
Jun 14
傍腫瘍性症候群(PNS)やTreatable Dementiaの鑑別で知っておきたい検査一覧と症例解説を更新しました。CASPR2抗体・VGKC複合体・FDG-PET・PNS Care Scoreほか、Graus 2021基準まで。チェック→ wix.to/5GBiANO #認知症 #神経内科 #PNS #臨床検査
1
17

Jun 13
My biggest learning from #ICTRIMS2026 today was not about a new antibody.
It was about the patients we are probably missing.
A few practical pearls that changed how I will approach my next OPD:
• If a dementia patient has insomnia severe enough to trouble the family, pause before calling it Alzheimer’s disease.
• Hyponatremia memory loss brief unexplained movements is not a lab abnormality plus dementia. It may be LGI1 until proven otherwise.
• A patient labelled as rapid Alzheimer’s who deteriorates over weeks to months deserves an autoimmune workup.
• New psychiatric symptoms after HSV encephalitis are not always psychiatric. Sometimes the virus leaves, but the immune system stays behind.
• Sleep history may be as valuable as MRI.
RBD, agrypnia, status dissociatus, unexplained limb movements during sleep can be autoimmune clues.
• Dementia biomarkers can lie.
A patient may show an Alzheimer’s-like CSF profile and still have a treatable autoimmune encephalitis.
• Antibody positivity is easy.
Phenotype matching is hard.
The future belongs to clinicians who can do both.
• Central hypoventilation in anti-NMDAR is not an ICU curiosity.
If you miss it, the patient may stop breathing before the diagnosis is obvious.
Perhaps the most important slide of the day was not the one showing antibodies.
It was the slide showing the red flags.
Because autoimmune dementia is not diagnosed by finding an antibody.
It is diagnosed by noticing that the story does not behave like ordinary dementia.
The lesson:
When the disease progresses too fast,
when cognition fluctuates,
when sleep becomes bizarre,
when seizures hide in plain sight,
don’t ask:
What antibody should I send?
Ask:
Am I looking at a treatable disease pretending to be a degenerative one?
That question may save more neurons than any biomarker.
Learning from #ICTRIMS2026
#Neurology #Neuroimmunology #AutoimmuneEncephalitis #LGI1 #NMDAR #CASPR2 #Dementia #CognitiveNeurology #MedTwitter #NeuroTwitter
3
10
37
1,625
Jun 12
A valuable learning from #ICTRIMS2026:
In neuroimmunology, don’t just ask:
Which antibody is positive?
Ask:
Which IgG subclass is driving the disease?
IgG1 diseases (AQP4, MOGAD, NMDAR):
→ Complement activation
→ Inflammation
IgG4 diseases (LGI1, CASPR2, MuSK-MG, NF155):
→ Protein interaction disruption
→ Often less responsive to IVIg
→ Frequently excellent responders to rituximab
Mechanism predicts treatment response.
Understanding antibody biology is increasingly as important as identifying the antibody itself.
#Neurology #Neuroimmunology #AutoimmuneEncephalitis #NMOSD #MOGAD #MyastheniaGravis
11
30
1,254

🧠🔬 Excellent neuroimaging case!
The MRI appears to show bilateral mesial temporal (hippocampal-amygdalar) FLAIR hyperintensities with predominant limbic system involvement, a pattern highly suggestive of Limbic Encephalitis.
📌 Leading Differentials: 🦠 HSV-1 Encephalitis — the critical diagnosis that must be excluded immediately, given its predilection for the temporal lobes and the need for urgent treatment.
🧬 Autoimmune Limbic Encephalitis — particularly Anti-NMDA, LGI1, CASPR2, and GABA-B receptor antibody-associated disease.
⚡ Post-ictal temporal lobe signal changes,
🦠 HHV-6 encephalitis, and
🧠 Infiltrative neoplasm/glioma remain important considerations.
🔍 Key MRI Pearl:
Symmetric bilateral mesial temporal involvement tends to favor autoimmune or limbic encephalitis, whereas asymmetric temporal lobe involvement with edema and hemorrhagic changes classically points toward HSV encephalitis.
🧪 Next essential steps: ✅ CSF analysis with HSV-PCR
✅ Autoimmune encephalitis antibody panel
✅ EEG for temporal lobe epileptiform activity
✅ Early empiric IV acyclovir while awaiting results if HSV remains a possibility
💡 In neurology, bilateral medial temporal FLAIR hyperintensities should immediately trigger a “Limbic Encephalitis Syndrome” workup until proven otherwise. 🧠⚡🔬💉 #Neuroradiology #Neurology #LimbicEncephalitis #HSVEncephalitis #MRI #MedEd
4
35
4,382

🧵🧠⚠️ 𝗘𝗻𝗰𝗲𝗳𝗮𝗹𝗶𝘁𝗶𝘀: 𝘂𝗻𝗮 𝗲𝗺𝗲𝗿𝗴𝗲𝗻𝗰𝗶𝗮 𝗻𝗲𝘂𝗿𝗼𝗹𝗼́𝗴𝗶𝗰𝗮 𝗴𝗹𝗼𝗯𝗮𝗹 𝗱𝗼𝗻𝗱𝗲 𝗲𝗹 𝘁𝗶𝗲𝗺𝗽𝗼 𝘀𝗶́ 𝗰𝗮𝗺𝗯𝗶𝗮 𝗱𝗲𝘀𝗲𝗻𝗹𝗮𝗰𝗲𝘀 🚨
@TheLancet @TheLancetNeuro
👇🏼👇🏼👇🏼👇🏼
📑🔗🔑🔓
t.me/ClubCrit
⬇️⬇️⬇️⬇️
🧵👇
Este 𝘚𝘦𝘮𝘪𝘯𝘢𝘳 de 𝗟𝗮𝗻𝗰𝗲𝘁 𝟮𝟬𝟮𝟲 deja un mensaje central: la encefalitis sigue causando una enorme carga de discapacidad y muerte, pero muchas formas son 𝙥𝙤𝙩𝙚𝙣𝙘𝙞𝙖𝙡𝙢𝙚𝙣𝙩𝙚 𝙩𝙧𝙖𝙩𝙖𝙗𝙡𝙚𝙨 si se reconocen temprano.
📌 La revisión estima 𝟱𝟬𝟬,𝟬𝟬𝟬–𝟭.𝟱 𝙢𝙞𝙡𝙡𝙤𝙣𝙚𝙨 de casos/año en el mundo y ~𝟭𝟬𝟬,𝟬𝟬𝟬 𝙢𝙪𝙚𝙧𝙩𝙚𝙨 anuales.
📌 En 𝙃𝙎𝙑 𝙚𝙣𝙘𝙚𝙛𝙖𝙡𝙞𝙩𝙞𝙨, iniciar 𝙖𝙘𝙞𝙘𝙡𝙤𝙫𝙞𝙧 𝙥𝙧𝙚𝙘𝙤𝙯 reduce la mortalidad de ~𝟳𝟬% a ~𝟮𝟬%.
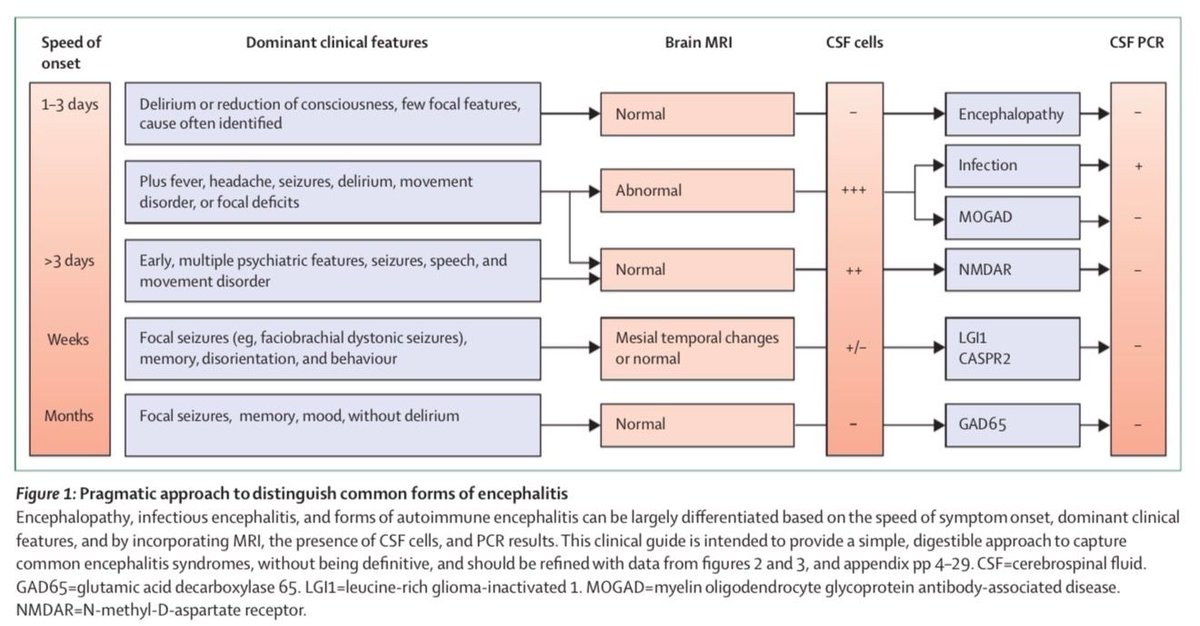
🔍🧠 𝙀𝙡 𝙥𝙧𝙞𝙢𝙚𝙧 𝙥𝙖𝙨𝙤 𝙥𝙧𝙖́𝙘𝙩𝙞𝙘𝙤: 𝙙𝙞𝙨𝙩𝙞𝙣𝙜𝙪𝙞𝙧 𝙚𝙣𝙘𝙚𝙛𝙖𝙡𝙤𝙥𝙖𝙩𝙞́𝙖 𝙙𝙚 𝙚𝙣𝙘𝙚𝙛𝙖𝙡𝙞𝙩𝙞𝙨
La revisión remarca que no todo paciente confuso tiene encefalitis 😵💫
👉 𝙀𝙣𝙘𝙚𝙛𝙖𝙡𝙤𝙥𝙖𝙩𝙞́𝙖: disfunción cerebral difusa, a menudo tóxica/metabólica, con RM y LCR frecuentemente normales
👉 𝙀𝙣𝙘𝙚𝙛𝙖𝙡𝙞𝙩𝙞𝙨: además de alteración mental, suele acompañarse de:
🌡️ fiebre
⚡ crisis de novo
🎯 déficits focales
🧪 pleocitosis en LCR
🩻 hiperintensidades en RM
🦠🤖 𝙃𝙤𝙮 𝙝𝙖𝙮 𝙦𝙪𝙚 𝙥𝙚𝙣𝙨𝙖𝙧 𝙚𝙣 𝙥𝙖𝙧𝙖𝙡𝙚𝙡𝙤: 𝙞𝙣𝙛𝙚𝙘𝙘𝙞𝙤𝙨𝙖 𝙮 𝙖𝙪𝙩𝙤𝙞𝙣𝙢𝙪𝙣𝙚
Gran cambio conceptual del paper 🔥
La encefalitis 𝙖𝙪𝙩𝙤𝙞𝙣𝙢𝙪𝙣𝙚 ya es 𝙖𝙡 𝙢𝙚𝙣𝙤𝙨 𝙩𝙖𝙣 𝙛𝙧𝙚𝙘𝙪𝙚𝙣𝙩𝙚 como la infecciosa en países de altos ingresos.
👉 En la práctica, eso significa que ante una encefalitis aguda hay que estudiar 𝙖𝙢𝙗𝙖𝙨 𝙧𝙪𝙩𝙖𝙨 𝙖𝙡 𝙢𝙞𝙨𝙢𝙤 𝙩𝙞𝙚𝙢𝙥𝙤:
🦠 PCR/serologías infecciosas
🧠 autoanticuerpos en suero y LCR
Enfoque útil: sospecha clínica → LCR urgente → RM → EEG → pruebas dirigidas infecciosas y autoinmunes en paralelo.
💉⏱️ 𝙋𝙚𝙧𝙡𝙖 𝙘𝙧𝙞́𝙩𝙞𝙘𝙖: 𝙚𝙡 𝙇𝘾𝙍 𝙙𝙚𝙗𝙚 𝙤𝙗𝙩𝙚𝙣𝙚𝙧𝙨𝙚 𝙥𝙧𝙤𝙣𝙩𝙤, 𝙮 𝙚𝙡 𝙖𝙘𝙞𝙘𝙡𝙤𝙫𝙞𝙧 𝙣𝙤 𝙙𝙚𝙗𝙚 𝙧𝙚𝙩𝙧𝙖𝙨𝙖𝙧𝙨𝙚
✅ si sospechas encefalitis aguda, haz 𝙥𝙪𝙣𝙘𝙞𝙤́𝙣 𝙡𝙪𝙢𝙗𝙖𝙧 𝙪𝙧𝙜𝙚𝙣𝙩𝙚 salvo pocas contraindicaciones claras
✅ y después, o si el LCR se retrasa, inicia 𝙖𝙘𝙞𝙘𝙡𝙤𝙫𝙞𝙧 𝙄𝙑 𝙚𝙢𝙥𝙞́𝙧𝙞𝙘𝙤
📌 Recomiendan considerar además cobertura para 𝙢𝙚𝙣𝙞𝙣𝙜𝙤𝙚𝙣𝙘𝙚𝙛𝙖𝙡𝙞𝙩𝙞𝙨 𝙗𝙖𝙘𝙩𝙚𝙧𝙞𝙖𝙣𝙖 cuando corresponda.
📌 El LCR tardío sigue siendo un problema frecuente y empeora oportunidades terapéuticas.
🦠 𝙇𝙤𝙨 𝙛𝙚𝙣𝙤𝙩𝙞𝙥𝙤𝙨 𝙞𝙣𝙛𝙚𝙘𝙘𝙞𝙤𝙨𝙤𝙨 𝙨𝙞́ 𝙖𝙮𝙪𝙙𝙖𝙣 𝙖 𝙤𝙧𝙞𝙚𝙣𝙩𝙖𝙧 𝙙𝙞𝙖𝙜𝙣𝙤́𝙨𝙩𝙞𝙘𝙤
La revisión resume varios patrones clínicos muy útiles:
🧠 𝙃𝙎𝙑-𝟭: la causa esporádica más común en países de altos ingresos; suele afectar lóbulos temporales
🦠 𝙑𝙕𝙑: piensa en vasculopatía y EVC isquémico/hemorrágico
🦟 𝙒𝙚𝙨𝙩 𝙉𝙞𝙡𝙚 𝙫𝙞𝙧𝙪𝙨: puede dar 𝙥𝙖𝙧𝙖́𝙡𝙞𝙨𝙞𝙨 𝙛𝙡𝙖́𝙘𝙞𝙙𝙖 𝙖𝙜𝙪𝙙𝙖
🦟 𝙅𝙖𝙥𝙖𝙣𝙚𝙨𝙚 𝙚𝙣𝙘𝙚𝙥𝙝𝙖𝙡𝙞𝙩𝙞𝙨 𝙫𝙞𝙧𝙪𝙨: predilección por 𝙜𝙖𝙣𝙜𝙡𝙞𝙤𝙨 𝙗𝙖𝙨𝙖𝙡𝙚𝙨/𝙩𝙖́𝙡𝙖𝙢𝙤 y trastornos del movimiento
🧒 𝙀𝙣𝙩𝙚𝙧𝙤𝙫𝙞𝙧𝙪𝙨: gran peso en encefalitis pediátrica
🧠✨ 𝙀𝙣 𝙖𝙪𝙩𝙤𝙞𝙣𝙢𝙪𝙣𝙚, 𝙚𝙡 𝙥𝙚𝙧𝙛𝙞𝙡 𝙘𝙡𝙞́𝙣𝙞𝙘𝙤 𝙢𝙪𝙘𝙝𝙖𝙨 𝙫𝙚𝙘𝙚𝙨 “𝙙𝙚𝙡𝙖𝙩𝙖” 𝙚𝙡 𝙖𝙣𝙩𝙞𝙘𝙪𝙚𝙧𝙥𝙤
Otro gran valor del paper 👇
👉 𝙉𝙈𝘿𝘼𝙍: inicio en días, psiquiatría florida temprana crisis movimientos anormales, sobre todo en jóvenes
👉 𝙇𝙂𝙄𝟭: adultos mayores, crisis focales frecuentes, amnesia, desorientación y 𝙘𝙤𝙣𝙫𝙪𝙡𝙨𝙞𝙤𝙣𝙚𝙨 𝙙𝙞𝙨𝙩𝙤́𝙣𝙞𝙘𝙖𝙨 𝙛𝙖𝙘𝙞𝙤𝙗𝙧𝙖𝙦𝙪𝙞𝙖𝙡𝙚𝙨
👉 𝘾𝘼𝙎𝙋𝙍𝟮: más disautonomía, sueño y nervio periférico
👉 𝙈𝙊𝙂: más frecuente en niños, RM anormal, encefalitis cortical/subcortical
👉 𝙂𝘼𝘿𝟲𝟱: epilepsia temporal progresiva, curso más subagudo
🎯 𝙀𝙡 𝙜𝙧𝙖𝙣 𝙩𝙖𝙠𝙚-𝙝𝙤𝙢𝙚: 𝙚𝙣𝙘𝙚𝙛𝙖𝙡𝙞𝙩𝙞𝙨 = 𝙧𝙚𝙘𝙤𝙣𝙤𝙘𝙚𝙧 𝙩𝙚𝙢𝙥𝙧𝙖𝙣𝙤, 𝙩𝙧𝙖𝙩𝙖𝙧 𝙩𝙚𝙢𝙥𝙧𝙖𝙣𝙤 𝙮 𝙥𝙚𝙣𝙨𝙖𝙧 𝙚𝙣 𝙨𝙚𝙘𝙪𝙚𝙡𝙖𝙨 𝙡𝙖𝙧𝙜𝙖𝙨
La revisión cierra con 3 mensajes potentes:
✅ 𝙖𝙘𝙞𝙘𝙡𝙤𝙫𝙞𝙧 𝙥𝙧𝙚𝙘𝙤𝙯 en sospecha de encefalitis infecciosa
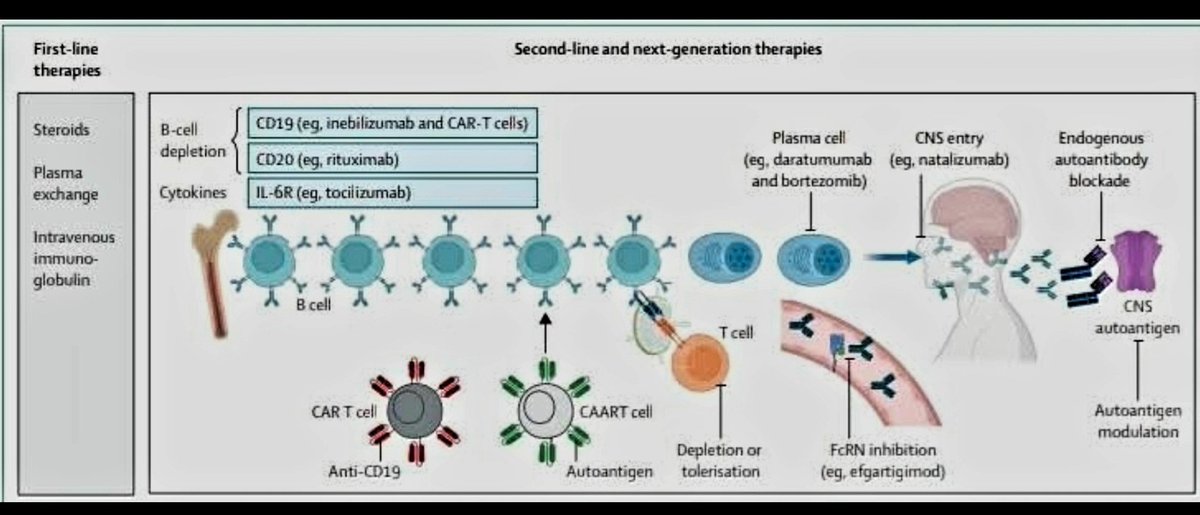
✅ 𝙞𝙣𝙢𝙪𝙣𝙤𝙩𝙚𝙧𝙖𝙥𝙞𝙖 𝙥𝙧𝙚𝙘𝙤𝙯 en encefalitis autoinmune mejora desenlaces
✅ la mayoría de pacientes quedan con secuelas cognitivas, físicas y psicosociales importantes
➡️En autoinmune ya existen múltiples líneas de inmunoterapia, pero en ambos grupos la carga residual sigue siendo alta.
🔥 Mensaje final: en encefalitis, el error más costoso no es pedir “demasiadas pruebas”; es 𝙣𝙤 𝙨𝙤𝙨𝙥𝙚𝙘𝙝𝙖𝙧𝙡𝙖 𝙖 𝙩𝙞𝙚𝙢𝙥𝙤, retrasar LCR/aciclovir o no considerar el componente autoinmune.
‼️Si te sirve: ❤️ Me gusta | 🔁 Repost | ➕ Follow para más👇🏼👇🏼👇🏼👇🏼
📚📖#ClubCrit👨🏻⚕️👨🏻🏫🧠🫶
📚📖 Más en el blog 👉 [buff.ly/6up7pdx]
#Encefalitis #NeurocriticalCare #FOAMed #FOAMcc
#ClubCrit #Encefalitis #NeurocriticalCare #Neurología #Encefalopatía #LCR #MRI #AutoimmuneEncephalitis #HSV #NMDAR #Acyclovir #LumbarPuncture #EmergencyNeurology #HSVencephalitis #WestNile #JapaneseEncephalitis #VZV #LGI1 #NMDAR #MOGAD #GAD65 #POCUS #FOAMed #FOAMcc #CriticalCare #CriticalCare #CuidadoCrítico #MedTwitter #CritCare #icu #intensivecare #diagnosis #management #UCI #MedicinaBasadaEnEvidencia #MedEd #MedX #IntensiveCare #MedIntensiva #MedXCommunity #MedED #ICUmanagement #MustRead #LecturaRecomendada

12
39
1,471

May 17
CME INDIA Clinical Pearls
Encephalitis 2026: Infectious vs Autoimmune Brain Inflammation — “Treat Early, Test Smart, Avoid Misdiagnosis”
1. Encephalitis is a neurological emergency, not a diagnostic curiosity. Any patient with fever, altered sensorium, seizures, new psychiatric symptoms, focal deficits, movement disorder, or rapidly evolving cognitive decline should be approached as possible encephalitis until proven otherwise. The Lancet Seminar emphasises encephalitis as a global emergency with substantial preventable morbidity and mortality.
2. First clinical split: infectious encephalitis vs autoimmune encephalitis. Infectious encephalitis often has fever, acute onset, CSF pleocytosis, and viral prodrome; autoimmune encephalitis may present with psychiatric symptoms, seizures, memory loss, dyskinesias, autonomic instability, or faciobrachial dystonic seizures. But overlap is common, so clinical impression must be supported by CSF, PCR, MRI, EEG, and antibody testing.
3. Do not wait for PCR before starting acyclovir when HSV encephalitis is possible. HSV encephalitis remains the “must-not-miss” treatable viral encephalitis. Early IV acyclovir improves outcome, and delay increases neurological disability and death. UK viral encephalitis guidance recommends IV aciclovir for proven HSV encephalitis for 14–21 days with repeat CSF HSV PCR at the end of therapy.
4. Temporal lobe signal on MRI is HSV until proven otherwise. Fever, seizures, behavioural change, aphasia, or memory disturbance with medial temporal/frontal involvement should trigger immediate acyclovir. A normal early CT does not exclude encephalitis; MRI is the imaging modality of choice when available.
5. CSF is the diagnostic backbone. Send opening pressure, cells, protein, glucose, Gram stain/culture, HSV/VZV/enterovirus PCR as locally relevant, and paired serum/CSF autoimmune antibody panels. CSF antibody testing is especially important for NMDAR-antibody encephalitis; serum-only low-titre antibodies can mislead.
6. EEG helps when the patient “looks psychiatric” but the brain is inflamed. Diffuse slowing supports encephalopathy; epileptiform activity or non-convulsive status epilepticus may explain persistent altered sensorium. EEG is particularly useful when seizures are subtle or when MRI is initially normal.
7. Autoimmune encephalitis is treatable, but overdiagnosis is dangerous. The Lancet Seminar specifically warns about frequent misdiagnosis of autoimmune encephalitis. Do not label autoimmune encephalitis solely because of psychiatric symptoms or a weakly positive serum antibody; require a compatible syndrome, objective CNS inflammation, and exclusion of mimics.
8. Recognise classic autoimmune patterns. Anti-NMDAR encephalitis often presents with psychiatric symptoms, seizures, dyskinesias, speech disturbance, autonomic instability, and reduced consciousness. LGI1 encephalitis often presents in older adults with faciobrachial dystonic seizures, memory impairment, hyponatraemia, and medial temporal MRI changes. CASPR2 may associate with Morvan syndrome, neuropathic pain, insomnia, dysautonomia, and thymoma.
9. Start immunotherapy early when autoimmune encephalitis is probable, but not blindly. Once infection is reasonably covered or excluded, first-line treatment usually includes high-dose corticosteroids, IVIG, or plasma exchange. Rituximab, cyclophosphamide, or other targeted approaches may be needed in refractory disease, ideally with neurology input.
10. In India, do not forget region-specific infectious causes. Japanese encephalitis, dengue, scrub typhus, tuberculosis, malaria, leptospirosis, chikungunya, rabies, Nipah in relevant geography, and post-infectious immune encephalitis should remain in the differential. Travel, season, vaccination history, animal exposure, mosquito exposure, and local outbreaks matter.
Next.....
sciencedirect.com/science/ar…
1
3
10
566
Apr 30
Two patients walk into your OPD.
Patient A:
Brief face-arm jerks, memory slips, sodium 126.
Patient B:
Insomnia, myokymia, cramps, sweating, confusion, weight loss.
Both may have autoimmune neurological disease.
One is LGI1.
One is CASPR2.
The diagnosis begins with the pattern.
A clinician’s case-board:#Neurotwitter #Medtwitter

2
5
27
1,547

Apr 16
Neurology consult → suspicion of peripheral nerve hyperexcitability.
- Test sent: VGKC antibodies
- Result : Positive for
• Anti-CASPR2
• Anti-LGI1
Thus came the diagnosis : Peripheral Nerve Hyperexcitability Syndrome, variant : Morvan Syndrome.
2
38

Apr 11
65M, 痙攣発症の側頭葉病変
両側扁桃体〜海馬、島で対称性のT2延長
増強効果ほぼなし, ASL 上がってない?
DWI高信号
非特異的な辺縁系脳炎すぎるが、ヘルペスにしては対称性すぎるから、自己免疫系?
A. Caspr2抗体関連
▫︎ 亜急性
▫︎ 50%に胸腺腫合併
▫︎ 睡眠障害との関連
1
6
617

I have some interesting blood tests coming up. I might finally find out what the lesion in my back really is. Crazy I have to figure it out by myself. Also there was an indication in Amatica’s RNA test I could have CASPR2 autoantibodies, which cause seizures that I have.
1
23
1,188

After a thorough examination, Dr. Tebartz van Elst found autoantibodies in her blood that target a brain protein called contactin-associated protein-like 2 (CASPR2).
CASPR2 is found in the CNS and is crucial to the transmission of neural signals.
Alina was treated with intravenous cortisone, and she "got [her] life back” almost immediately.
Alina could jog a few days after treatment for the first time in nearly a decade.
3
15
191
19,677

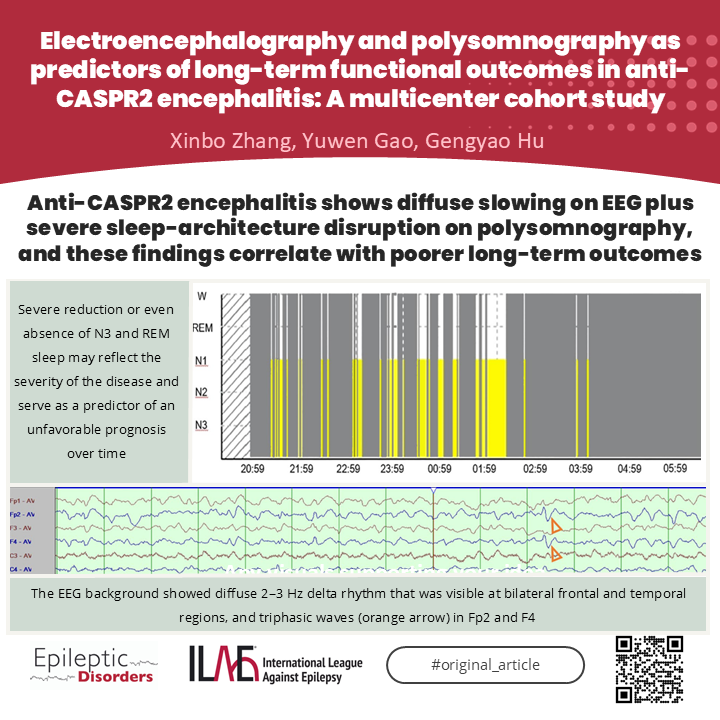
Anti-CASPR2 encephalitis on EEG many patients show (DSWA) and IED , reflecting widespread cortical dysfunction. Importantly, diffuse slowing and absence of deep (N3) sleep may signal a worse prognosis. CLICK THIS TO READ LINK
onlinelibrary.wiley.com/doi/…
7
33
1,545

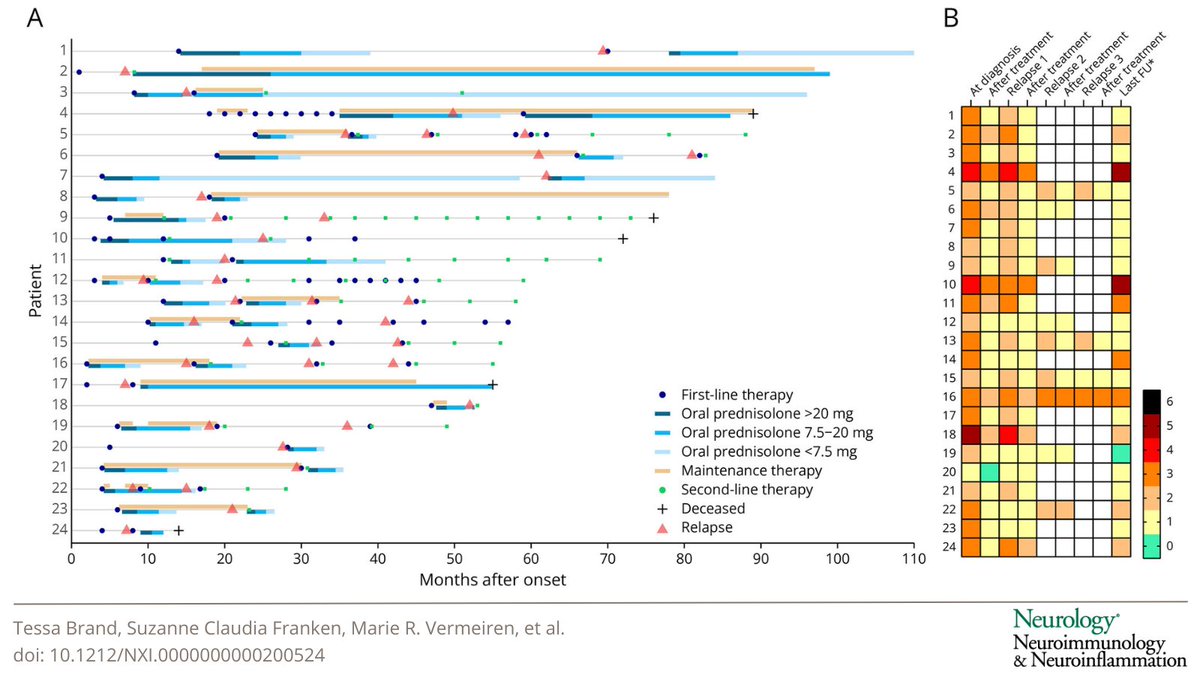
This study shows a twofold higher relapse rate in anti-CASPR2 disease compared with previous studies. Prolonged immunotherapy beyond the acute stage seems needed in patients prone to relapse to prevent further relapses: hubs.la/Q03ZHKXx0
2
12
1,415

29 Dec 2025
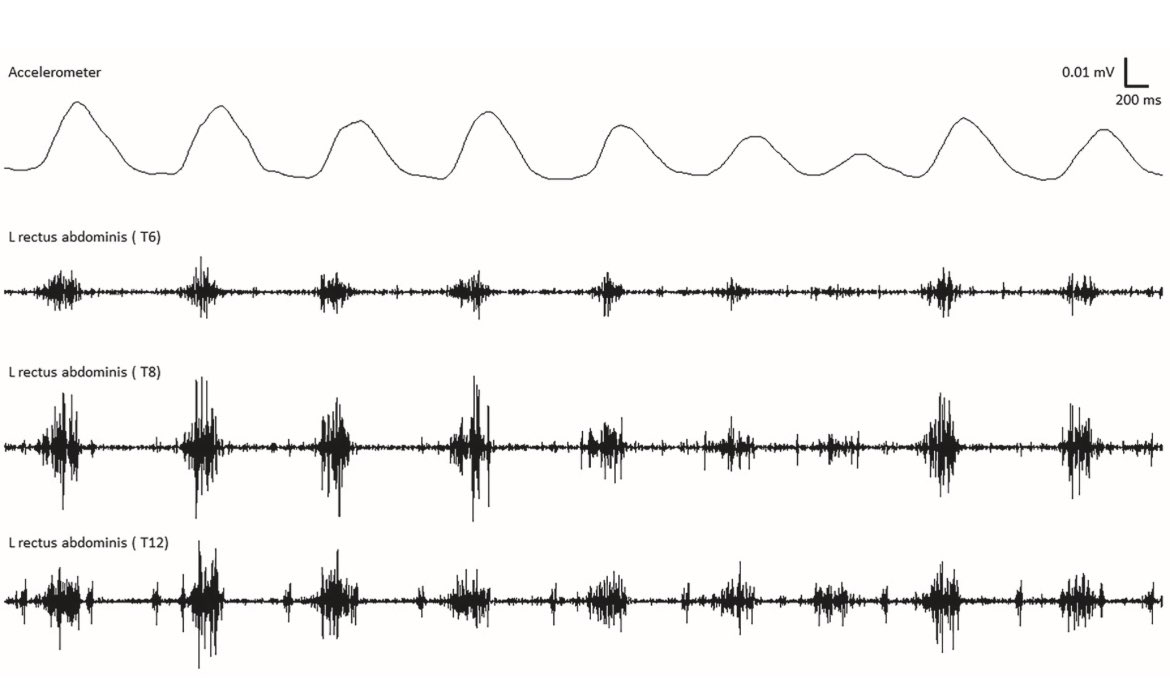
Movement disorders rounds: Neurophysiological findings in abdominal movements in CASPR2 encephalitis
#abdominalmovements #CASPR2
#encephalitis #autoimmune #neurophysiology
prd-journal.com/article/S135…
@PRDAssociation
Expert commentary
prd-journal.com/article/S135…
1
5
545

21 Dec 2025
1/4 🧵 Nuevo paper en Neuroimmunol Neuroinflamm (Brand et al. 2026) redefine el manejo de anti-CASPR2.
N=44 cohorte nacional.
Hallazgo crítico: Tasa de recaída del 60% (vs 25-30% histórico).
Esto exige vigilancia a largo plazo. 📉

1
2
55

24 Nov 2025
急に「直前の出来事を覚えられなくなる」のを一過性全健忘(TGA)といい、ある日突然、同じ質問を何度も繰り返したりして救急に来たりします。ほっとけば治るんですが、このTGAの症状が稀に脳炎の初期症状ってことはあるんですね
どの抗体があるのかな?と調べると
・AMPAR抗体脳炎
・LGI1 抗体脳炎
・CASPR2 抗体脳炎
・GABAbR抗体脳炎
・NMDAR抗体脳炎
・GAD65抗体関連
・Ma2 などのパラネオ
いや、ほぼ全部かい笑
結局、辺縁系脳炎のタイプになりうる脳炎なら、TGAと誤認するかもしれないねって話
#脳炎メモ
2
10
67
14,626

23 Nov 2025
▶️Morvan syndrome is an autoimmune peripheral nerve hyperexcitability disorder.
▶️It features neuromyotonia, autonomic dysfunction, and severe insomnia.
•It involves both the PNS and CNS.
•Strongly associated with CASPR2 (± LGI1) antibodies and sometimes thymoma.
6
190

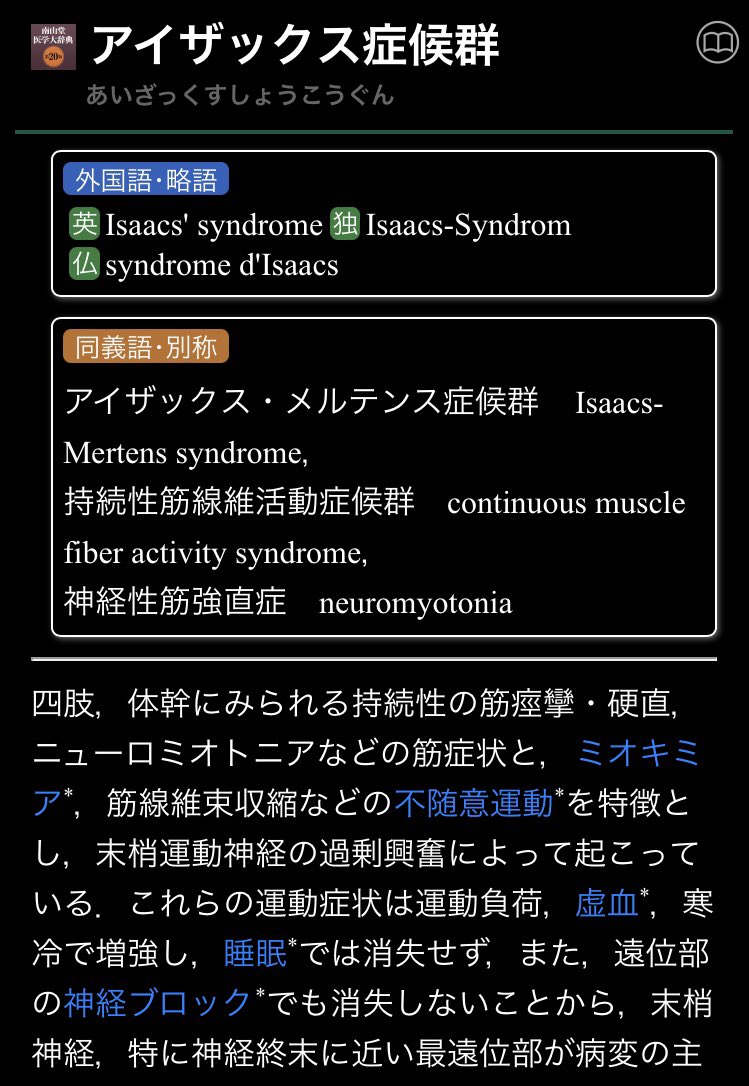
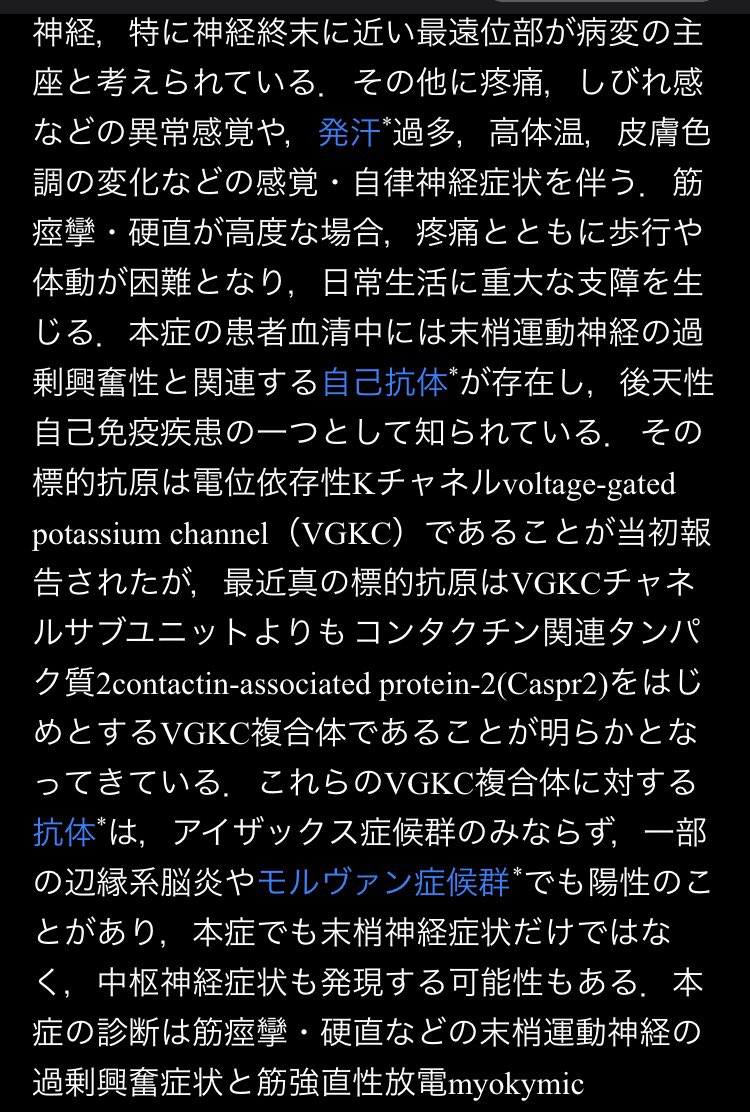
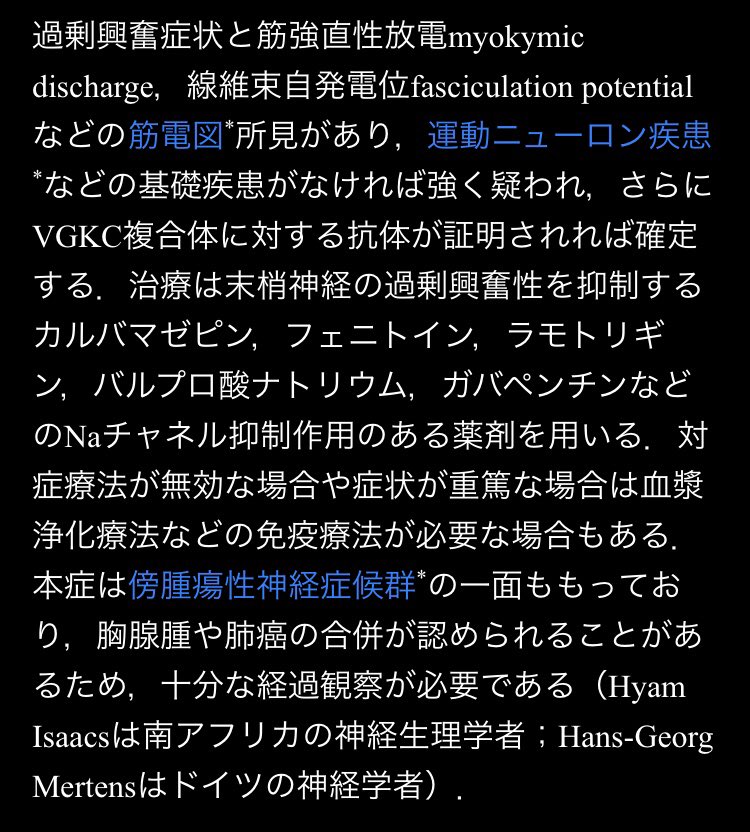
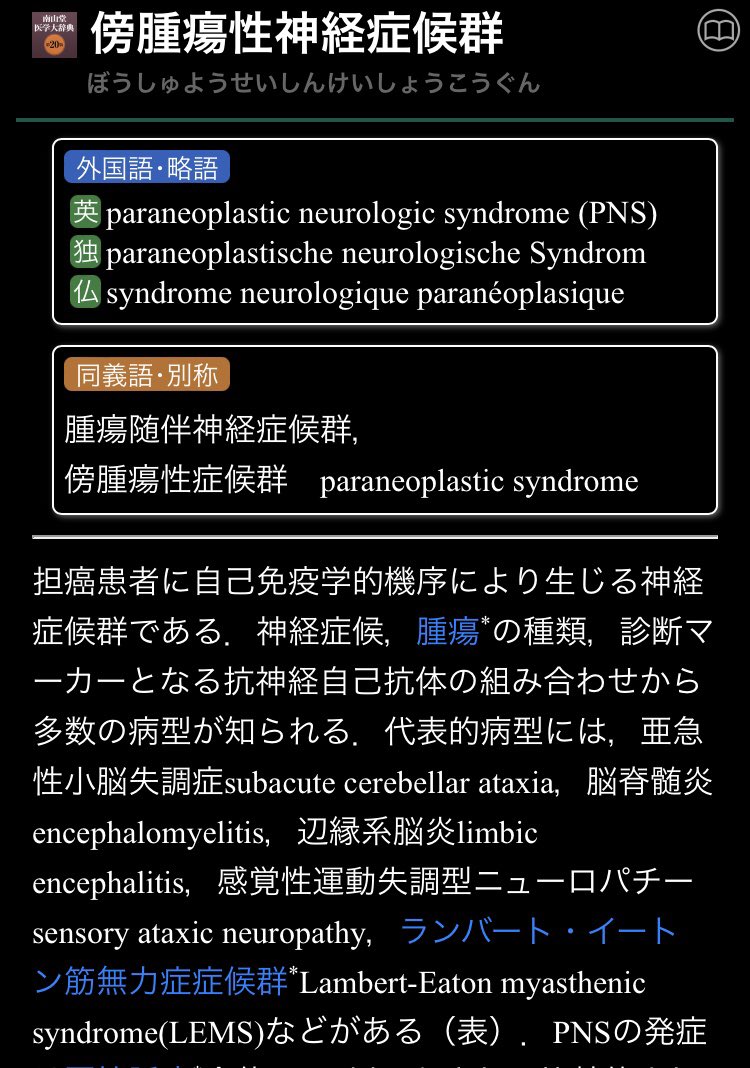
胸腺腫の併発か…
"筋肉がピクピク、強い痛みも ~アイザックス症候群~" - 時事メディカル
神経を過剰興奮させる自己抗体として「LGI―1抗体」「CASPR2抗体」などが発見されている。
l.smartnews.com/m-6C2tEOEE/G…
6
589

8 Nov 2025
🏥🧠🔥 Actualización 2025 con enfoque en terapia intensiva 🆓 Open Access
📖 DEFINICIONES:
▷ Estado epiléptico (EE): ≥5 minutos de actividad epiléptica continua o crisis repetitivas sin recuperación de la conciencia entre ellas (anteriormente actividad epiléptica o crisis repetitivas >30 minutos).
▷ Estado epiléptico convulsivo (EEC): crisis epilépticas con alteración del nivel de consciencia que cumplen los criterios de EE.
▷ Estado epiléptico no convulsivo (EENC): se define como un estado epiléptico sin un componente motor prominente (clínicamente evidente) y depende de los hallazgos del electroencefalograma (EEG). En ocasiones existe un cambio en el estado mental o el comportamiento respecto al estado basal.
▷ Estado epiléptico refractario (EER): EE que no responde al tratamiento farmacológico inicial (fármaco anticrisis [FAC] benzodiazepínico y otro no benzodiazepínico).
▷ Estado epiléptico superrefractario (EESR): EE que persiste o reaparece tras 24 horas de infusión adecuada de agentes intravenosos (sospechar encefalitis autoinmune).
▷ Trastorno de ataque no epiléptico (TANE): crisis disociativas no epilépticas. Es una afección en la que las personas experimentan episodios que se asemejan a las crisis epilépticas, pero sin una causa física relacionada con una actividad eléctrica anormal en el cerebro (anteriormente crisis disociativas, no epilépticas psicógenas, no epilépticas, pseudocrisis o conversivas).
💉 MANEJO POR TIEMPO:
➤ ETAPA 1 (0 min): Estabilización y medidas de soporte, si fracasa ↓
➤ ETAPA 2 (0-15 min): Lorazepam 4mg IV cada 5 a 10 min, si fracasa ↓
➤ ETAPA 3 (15-30 min): Levetiracetam 60mg/kg (max 4.5g), Fenitoina 20mg/kg (max 2g) o valproato 40 mg/kg (max 3g), si fracasa ↓
➤ ETAPA 4 (30-60 min): Sedación propofol 4 mg/kg/h y/o midazolam 0.1-0.2 mg/kg en bolo y posteriormente 0.05-0.5 mg/kg/h, si fracasa ↓
➤ ETAPA 5 (>60 min): EEG continua, terapia combinada de FAC, aumentar sedación y abordaje de escenarios atípicos
🤔 ¿Cuándo considerar el ingreso a UCI?
1️⃣ EE que requiere intubación y VMI
2️⃣ El nivel de consciencia permanece disminuido después de finalizar las crisis e impiden la capacidad de proteger su vía aérea
3️⃣ Las alteraciones fisiológicas y metabólicas del paciente son significativas y requieren monitorización.
🎯 METAS DE MANEJO Y ABORDAJE
✅ En VMI: Volumen corriente 6–8 ml/kg de peso ideal, presión plateau < 30 cmH₂O, PEEP >5 cmH20, Pa02 >8 kPa
✅ PAM >65 mmHg
✅ No suspender sedaciones diarias de "rutinaria" → reducción gradual
✅ Nutrición enteral precoz (dentro de las primeras 48 h)
✅ Descartar meningitis o encefalitis (PCR, Hemograma, gasometría, lactato y punción lumbar)
✅ Análisis toxicológico
✅ Radiografía de tórax buscando signos de aspiración o TAC de craneo si no hay etiología desencadenante clara
✅ EEG de ingreso
✅ Creatina quinasa (CK) ± triglicéridos si se utiliza propofol en dosis altas (>4 mg/kg/h) o si hay sospecha de rabdomiólisis
🧪 EXÁMENES EN ESCENARIOS ESPECIALES O ATÍPICOS
¿Vasculitis? → Anticuerpos antinucleares (ANA), antígenos nucleares extraíbles (ENA) y anticuerpos anticitoplasma de neutrófilos (ANCA)
¿Encefalitis autoinmune? → Anticuerpos anti: NMDAR, LGI1, CASPR2, GAD y TPO
🧠 ELECTROENCEFALOGRAFÍA CONTINUA: debe continuarse durante al menos 24 horas después de la resolución de la actividad epiléptica, mientras el paciente esté sedado.
🧩 Si no hay mejoría, considere la posibilidad de una encefalitis autoinmune, estado epiléptico refractario mediado por el sistema inmunitario, estado epiléptico refractario de inicio reciente (NORSE) o síndrome epiléptico relacionado con infección febril (FIRES).
▷ Metilprednisolona IV 1 g/día por 3 días
▷ Inmunoglobulina intravenosa (IGIV) o plasmaféresis
▷ Rituximab IV 375 mg/m^2 dosis semanal por 4 semanas o 1 g en dos dosis, los días 1 y 14.
▷ Ciclofosfamida 500–1000 mg/m^2 mensualmente por 3-6 meses
▷ Tocilizumab 8 mg/kg mensuales por ≥2 o más ciclos
▷ Anakinra 5 mg/kg 2 veces al día
▷ Últimas opciones: Bortezomib o Canabidol
💻 Referencia: 10.1177/17511437251321338
2
132
360
19,994