
May 29
That’s why we want business names, we will verify even the existence of these. CIPV database is open for public use.
So if one wants to lie, they must carry that lie all the way to the end. It won’t be nice.
4
158

L’Alliance recherche un(e) consultant(e) pour soutenir la phase de cadrage de notre projet au Bénin visant à soutenir l’adoption de la solution ePhyto de la Convention internationale pour la protection des végétaux (CIPV).
Date limite de candidature : 28 avril 2026 !
tradefacilitation.org/procur…
---
The Alliance is seeking for a consultant to support our project in Benin aimed at deploying the ePhyto solution of the International Plant Protection Convention (IPPC).
Last call for applications on 28 April 2026!
tradefacilitation.org/procur…

4
130

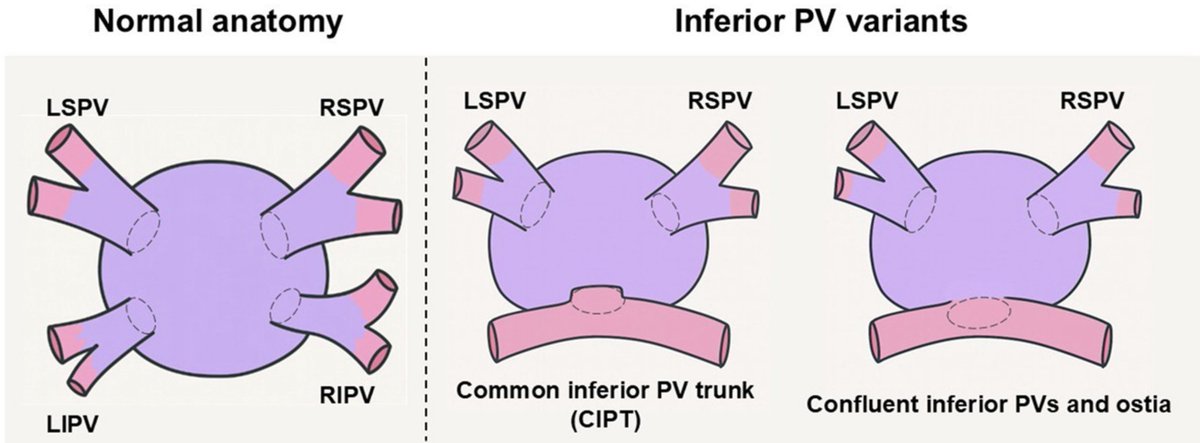
The CIPV trunk is a rare pulmonary venous anatomical variation, observed in about 0.5% of cases. #Epeeps
@drtahasahin @alsertdemir
1
7
56
4,085

#MbanzaNgungu. Lutte contre les organismes nuisibles. La FAO, la Convention internationale pour la protection des végétaux #CIPV, en partenariat avec @minagri_rdc et #UA, lancent ce 4/2/ 2026, une formation de 24 experts congolais sur Programme phytosanitaire pour l’Afrique #PPA

1
2
6
172

Importante mensaje del tocuyano @PABLOMEDINAML (Presidente de la Junta Patriótica y miembro de la Coalición Internacional por Venezuela, CIPV):
* Desde los tiempos del genocida Hugo Chávez se han intentado múltiples vías para sacarlo
* El #ChavismoEsTerrorismo le abrieron las puertas al terrorismo y narcotráfico: Rusia, China, Iran, #FARC, #ELN, #Hezbollah, #HamasRapists, #ISISterror, #AlQaeda, Cuba, etc
* El #ChavismoCriminal impulso crímenes de Lesa humanidad como política de Estado: #PresosPoliticos, #Torturas, expropiaciones, secuestros, etc que impulso a los #VenezolanosMigrantes a salvaguardar sus vidas
* Se ha violado el tratado interamericano de asistencia recíproca (#TIAR)
* Los venezolanos hemos luchado en solitario por más de 26 años
* Por eso ahora le damos la bienvenida a todas las fuerzas en el Caribe: #LanzaDelSur: #OpSouthernSpear) ... gracias a @realDonaldTrump y a @SecRubio: #BienvenidosLosBarcosGringos
* Solicitamos, enmarcados en el #TIAR: colaborar en una segunda independencia de 🇻🇪 🙏 💛💙♥️
16
21
1,437

4 Nov 2025
Se tem o certificado internacional (CIPV), cabou. Só ele.
1
3
1,190

8 Oct 2025
🧬 Teaching the Body to Heal Itself — Part 4 of 4
How $NWBO #DCVax, RevImmune, and Advent BioServices Turn Proof into Platform
Durability, policy, and scale—the immune system learns to remember.
TL;DR
After decades of searching, the immune system’s cure is no longer a moment—it’s a structure.
This final installment shows how durability is measured, how regulatory policy enables it to scale, and how end-to-end manufacturing through Advent BioServices and the FDA’s #CIPV program transforms $NWBO #DCVax RevImmune IL-7 from concept into deployable infrastructure.
The body can now keep learning—without forgetting, without dependence, and without delay.
🧭 Section VI | The Blueprint for Durable Immunity: Measuring What Lasts
For decades, medicine judged success by what it could see on a chart: viral load, tumor size, antibody titer.
But durability—the true sign of a healed immune system—is quieter and harder to measure.
It lives in the rhythm of cells that persist, in the diversity of receptors that remember, and in the steady balance of activation and calm.
The blueprint for proving it has finally taken shape.
1️⃣ What “Durable Immunity” Really Means
Durable immunity isn’t just about killing an infection; it’s about the body maintaining equilibrium after the fight is over.
Three principles define it:
1. Persistence: immune cells remain alive and functional long after therapy ends.
2. Diversity: multiple lineages of T and B cells survive, preventing the system from narrowing into exhaustion.
3. Recall: those cells can respond quickly if the pathogen reappears, without reigniting chronic inflammation.
It is, in essence, the ability of the immune system to sustain its own memory without further instruction.
2️⃣ The Laboratory Language of Durability
Scientists now have a vocabulary for seeing this invisible endurance.
Flow Cytometry: tracks memory subsets—naïve (CD45RA⁺CCR7⁺), central-memory (CD45RA⁻CCR7⁺), and effector-memory (CD45RA⁻CCR7⁻).
Durable responders show high frequencies of central-memory cells that persist for months or years.
ELISPOT and Intracellular Cytokine Staining: re-expose patient cells to the original antigen and count how many secrete IFN-γ, IL-2, or TNF-α.
If cells still respond months later—especially producing IL-2 and IFN-γ simultaneously—it’s proof of lasting recall.
T-cell Receptor (TCR) Sequencing: each T cell has a unique DNA signature; seeing the same clones reappear proves long-term memory.
Serum Cytokine Profiles: balanced IL-7 and IL-15 with low IL-6 and TNF-α mark quiet homeostasis—the fingerprint of durability.
3️⃣ Evidence From the Trials
In the DALIA and DALIA-2 studies, the same HIV-specific T-cell clones detected immediately after vaccination were still present a year later.
Flow cytometry confirmed dominance of central-memory cells, and ELISPOT assays showed sustained polyfunctional responses.
Even when viral rebound occurred, these patients regained control faster—memory depth translated into functional resilience.
In INSPIRE and later CYT107 programs, IL-7 therapy achieved similar persistence without continuous dosing.
T-cell counts and diversity remained elevated for more than a year, with normalized cytokine balance.
The body had not just regained numbers—it had restored the machinery of renewal.
4️⃣ The Self-Healing Architecture
Durability is continuity.
In a self-sustaining immune system:
• Dendritic cells keep teaching new T cells.
• IL-7 maintains the population’s rhythm.
• Tregs hold the tone steady.
When this loop stabilizes, the immune system becomes an ecosystem that regulates itself—no external drugs, no constant intervention.
The body becomes its own therapy: reinstated self-governance.
5️⃣ How We Know When Independence Has Been Achieved
Signs of genuine immune independence include:
• Long-term central-memory dominance.
• Stable TCR repertoire richness across follow-ups.
• Restored CD127 (IL-7 receptor) expression.
• Absence of rebound inflammation or autoimmunity.
• Clinical quiet—normal counts, no relapse.
When these align, the patient is no longer being kept healthy; their immune system is choosing health.
6️⃣ The Beauty of Durability
Durability represents the highest art of medicine: restoring the ability to self-regulate.
It is the moment when therapy ends but healing continues—when IL-7, dendritic-cell instruction, and Treg moderation have rebuilt the body’s innate wisdom.
It’s the difference between giving a person medicine and teaching their biology how to generate its own.
Durability is not the absence of disease; it’s the presence of memory strong enough to keep balance without supervision.
That’s the beauty of this new era.
The goal is no longer constant treatment—it’s teaching the immune system how to fish, so it can feed health for a lifetime.
🧬 Section VII | Epilogue: The Memory That Learns Back
The story that began with a single virus now defines the next generation of medicine.
HIV, once a symbol of hopeless persistence, became the proving ground for a universal principle:
if you restore the architecture of the immune system — its teachers, its sustainers, and its regulators — the body can manage almost any chronic threat on its own.
But even when the science matures, regulation and manufacturing must evolve with it.
That is where the Commissioner’s Independent Priority Voucher (CIPV) and the new FDA plausible-pathway framework come together with the Advent BioServices acquisition to form the infrastructure of what happens next.
1️⃣ The Bottleneck That Had to Break
Old regulatory models were built for single-target drugs: one molecule, one disease, one label.
That framework was never meant for platform biologics — living systems that can be tuned to fight cancer, infection, or autoimmunity using the same cellular language.
It also didn’t anticipate the manufacturing complexity of individualized vaccines.
Without vertically integrated production, even the most elegant dendritic-cell therapy would be stuck in trial mode forever, unable to scale or meet FDA traceability standards.
That bottleneck — scientific, regulatory, and logistical — has finally broken.
2️⃣ The Plausible Pathway and the CIPV
The plausible-pathway concept allows regulators to approve mechanism and process, not just indication.
Once a cellular platform has proven it can educate the immune system safely and reproducibly, it can be adapted across diseases without starting from zero.
The CIPV, the Commissioner’s Independent Priority Voucher, is the fast track through that door — an accelerated approval channel for biologics serving national health priorities.
It was designed for therapies exactly like IL-7 dendritic-cell immunotherapy: modular, tissue-agnostic, and capable of addressing multiple diseases through the same immune operating system.
3️⃣ The Final Piece: End-to-End Control Through Advent
When Northwest Biotherapeutics completed its acquisition of Advent BioServices, it gained more than a facility — it gained total vertical integration.
Advent’s MHRA-licensed GMP plant in Sawston, U.K., can now produce clinical and commercial dendritic-cell vaccines from start to finish:
• Cell procurement and isolation in sterile Grade C cleanrooms.
• Flaskworks Eden closed-system automation for consistent manufacturing.
• Cryogenic preservation and batch-level quality control for multi-year dose storage.
• Full digital traceability meeting both MHRA and FDA standards.
This internal supply chain removes the last friction between discovery and delivery.
It is now possible — physically, legally, and regulatorily — to take a dendritic-cell therapy from a patient’s blood draw to a ready-to-use, fully documented product under one roof.
That end-to-end control transforms the vision of immune self-restoration from concept into operational reality.
4️⃣ A Regulatory Framework Built for Scale
With Advent’s integrated production and the CIPV’s fast-track pathway, a new ecosystem emerges:
• RevImmune’s IL-7 (CYT107) fuels immune endurance.
• Northwest’s DCVax teaches antigenic recognition.
• Advent’s GMP facility ensures global manufacturability.
• The CIPV and plausible-pathway structure let these therapies move fluidly across indications — cancer, infection, or beyond — without redundant review.
This framework treats the immune-restoration platform as what it truly is: a national biologic infrastructure, not a single-use product.
It’s the difference between certifying one airplane route and approving the entire aircraft design — once validated, it can fly anywhere.
5️⃣ From One Indication to Many
Under this model, the same platform that extended survival in glioblastoma (DCVax-L) can be applied to solid tumors, #HIV, autoimmune disease, and post-viral immune depletion.
Each use follows the same cellular and manufacturing logic already validated by Advent’s GMP system.
The #CIPV allows these expansions to move through regulatory review in months instead of years because the safety, quality, and mechanism are already proven.
That is how medicine escapes the old one-indication bottleneck and becomes truly disease-agnostic.
6️⃣ When Biology and Infrastructure Align
For decades, the dream of personalized immunotherapy was hindered not by science but by logistics.
With Advent’s full manufacturing control, that barrier is gone.
Now biology, regulation, and production form a single, self-reinforcing loop:
1. Dendritic cells re-educate the immune system.
2. IL-7 preserves the memory of that lesson.
3. Tregs ensure learning heals rather than harms.
4. Advent manufactures at global scale.
5. CIPV moves it efficiently through the regulatory gate.
That convergence — scientific, infrastructural, and regulatory — creates the first realistic path to widespread, durable immune restoration.
7️⃣ The New Definition of Cure
In this world, a cure is no longer an event; it is a structure — biological, logistical, and regulatory — working in harmony.
The IL-7 DCVax platform, supported by RevImmune, Northwest Biotherapeutics, and Advent BioServices, and validated under the CIPV plausible-pathway framework, represents that structure fully realized.
It is the moment when the architecture of the immune system, manufacturing, and regulation finally align.
And in that alignment lies the quiet revolution of modern medicine:
the ability to teach the body to heal itself,
to manufacture that teaching sustainably,
and to deliver it anywhere in the world without delay.
That is no longer theory — it is now, for the first time, logistically and regulatorily possible.
#NWBO #DCVax #RevImmune #AdventBioServices #IL7 #CIPV #FDA #Immunotherapy #CellTherapy #ImmuneRestoration #DurableImmunity #Biotech #MedicalInnovation #ImmuneIndependence #TeachingTheBodyToHeal
📚 Sources
Scientific and Clinical Foundations
• Lévy Y et al. Safety and immunogenicity of a dendritic-cell therapeutic vaccine in HIV-1–infected patients receiving ART (DALIA trial). Science Translational Medicine. 2014.
• Lévy Y et al. VRI04–DALIA2 trial design: IL-7 plus dendritic-cell vaccine in ART-treated HIV infection. Vaccine Research Institute / ANRS Reports. 2018–2024.
• Sereti I et al. Recombinant human interleukin-7 (CYT107) promotes T-cell recovery in HIV infection: results of INSPIRE-1 and INSPIRE-2. Journal of Infectious Diseases. 2013; 207(4): 573–586.
• Lévy Y et al. IL-7 immunotherapy in chronic HIV infection: restoring immune homeostasis. Science Translational Medicine. 2012.
• Katlama C et al. RevImmune’s CYT107 (IL-7) in HIV infection: randomized clinical study. ANRS ILIADE Consortium Reports. 2016.
• Brezar V et al. Regulatory T-cell dynamics and vaccine-induced immunity in DALIA trial participants. PLoS Pathogens. 2015.
• He R et al. Treg depletion and latency reversal in SIV controllers. Nature Communications. 2021.
• Kalinski P et al. Type-1 polarized dendritic cells (αDC1) as potent inducers of cytotoxic T lymphocytes for cancer and viral immunotherapy. Journal of Immunology. 2009.
• Kalinski P et al. αDC1 vaccination in glioma: preclinical and translational results. Journal of Translational Medicine. 2012.
Platform and Corporate Integration
• Northwest Biotherapeutics. DCVax-L Phase III Trial Results Presentation (ASCO 2023).
• Northwest Biotherapeutics. DCVax-L Mechanism of Action and External Controls Methodology. JAMA Oncology Supplement (Liau et al., 2022).
• RevImmune Inc. CYT107 (efineptakin alfa) Clinical Overview. Corporate Data Sheet, 2023.
• Advent BioServices (MHRA Licence 54923). Facility Capability and GMP Certification. MHRA Public Database, 2023.
• Northwest Biotherapeutics. Advent Acquisition Press Release. SEC Filings, April 2024.
• Flaskworks LLC (a NWBO subsidiary). Eden Automated Closed-System Manufacturing Patent. USPTO filings, 2021–2023.
Regulatory and Framework References
• U.S. Food and Drug Administration (FDA). Commissioner’s Independent Priority Voucher (CIPV) Initiative. 2023.
• FDA, CBER & NIH. Plausible Pathway Framework for Tissue-Agnostic Biologics and Regenerative Cell Therapies. 2024 Draft Guidance.
• European Medicines Agency (EMA) & MHRA. Reflection Paper on Platform Manufacturing Approaches for Cell and Gene Therapy. 2023.
• Mishra-Kalyani PS, Amiri-Kordestani L, Rivera DR et al. External Control Arms in Oncology: Current Use and Future Directions. Annals of Oncology. 2022.
⚖️ Disclaimer
This narrative is an educational synthesis based on publicly available scientific publications, regulatory documents, and corporate disclosures.
It represents interpretive analysis for informational purposes only and should not be construed as medical advice, investment guidance, or a solicitation of any kind.
Clinical outcomes described reflect published or reported data as of 2025; ongoing and future trials may alter interpretations or conclusions.
All company names, trademarks, and study identifiers remain the property of their respective owners.
Readers should consult primary literature, regulatory filings, and qualified medical professionals for detailed and current information.
8 Oct 2025

🧬 Teaching the Body to Heal Itself — Part 3
How $NWBO #DCVax and RevImmune’s IL-7 Moved From Lab to Life
Proof that the lesson works.
TL;DR
The principles of dendritic-cell instruction and IL-7 homeostasis left the lab and entered patients.
France’s DALIA and DALIA-2 trials proved the immune system could be re-taught; RevImmune’s CYT107 showed the body could keep that lesson alive.
Across the Atlantic, NIH-funded INSPIRE studies confirmed IL-7’s safety and power.
Public science met private innovation to form the architecture now embodied in $NWBO #DCVax RevImmune IL-7 — the first platform built to teach, sustain, and remember immunity itself.
🧪 Section V | The Human Experiments: From DALIA to CYT107
Every scientific theory eventually leaves the laboratory and steps into the world.
For IL-7 and dendritic-cell immunotherapy, that moment arrived through an unusual alliance — universities, national health agencies, and small biotechs working together on a single, patient-centered idea:
what if the body could be taught to heal itself?
#HIV became the testing ground for that idea.
1️⃣ France Takes the First Step: The DALIA Trial
In 2007, the French National Agency for Research on AIDS and Viral Hepatitis (ANRS) launched a trial unlike anything before it.
At Hôpital Henri-Mondor in Créteil, researchers from the Vaccine Research Institute (VRI) collected monocytes from patients on stable antiretroviral therapy.
They cultured these cells into dendritic cells, loaded them with five synthetic HIV peptides (a formulation known as LIPO-5), and re-infused them back into each patient’s lymphatic system.
It was a purely publicly funded experiment, supported by ANRS and the French Ministry of Health.
There was no commercial sponsor, no drug company dictating design — just a national belief that the immune system itself might hold the key.
The results, published in Science Translational Medicine, were quiet but historic.
The vaccine was safe, well tolerated, and it produced polyfunctional T cells — the kind that release multiple cytokines at once, the hallmark of durable immunity.
When antiretroviral therapy was briefly paused under close supervision, some patients delayed viral rebound for weeks beyond expectation.
For the first time, a therapeutic vaccine hinted that HIV control could be taught rather than enforced.
2️⃣ The Next Generation: DALIA-2 and the Arrival of IL-7
The first DALIA trial proved the concept; DALIA-2 aimed to sustain it.
Led again by ANRS and the Vaccine Research Institute, the new trial introduced recombinant human IL-7 (CYT107), supplied by a small Franco-American company called RevImmune Inc.
RevImmune’s CYT107 had already shown it could safely expand T cells in HIV-positive individuals.
By combining it with the dendritic-cell vaccine, researchers hoped to transform a short-lived immune response into a self-renewing one.
The design had four arms:
1. Vaccine alone.
2. IL-7 alone.
3. IL-7 before vaccination (to expand the classroom).
4. IL-7 after vaccination (to preserve the memory).
Funding again came largely from public sources — ANRS, INSERM, and European research grants — with RevImmune providing the biologic and technical oversight for dosing.
It was a model of science as shared infrastructure: governments funding the question, industry supplying the means, and clinicians executing the vision.
Although DALIA-2 is still analyzing long-term outcomes, early data show clear immunologic synergy.
IL-7 amplified the number of vaccine-specific T cells, maintained their central-memory phenotype, and improved their ability to traffic back into lymphoid tissue.
What began as an academic exercise was becoming a clinical architecture.
3️⃣ Across the Atlantic: INSPIRE and NIH-Supported Trials
The National Institutes of Health (NIH) in the United States soon joined the effort.
Through its Division of AIDS (DAIDS) and the National Institute of Allergy and Infectious Diseases (NIAID), it funded the INSPIRE-1 and INSPIRE-2 trials to study IL-7 in American HIV patients.
RevImmune supplied CYT107; federal grants supported clinical infrastructure and data analysis.
At institutions like the University of Pittsburgh and Massachusetts General Hospital, patients on ART received carefully titrated doses of IL-7 to restore immune homeostasis.
The results mirrored France’s: sustained CD4⁺ and CD8⁺ expansion, diversification of T-cell receptors, and no significant adverse events.
By the early 2020s, IL-7 was being tested not just as immune support, but as an adjunctive therapy to vaccines and latency-reversing agents under NIH cooperative protocols.
This dual-track approach — public funding for exploratory science, private stewardship for manufacturing and scale — became a global model of translational medicine.
4️⃣ RevImmune and Northwest Biotherapeutics: One Vision, Two Platforms
Behind the scenes, the convergence deepened.
RevImmune, led by Linda Powers, developed IL-7 as the universal fuel of immune endurance.
Her other company, Northwest Biotherapeutics, was simultaneously proving that dendritic-cell vaccines could extend survival in terminal cancer.
One company taught the immune system how to last; the other taught it what to recognize.
Together they formed the missing circuit — cytokine sustainability joined with antigenic instruction.
It was not difficult to imagine the two technologies one day meeting in a single therapeutic ecosystem: dendritic-cell vaccination powered by IL-7’s ability to preserve memory.
That conceptual bridge, first tested in publicly funded HIV trials, is now being applied to solid tumors, sepsis, and immune recovery after viral injury.
5️⃣ The Meaning of Government Partnership
It is easy to overlook the elegance of how the world’s most transformative discoveries are built.
The HIV dendritic-cell and IL-7 trials looked, on paper, like ordinary government science — ANRS and INSERM in France, the NIH in Bethesda — programs that nurtured pure immunology without commercial pressure. But within that structure, someone was already thinking a decade ahead.
When Linda Powers acquired the recombinant IL-7 program (CYT107) through RevImmune, she wasn’t “taking over” academic work; she was preserving the bridge between what public science had proved and what the clinic still needed.
The molecule’s original developer, Cytheris SA, had collapsed under financial strain, threatening to erase nearly two decades of research funded by ANRS, INSERM, and NIH. Powers stepped in through Cognate BioServices, acquiring the IL-7 asset out of bankruptcy for a fraction of its value — not as a speculative buyout, but as a rescue mission. Without that intervention, the IL-7 trials would have gone dark, their regulatory filings and manufacturing systems dismantled.
She recognized that the government-funded trials had uncovered the missing half of long-term immune control: dendritic-cell instruction could ignite an immune response, but IL-7 was the signal that made it last.
Public agencies had created the arena where those truths could surface — where HIV researchers could measure, cell by cell, how IL-7 expanded central-memory T cells and how dendritic-cell vaccination re-educated exhausted immunity.
What Powers saw was the architecture beneath the data: a living feedback loop that, if protected and scaled, could form the backbone of durable therapy for cancer, infection, and beyond.
Through RevImmune, she ensured IL-7 survived and stayed available to government and academic investigators. Through Northwest Biotherapeutics, she placed that same biology inside a regulated, manufacturable framework.
Together they became the two halves of a single continuum — discovery and deployment, instruction and endurance.
That is what true public-private partnership looks like:
• Public science reveals the mechanism of truth.
• Private vision preserves it and turns it into infrastructure.
The HIV studies proved that collaboration at this depth can yield more than transient control. They produced a framework for sustained biological independence — a model in which the
government builds the foundation of knowledge, and visionary leadership ensures that knowledge keeps living in patients, not archives.
She didn’t just seize the field; she understood its destiny and gave it permanence.
When knowledge survives the hand-off from discovery to design, something remarkable happens: the immune system itself becomes the beneficiary of that same continuity.
What began as data in government laboratories evolves into a living process inside the body — cells remembering, correcting, and rebuilding on their own.
This is where the partnership between public science and private vision completes its circuit, where the infrastructure of medicine dissolves into physiology.
It is here, in the body’s restored ability to remember and renew, that treatment becomes something greater.
6️⃣ From Treatment to Self-Restoration
Across the DALIA and INSPIRE programs, one theme echoed again and again: durability.
Patients didn’t just show transient immune activation; they retained stable, diverse T-cell populations long after dosing stopped.
Cytokine levels normalized, inflammatory markers fell, and the immune system regained its rhythm.
For some participants, this meant the difference between a body that needed constant pharmaceutical support and a body capable of regulating itself.
It was the proof of concept for “teach the body to fish” medicine — restoring self-reliance instead of endless maintenance.
That, ultimately, is what makes the HIV platform so important: it is not merely about viral control, but about re-learning physiological independence.
Every IL-7 molecule and every dendritic cell in these trials carried the same message — remember what health feels like, and stay there.
⮕ Transition to Part 4
The final installment explains how proof becomes practice — how durability is measured, how policy and infrastructure enable scale, and how Advent BioServices and the FDA’s CIPV framework make immune restoration a deployable reality.
#NWBO #DCVax #RevImmune #IL7 #DALIA #DALIA2 #INSPIRE #Immunotherapy #ImmuneRestoration #DurableImmunity #PublicScience #Biotech #MedicalInnovation #TeachingTheBodyToHeal
1
7
1,877
8 Oct 2025
🧬 Teaching the Body to Heal Itself — Part 3 of 4
How $NWBO #DCVax and RevImmune’s IL-7 Moved From Lab to Life
Proof that the lesson works.
TL;DR
The principles of dendritic-cell instruction and IL-7 homeostasis left the lab and entered patients.
France’s DALIA and DALIA-2 trials proved the immune system could be re-taught; RevImmune’s CYT107 showed the body could keep that lesson alive.
Across the Atlantic, NIH-funded INSPIRE studies confirmed IL-7’s safety and power.
Public science met private innovation to form the architecture now embodied in $NWBO #DCVax RevImmune IL-7 — the first platform built to teach, sustain, and remember immunity itself.
🧪 Section V | The Human Experiments: From DALIA to CYT107
Every scientific theory eventually leaves the laboratory and steps into the world.
For IL-7 and dendritic-cell immunotherapy, that moment arrived through an unusual alliance — universities, national health agencies, and small biotechs working together on a single, patient-centered idea:
what if the body could be taught to heal itself?
#HIV became the testing ground for that idea.
1️⃣ France Takes the First Step: The DALIA Trial
In 2007, the French National Agency for Research on AIDS and Viral Hepatitis (ANRS) launched a trial unlike anything before it.
At Hôpital Henri-Mondor in Créteil, researchers from the Vaccine Research Institute (VRI) collected monocytes from patients on stable antiretroviral therapy.
They cultured these cells into dendritic cells, loaded them with five synthetic HIV peptides (a formulation known as LIPO-5), and re-infused them back into each patient’s lymphatic system.
It was a purely publicly funded experiment, supported by ANRS and the French Ministry of Health.
There was no commercial sponsor, no drug company dictating design — just a national belief that the immune system itself might hold the key.
The results, published in Science Translational Medicine, were quiet but historic.
The vaccine was safe, well tolerated, and it produced polyfunctional T cells — the kind that release multiple cytokines at once, the hallmark of durable immunity.
When antiretroviral therapy was briefly paused under close supervision, some patients delayed viral rebound for weeks beyond expectation.
For the first time, a therapeutic vaccine hinted that HIV control could be taught rather than enforced.
2️⃣ The Next Generation: DALIA-2 and the Arrival of IL-7
The first DALIA trial proved the concept; DALIA-2 aimed to sustain it.
Led again by ANRS and the Vaccine Research Institute, the new trial introduced recombinant human IL-7 (CYT107), supplied by a small Franco-American company called RevImmune Inc.
RevImmune’s CYT107 had already shown it could safely expand T cells in HIV-positive individuals.
By combining it with the dendritic-cell vaccine, researchers hoped to transform a short-lived immune response into a self-renewing one.
The design had four arms:
1. Vaccine alone.
2. IL-7 alone.
3. IL-7 before vaccination (to expand the classroom).
4. IL-7 after vaccination (to preserve the memory).
Funding again came largely from public sources — ANRS, INSERM, and European research grants — with RevImmune providing the biologic and technical oversight for dosing.
It was a model of science as shared infrastructure: governments funding the question, industry supplying the means, and clinicians executing the vision.
Although DALIA-2 is still analyzing long-term outcomes, early data show clear immunologic synergy.
IL-7 amplified the number of vaccine-specific T cells, maintained their central-memory phenotype, and improved their ability to traffic back into lymphoid tissue.
What began as an academic exercise was becoming a clinical architecture.
3️⃣ Across the Atlantic: INSPIRE and NIH-Supported Trials
The National Institutes of Health (NIH) in the United States soon joined the effort.
Through its Division of AIDS (DAIDS) and the National Institute of Allergy and Infectious Diseases (NIAID), it funded the INSPIRE-1 and INSPIRE-2 trials to study IL-7 in American HIV patients.
RevImmune supplied CYT107; federal grants supported clinical infrastructure and data analysis.
At institutions like the University of Pittsburgh and Massachusetts General Hospital, patients on ART received carefully titrated doses of IL-7 to restore immune homeostasis.
The results mirrored France’s: sustained CD4⁺ and CD8⁺ expansion, diversification of T-cell receptors, and no significant adverse events.
By the early 2020s, IL-7 was being tested not just as immune support, but as an adjunctive therapy to vaccines and latency-reversing agents under NIH cooperative protocols.
This dual-track approach — public funding for exploratory science, private stewardship for manufacturing and scale — became a global model of translational medicine.
4️⃣ RevImmune and Northwest Biotherapeutics: One Vision, Two Platforms
Behind the scenes, the convergence deepened.
RevImmune, led by Linda Powers, developed IL-7 as the universal fuel of immune endurance.
Her other company, Northwest Biotherapeutics, was simultaneously proving that dendritic-cell vaccines could extend survival in terminal cancer.
One company taught the immune system how to last; the other taught it what to recognize.
Together they formed the missing circuit — cytokine sustainability joined with antigenic instruction.
It was not difficult to imagine the two technologies one day meeting in a single therapeutic ecosystem: dendritic-cell vaccination powered by IL-7’s ability to preserve memory.
That conceptual bridge, first tested in publicly funded HIV trials, is now being applied to solid tumors, sepsis, and immune recovery after viral injury.
5️⃣ The Meaning of Government Partnership
It is easy to overlook the elegance of how the world’s most transformative discoveries are built.
The HIV dendritic-cell and IL-7 trials looked, on paper, like ordinary government science — ANRS and INSERM in France, the NIH in Bethesda — programs that nurtured pure immunology without commercial pressure. But within that structure, someone was already thinking a decade ahead.
When Linda Powers acquired the recombinant IL-7 program (CYT107) through RevImmune, she wasn’t “taking over” academic work; she was preserving the bridge between what public science had proved and what the clinic still needed.
The molecule’s original developer, Cytheris SA, had collapsed under financial strain, threatening to erase nearly two decades of research funded by ANRS, INSERM, and NIH. Powers stepped in through Cognate BioServices, acquiring the IL-7 asset out of bankruptcy for a fraction of its value — not as a speculative buyout, but as a rescue mission. Without that intervention, the IL-7 trials would have gone dark, their regulatory filings and manufacturing systems dismantled.
She recognized that the government-funded trials had uncovered the missing half of long-term immune control: dendritic-cell instruction could ignite an immune response, but IL-7 was the signal that made it last.
Public agencies had created the arena where those truths could surface — where HIV researchers could measure, cell by cell, how IL-7 expanded central-memory T cells and how dendritic-cell vaccination re-educated exhausted immunity.
What Powers saw was the architecture beneath the data: a living feedback loop that, if protected and scaled, could form the backbone of durable therapy for cancer, infection, and beyond.
Through RevImmune, she ensured IL-7 survived and stayed available to government and academic investigators. Through Northwest Biotherapeutics, she placed that same biology inside a regulated, manufacturable framework.
Together they became the two halves of a single continuum — discovery and deployment, instruction and endurance.
That is what true public-private partnership looks like:
• Public science reveals the mechanism of truth.
• Private vision preserves it and turns it into infrastructure.
The HIV studies proved that collaboration at this depth can yield more than transient control. They produced a framework for sustained biological independence — a model in which the
government builds the foundation of knowledge, and visionary leadership ensures that knowledge keeps living in patients, not archives.
She didn’t just seize the field; she understood its destiny and gave it permanence.
When knowledge survives the hand-off from discovery to design, something remarkable happens: the immune system itself becomes the beneficiary of that same continuity.
What began as data in government laboratories evolves into a living process inside the body — cells remembering, correcting, and rebuilding on their own.
This is where the partnership between public science and private vision completes its circuit, where the infrastructure of medicine dissolves into physiology.
It is here, in the body’s restored ability to remember and renew, that treatment becomes something greater.
6️⃣ From Treatment to Self-Restoration
Across the DALIA and INSPIRE programs, one theme echoed again and again: durability.
Patients didn’t just show transient immune activation; they retained stable, diverse T-cell populations long after dosing stopped.
Cytokine levels normalized, inflammatory markers fell, and the immune system regained its rhythm.
For some participants, this meant the difference between a body that needed constant pharmaceutical support and a body capable of regulating itself.
It was the proof of concept for “teach the body to fish” medicine — restoring self-reliance instead of endless maintenance.
That, ultimately, is what makes the HIV platform so important: it is not merely about viral control, but about re-learning physiological independence.
Every IL-7 molecule and every dendritic cell in these trials carried the same message — remember what health feels like, and stay there.
⮕ Transition to Part 4
The final installment explains how proof becomes practice — how durability is measured, how policy and infrastructure enable scale, and how Advent BioServices and the FDA’s CIPV framework make immune restoration a deployable reality.
#NWBO #DCVax #RevImmune #IL7 #DALIA #DALIA2 #INSPIRE #Immunotherapy #ImmuneRestoration #DurableImmunity #PublicScience #Biotech #MedicalInnovation #TeachingTheBodyToHeal
8 Oct 2025
🧬 Teaching the Body to Heal Itself — Part 2
How $NWBO #DCVax and RevImmune’s IL-7 Rebuild the Language of Immunity
The lifeline that keeps the lesson alive.
TL;DR
If dendritic cells are the immune system’s teachers, interleukin-7 (IL-7) is its atmosphere — the quiet signal that keeps every T cell breathing.
When #HIV silenced that signal, immunity forgot how to remember.
RevImmune’s CYT107, a recombinant IL-7, restores that rhythm, and when combined with $NWBO #DCVax’s dendritic-cell instruction, the immune system can maintain memory indefinitely.
This part explores IL-7’s biology, its partnership with dendritic-cell vaccination, and the completion of the triad — #Tregs, IL-7, and DCs — that allows the body to heal itself and remain in balance.
🌿 Section III | Interleukin-7: The Lifeline of Immune Memory
Every tissue in the body whispers maintenance instructions to its immune cells.
Among those messages, interleukin-7 (IL-7) is the one that keeps the conversation alive.
It does not start immune responses; it preserves them.
Without IL-7, the adaptive immune system gradually forgets what it has learned.
1️⃣ Where IL-7 Comes From and What It Does
IL-7 is produced constantly by the stromal framework of bone marrow, lymph nodes, and the thymus.
Unlike inflammatory cytokines that surge during infection, IL-7 is always present at low levels, quietly signaling: “Stay alive, stay ready.”
Each resting T cell carries an IL-7 receptor, built from two pieces: the α-chain (CD127) and the common γ-chain shared with IL-2 and IL-15 receptors.
When IL-7 binds, it flips a molecular switch — the JAK-STAT5 pathway — that turns on survival genes (BCL-2, MCL-1) and silences pro-death genes like BIM.
The cell keeps its mitochondria healthy, divides occasionally, and resists exhaustion.
Through this quiet signaling, IL-7 performs three ongoing jobs:
1. Prevents cell death of naïve and memory T cells.
2. Maintains population balance by slow “tick-over” proliferation.
3. Preserves diversity, keeping rare T-cell clones alive so future threats can still be recognized.
2️⃣ How HIV Disrupts the IL-7 Network
HIV attacks the system at both ends.
• Receptor deafness. Chronic activation drives T cells to shed CD127; even as the body floods the blood with IL-7 in panic, the cells can no longer hear it.
• Damage to the source. HIV inflames and scars the thymus and lymph-node stroma that make IL-7.
• Loss of renewal. With fewer naïve cells entering from the thymus and more dying in the periphery, the repertoire narrows to a handful of exhausted clones.
The result is a cruel paradox: high IL-7 in the bloodstream, yet functional starvation inside the tissues.
Under ART the numbers look normal, but immune diversity and stamina keep fading.
3️⃣ Giving IL-7 Back — RevImmune and CYT107
To repair that missing conversation, scientists turned to recombinant human IL-7 (rhIL-7), a biologic now developed by RevImmune Inc. — a company chaired by Linda Powers, who also leads Northwest Biotherapeutics.
RevImmune’s lead product, CYT107 (efineptakin alfa), is a long-acting form of IL-7 engineered for safe, sustained release.
Across multiple clinical trials — in HIV, cancer, and sepsis — CYT107 has shown a reproducible pattern:
• Expansion of CD4⁺ and CD8⁺ T cells by 50–300 cells/µL within weeks.
• Preferential growth of central- and stem-memory subsets.
• Restoration of repertoire breadth, with new clones appearing after years of dormancy.
• Improved gut and lymph-node homing (↑ α4β7 integrin expression).
• Excellent tolerability with only mild injection-site reactions.
Mechanistically, CYT107 revives thymic output and extends the life span of existing memory T cells simultaneously.
It also improves dendritic-cell numbers and trafficking, re-linking the survival loop between the immune system’s teachers and their students.
Transient “viral blips” sometimes appear as latent HIV-infected cells divide under IL-7’s influence, but these spikes fade quickly.
They are evidence that IL-7 is stirring the reservoir into view while strengthening the cytotoxic cells that can eliminate it.
4️⃣ Why IL-7 Complements Dendritic-Cell Vaccination
A dendritic-cell (DC) vaccine instructs; IL-7 sustains.
After vaccination, the body produces hundreds of HIV-specific T-cell clones. Without support, most would die within weeks once the antigen fades. IL-7 changes that outcome.
• It guides activated cells into a central-memory phenotype capable of long-term self-renewal.
• It preserves mitochondrial and metabolic fitness, preventing exhaustion.
• It maintains breadth, ensuring that when HIV mutates, some clones still recognize it.
Given shortly after a DC vaccine, CYT107 acts like a nutrient feed to the immune network — turning a brief burst of activity into a stable, long-term memory circuit.
In cancer and HIV pilot studies, patients who received IL-7 after DC vaccination kept robust antigen-specific responses for many months longer than vaccine-only controls.
5️⃣ Why RevImmune Matters in This Story
RevImmune and Northwest Biotherapeutics represent two halves of a single strategy led by the same architect, Linda Powers:
• Northwest Biotherapeutics built the world’s most advanced dendritic-cell vaccine platform (DCVax).
• RevImmune built the cytokine engine (IL-7/CYT107) that keeps those vaccine-primed T cells alive and diverse.
Mechanistically, the pairing closes the loop of immune restoration: the dendritic cell teaches, IL-7 preserves, and together they create an immune system that no longer forgets.
6️⃣ The Broader Meaning
IL-7 therapy doesn’t attack HIV directly.
It repairs the terrain on which every immune response depends.
By restoring thymic renewal and T-cell survival, it replaces a chaotic, inflammatory network with one capable of enduring vigilance.
When dendritic-cell education and IL-7 homeostasis operate together, the body stops fighting a losing battle and begins remembering on its own.
That principle — the marriage of instruction and survival — is what may finally transform HIV from a chronic infection into a controllable, self-regulated equilibrium.
⚖️ Section IV | The Triad: Tregs, IL-7, and Dendritic Cells in Balance
Every immune system is a conversation among three voices: Dendritic cells that teach, T cells that act, and Tregs that translate intensity into harmony.
When this triad works together, the body is self-correcting — a living network capable of learning, fighting, and then healing without outside instruction.
HIV disrupted that grammar. It silenced the teachers, exhausted the fighters, and let the translators speak only of restraint.
The result was an immune language half-forgotten.
Now, for the first time, IL-7 and dendritic-cell vaccines can rebuild that conversation. And when the Treg component is properly tuned, the language becomes complete again — the immune system regains fluency in its own logic.
1️⃣ The Natural Grammar of Immunity
In health, dendritic cells introduce an antigen like a teacher introducing a new subject.
They deliver three synchronized signals:
• What the threat is (antigen on MHC molecules).
• Whether it is dangerous (co-stimulatory molecules).
• How to respond (cytokine context).
The students — T cells — learn, respond, and then quiet down when the lesson is over.
That quieting comes from regulatory T cells (Tregs), which release IL-10 and TGF-β, signaling the immune system to stop fighting and start repairing.
Meanwhile, IL-7 ensures the memory of that encounter endures, keeping a few cells alive to remember the lesson for next time.
In this normal state, activation, memory, and tolerance form a perfect triangle — agility without chaos, control without fragility.
2️⃣ HIV’s Distortion of the Dialogue
HIV twisted this language into a stutter.
• Tregs multiplied uncontrollably, enforcing silence even as the virus spread.
• Dendritic cells stopped teaching, producing IL-10 instead of IL-12 and losing their co-stimulatory voice.
• Effector T cells burned out, their IL-7 receptors lost, their energy gone.
The conversation became one-sided: regulators without resistance, peace without victory.
The immune system could neither fight effectively nor remember how.
3️⃣ IL-7: Restoring the Breath of the System
IL-7 does not attack the virus; it re-oxygenates the system.
By reviving thymic function and rescuing central-memory T cells, it rebuilds the immune population with diversity and stamina.
Crucially, IL-7 restores the effector-to-Treg ratio that defines healthy equilibrium.
When the network is bathed in IL-7, dendritic cells flourish again, T cells regain responsiveness, and inflammation becomes measured rather than chronic.
It is the biological equivalent of restoring breath to an exhausted lung — sustaining function long after external support is removed.
4️⃣ Dendritic-Cell Vaccination: Teaching Again
The dendritic-cell vaccine returns content to this rejuvenated system.
Re-trained outside the body and pulsed with the full antigenic library of HIV, these cells re-enter the lymph nodes and speak in clear molecular sentences once more:
Here is the threat. Here is how to recognize it. Here is how to remember it.
Because the vaccine teaches thousands of antigenic “words” at once, HIV can no longer hide behind mutation.
And with IL-7 maintaining the memory environment, the immune system can keep rehearsing that lesson indefinitely, even after therapy stops.
5️⃣ The Role of Tregs: Completing the Language
The Treg component is not a flaw to be removed — it is the punctuation that makes the sentence readable.
Too many, and they erase meaning; too few, and the sentence runs on into chaos.
When IL-7 and DC vaccination recalibrate the system, Tregs return to their proper function: mediating precision, not paralysis.
In that balanced state, Tregs no longer protect HIV; they protect the tissue while allowing full DCVax potential to be unlocked.
They enable sustained, safe activation — a measured fire that burns only what it must.
This is the true completion of the immune language: activation, restraint, and memory speaking in harmony.
6️⃣ Sustained Durability: Teaching the Body to Heal Itself
The most beautiful outcome of this triad is not viral clearance alone — it is autonomy.
When dendritic-cell instruction, IL-7 support, and Treg moderation operate together, the immune system no longer needs constant pharmacologic intervention.
It becomes self-maintaining, able to renew its own balance and repair its own damage.
This is the medical equivalent of the proverb: don’t give a person a fish — teach them how to fish.
Instead of endless drug dependence, the body is taught how to manage the infection on its own terms.
Durability is the quiet miracle here.
Each component — teacher, sustainer, and regulator — works so that when treatment ends, equilibrium remains.
The immune system continues its dialogue without supervision, healing itself from within.
That is not just therapy; it is restoration of biological independence.
And in that independence lies the future of all immunotherapy — the moment when medicine stops fighting for the body, and the body learns to fight, remember, and heal for itself.
⮕ Transition to Part 3
The next chapter moves from theory to human evidence — the DALIA and DALIA-2 trials, INSPIRE, and the collaboration between RevImmune’s IL-7 and $NWBO #DCVax that turned this scientific triad into real-world results.
#NWBO #DCVax #RevImmune #IL7 #Tregs #ImmuneBalance #DendriticCells #αDC1 #Immunotherapy #ImmuneRestoration #DurableImmunity #Biotech #MedicalInnovation #TeachingTheBodyToHeal
1
4
1,374
8 Oct 2025
🧬 Teaching the Body to Heal Itself — Part 1 of 4
How $NWBO #DCVax and RevImmune’s IL-7 Are Rewriting the Architecture of Immune Memory
From the virus that rewrote immunity to the blueprint that restores it.
TL;DR
For forty years, #HIV has been medicine’s toughest classroom. It forced scientists to learn how memory, tolerance, and regulation truly work. What few outside the field know is that, hidden inside that struggle, two public research programs quietly achieved something revolutionary.
In France, the DALIA and DALIA-2 trials, funded by the ANRS and Vaccine Research Institute, used a patient’s own dendritic cells to retrain immunity against HIV. These cells were matured ex vivo in cytokine cocktails — an early version of what is now known as type-1 polarized dendritic cells (αDC1) — and they proved that the immune system could be re-educated to recognize a chronic invader again.
At the same time, U.S. and European studies of interleukin-7 (IL-7), supplied by RevImmune Inc. — a company led by Linda Powers, who also chairs Northwest Biotherapeutics — showed that the body’s T-cell population could be safely rebuilt and maintained for the long term.
Those two threads — dendritic-cell instruction and IL-7-driven persistence — would later converge in the industrialized DCVax platform. DCVax perfected the same biological principle discovered in the HIV studies but under full GMP control: it uses the advanced αDC1 maturation process developed by Dr. Pawel Kalinski to generate dendritic cells that secrete high levels of IL-12 p70 and coordinate broad, durable cytotoxic responses.
With Advent BioServices’ end-to-end manufacturing now integrated under Northwest Biotherapeutics, every step — from leukapheresis to cryopreserved, ready-to-use doses — can occur within a single licensed facility. This eliminates the last barrier that kept academic discoveries from real-world deployment.
Finally, the new FDA Commissioner’s Independent Priority Voucher (CIPV) and its plausible-pathway framework provide the regulatory bridge. They allow validated immune-education platforms like IL-7 DCVax to move fluidly across diseases — cancer, infection, or autoimmunity — without repeating the entire approval process for each indication.
Together, these advances mean the concept first glimpsed in government-funded HIV research is ready to scale: a platform capable of teaching the body to heal itself — durably, safely, and at global manufacturing capacity.
🧬 Section I | The Biology of Elusiveness: HIV as the True Proving Ground of Immune Memory
HIV is where modern immunology met its limits. Every concept now driving cancer immunotherapy — antigen breadth, checkpoint balance, memory exhaustion — was first tested here. For four decades this virus has served as the proving ground for immune medicine itself: the field’s longest experiment in how a pathogen can erase memory, hijack tolerance, and turn regulation into camouflage.
1️⃣ The Invisible Integration
Most viruses invade, replicate, and die. HIV integrates. Its envelope glycoprotein gp120 binds CD4 and the co-receptors CCR5 or CXCR4, fuses membranes, and inserts viral DNA directly into the host genome. From that moment every infected cell carries a hidden copy of the virus.
A few cells explode in inflammation; others enter a quiescent state and become latent reservoirs in lymph nodes, gut, and brain — beyond the reach of drugs or antibodies. ART freezes replication but not the code itself. When therapy pauses, those silent proviruses awaken within days, proving that chemical suppression alone cannot cure a genetic ghost.
2️⃣ The Collapse of Coordination
HIV’s genius lies in dismantling conversation.
• Dendritic cells (DCs) lose their voice, producing little IL-12 and presenting antigens poorly.
• CD8⁺ cytotoxic T cells overfire until exhaustion, expressing PD-1 and TIM-3.
• B cells lose guidance as helper networks dissolve.
• The thymus shrinks, narrowing the range of naïve T cells.
Even after ART restores counts, coordination is gone — an orchestra still playing but no longer in tune.
3️⃣ The Paradox of the Regulators
The 2025 Nobel Prize honored the discovery of FOXP3, the transcription factor that defines regulatory T cells (Tregs). Tregs are the immune system’s peacekeepers, releasing IL-10 and TGF-β to prevent self-destruction. In HIV, that restraint becomes the virus’s shield.
FOXP3⁺ Tregs expand throughout infection, especially in gut tissue. They suppress dendritic-cell maturation, paralyze cytotoxic T-cell killing, and even serve as a reservoir themselves — long-lived, apoptosis-resistant, and carrying integrated HIV. The same tolerance that prevents autoimmunity now enforces viral invisibility.
4️⃣ The Lost Signal of Survival
Sensing lymphopenia, the body floods the bloodstream with interleukin-7 (IL-7) — the cytokine that maintains T-cell homeostasis. But chronic activation strips T cells of the IL-7 receptor α-chain (CD127), leaving them deaf to the message. Without IL-7 signaling, naïve and central-memory T cells die faster, the thymus atrophies, and the immune repertoire contracts. What remains is an immune system numerically rebuilt yet cognitively impaired: counts normal, memory gone.
5️⃣ Why Cures Fail
All failed approaches share one blind spot — HIV’s command of the immune environment.
1. ART silences replication but not remembrance.
2. Vaccines ignite but can’t persist.
3. Cytokine therapy lacked selectivity; IL-2 fed both attackers and guards.
Real cure requires re-teaching the system to recognize, remember, and restrain the virus on its own.
6️⃣ The Emerging Blueprint
• Dendritic-cell vaccines provide the vocabulary.
• IL-7 supplies the atmosphere.
• Treg modulation acts as the governor.
Together they form a program of immune re-education rather than brute eradication.
7️⃣ Why HIV Cannot Hide from a Dendritic-Cell Vaccine
A DC vaccine such as DCVax dismantles HIV’s favorite defense — antigenic narrowness. Traditional vaccines target one or two proteins; HIV mutates them away. DCVax uses autologous antigen breadth: patient-derived DCs pulsed with whole inactivated virus or broad peptide libraries, matured to display thousands of epitopes on MHC I and II.
Because the vaccine mirrors the patient’s own viral quasispecies, every latent variant is represented somewhere on a DC surface. Re-infused DCs activate a polyclonal swarm of CD4⁺ and CD8⁺ T cells that recognize multiple conserved regions across the proteome. Even if one mutant escapes, dozens remain visible. Breadth defeats mutation; cross-presentation bridges latency; IL-7 sustains pursuit. In theory — and in data — the virus has nowhere to hide.
HIV once relied on immune forgetfulness; dendritic-cell vaccination takes that forgetfulness away. If re-education works here — against a pathogen that rewrote the rules of memory — it will work anywhere.
🧩 Section II | The First Teachers: Dendritic Cells and How the Vaccine Restores the Lesson
Think of the immune system as a vast school, where every infection is a lesson and every cell a student or teacher. At the front of the classroom stands the dendritic cell (DC) — the teacher who decides what the immune system should pay attention to and how it should respond. When HIV arrived, it didn’t just attack the students (CD4⁺ T cells); it went for the teachers, corrupting the curriculum itself.
1️⃣ How Dendritic Cells Normally Work
DCs patrol tissues, sample antigens, and upon sensing danger migrate to lymph nodes to present fragments on MHC I and II molecules. They supply co-stimulation (CD80, CD86) and cytokines (IL-12, TNF-α) that tell T cells what kind of response to mount. When all three signals — antigen, co-stimulation, cytokine context — are delivered, T cells form lasting memory.
2️⃣ How HIV Silences the Teachers
• Hijacking: DC-SIGN captures HIV but ferries it intact to CD4 T cells (trans-infection).
• Cytokine inversion: IL-12 falls, IL-10/TGF-β rise → tolerance instead of alarm.
• Motivational loss: chronic exposure reduces CD80/CD86; T cells receive weak signals.
• Treg pressure: Tregs engage CTLA-4 and induce IDO in DCs, depleting tryptophan and producing more Tregs.
3️⃣ What a Dendritic-Cell Vaccine Does Differently
A DC vaccine removes those teachers from their toxic environment and re-trains them ex vivo. Monocytes from the patient’s blood are cultured with GM-CSF and IL-4 to become immature DCs, then pulsed with whole inactivated HIV or long peptide libraries. They are matured with strong stimulants that restore IL-12 and TNF-α secretion and up-regulate co-stimulation. When re-infused, these DCs deliver a clear message: This is the threat. Find it. Destroy it. Remember it.
4️⃣ Why HIV Can’t Hide From This
The vaccine teaches the immune system hundreds of viral faces at once. Latent reservoirs can’t mask them all. Even brief antigen expression exposes infected cells to newly trained cytotoxic T cells. Breadth and redundancy guarantee coverage even as HIV mutates.
5️⃣ Why This Matters for the Bigger Picture
Rebuilding DC communication doesn’t just fight HIV; it proves that fixing the teachers fixes memory. If DCVax can overcome the virus that silenced the immune system, it can overcome almost anything.
⮕ Transition to Part 2
The next installment explores how RevImmune’s IL-7 (CYT107) restores homeostasis and how $NWBO #DCVax and IL-7 together achieve durability through the triad of DCs, IL-7, and Tregs.
#NWBO #DCVax #RevImmune #IL7 #HIV #DendriticCells #ImmuneMemory #αDC1 #Immunotherapy #ImmuneRestoration #DurableImmunity #Biotech #MedicalInnovation #AdventBioServices #TeachingTheBodyToHeal
1
1
29
3,709

4 Sep 2025
「家」
ウラル *kota
テュルク *eb
モンゴル ger ↔︎ チベット「テント」gur
満洲 boo
韓 *cipV
倭 *ip-
1
4
1,916
31 Aug 2025
🧬 The Immune OS: $NWBO #DCVax Meets the Nature Comms CD137 TIL Study to Build a Deployable Immune Loop
🎯 Why this matters
Glioblastoma has resisted almost every form of immunotherapy. Checkpoint inhibitors fail in GBM both because there are too few T cells inside the tumor to unleash, and because antibody penetration across the blood–brain barrier is limited. DCVax changes both equations by driving tumor-specific T cells into the brain, where even partial checkpoint access can sustain their activity.
TIL therapies also falter because the tumor environment is too “cold” to provide enough consistent material to work with. DCVax fixes that too, by priming and driving diverse, tumor-specific T cells into the tumor bed.
A recent Nature Communications study shows that these rare tumor-reactive T cells can be identified by CD137 and expanded. On its own, this approach struggles in GBM. But combined with DCVax, it becomes the foundation of a closed immune loop — prime → harvest → expand → redeploy.
📄 Study link: nature.com/articles/s41467-0…
👤 Peer-reviewed by Dr. Robert Prins — co-author of the JAMA Oncology Phase III DCVax-L trial, pioneer in dendritic cell immunotherapy, and now a reviewer on the CD137 TIL paper that validates the harvest step.
🎯 Study Design and Rationale
The Nature Communications 2025 trial evaluated whether glioblastoma (GBM) tumor infiltrating lymphocytes (TILs) could be harvested, enriched, and expanded.
•Cohort: 161 glioma patients; TILs isolated from surgical aspirates (CUSA).
•Methodology: Immunoselection of CD137⁺ TILs (marker of recent antigen engagement).
•Endpoints: Expansion feasibility, cytotoxic function against autologous tumor, tumor response in xenograft models.
•Results: Expansion succeeded in 54% of gliomas overall (59% GBM, 26% IDH1-mutant). Expanded cells retained memory-like phenotypes, killed autologous GBM cells in vitro, and slowed tumor growth in vivo.
•Resistance: Tumor cells upregulated PD-L1 within 3–5 days of TIL engagement, blunting cytotoxicity; PD-1 blockade restored function.
Importantly, this work was peer-reviewed by Dr. Robert Prins, who also co-authored the DCVax-L Phase III trial (JAMA Oncology, 2023). That bridges dendritic cell vaccination and adoptive T-cell therapy in GBM.
⚠️ Note: The published study focused only on isolating and expanding CD137⁺ TILs from glioma tissue. It did not test DCVax or the broader loop described below. What follows is a synthesis — integrating those new findings into the DCVax framework to show how the pieces connect into a deployable immune operating system.
🧬 Mechanistic Integration with DCVax
DCVax-L primes the immune system using autologous dendritic cells pulsed with whole tumor lysate:
•Breadth: Immunopeptidomics revealed thousands of MHC-presented peptides, with hundreds tumor-specific.
•Immune Monitoring: Phase III trial confirmed expansion of hundreds of new TCR clones sustained for months.
•Clinical Survival: Median OS 22.4 months from surgery in newly diagnosed GBM (13% alive at 5 years) vs 16.5 months in controls; 13.2 months in recurrent GBM vs 7.8 months in controls.
CD137⁺ TILs are the product of that priming. Without DCVax, gliomas are immunologically “cold” with scarce reactive TILs. With DCVax, vaccine-educated T cells infiltrate tumors, wear the CD137 badge, and become harvestable material.
🏗️ The Full Loop Architecture
1. Prime — DCVax-L educates the immune system across the tumor’s entire antigen library.
2. Boost — Hiltonol (Poly-ICLC) supercharges dendritic cell maturation and type I interferon signaling.
3. Target — IRIS (splicing-derived antigen discovery; Liau, Prins, Xing) identifies cryptic epitopes to emphasize during priming.
4. Program — EDITH (Engineered Dendritic-cell Immune Therapy Hub; Flaskworks patent) embeds booster logic into dendritic cell manufacture.
5. Gate — Advent BioServices (UK GMP, HTA, SI 87, QP release) is the live regulatory gate currently releasing DCVax doses under Specials pathway.
6. Harvest — Isolate CD137⁺ TILs from resection, proof of in-vivo tumor recognition.
7. Tune — iHOTT (immune High-Order Targeting/Tuning) computationally profiles TCR repertoires, enriching optimal tumor-killing clones.
8. Expand — Eden (Flaskworks automated closed-system) scales TILs reproducibly to billions under GMP.
9. Sustain — Anti-PD-1/PD-L1 checkpoint blockade neutralizes adaptive PD-L1 rebound (Day 3–5).
10. Preserve — RevImmune (CYT107, recombinant IL-7) restores systemic T-cell homeostasis and supports survival of infused and vaccine-primed memory clones.
11. Repeat — Each recurrence can be resected, generating new vaccine lots and new TIL harvests.
12. Scale — Advent Eden EDITH make this replicable as a regulated global immune operating system.
📊 Comparative Insights
Against TIL-First Approaches
TIL therapy works in melanoma because those tumors are naturally “hot” — inflamed and loaded with reactive immune cells. GBM is the opposite: cold, sparse, and dominated by exhausted clones.
•Melanoma TIL therapy (lifileucel, NCT03645928): Expansion success >90%, ORR ~31%, with durable CRs in 12%.
•Glioma TIL attempts (historical): Expansion unreliable; infused bulk TILs showed little efficacy.
•Improvement with Prime Harvest: DCVax first creates tumor-reactive TILs, increasing yield and quality. CD137 selection enriches the true effectors.
Why TIL-only in GBM Doesn’t Make Sense
The Nature Comms study confirmed this limitation — even under optimized conditions, expansion succeeded in only ~54% of gliomas, dropping to ~26% in IDH1-mutant disease. That ceiling makes TIL-only approaches unreliable. Without DCVax priming, there is little substrate to expand. CD137 selection improves purity but cannot solve scarcity. In GBM, a TIL-only playbook multiplies zero. DCVax fixes the equation by generating the clones that CD137 selection can capture and Eden can scale.
Against Checkpoint-Only Approaches
•CheckMate 143 (Nivolumab in GBM, NCT02017717): No OS benefit over bevacizumab.
•CheckMate 498/548: Failed primary endpoints in newly diagnosed GBM.
•Reason: Too few reactive T cells in GBM to “unleash.”
•Improvement with Loop: DCVax TIL infusion ensures abundant, activated T cells are present before checkpoint therapy is applied.
Against Vaccine-Only Approaches
•ICT-107 (NCT01280552): Modest signals but underpowered; single-antigen vaccines prone to tumor escape.
•DCVax-L Phase III (NCT00045968): Statistically significant survival benefit across NDGBM and recurrent cohorts.
•Limitation: Incremental median survival gain, not curative for most.
•Improvement with Loop: Vaccine provides breadth, but scaling via TIL infusion plus checkpoint and RevImmune aims for deep, durable responses. Vaccine-only approaches create the blueprint, but without amplification and sustainment the effect remains incremental. In GBM, breadth without scale is not enough.
⚠️ Safety and Limitations
•DCVax-L: Mild AEs, injection-site reactions; well tolerated in elderly.
•Hiltonol: Flu-like symptoms; widely tested as adjuvant.
•TIL Therapy: Requires lymphodepletion (risk of infection, cytopenia), hospitalization, IL-2 historically used (toxic). Using IL-7 (RevImmune) instead mitigates risk.
•Checkpoint Inhibitors: Risk of immune-related AEs (colitis, pneumonitis, endocrinopathy). In GBM, watch for cerebral edema.
•Operational: Requires tumor tissue at baseline (for vaccine) and recurrence (for TIL harvest). Cold tumors (pancreas, MSS colorectal) may need stronger priming or combinatorial boosters.
🧩 Strategic Interpretation
•Clinical Impact: This loop converts GBM from an incremental fight into a potentially durable system of immune control.
•Regulatory Implications: Advent (UK) shows pathway is already live under SI 87. FDA’s CNPV/CIPV frameworks may allow rapid approval if survival GMP readiness demonstrated.
•Platform Fit:
•DCVax = instruction engine.
•Hiltonol/EDITH = booster logic.
•IRIS = targeting intelligence.
•Advent = regulatory gate.
•CD137/iHOTT/Eden = amplification system.
•Checkpoint/RevImmune = sustainment and preservation.
•Adoption: Initially at specialized nodes (Advent, NCI-like centers), scalable globally as Eden automation and EDITH modular hubs deploy.
✅ Decision-Ready Takeaway
The Nature Communications study proved that CD137⁺ TILs from gliomas can be harvested and expanded — but it also exposed the ceiling of TIL-only strategies in GBM. Without priming, success rates collapse and the biology stalls. That silence is telling: the logic of the study only fully coheres in a system where dendritic cell vaccination has already driven tumor-specific T cells into the brain.
Seen in that light, this is no longer a collection of experimental silos. It is the architecture of a regulated, modular immune operating system:
DCVax primes → Hiltonol boosts → IRIS targets → EDITH programs → Advent gates → CD137 harvests → iHOTT tunes → Eden expands → Checkpoint sustains → RevImmune preserves → Repeat and Scale.
With Advent as the live gate, EDITH and Eden as manufacturing engines, IRIS and iHOTT as intelligence layers, and checkpoint RevImmune as sustainment, this loop is not theoretical. It is executable, regulatorily grounded, and globally scalable — and the CD137 study inadvertently validated why DCVax is the indispensable first cause.
⚠️ Disclaimer: This is an expert synthesis of published and peer-reviewed research. It is not investment advice or a treatment recommendation.
1
4
38
2,044
30 Aug 2025
🎬⚡ The Spinner Has Fallen: How $NWBO #DCVax Could Move From 1–2 Month Approval to Global Expansion
TLDR — The Spinner Test
In Inception, Cobb’s spinning top was his totem. If it spun forever, he was still trapped in a dream. If it wobbled and fell, he was awake in reality.
Cancer approvals have been stuck in that dream for decades — 18-month reviews, endless delays, patients dying while time spun away. The top never fell.
Now it has. The FDA’s Commissioner’s Priority Voucher (CIPV) and the UK’s Plan B are regulatory twins designed to collapse approvals to 30–60 days once survival data and GMP readiness exist. Advent at Sawston is already live and integrated into NWBO, releasing vaccines under license. In the U.S., approval under CIPV will require a domestic node — and Winterfell, Merck’s Building 50 at West Point, Pennsylvania, is the obvious anchor.
From there, the system scales like a franchise: Canada under ATP, Europe under EMA, Asia through joint ventures. Each new node both produces vaccines and validates the model with local outcomes and reimbursement wins.
The sequence is simple: Accelerate → Franchise → Validate → Consolidate. Just like Kite Pharma (bought for $12B) and Juno (bought for $9B), expansion leads to buyout. NWBO is now at that inflection point — except this time the approvals that unlock the cycle are measured in weeks, not years.
⚡ Regulatory Twins Rewrite the Clock
For most of biotech history, the calendar was the killer. FDA reviews stretched over a year, and MHRA approvals often took longer. Regulators were siloed; questions bounced back and forth for months. Patients had no time, and the system gave them none.
CIPV and Plan B are the counterfactual. CIPV, limited to five per year, commits the FDA to final decisions within 30–60 days. It works by holding cross-disciplinary “tumor board” reviews, allowing rolling CMC and labeling submissions, and collapsing what was sequential into parallel.
Plan B, under the UK’s Statutory Instrument 87, achieves the same outcome through conditional approvals. If survival data exist and confirmatory evidence is already being collected, MHRA can approve now and monitor in real time. Advent’s Specials program has been generating that confirmatory data since 2022.
Different names, different agencies, but the same philosophy: stop spinning, start acting.
🏗️ Advent as Proof of Execution
A fast lane only matters if the car is built. For most small biotechs, that is where the story ends. But NWBO already has the car — Advent at Sawston.
Licensed by MHRA and HTA, Advent has manufactured and released DCVax-L doses for real patients under QP authority. In 2025, NWBO acquired Advent outright, folding IP, staff, and licenses into the parent. No dependency risk. No balance sheet shadows. Total integration.
Think of Sawston as the AWS Virginia data center of immunotherapy. It is the flagship node. Every vaccine batch released is proof the system is real, not hypothetical. Regulators don’t have to ask “can you do this?” — the logs already show “we did.”
🇺🇸 The U.S. Anchor: Winterfell at West Point
The U.S. is too large to be served from abroad. FDA approval under CIPV will only be operationally viable with domestic manufacturing capacity. That’s where Winterfell comes in.
Merck’s Building 50 at West Point, Pennsylvania — modular cleanrooms, cryogenic storage, Eden-compatible automation — is widely seen as the logical American counterpart to Sawston. Whether NWBO builds its own node or aligns with Winterfell, the strategy is the same: replicate Sawston under FDA oversight, prove fidelity, and scale to U.S. demand.
This makes the U.S. not just another franchise, but the flagship franchise territory. CIPV approval unlocks it, Winterfell anchors it, and the U.S. revenue base reinforces NWBO’s bargaining power abroad.
🌍 Franchising as the Expansion Model
Scaling personalized cell therapies demands decentralization with fidelity. That is franchising logic. NWBO is the franchisor: it owns the recipe, the IP, and the QA standards. Partners act as master franchisees:
•Canada: through its Advanced Therapeutic Pathway, with BioCanRx or GMP consortia as licensees.
•Europe: via EMA-compliant suites in Germany or the Netherlands.
•Asia: through Japan’s regenerative medicine approvals or Chinese JVs, echoing the Fosun Kite CAR-T precedent.
Franchisees build the plants, take the capital risk, and operate under license. NWBO enforces fidelity and collects royalties. The model aligns regulators, investors, and patients: local production, global reach, strict process fidelity.
📊 Validation Loop
Every node is more than a factory — it is a validation engine. Sawston already proves the Phase III survival benefit holds in the real world. NICE will fold Specials data into cost-effectiveness models. Insurers in the U.S. will follow suit.
Each franchise node repeats the loop: patients treated, outcomes logged, reimbursement secured. Revenue flows confirm viability. Validation is not a one-time milestone; it is a flywheel, gaining momentum with each geography added.
🤝 Consolidation: The Buyout Horizon
Franchise systems always consolidate. In fast food, franchisors buy back stores. In biotech, innovators are acquired once validated. Kite licensed CAR-T regionally, then Gilead paid $12B. Juno partnered regionally, then Celgene paid $9B.
NWBO’s sequence is identical:
•Accelerate under CIPV and Plan B.
•Franchise nodes in U.S., Canada, Europe, Asia.
•Validate survival and reimbursement at scale.
•Consolidate via merger, buyout, or management-led reacquisition.
Linda Powers’ governance ensures continuity in any transaction. Shareholders’ upside crystallizes when consolidation comes.
🔑 Conclusion — The Spinner Has Fallen
In Inception, Cobb’s top spun forever in dreams, but fell in reality. For decades, oncology approvals spun endlessly, a dream of progress while patients died waiting.
That era is finished. CIPV and Plan B are the moment the spinner hits the table. Approvals that once took 18 months now take 30–60 days. Advent is live. Winterfell anchors the U.S. Canada, Europe, and Asia follow under franchise models. And just as in every franchise system, growth ends in consolidation — mergers and buyouts that crystallize value.
The immune OS is alive. The spinner has fallen. Time has changed. What once took years now takes days.
⚖️ Disclaimer: This analysis is for informational purposes only. It does not constitute investment advice or medical guidance. Outcomes depend on regulatory decisions and corporate actions.
2
5
47
3,280

27 Aug 2025
MAYBE IT HAS SOMETHING TO DO WITH "COLD ADAPATED VIRAL ATTENUATION" USED MAKING LIVE-ATTENUATED VACCINES?!
We generated Cold-Adapted Viral Attenuation (CAVA) poliovirus strains by serial passage at low temperature and subsequent genetic engineering, which contain the capsid sequences of cIPV strains combined with a set of mutations identified during cold-adaptation. These viruses displayed a highly temperature sensitive phenotype with no signs of productive infection at 37°C as visualized by electron microscopy. Furthermore, decreases in infectious titers, viral RNA, and protein levels were measured during infection at 37°C, suggesting a block in the viral replication cycle at RNA replication, protein translation, or earlier. However, at 30°C, they could be propagated to high titers (9.4–9.9 Log10TCID50/ml) on the PER.C6 cell culture platform.
pmc.ncbi.nlm.nih.gov/article… @dlingenfelter @Biorealism
1
2
158






25 May 2025
Thanks @JGarciaMD for your feedback
Thanks @KellySaid6 for sharing your case
Nowadays, I think PFA should be the gold standard for this anatomy due to more risk of complications w/RFA.
Esophagus is closer in CIPV.
On the other side, RFA is feasible if not availability for PFA
1
2
133
24 May 2025
Confluent inferior pulmonary veins (CIPV) & RFA.
A very rare anatomical variant w/
RFA challenges. CIPV wall thickness is 0.7 mm as reported in @JICE_EP
Open access:
doi: 10.1007/s10840-023-01613-w.
1st case we face. What is your approach ?
Done w/ @nlcabanillas
4
10
39
3,622

19 Dec 2024
Meu Deus, como vocês "patriotas" são ridículos. O que o Reino Unido fez foi biopirataria, isso é um crime de acordo com a CIPV.
2
34

26 Nov 2024
Moving Object Network
The moving object network (206b) is extensively detailed in patent US20230057509A1, which focuses on autonomous driving ML models using adjustable virtual cameras.
This patent distinguishes observed objects into VRUs (Vulnerable Road Users - pedestrians, strollers, etc.) and non-VRUs (non-vulnerable road users, vehicles, etc.), applying different virtual camera heights (1.5m vs. 15m) and views (panoramic vs. periscope) for each category, as illustrated in Figures 3B and 4B.
For VRU networks (Figure 3B), the system employs relatively low-height (e.g., 1.5m) virtual cameras in panoramic view, deliberately distorting targets to appear larger than actual size. This enhancement enables rapid response to sudden VRU appearances. The improved FSD response to wildlife since v12.3 likely stems from this technology.
Conversely, non-VRU networks (Figure 4B) utilize higher-height (e.g., 15m) virtual cameras in periscope view, distorting targets to appear smaller than actual size. While the specific purpose isn't detailed, this likely facilitates recognition and response to multiple vehicles across a broader field of view.
Additionally, the patent presents a SuperNarrow ML model for emergency response, such as sudden lane intrusions. This model appears to focus on identifying the Closest In-Path Vehicle (CIPV) and continuously monitoring its distance, velocity, and acceleration for accident prevention.
The moving object network (206b) appears to have been implemented since FSD v12.3, demonstrating remarkable effectiveness.


7 Oct 2024

Vision-Based Machine Learning Model for Autonomous Driving with Adjustable Virtual Camera
@Tesla's US20230057509A1 patent introduces an innovative vision-based machine learning model for autonomous driving that uses only cameras, eliminating the need for LiDAR and radar.
The system uniquely processes information for vulnerable road users (VRUs) like small animals and pedestrians and non-VRUs like vehicles separately, optimizing detection for each category. 🧵
[FIG. 1A: Block diagram illustrating an example autonomous vehicle which includes a multitude of image sensors an example processor system]
[FIG. 1B: Block diagram illustrating the example processor system determining object/signal information based on received image information from the example image sensors]

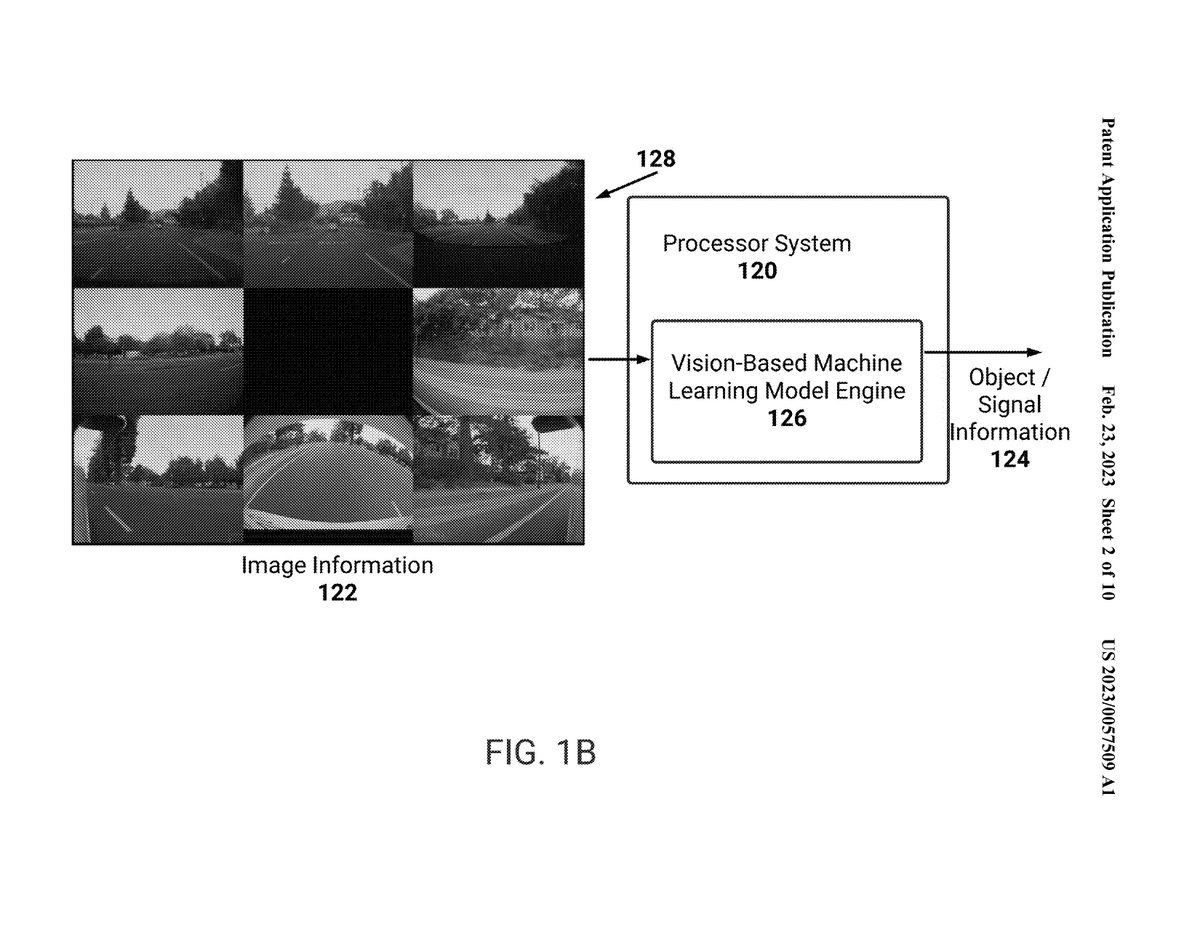
1
4
559
23 Nov 2024
이동 객체 네트워크(206b)에 대한 자세한 내용은 조정 가능한 가상 카메라를 통한 자율주행 ML 모델에 관한 US20230057509A1 특허에 잘 나타나 있습니다.
해당특허는 수집된 비전 데이터를 바탕으로 관측된 객체를 VRU(취약한 도로 사용자 - 보행자, 유모차 등)와 non-VRU(비-취약한 도로 사용자, 차량 등)으로 구분하고, 각각에 대해서 다른 가상 카메라 높이(1.5m vs 15m)와 뷰(파노라마 뷰 vs 잠망경 뷰)를 적용하는 기술을 개시하고 있습니다. 이러한 예시는 도면 3B와 4B에 잘 나타나 있습니다.
VRU에 대한 네트워크(도면 3B)의 경우, 상대적으로 낮은 높이(1.5m 등)의 가상 카메라를 통해 파노라마 뷰 형태로 인식함으로써, 대상을 실제보다 크게 왜곡하여 인지하는 것으로 기재하고 있습니다. 이 기술을 통해 주행 중 갑작스러운 VRU 등장에 대해 신속하게 대응할 수 있습니다. FSD v12.3 이후 야생동물들에 대해서 FSD가 잘 대응하는 것은, 이 기술의 영향이 아닐까 생각하고 있습니다.
대조적으로, non-VRU에 대한 네트워크(도면 4B)의 경우, 상대적으로 높은 높이(15m 등)의 가상 카메라를 통해 잠망경 뷰 형태로 인식함으로써, 대상을 실제보다 작게 왜곡하여 인지하고 있는 것으로 기재하고 있습니다. 이 기술의 구체적인 목적은 자세히 설명되어 있지 않지만, 보다 넓은 시야에서 보다 많은 수의 차량을 인식하고 대응하기 위함으로 보입니다.
또한, 해당특허는 갑자기 차량이 차선에 난입하는 등, 비상사태에 대응하기 위한 안전 시스템으로, SuperNarrow ML모델도 제시하고 있습니다. 해당 모델은, 가장 가까운 경로 차량(CIPV)을 인지하고, 해당 차량과의 거리, 해당 차량의 속도와 가속도 등을 지속적으로 체크함으로써, 사고를 방지하는 것이 주요 기능으로 추정됩니다.
이러한 이동 객체 네트워크(206b)는 이미 FSD v12.3부터 적용된 것으로 추정되며, 매우 높은 완성도를 보여주고 있는 것으로 보입니다.
x.com/seti_park/status/18430…
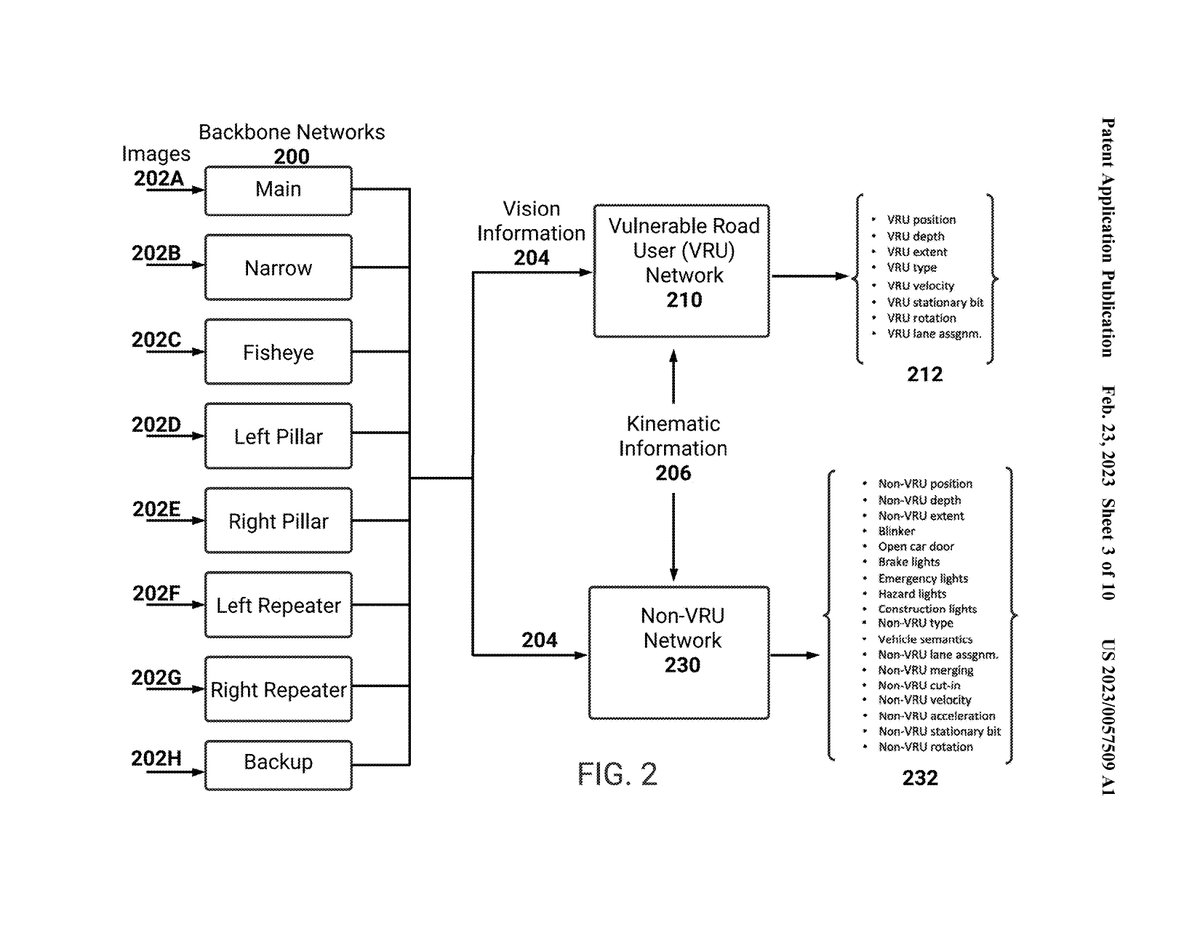
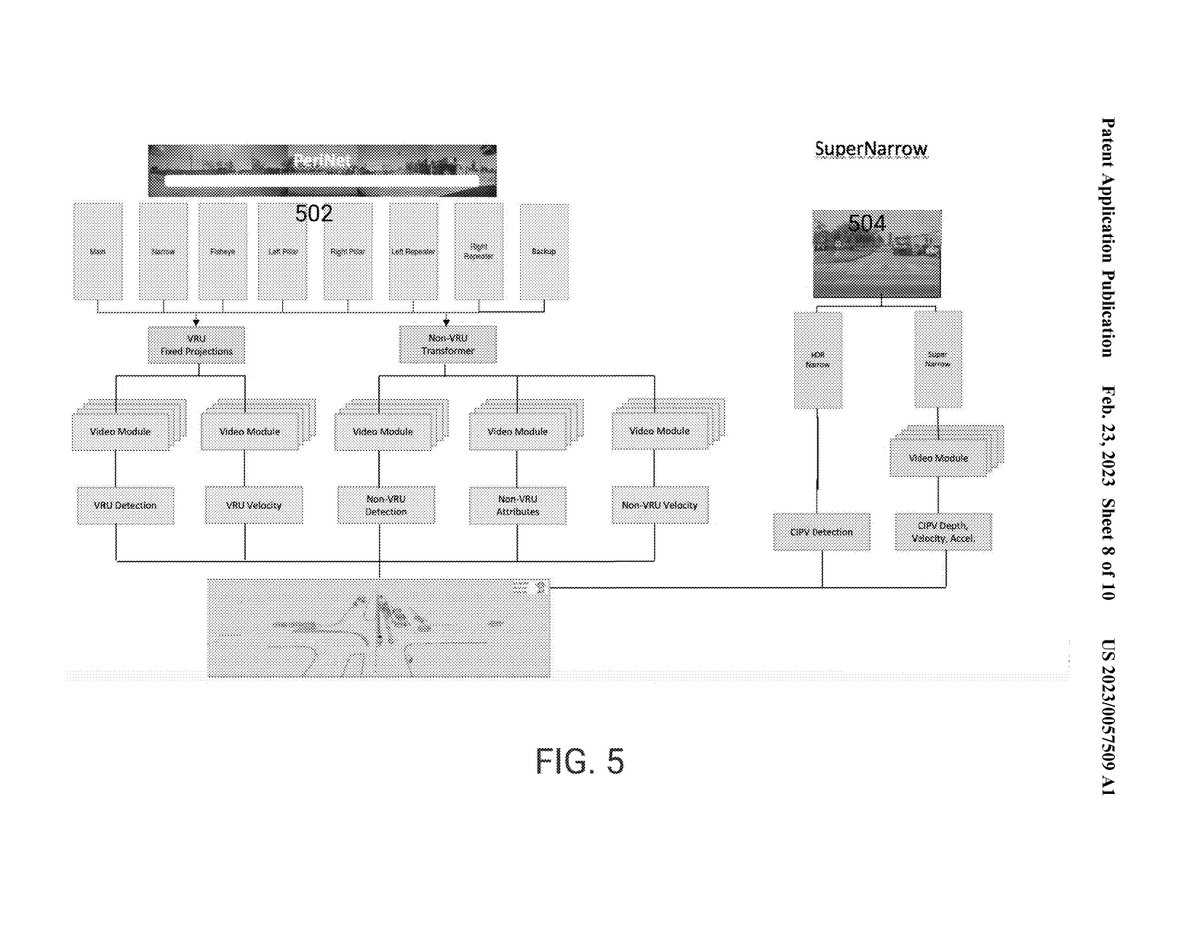
7 Oct 2024
Vision-Based Machine Learning Model for Autonomous Driving with Adjustable Virtual Camera
@Tesla's US20230057509A1 patent introduces an innovative vision-based machine learning model for autonomous driving that uses only cameras, eliminating the need for LiDAR and radar.
The system uniquely processes information for vulnerable road users (VRUs) like small animals and pedestrians and non-VRUs like vehicles separately, optimizing detection for each category. 🧵
[FIG. 1A: Block diagram illustrating an example autonomous vehicle which includes a multitude of image sensors an example processor system]
[FIG. 1B: Block diagram illustrating the example processor system determining object/signal information based on received image information from the example image sensors]
1
32
2,223

13 Nov 2024
Quem o CIPV está pendente tenta no WhatsApp da ANVISA, no msm dia resolvem.
3
2
1,659