
Jun 12
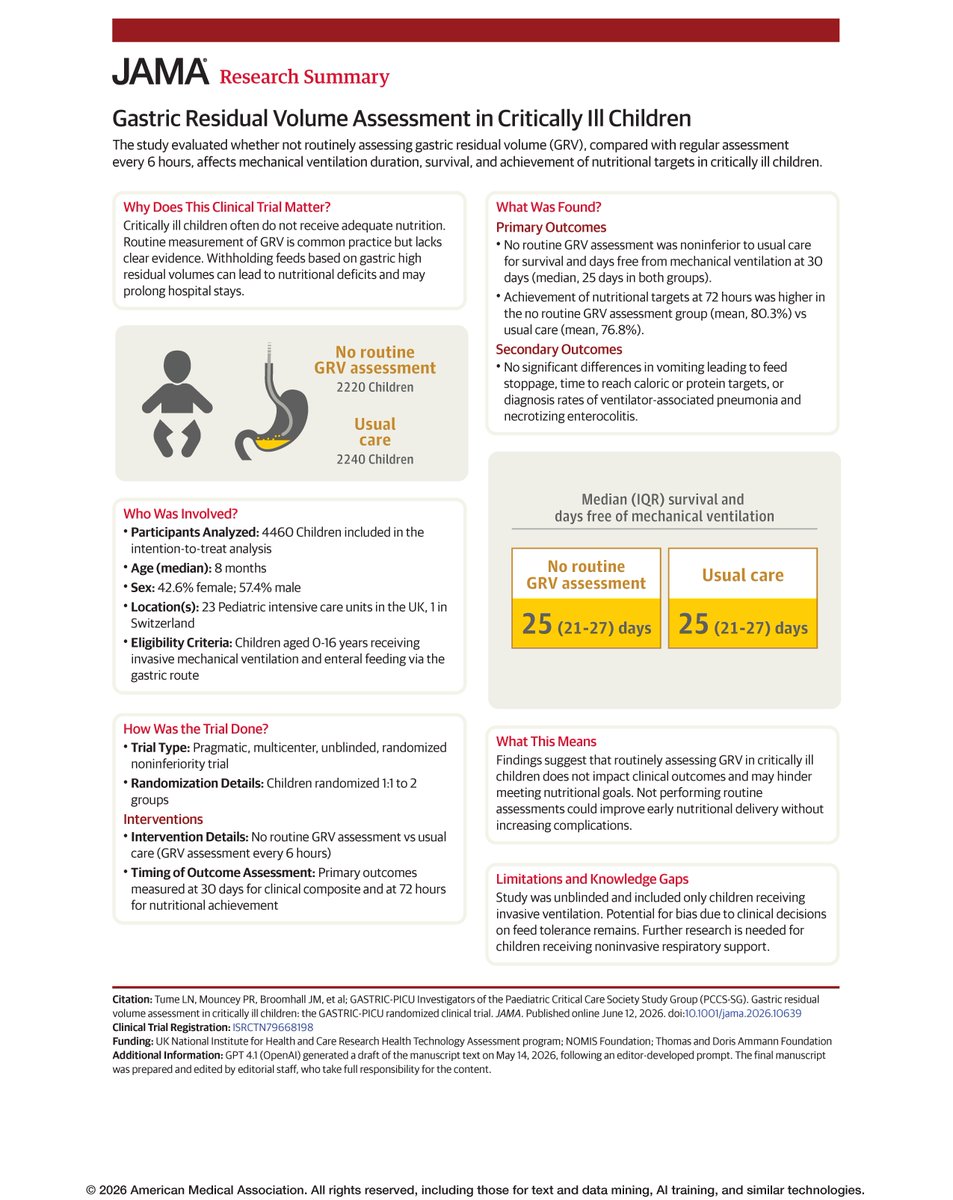
📊 Research Summary: In critically ill children, omitting routine #GRV measurement did not affect survival or ventilator-free days and improved nutritional target achievement, supporting deimplementation.
#CCR26 @CritCareReviews
ja.ma/4oti4ma
3
8
2,772

@VR_Cornelius Please reconsider routine mucolytic prescribing in resp failure, the evidence is not there. Reinforcement from panel that modern trials are less about implementing and more about deimplementation of non-evidence based interventions #CCR26 @CritCareReviews @ICNARC
42

Apr 17
Checks, checks and more checks! How many are really necessary?
#deimplementation #NHS
2
2
153

When Competing Risks Compete With Common Sense: A Critical Look at Gupta et al., JAMA 2026
Lately I've been a bit obsessed with oncology studies. Why? I don't know. I'm very interested in knowing how science is made outside cardiology — what the standards are, how evidence is framed, where the reasoning is tight and where it isn't. It's been a humbling and fascinating exercise. So, if a made any mistakes, people who know, please correct me! Criticism is always welcome.
Yesterday, Gupta et al. published a large retrospective cohort study in @JAMAJournal examining colorectal cancer (CRC) risk among adults ≥75 with vs without adenoma at prior colonoscopy (n = 91,952 US veterans).
The headline: CRC incidence and CRC death were low in both groups and were "far exceeded" by non-CRC mortality. The conclusion: older adults may consider "deprioritizing surveillance colonoscopy relative to other health concerns."
The study is generating enthusiasm among screening skeptics. The framing is seductive — a 96:1 ratio of non-CRC death to CRC death. Who would argue with that?
I would. Here's why.
The study in brief
Individuals who had a colonoscopy between ages 65 and 75 were classified at age 75 based on their most recent colonoscopy findings: adenoma detected (n = 25,538) vs no adenoma (n = 66,414). Follow-up began at the 75th birthday.
At 10 years: • CRC incidence: 1.1% (adenoma) vs 0.7% (no adenoma) — Gray test P < .001 • CRC death: 0.5% vs 0.4% — P = .005 • Non-CRC death: ~48% in both groups
The authors framed the overwhelming non-CRC mortality as evidence that surveillance colonoscopy offers negligible benefit in this population.
What the authors hypothesized vs. what they found
This is worth reading carefully. In the Methods, the authors state they "postulated finding similar CRC risk for older adults with adenoma at prior colonoscopy as for those without adenoma would support analogous recommendations regarding surveillance."
In other words: if the adenoma group had the same CRC risk as the no-adenoma group, you could argue that surveillance is unnecessary — just as the USPSTF already recommends against repeat screening in those with prior normal colonoscopy.
Their own data refuted this hypothesis. The adenoma group had significantly higher CRC incidence and CRC death. The groups were not equivalent. The conditional failed.
Rather than accepting this as a negative result, the authors pivoted to a different argument: "Yes, adenoma patients have higher risk, but both risks are so low in absolute terms, and competing mortality is so dominant, that the difference is clinically irrelevant."
Do I agree that that pivot may be reasonable? Maybe. But it's a different argument than the one they set up.
Statistical significance ≠ clinical magnitude
With 91,952 patients, even trivial absolute differences become statistically significant. A 0.4 percentage-point difference in CRC incidence (0.7% vs 1.1%) and a 0.1 percentage-point difference in CRC death (0.4% vs 0.5%) — these P-values reflect sample size, not clinical magnitude.
But here's the other side: 0.7% CRC incidence in the "normal colonoscopy" group isn't zero. The very benchmark group the USPSTF says doesn't need more screening still develops CRC. Does that weaken the entire premise of using them as the "safe to stop" reference? I don’t know. Honestly. You tell me. But it’s not so distant from the 1.1%.
10-year estimates from 2.5-year follow-up
The median follow-up was 2.50 years for the adenoma group and 3.23 years for the no-adenoma group. At 10 years, only 3.2% and 5.7% of each group, respectively, remained at risk.
This means the 10-year cumulative incidence estimates that anchor the paper's central message — 1.1% CRC, 48% non-CRC death — are extrapolated from a tiny, heavily censored tail of the survival curve, which creates distortion & instability in the projections.
The 5-year estimates are more robust: 0.6% vs 0.3% for CRC, ~22% for non-CRC death. Still low, still dominated by competing mortality, but the contrast is far less dramatic than the 10-year headline.
CRC death in the adenoma group at 10 years: 45 events. An entire clinical recommendation is being built on fewer than 50 events.
The competing risk framework
Let me be clear: the statistical method is correct. When nearly half the population dies of non-CRC causes within 10 years, you must account for competing risks. Standard Kaplan-Meier would overestimate CRC incidence by treating non-CRC deaths as censored. The cumulative incidence function with competing risks (Fine & Gray) avoids that. So yes, again: this is the correct way to do it.
The problem isn't the method but rather how it's used interpretively.
There's a critical distinction between two uses of competing risk analysis:
Analytical use: "We need competing risks to estimate CRC incidence accurately in this elderly population." Correct. Necessary.
Rhetorical use: "Competing mortality is so high that CRC doesn't matter, therefore stop surveillance." This is a clinical judgment dressed up as a statistical finding.
By placing CRC incidence (1.1%) next to non-CRC death (48%) in every table and figure, the paper creates a visual contrast that makes CRC look trivial. But what disease in a 75-year-old wouldn't look trivial against the aggregate of all other causes of death? You could run this exact analysis for virtually any single condition and reach the same conclusion: "competing mortality dominates, so don't bother."
The question the paper answers: "Is CRC common relative to all-other-cause mortality?" The answer is no. Obviously.
Now, the question the paper doesn't answer is this: "Does surveillance colonoscopy reduce CRC risk in this population?" That's the question that actually matters for clinical decision-making, and this study design cannot address it.
Cause-specific hazard
The paper reports subdistribution hazards (Fine & Gray), which estimate the probability of developing CRC in a world where competing deaths happen. Patients who die of non-CRC causes remain in the denominator. As more people die of other causes, the CRC probability gets diluted. Again, this is correct.
What the paper doesn't report is the cause-specific hazard: the instantaneous rate of CRC among people who are currently alive and CRC-free.
Why does this matter? Consider this: among 1,000 patients aged 75 with prior adenoma, if 480 die of non-CRC causes and 11 develop CRC over 10 years, the cumulative incidence is 1.1%. But among the 520 who survived long enough to potentially develop CRC, the rate is ~2.1%.
That second number is what matters for surveillance decisions. Let's agree you're not screening dead people (unless you have some really weird stuff going on). You're screening the living & relatively well (you're not screening those soon-to-be dead either, are you?). The relevant denominator is patients who are alive and could benefit, not the entire cohort diluted by competing deaths.
The cause-specific hazard would tell us whether CRC biology is genuinely attenuated in this population or whether CRC merely looks rare because people keep dying of other things before it manifests. The paper cannot distinguish between these two scenarios.
Surveillance bias
The study cannot distinguish surveillance colonoscopies from diagnostic ones after age 75. If some patients in the adenoma group received surveillance that detected and removed pre-malignant lesions, this would lower observed CRC incidence, paradoxically making surveillance look unnecessary when it may have been the reason CRC rates were low.
The authors' exploratory analysis (Fisher exact test on colonoscopy counts) is too coarse to address this. This is the fundamental limitation of an observational study asking an interventional question.
A word on costs, risks, and overtreatment
Now, to be fair: colonoscopy in the elderly is not without harm. Procedural risks increase with age and frailty — some studies report 3.8% to 6.8% of older adults require an ED visit or hospitalization within 30 days. Colonoscopy is also a finite, costly resource. And the broader concern about overtreatment and overdiagnosis in elderly populations is legitimate and important.
But here's the thing: this study doesn't address any of these questions either. It doesn't quantify procedural complications. It doesn't estimate cost-effectiveness. It doesn't model the tradeoff between CRC prevented and colonoscopy-related harm. It describes natural history — the probability of developing CRC — and then uses competing mortality to argue the probability is too low to justify surveillance. The harm-benefit calculus that would actually support or refute that conclusion is simply not in the paper.
So if we can't use this study to say surveillance works, we also can't use it to say surveillance isn't worth the risk. Both claims require evidence this study doesn't provide.
A thought experiment: what if we applied this logic to aortic stenosis?
Since I'm a plumber, I thought I'd illustrate why the competing risk argument is structurally flawed as a decisional tool. Consider the following fictional — but structurally identical — abstract:
Aortic Stenosis–Related Mortality and Competing Risk Among Older Adults With vs Without Aortic Valve Calcification on Prior Echocardiography
Among 90,000 US veterans ≥75 years who underwent echocardiography, cumulative incidence of AS-related death at 10 years was 1.8% among those with aortic calcification vs 0.4% without. Non-AS death was 47.3% across both groups. The cumulative incidence of non-AS death far exceeded AS-related mortality across all frailty strata.
Conclusion: Older adults may consider deprioritizing echocardiographic surveillance and TAVI referral relative to other health concerns.
The numbers above are fictional. But the real data is, if anything, worse. In the egnite database (JACC 2023, ~595,000 patients), 4-year untreated all-cause mortality for severe AS was ~45%, and only 60% of patients with severe AS received AVR within 4 years. If you decomposed all-cause mortality into "AS-specific death" vs "non-AS death" using the same competing risk framework, non-AS death would dominate — because these elderly patients are, well… very sick, in general. You know.
Yet no cardiologist would accept the conclusion. We know untreated severe AS is lethal. We know TAVI changes outcomes. We don't tell a 78-year-old with moderate AS: "You'll probably die of something else anyway, so let's skip the follow-up echo."
Why does this argument feel absurd for aortic stenosis but persuasive for CRC? Not because the math is different. It's because we have RCT evidence (PARTNER, Evolut) proving that intervening on AS works. For CRC surveillance in the elderly, we don't have that RCT evidence yet.
That's not an argument against surveillance. It's an argument for running a trial. Which the authors reference: the COOP trial (NCT05612347), randomizing older adults with prior polypectomy to colonoscopy vs FIT. Nice.
One more thing
Some might argue the AS analogy fails because TAVI is a treatment, while colonoscopy is "just" a diagnostic test. But colonoscopy is simultaneously diagnostic and therapeutic. When a gastroenterologist finds an adenoma during surveillance, they remove it in the same session. Polypectomy interrupts the adenoma-to-carcinoma sequence. Even when colonoscopy detects early-stage CRC rather than adenoma, early detection enables curative surgery vs late-stage palliative care.
Surveillance echocardiography, by contrast, is purely diagnostic — it measures a gradient but treats nothing. Yet no one questions its value in elderly patients with known valve disease because the diagnostic information changes management.
If we accept purely diagnostic surveillance for AS, it would be inconsistent to reject a procedure that is simultaneously diagnostic and therapeutic for CRC — using the same competing-risk argument we'd never accept for valvular heart disease.
Why do I care about this?
I'm an interventional cardiologist. This is not my lane.
But I'm also alive. And I would like to know what I can do to stay that way for as long as possible. When a study in JAMA tells me that surveillance for a known pre-malignant condition might not be worth it because I'll "probably die of something else," I want to make sure the reasoning behind that claim is airtight. To me, in this case, well…it isn't.
What this study proves
• Among VA patients ≥75 with prior colonoscopy, absolute CRC incidence is low regardless of adenoma status. • Competing non-CRC mortality dominates across all frailty strata. • The absolute difference in CRC risk between adenoma and no-adenoma groups, while statistically significant, is clinically small.
What this study does NOT prove
• That surveillance colonoscopy after 75 is ineffective. The low CRC incidence may partly reflect the benefit of ongoing surveillance. • That stopping surveillance is safe. This requires a randomized deimplementation trial. • That these results apply to women (98% male cohort), non-VA populations, or patients with high-risk adenomas (only 10.8% of the adenoma group).
What we still need
The COOP trial. A pragmatic RCT directly testing surveillance colonoscopy vs FIT in older adults with prior polypectomy. Until that trial reports, the Gupta paper gives us natural history — valuable, but insufficient for practice change.
The competing risk framework is the right statistical tool for estimating disease incidence. It is the wrong decisional tool for determining whether surveillance has value. Confusing one for the other is not evidence-based medicine — it's numeracy without clinical judgment.
Best
SG
#CardiologyX #MedEd #EBM
1
3
4
696

Feb 25
Growth is sometimes about refining tools and practice.
That includes knowing what to undo in your classroom.
Join @MmeLockhartLDS for Deimplementation for Literacy Growth- professional learning centring teacher expertise and the courage to evolve practice. bit.ly/MentoreeEventbrite

2
3
126

17 Dec 2025
Teacher’s understanding is superior than teacher’s compliance.
You can enforce compliance, but you will never enforce teacher effectiveness. We all have seen it.
If the goal is effective instruction, then ed leaders need to lead in such a way that they inspire and support teachers’ instructional philosophical shifts. This type system wide change can only endure and succeed when leadership is self aware and knows what they don’t know and what they do know and more importantly, when they seek to understand what effective instruction looks and sound like, based on learning research. Why? So that they not only set high the instructional bar, but that they can also inspire, and lead with the how and why of implemention and deimplementation.
This will require they do away with the “one training and done” mentality because that is just a sort of “checking a box and washing one’s hands off” the number one responsibility ed leaders have, which is to make sure that all teachers are equipped with the skills, knowledge, programs and tools that support effective instruction and all students receive the type of instruction that they need and deserve.
16 Dec 2025

Really good article. Compliance can never be the goal during instruction and things rarely go as planned.
1
3
6
1,147
15 Dec 2025
↪️Deimplementation for Literacy Growth with
@MmeLockhartLDS is back for another round.
Join Kim as she presents on why deimplementation can fuel literacy skills and effective, evidence-based instruction by intentionally phasing out or changing practices. bit.ly/MentoreeEventbrite
1
2
319

#PedsICU best of Nov 2025 collection is here. It doesn't include #CCRdownunder articles. picujournalwatch.com/journal… Includes deimplementation delphi, trials, trial protocols, multicentre studies incl content relevant to ECLS/ECMO etc. @OsamaHosheh @DrToyinOcholi @Dr_Hari_Krishna
8
17
1,430
4 Dec 2025
Last night, @MmeLockhartLDS led the third session of a 3-part Mpact on Deimplementation for Literacy Growth. Understanding de-implementation is essential for literacy growth. It helps educators make space for the most effective, research-backed practices. Winter sessions coming.

2
3
107

13 Nov 2025
Deimplementation: It’s for States, Too!
13 Nov 2025

Former Louisiana state leaders @Kunjan19 and Jessica Baghian weigh into the WonkaThon, and it’s 🎯 .
“Adding literacy onto a pile of pre-existing state priorities won’t help more kids read—the pile has to go...
As the saying goes, you can do anything but not everything.”
@MichaelPetrilli @educationgadfly @kellibottger


1
6
636
2 Nov 2025
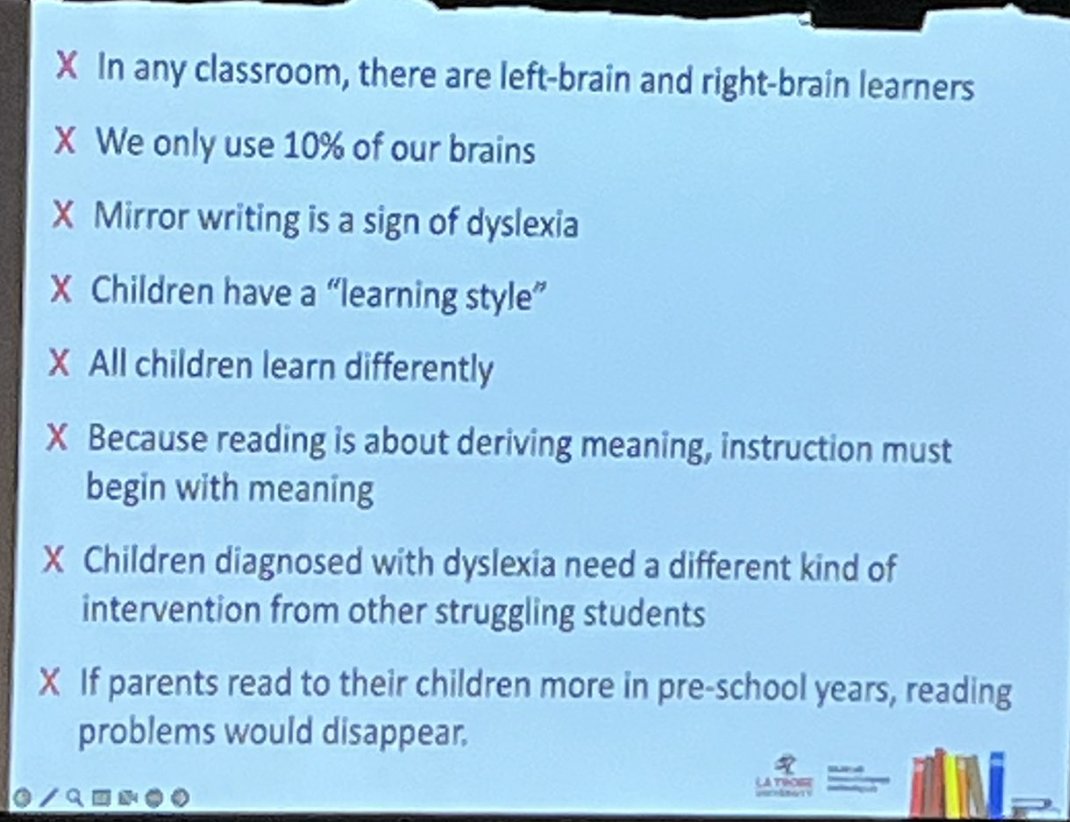
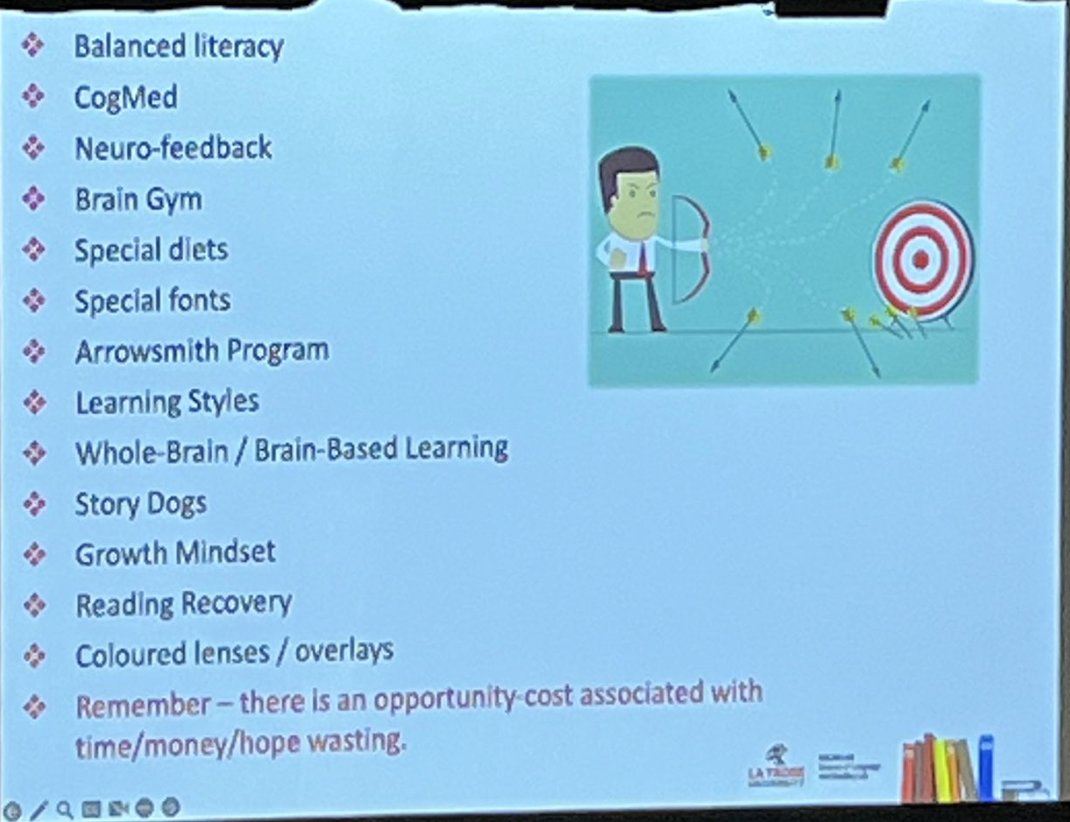
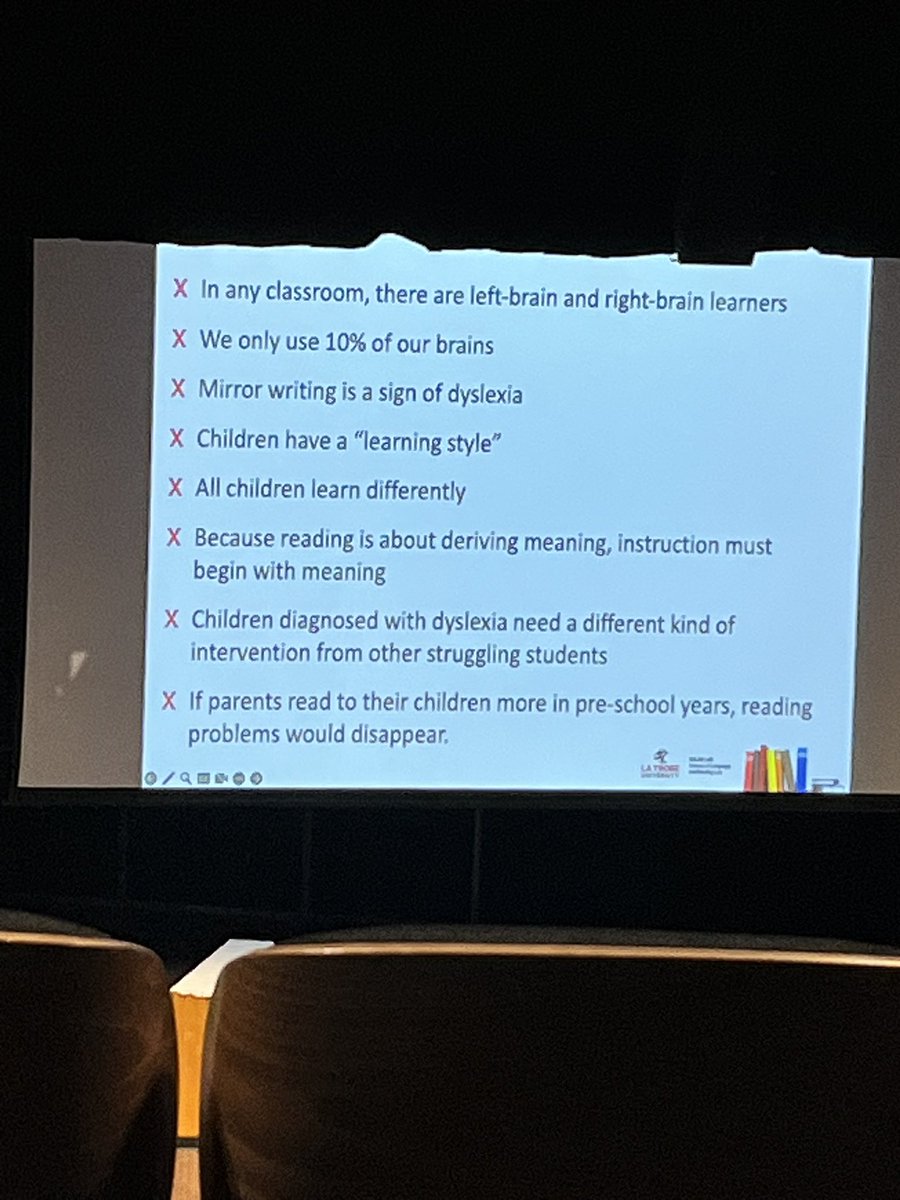
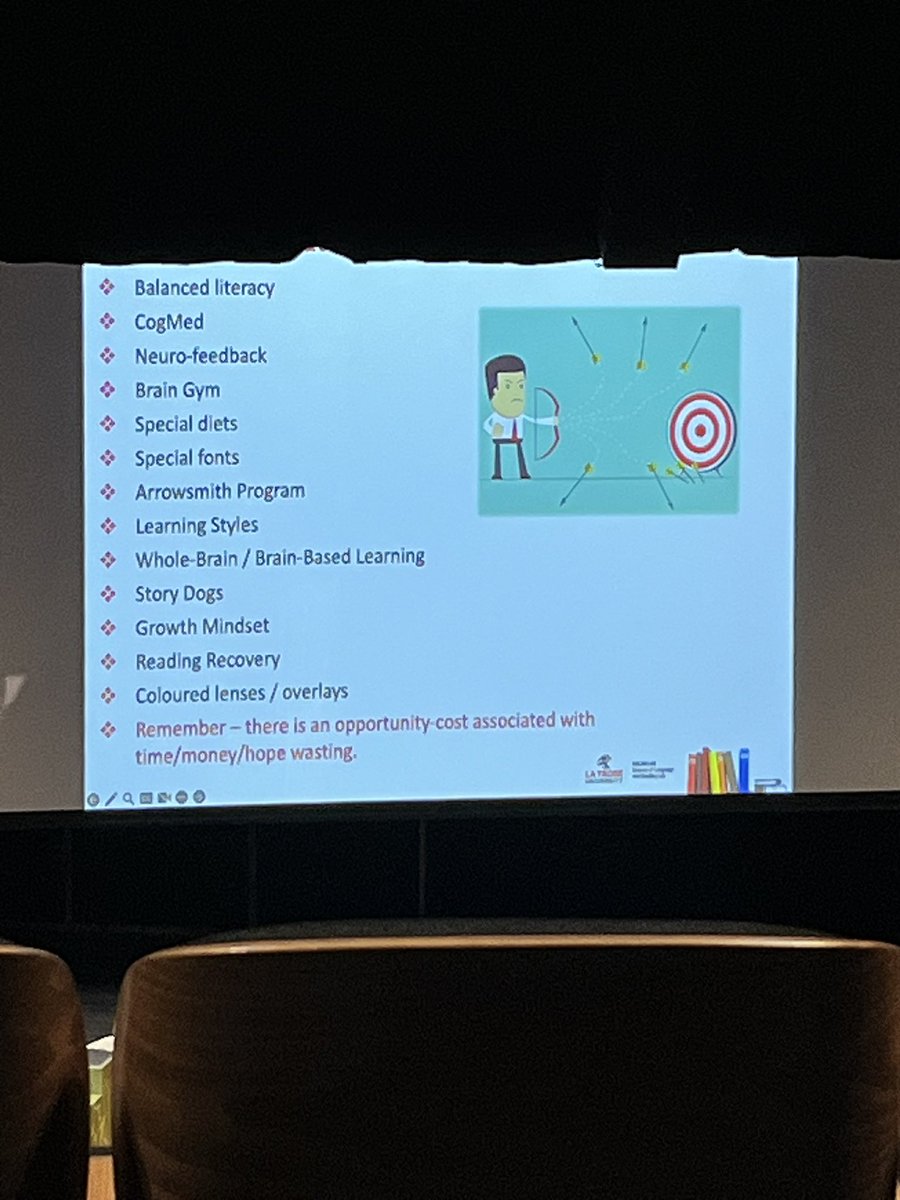
Educational myths.
True educational reform can't happen unless deimplementation is front and center.
1 Nov 2025

If only ALL teacher trainees were introduced to these myths in their ITT. @PamelaSnow2 @latrobe @researchED_Aus
1
8
1,680

28 Oct 2025
Teaching literacy has changed, and that can feel overwhelming. But you don’t have to navigate it alone. The Deimplementation for Literacy Growth series is designed to help you let go of practices that no longer serve your students and embrace evidence-based approaches that do.
1
4
622

27 Oct 2025
One key focus of the Southern Surge states was to retrain their teachers. Oklahoma dedicated $13 million of ARP funds to retrain 10,000 teachers with LETRS, yet the worksheets coming home, spelling inventories, and rampant sight word demands show implementation is still missing the mark.
I’m curious if the concept of Deimplementation plays a role in the effectiveness of different training initiatives.
#oklaed #SouthernSurge #SoR
2
4
15
10,285
23 Oct 2025
1 week, until the first session in a 3-part Deimplementation for Literacy Growth series with @MmeLockhartLDS, an opportunity to rethink what we keep, what we let go, and how we grow.
Empower your staff. Strengthen literacy learning. eventbrite.ca/e/146544118703… #literacy #learning

1
2
229

18 Oct 2025
Would start with a deimplementation trial in ESRD. The time zero of OAC often precedes development of ESRD.
1
4
1,607

16 Oct 2025
📢 Our new editorial exposes a silent epidemic: Overdiagnosis & Overtreatment ⚠️
👉 journals.sagepub.com/doi/10.…
In LMICs, it’s not just clinical harm—it’s the squandering of scarce resources that could have saved lives
Curbing waste is a moral imperative because every unnecessary test or surgery doesn’t just waste money—it steals care from someone who truly needs it
#GlobalHealth #ChoosingWisely # Deimplementation

1
3
4
192
8 Oct 2025
Gearing up for a great MPact experience with @MmeLockhartLDS leading this 3-part learning on Deimplementation for Literacy Growth. Read about how each session addresses 2 aspects of your literacy program to deimplement, and adds 2 evidence-based practices: bit.ly/MentoreeEventbrite
2
2
834

6 Oct 2025
In this quality improvement study, a multifaceted deimplementation strategy to reduce unnecessary preoperative testing before common, low-risk surgical procedures was feasible to implement. ja.ma/4pOzTfw
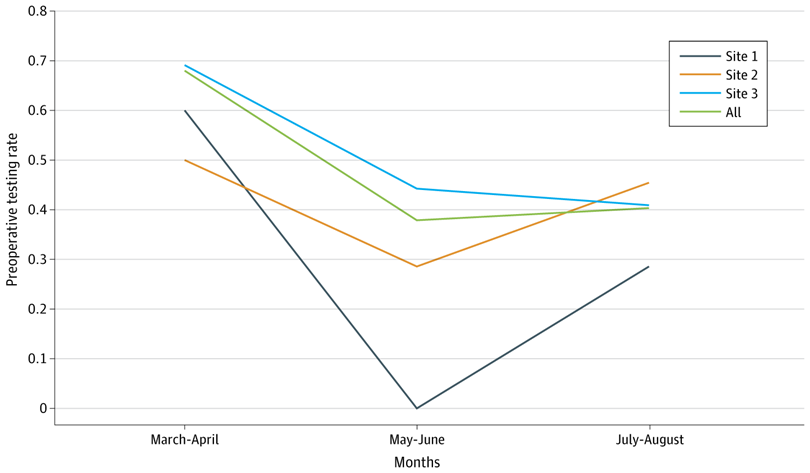
ALT Line graph showing preoperative testing rates for Sites 1, 2, and 3, and overall, over time. The X axis displays months (March-April, May-June, July-August), and the Y axis shows rate (0-0.8). Site 1 drops in May-June but increases in July-August.
1
2
753
24 Sep 2025
Really excited for @MmeLockhartLDS’s session tonight from
7-8pm EST on Deimplementation for Literacy Growth. Learn more and register: bit.ly/MentoreeEventbrite. #literacy #evidencebased #research #bestpractices #OntEd #Edu
2
7
1,229
15 Sep 2025
@MmeLockhartLDS is leading a Motivators event on Deimplementation for Literacy Growth on Sept. 24th. Sometimes you have to pare down to level up. Learn more and register at bit.ly/MentoreeEventbrite.
#Literacy #mentormonday #deimplementation #OntEd #edu #teachersupport #mentoring
1
3
5
4,515