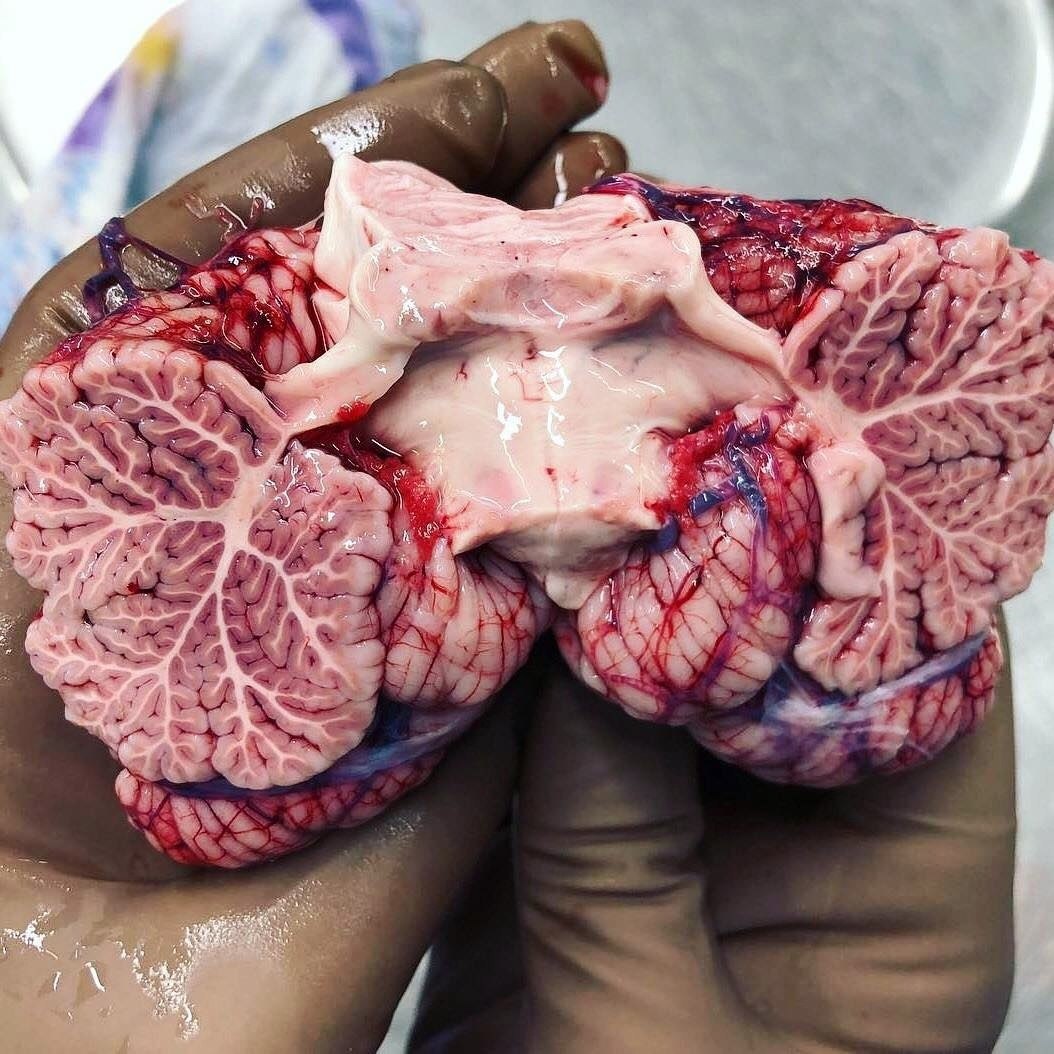
The Cerebellum and its Trees of Life
.
.
.
.
#cerebellum #brainanatomy #neuroscience #treeoflife #cerebellarfunction #brainhealth #anatomy #neurology #centralnervoussystem #medicaleducation #brainstructure #healthscience
4
134

The brain starts forming early in fetal development, with the neural tube developing into the brain and spinal cord.
As a baby grows, the brain's cells form complex networks, connecting regions responsible for motor skills, cognition, and emotions.
Brain development continues through childhood, laying the foundation for learning, memory, and behavior.
#BrainFormation #Neurodevelopment #FetalDevelopment #BrainDevelopment #Neuroscience #CognitiveGrowth #NeuralConnections #EarlyChildhood #BrainHealth #Neuroplasticity #LearningAndMemory #BrainCells #ChildDevelopment #NeuroscienceFacts #HealthyBrain #MentalGrowth #BrainBuilding #Neurogenesis #Neurobiology #MotorSkills #ChildhoodDevelopment #CognitiveScience #BrainStructure #NeuralNetwork #BrainPower #NeurodevelopmentalDisorders #BrainPlasticity #Neuroeducation #LearningBrain #EarlyBrainDevelopment #drgalen

2
36

28 Nov 2024
Better maternal diet boosts brain growth and IQ in kids 🧠🍴🍼 news-medical.net/news/202411… #MaternalDiet #BrainDevelopment #ChildNutrition #PrenatalHealth #IQ #BrainStructure #EarlyNutrition #Pregnancy #KidsHealth @AJCNutrition @nutritionorg

1
2
4
180

27 Nov 2024
久々にSpotifyでポッドキャスト「ブレインストラクチャー」の #小島秀夫監督 × #押井守監督 の神回を聴き直した
押井監督もデスストランディングをプレイしたが、繋がりたくないからオフラインで動かしていたり、ストーリー無視で配達に行かないで海岸線を走っていたり、ミュールの性能の悪いトラックをかっぱらって走らせていたところがウケる🤣荷物を溜め込んでいるミュールの襲撃を繰り返しながら商売しているってもう最高!自由過ぎる〰️😂
#brainstructure
3
24
1,061
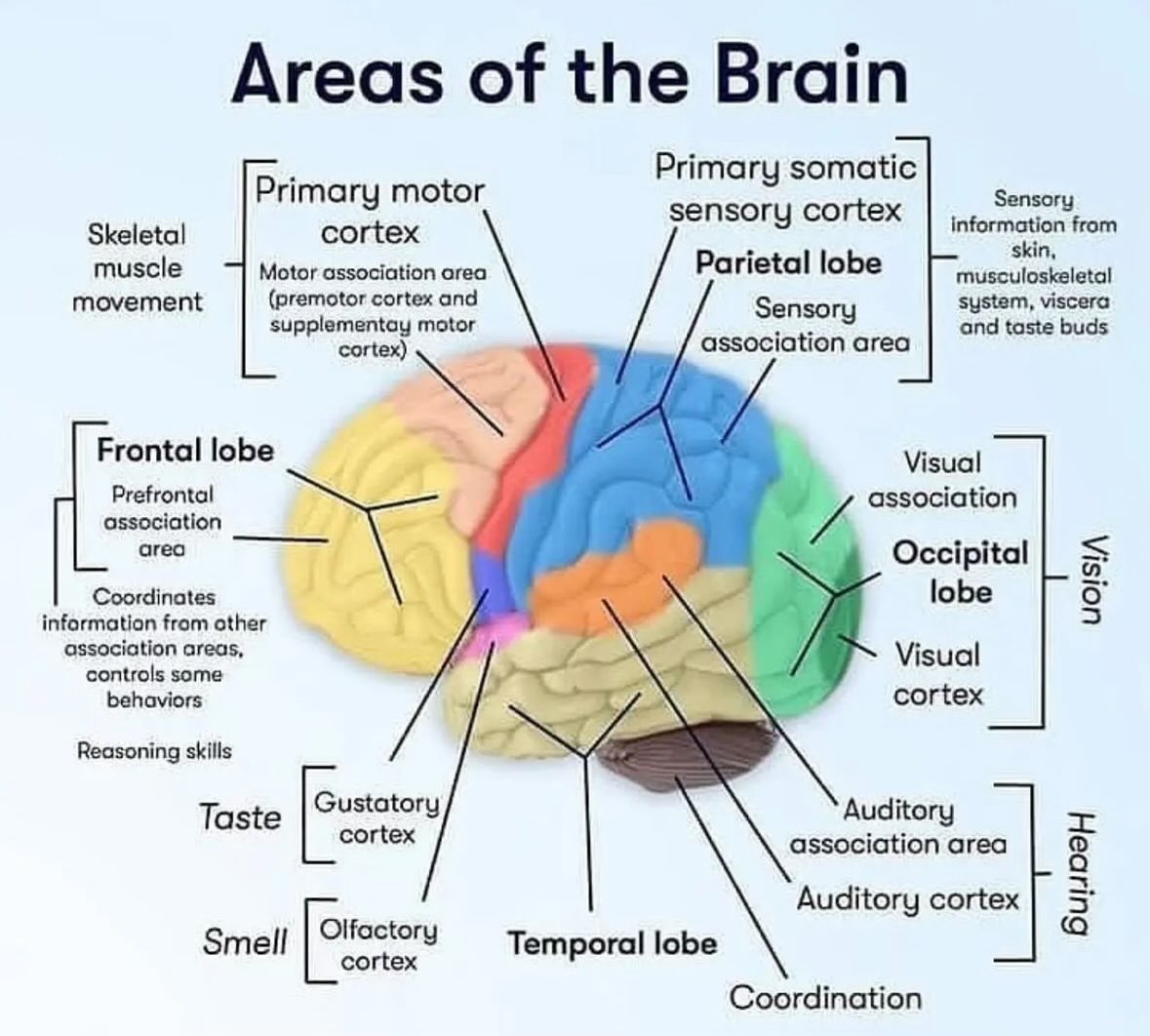
Exploring the brain's amazing regions!
Each area plays a unique role—memory, movement, emotions, and so much more. 🧠✨
#BrainRegions #Neuroscience #BrainHealth #MindMatters #MedicalEducation #BrainPower #Neuroanatomy #CognitiveFunction #HealthAwareness #Neurology #HumanBrain #MentalWellness #CortexFunction #LimbicSystem #BrainFacts #BrainScience #Cerebellum #BrainStructure #FrontalLobe #MemoryCenter #EmotionalHealth #NervousSystem #MedicalKnowledge #HealthEducation #MedStudentLife #BrainFunctionality #HealthcareProfessionals #MentalHealthAwareness #BrainResearch #drgalen

The different areas of the brain and the functions they hold
1
2
29