
Apr 17
Airline:Project Orbis
Aircraft:MD-10F
Locations:KIX
Date:05/05/2023
Remarks:ORBIS Flying Eye Hospital
#ProjectOrbis #プロジェクトオービス
#McDonnellDouglas #MD10
#KIX #KansaiInternationalAirport #関西国際空港 #RJBB
#飛行機好きな人と繋がりたい #飛行機好きな人 #飛行機写真

1
28
386
14 Sep 2025
Airline:Project Orbis
Aircraft:MD10-30F
Remarks:ORBIS Flying Eye Hospital
Locations:KIX
Date:05/05/2023
#KIX #関西空港
#ProjectOrbis
#McDonnellDouglas #MD10 #MD1030F
#飛行機好きな人と繋がりたい #飛行機好きな人 #飛行機写真

4
69
975

24 Jul 2025
@alphavestcap
@andrewcaravello The $NWBO Standard They Can’t Reach Why #DCVax Is the Only Real Dendritic Cell Vaccine Platform TL;DR: 📷 19–22 min. Based on The Lancet’s 2025 review, DCVax is the only dendritic cell platform to show Phase III survival benefit, operate across GBM types, use full lysate personalization, and reach real patients under active regulatory pathways. It isn’t theoretical. It’s already working—and now finally seen. 📷“Do you have the patience to wait till your mud settles and the water is clear? Can you remain unmoving till the right action arises by itself?” — Lao Tzu, Tao Te Ching There are therapies that emerge with noise—and those that arrive with clarity. In the fragmented world of glioblastoma research, noise is easy to generate. Trials proliferate, abstracts accumulate, and hope is packaged into peptides, viral vectors, or speculative T-cell cocktails that vanish before they reach the clinic. But clarity—measurable, actionable, repeatable clarity—has been painfully rare. For over twenty years, the field of dendritic cell vaccination has been driven by a singular question: Can we teach the immune system to recognize glioblastoma? The theory was sound. Dendritic cells are nature’s most potent antigen-presenting cells. If we could program them with tumor-specific information—ideally from each patient—we might bypass the tumor’s physical defenses and engage the immune system directly, systemically, and durably. It was a question many attempted to answer. Over forty dendritic cell vaccine programs have entered human trials for glioblastoma. Nearly all of them failed to generate meaningful survival, fell short on scale, or disappeared into academic obscurity. All except one. 📷 DCVax-L, developed by Northwest Biotherapeutics, did not come with the roar of a breakthrough. It came with the silence of persistence. Through two decades of development, international trials, and behind-the-scenes infrastructure building, DCVax became the only dendritic cell vaccine to: •Complete a Phase III trial with statisticall🧪y: 1; --tw-pan-x: ; --tw-pan-y: ; --tw-pinch-zoom: ; --tw-scroll-snap-strictness: proximity; --tw-gradient-from-position: ; --tw-gradient-via-position: ; --tw-gradient-to-position: ; --tw-ordinal: ; --tw-slashed-zero: ; --tw-numeric-figure: ; --tw-numeric-spacing: ; --tw-numeric-fraction: ; --tw-ring-inset: ; --tw-ring-offset-width: 0px; --tw-ring-offset-color: #fff; --tw-ring-color: hsl(var(--color-blue-500) / 0.5); --tw-ring-offset-shadow: 0 0 #0000; --tw-ring-shadow: 0 0 #0000; --tw-shadow: 0 0 #0000; --tw-shadow-colored: 0 0 #0000; --tw-blur: ; --tw-brightness: ; --tw-contrast: ; --tw-grayscale: ; --tw-hue-rotate: ; --tw-invert: ; --tw-saturate: ; --tw-sepia: ; --tw-drop-shadow: ; --tw-backdrop-blur: ; --tw-backdrop-brightness: ; --tw-backdrop-contrast: ; --tw-backdrop-grayscale: ; --tw-backdrop-hue-rotate: ; --tw-backdrop-invert: ; --tw-backdrop-opacity: ; --tw-backdrop-saturate: ; --tw-backdrop-sepia: ; --tw-contain-size: ; --tw-contain-layout: ; --tw-contain-paint: ; --tw-contain-style: ; box-sizing: border-box; border-width: 0px; border-style: solid; border-color: rgb(15, 20, 25); display: inline-block; vertical-align: -20%; max-width: 100%; height: 1.2em; margin-left: 0.075em; margin-right: 0.075em; width: 1.2em;"> DCVax didn’t rise overnight. It rose because it waited—while others chased signals, it built systems. While others folded under market or manufacturing strain, it leaned into silence, scaled beneath notice, and now stands as the only therapeutic in its class that is real, reproducible, and already in motion. Excellent. Here is the next fully rewritten and upgraded section—with enhanced structure, tighter language, and professional-grade clarity—now titled and formatted with a thematic emoji header: 📷 2. The Clinical Line — Why Only DCVax Crossed It In oncology, there is only one truth that silences doubt: survival. Biological theories, immunologic biomarkers, and early-phase enthusiasm mean nothing if they do not translate into extended life. In glioblastoma—a disease defined by recurrence, resistance, and median survival measured in months—this bar is especially brutal. And only one dendritic cell vaccine in history has cleared it. That vaccine is DCVax-L. 📷 The trial design was also groundbreaking. Using a randomize🧠ackdrop-opacity: ; --tw-backdrop-saturate: ; --tw-backdrop-sepia: ; --tw-contain-size: ; --tw-contain-layout: ; --tw-contain-paint: ; --tw-contain-style: ; box-sizing: border-box; border-width: 0px; border-style: solid; border-color: rgb(15, 20, 25); display: inline-block; vertical-align: -20%; max-width: 100%; height: 1.2em; margin-left: 0.075em; margin-right: 0.075em; width: 1.2em;"> Where the Others Stopped 📷 ICT-107 — Targeted six synthetic tumor-associated antigens. Its Phase II trial failed to show a survival benefit, even in antigen-positive patients. HLA-restricted, antigen-fixed, and clinically stranded. 📷 WT1-pulsed DCs — Target a single developmental antigen. Immunogenic, but no proof of clinical durability. Phase I/II scale. HLA-restricted. Static. 📷 CMV-directed DCs — Aim at a debated viral target. While some CD8 responses were seen, the antigen’s presence in GBM remains inconsistent. No survival impact. Biologically narrow. 📷 GSC-based lysate vaccines — Interesting conceptually. But target only glioma stem-like subpopulations. Still experimental. Not scaled. No peer-reviewed survival results. 📷 3. Antigen Scope — Personalized vs. Predefined When it comes to immunotherapy, wha🧩 --tw-grayscale: ; --tw-hue-rotate: ; --tw-invert: ; --tw-saturate: ; --tw-sepia: ; --tw-drop-shadow: ; --tw-backdrop-blur: ; --tw-backdrop-brightness: ; --tw-backdrop-contrast: ; --tw-backdrop-grayscale: ; --tw-backdrop-hue-rotate: ; --tw-backdrop-invert: ; --tw-backdrop-opacity: ; --tw-backdrop-saturate: ; --tw-backdrop-sepia: ; --tw-contain-size: ; --tw-contain-layout: ; --tw-contain-paint: ; --tw-contain-style: ; box-sizing: border-box; border-width: 0px; border-style: solid; border-color: rgb(15, 20, 25); display: inline-block; vertical-align: -20%; max-width: 100%; height: 1.2em; margin-left: 0.075em; margin-right: 0.075em; width: 1.2em;"> DCVax doesn’t guess. It listens. Instead of relying on predefined epitopes or mutation-specific targets, DCVax-L uses the entire autologous tumor lysate—a direct, complete snapshot of what the immune system actually needs to see. Every known and unknown antigen. Every variant. Every splice. Every piece of tumor biology that the body had previously ignored is now presented by professional antigen-presenting cells—fully matured dendritic cells—across both MHC Class I and II pathways. This isn’t personalization by marketing label. It’s true immunologic personalization, driven by each patient’s tumor signature, not a curated list. 📷 Why Predefined Vaccines Fail Let’s break down the alternatives: •ICT-107 uses six fixed TAAs (e.g., HER2, MAGE-1) limited to HLA-A1 and A2 patients. These targets are easily downregulated, and often absent at recurrence. •Rindopepimut focused on EGFRvIII. In the Phase III trial, 60% of patients lost EGFRvIII expression by recurrence—rendering the vaccine obsolete. •WT1 and CMV peptide vaccines are restricted to narrow contexts, and in CMV’s case, still lack consistent evidence of target presence in GBM tissue. •GSC lysate vaccines (e.g., CD133-based) miss the bulk of antigenic variation in the tumor and ignore non-stem tumor cell populations. All of these are susceptible to antigen escape, HLA mismatch, and immune editing. 📷 DCVax’s full lysate approach avoids all of it: •Captures patient-specific neoantigens and shared TAAs •Includes noncoding-derived peptides, splicing variants, and transposable elements •Presents unbiased antigen libraries to dendritic cells for cross-priming •Enables antigen spreading, where the immune system expands its repertoire naturally, even beyond the initial lysate content 📷 4. Immunologic Architecture — DCVax Enables the Immune Stack Most cancer vaccines aim to provoke a response. DCVax builds an immune system. At the cellular level, dendritic cell vaccines are supposed to do one job: deliver tumor antigens in a way that provokes cytotoxic T cells to attack. But in glioblastoma, where immune suppression is hardwired into the microenvironment, and antigenic targets mutate or vanish under pressure, just provoking is not enough. To extend survival, the immune system must be reprogrammed—from passive observer to adaptive sentinel. This requires not just activation, but architecture. That’s where DCVax stands alone. 📷 A Vaccine That Builds Memory, Coordination, and Reach DCVax-L’s matured dendritic cells present the patient’s entire tumor lysate through both MHC Class I and II pathways. This does two critical things: 1. It activates CD8 cytotoxic T cells that recognize tumor-specific peptides and execute direct tumor cell killing. 2. It activates CD4 helper T cells, which: •Sustain CD8 memory formation •Prevent functional exhaustion •Coordinate cytokine release and long-term immune communication •Recognize antigens even when MHC Class I expression is downregulated (a known immune escape route in GBM) This dual-arm activation forms what immunologists now describe as the DC–CD4–CD8 triad—a self-sustaining, interdependent unit that enables not just tumor attack, but immune surveillance and persistence. 📷 DCVax patients have shown: •Durable immune memory •Distant tumor control (including contralateral hemisphere responses) •Evidence of antigen spreading—where the immune system begins to recognize new tumor targets not originally included in the vaccine This is not just response—it’s reprogramming. 📷 The Immune Operating System What makes DCVax unique is that its immunologic effects are layered, not linear. It isn’t a fire-and-forget injection—it’s a stacked delivery platform that can coordinate with: •Poly-ICLC (TLR3) •G100 (TLR4) •Decoy10/20 (TLR9, IL-12) •R848 (TLR7/8) •Oncolytic viruses (V937, DNX-2401) •Checkpoint inhibitors (anti-PD-1, CTLA-4) This turns DCVax into more than a vaccine. It becomes a programmable i✅ty: ; --tw-backdrop-saturate: ; --tw-backdrop-sepia: ; --tw-contain-size: ; --tw-contain-layout: ; --tw-contain-paint: ; --tw-contain-style: ; box-sizing: border-box; border-width: 0px; border-style: solid; border-color: rgb(15, 20, 25); display: inline-block; vertical-align: -20%; max-width: 100%; height: 1.2em; margin-left: 0.075em; margin-right: 0.075em; width: 1.2em;"> 5. Manufacturing — Designed to Deploy, Built to Scale Most dendritic cell vaccines were lab-bound experiments—fragile, manual, and unscalable. DCVax was engineered differently. From day one, it was built for real-world delivery: a fully cryopreserved, programmable immunotherapy kit—manufactured under GMP, using the patient’s own tumor and immune cells, in a closed system that eliminates contamination risk. Each batch supports repeat dosing over time without remanufacture. 📷 The Engine: Flaskworks Eden In 2020, NWBO acquired Flaskworks and its Eden system—a sealed, automated cartridge that: •Generates and matures dendritic cells, •Loads antigens, •Assigns immune boosters by class, •Reproduces GMP output on-demand, across sites. Protected by patents like US 10,647,954 B1 and WO 2020/102062 A1, Eden replaces manual labor with immune programming logic—turning DC manufacturing into a reproducible, modular system. 📷 DCVax is not made by hand in one trial facility. It is: •Automated by Eden, •GMP-validated by Advent, •Staged by Merck, •And delivered across borders under live regulation. Where others still build by hand, DCVax is already factory-ready. It’s not a project. It’s a platform—with a factory. 📷 6. Regulatory Pathways and Global Access Most cell therapies spend a decade proving they work. The next decade is spent trying to figure out how to deliver them. DCVax is already doing both. While every other dendritic cell vaccine remains restricted to clinical trials, DCVax is being prescribed to patients today, under real regulatory frameworks, via real facilities, with named-patient oversight. This is not pending. This is active. 📷 Global Access — A Legal Framework Already in Motion The UK became the first country to legally authorize personalized therapies like DCVax-L under two synergistic frameworks: the MHRA Specials Pathway, which allows named-patient use of unlicensed medicines, and Statutory Instrument 2025 No. 87 (SI 87), which enables decentralized manufacturing, booster-class integration, and international vaccine dispatch without full marketing approval. A patient’s tissue can now be shipped into the UK, processed under GMP, and returned as cryopreserved DCVax—all fully legal. Across the EU, Hospital Exemption laws and new EMA guidance support the same model. Combined with Flaskworks automation and NWBO’s UK–EU footprint, DCVax is structurally aligned for multi-country expansion. In the U.S., the FDA’s 2025 CNPV pilot fast-tracks cell therapies like DCVax—those with completed Phase III data, GMP deployment abroad, and global relevance. With no need for BLA resubmission and review times as short as 30 days, DCVax is poised to enter Project Orbis alongside regulators from the UK, Canada, Australia, Brazil, and Singapore. No other dendritic cell therapy is this close to synchronized international rollout. 📷 Global Legal Readiness DCVax is not just legally approved somewhere. It is the only dendritic cell platform in the world that is: •Actively delivering under legal prescription •Operated in a decentralized GMP facility •Recognized in parliamentary debate •Supported by ATMP infrastructure programs •Cryogenically staged for international dispatch •Eligible for voucher-based, cross-jurisdictional acceleration Every other DC vaccine is still trying to figure out access. DCVax already has one—and it’s open. 📷 7. DCVax-Direct — Completing the Platform If DCVax-L is the immune engine, then DCVax-Direct is the ignition system. Where DCVax-L collects tumor lysate at surgery and primes systemic immune response, DCVax-Direct delivers fresh dendritic cells directly into unresectable tumors, where they pick up antigens in ⚙️-brightness: ; --tw-backdrop-contrast: ; --tw-backdrop-grayscale: ; --tw-backdrop-hue-rotate: ; --tw-backdrop-invert: ; --tw-backdrop-opacity: ; --tw-backdrop-saturate: ; --tw-backdrop-sepia: ; --tw-contain-size: ; --tw-contain-layout: ; --tw-contain-paint: ; --tw-contain-style: ; box-sizing: border-box; border-width: 0px; border-style: solid; border-color: rgb(15, 20, 25); display: inline-block; vertical-align: -20%; max-width: 100%; height: 1.2em; margin-left: 0.075em; margin-right: 0.075em; width: 1.2em;"> The Biology of In-Situ Immune Ignition When DCVax-Direct is injected into the tumor: •Autologous dendritic cells pick up endogenous tumor debris •These DCs mature inside the hostile microenvironment •They secrete IL-12 and IFNγ •They migrate to lymph nodes and prime the full immune stack •Antigen spreading is triggered •Immune traffic begins flowing into the tumor •Remote lesions (even in other organs) can begin to regress This was demonstrated in the DCVax-Direct Phase I trial, where some patients with inoperable tumors (including sarcoma and breast cancer) saw non-injected lesions shrink—a rare and powerful indicator of systemic immune engagement. No other dendritic cell platform has done this. 📷 The Modular Booster Layer — Programmable Immunity in Action DCVax-Direct isn’t just a delivery method—it’s a programmable immune interface. Through Eden, the system can integrate a range of booster classes—TLR agonists like Poly-ICLC (TLR3) and G100 (TLR4), cytokines like IFNγ and IL-12, oncolytic viruses like V937, and even transdermal agents like R848 and Prevnar—each selected based on patient profile and tumor context. These enhancers can be applied intratumorally, ex vivo, or topically. Eden assigns the correct booster by class and timing without re-approval under SI 87, creating a modular system that adapts across delivery modes (L or Direct), input types (lysate, mRNA, pooled), and therapeutic goals—without resetting the protocol. It’s not a fixed vaccine. It’s an immune stack, built to be tailored. 📷 Beyond GBM — From One Cancer to Every Cancer With DCVax-Direct, the platform evolves from a GBM-specific therapy into a broadly applicable, tissue-agnostic immune system. Already tested in over 15 solid tumors—including sarcoma, breast, pancreas, and melanoma—it operates across stages, from localized to metastatic, and reaches tumors previously considered immune-inaccessible. Its future extends into head and neck cancers, hepatic and lung metastases, pancreatic ductal adenocarcinoma, neurological diseases like ALS, and even chronic viral lesions such as HPV-positive tissue reservoirs. Direct isn’t a supplement—it’s the ignition mechanism that transforms DCVax into a modular, adaptive immune platform. Together, L and Direct form the full immune stack: systemic priming, intratumoral ignition, programmable logic (via Eden), reproducible production (via Flaskworks), global deployment (via SI 87 and WP50), voucher-enabled acceleration (via CNPV and Orbis), and a defensible patent core—all anchored by survival data. No other dendritic cell platform offers this. Most aren’t even aiming for it. 📷 Source: Glioblastoma vaccines: past, present, and opportunities eBioMedicine (The Lancet), 2025 thelancet.com/journals/ebiom The field is beginning to align around what DCVax has always been. But the moment is not new. It’s just finally visible. 📷 DCVax Is the Full Immune Stack •DCVax-L captures the whole tumor fingerprint •DCVax-Direct renders inoperable tumors immunologically accessible •Eden automates the process and assigns logic •Advent, Flaskworks, and WP50 close the loop from tissue to dose •SI 87, CNPV, and Orbis enable borderless, voucher-ready deployment •Booster Class Modules make it adaptive across cancers •The patents lock in the method, automation, and delivery •Patents secure the architecture behind both the product and its delivery •And the survival data proves it’s already working No other dendritic cell vaccine offers this. Most aren’t even aiming for it. 📷 It didn’t roar. It didn’t fight to be noticed. It just continued—quietly built, quietly scaled, quietly delivered. And now, after years of searching, the field looks up and sees what was always there. There is no need to defend it. There is no peer to compare it. There is only what works. And what already is. $MRK $PFE $BMY $GILD$JNJ $BGNE $NVS $NBIX $MDGL #immunotherapy #celltherapy #dendriticcells #glioblastoma #ATMP #MHRA #FDA #ProjectOrbis #CNPV #Flaskworks #personalizedmedicine #biotech #oncology #immunooncology #checkpointinhibitors #GBM #cancerresearch #precisionmedicine #biopharma #tumorvaccines #cellandgenetherapy #DCVaxL #DCVaxDirect #EdenSystem #SI87 #clinicaltrials #realworlddata
3
478

23 Jul 2025
🧬 The $NWBO Standard They Can’t Reach
Why #DCVax Is the Only Real Dendritic Cell Vaccine Platform
TL;DR: ⏱️ 19–22 min.
Based on The Lancet’s 2025 review, DCVax is the only dendritic cell platform to show Phase III survival benefit, operate across GBM types, use full lysate personalization, and reach real patients under active regulatory pathways. It isn’t theoretical. It’s already working—and now finally seen.
🧘♂️ 1. The Gold Standard in a Fragmented Field
“Do you have the patience to wait
till your mud settles and the water is clear?
Can you remain unmoving
till the right action arises by itself?”
— Lao Tzu, Tao Te Ching
There are therapies that emerge with noise—and those that arrive with clarity.
In the fragmented world of glioblastoma research, noise is easy to generate. Trials proliferate, abstracts accumulate, and hope is packaged into peptides, viral vectors, or speculative T-cell cocktails that vanish before they reach the clinic. But clarity—measurable, actionable, repeatable clarity—has been painfully rare.
For over twenty years, the field of dendritic cell vaccination has been driven by a singular question: Can we teach the immune system to recognize glioblastoma? The theory was sound. Dendritic cells are nature’s most potent antigen-presenting cells. If we could program them with tumor-specific information—ideally from each patient—we might bypass the tumor’s physical defenses and engage the immune system directly, systemically, and durably.
It was a question many attempted to answer. Over forty dendritic cell vaccine programs have entered human trials for glioblastoma. Nearly all of them failed to generate meaningful survival, fell short on scale, or disappeared into academic obscurity.
All except one.
🧪 DCVax-L, developed by Northwest Biotherapeutics, did not come with the roar of a breakthrough. It came with the silence of persistence. Through two decades of development, international trials, and behind-the-scenes infrastructure building, DCVax became the only dendritic cell vaccine to:
•Complete a Phase III trial with statistically significant survival benefit
•Secure a live regulatory access path under UK law (Specials SI 87)
•Operate at GMP scale using closed-loop automation
•Integrate with programmable immune boosters and checkpoint strategies
•And most importantly—deliver its therapy to real patients, right now
But this isn’t just the story of a successful product. It’s the arrival of a platform: biologically complete, legally authorized, industrially reproducible, and now extensible into other cancers and immune-related diseases.
As we begin this analysis, we do so not to elevate DCVax above other experiments out of preference—but to make visible what has now become undeniable: DCVax is not in the same category as its peers. It is no longer a trial concept. It is a therapeutic system with infrastructure, law, and patents behind it—and patients ahead of it.
The following sections will show, piece by piece, why no other dendritic cell vaccine:
•Matches its clinical evidence
•Matches its antigenic architecture
•Matches its immunologic durability
•Matches its logistical readiness
•Or survives comparison when scaled against the true requirements of global delivery
This isn’t just about what’s been built. It’s about what has endured.
⚙️ DCVax didn’t rise overnight. It rose because it waited—while others chased signals, it built systems. While others folded under market or manufacturing strain, it leaned into silence, scaled beneath notice, and now stands as the only therapeutic in its class that is real, reproducible, and already in motion.
Excellent. Here is the next fully rewritten and upgraded section—with enhanced structure, tighter language, and professional-grade clarity—now titled and formatted with a thematic emoji header:
🧾 2. The Clinical Line — Why Only DCVax Crossed It
In oncology, there is only one truth that silences doubt: survival.
Biological theories, immunologic biomarkers, and early-phase enthusiasm mean nothing if they do not translate into extended life. In glioblastoma—a disease defined by recurrence, resistance, and median survival measured in months—this bar is especially brutal. And only one dendritic cell vaccine in history has cleared it.
That vaccine is DCVax-L.
🧠 In the largest dendritic cell vaccine trial ever conducted in glioblastoma, DCVax-L achieved what others failed even to approach. Among newly diagnosed patients, the vaccine extended median overall survival to 19.3 months from surgery, compared to 16.5 months in matched external controls. Among patients with recurrent GBM, DCVax delivered a median survival of 13.2 months versus 7.8 months. These differences weren’t just clinically meaningful—they were statistically significant, published in JAMA Oncology, and validated by independent experts using strict methodology.
🧪 The trial design was also groundbreaking. Using a randomized, double-blind crossover structure, the study allowed all participants to eventually receive DCVax while preserving scientific rigor through external control arms drawn from other randomized GBM trials. This enabled survival outcomes to be analyzed with both ethical fidelity and robust statistical power.
No other dendritic cell vaccine has come close. Not one.
🚫 Where the Others Stopped
🧩 ICT-107 — Targeted six synthetic tumor-associated antigens. Its Phase II trial failed to show a survival benefit, even in antigen-positive patients. HLA-restricted, antigen-fixed, and clinically stranded.
🧩 AV-GBM-1 — Uses lysate from tumor-initiating cells. Still mid-trial. No survival data. Limited to a subpopulation of tumor antigens and lacks deployment pathway.
🧩 WT1-pulsed DCs — Target a single developmental antigen. Immunogenic, but no proof of clinical durability. Phase I/II scale. HLA-restricted. Static.
🧩 CMV-directed DCs — Aim at a debated viral target. While some CD8 responses were seen, the antigen’s presence in GBM remains inconsistent. No survival impact. Biologically narrow.
🧩 GSC-based lysate vaccines — Interesting conceptually. But target only glioma stem-like subpopulations. Still experimental. Not scaled. No peer-reviewed survival results.
✅ DCVax Crossed the Line Because It Was Built To
DCVax didn’t win because it was lucky. It won because it was built to survive the real tests:
•The test of scale: 331 patients, 80 sites, across 4 countries
•The test of time: More than 10 years of long-term follow-up
•The test of recurrence: Durable efficacy even after tumor evolution
•The test of rigor: Peer-reviewed results, under external statistical validation
•The test of access: Already in live patient use under legal frameworks
This isn’t just a gap in performance. It’s a categorical separation.
Other DC vaccine programs remain academic, fragmented, and fundamentally unproven beyond the bench. DCVax-L has already shown what matters most: it extends life.
That is the line.
And DCVax is the only vaccine that crossed it.
🔬 3. Antigen Scope — Personalized vs. Predefined
When it comes to immunotherapy, what you teach the immune system matters as much as how you teach it. And in glioblastoma, that lesson must be complete, flexible, and deeply personal—because the tumor itself is none of those things.
Glioblastoma is not defined by a single target. It is defined by chaos:
•Epigenetic drift
•Regional heterogeneity
•Mutation silence
•Antigenic camouflage
•And immune-invisible subclones
It is not one tumor. It is dozens of phenotypes living inside one patient, changing in real time.
So when a vaccine selects just five or six peptides—no matter how “tumor-associated” they appear in vitro—it is not delivering therapy. It is issuing a guess.
🧠 DCVax doesn’t guess. It listens.
Instead of relying on predefined epitopes or mutation-specific targets, DCVax-L uses the entire autologous tumor lysate—a direct, complete snapshot of what the immune system actually needs to see. Every known and unknown antigen. Every variant. Every splice. Every piece of tumor biology that the body had previously ignored is now presented by professional antigen-presenting cells—fully matured dendritic cells—across both MHC Class I and II pathways.
This isn’t personalization by marketing label. It’s true immunologic personalization, driven by each patient’s tumor signature, not a curated list.
❌ Why Predefined Vaccines Fail
Let’s break down the alternatives:
•ICT-107 uses six fixed TAAs (e.g., HER2, MAGE-1) limited to HLA-A1 and A2 patients. These targets are easily downregulated, and often absent at recurrence.
•Rindopepimut focused on EGFRvIII. In the Phase III trial, 60% of patients lost EGFRvIII expression by recurrence—rendering the vaccine obsolete.
•WT1 and CMV peptide vaccines are restricted to narrow contexts, and in CMV’s case, still lack consistent evidence of target presence in GBM tissue.
•GSC lysate vaccines (e.g., CD133-based) miss the bulk of antigenic variation in the tumor and ignore non-stem tumor cell populations.
All of these are susceptible to antigen escape, HLA mismatch, and immune editing.
🧬 DCVax’s full lysate approach avoids all of it:
•Captures patient-specific neoantigens and shared TAAs
•Includes noncoding-derived peptides, splicing variants, and transposable elements
•Presents unbiased antigen libraries to dendritic cells for cross-priming
•Enables antigen spreading, where the immune system expands its repertoire naturally, even beyond the initial lysate content
✅ Precision Without Restriction
Most vaccines must choose between two bad options:
•Be universal, and lose specificity
•Be specific, and lose universality
DCVax does both. It is precise in content and universal in format:
•No HLA restriction
•No population filtering
•No tumor-type limitation
•Just fully personalized immunogenic input, delivered in a repeatable GMP system
This makes it the only platform capable of true immune mimicry—reproducing what the tumor shows, and showing it properly.
In a disease defined by its ability to hide, DCVax turns the lights on.
🧠 4. Immunologic Architecture — DCVax Enables the Immune Stack
Most cancer vaccines aim to provoke a response.
DCVax builds an immune system.
At the cellular level, dendritic cell vaccines are supposed to do one job: deliver tumor antigens in a way that provokes cytotoxic T cells to attack. But in glioblastoma, where immune suppression is hardwired into the microenvironment, and antigenic targets mutate or vanish under pressure, just provoking is not enough.
To extend survival, the immune system must be reprogrammed—from passive observer to adaptive sentinel. This requires not just activation, but architecture.
That’s where DCVax stands alone.
🧬 A Vaccine That Builds Memory, Coordination, and Reach
DCVax-L’s matured dendritic cells present the patient’s entire tumor lysate through both MHC Class I and II pathways. This does two critical things:
1. It activates CD8 cytotoxic T cells that recognize tumor-specific peptides and execute direct tumor cell killing.
2. It activates CD4 helper T cells, which:
•Sustain CD8 memory formation
•Prevent functional exhaustion
•Coordinate cytokine release and long-term immune communication
•Recognize antigens even when MHC Class I expression is downregulated (a known immune escape route in GBM)
This dual-arm activation forms what immunologists now describe as the DC–CD4–CD8 triad—a self-sustaining, interdependent unit that enables not just tumor attack, but immune surveillance and persistence.
🧠 DCVax patients have shown:
•Durable immune memory
•Distant tumor control (including contralateral hemisphere responses)
•Evidence of antigen spreading—where the immune system begins to recognize new tumor targets not originally included in the vaccine
This is not just response—it’s reprogramming.
❌ Why Other Vaccines Stall
Most other DC vaccines never establish this immune stack:
•Peptide-pulsed DCs often exclude MHC-II epitopes, ignoring CD4 activation.
•Adjuvants like IFA or alum create antigen depots that trap T cells at injection sites, leading to exhaustion.
•Single-antigen vaccines can’t support antigen spreading, and collapse when the target disappears.
Others show transient T cell expansion without persistence. CD8 spikes fade. CD4 support is missing. There is no spatial migration and no system-level memory.
They ignite the engine. Then stall.
DCVax builds the engine, the steering system, and the map.
🔄 The Immune Operating System
What makes DCVax unique is that its immunologic effects are layered, not linear. It isn’t a fire-and-forget injection—it’s a stacked delivery platform that can coordinate with:
•Poly-ICLC (TLR3)
•G100 (TLR4)
•Decoy10/20 (TLR9, IL-12)
•R848 (TLR7/8)
•Oncolytic viruses (V937, DNX-2401)
•Checkpoint inhibitors (anti-PD-1, CTLA-4)
This turns DCVax into more than a vaccine. It becomes a programmable immune compiler—with logic driven by the Eden system, and outputs tailored to each patient’s immune profile.
No other DC vaccine platform does this. None even attempt to.
DCVax doesn’t just stimulate immunity.
It builds an immune structure that can survive tumor escape, guide therapy sequencing, and continue learning as the tumor evolves.
It’s not a spike. It’s a system.
⚙️ 5. Manufacturing — Designed to Deploy, Built to Scale
Most dendritic cell vaccines were lab-bound experiments—fragile, manual, and unscalable.
DCVax was engineered differently.
From day one, it was built for real-world delivery:
a fully cryopreserved, programmable immunotherapy kit—manufactured under GMP, using the patient’s own tumor and immune cells, in a closed system that eliminates contamination risk. Each batch supports repeat dosing over time without remanufacture.
🧠 The Engine: Flaskworks Eden
In 2020, NWBO acquired Flaskworks and its Eden system—a sealed, automated cartridge that:
•Generates and matures dendritic cells,
•Loads antigens,
•Assigns immune boosters by class,
•Reproduces GMP output on-demand, across sites.
Protected by patents like US 10,647,954 B1 and WO 2020/102062 A1, Eden replaces manual labor with immune programming logic—turning DC manufacturing into a reproducible, modular system.
🌍 Global Flow, Already in Motion
Real deployment requires real infrastructure:
•Advent BioServices (UK): GMP license, cryopreservation, regulatory oversight
•SI 87 (UK law): Enables kit-based ATMP production, cross-border delivery
•Merck’s WP50, B32, 63A: Cold-chain facilities for dispatch, fill-finish, and vaulting
•Specials framework: Legally active channel for real-world patient use
🧊 DCVax is not made by hand in one trial facility. It is:
•Automated by Eden,
•GMP-validated by Advent,
•Staged by Merck,
•And delivered across borders under live regulation.
Where others still build by hand, DCVax is already factory-ready.
It’s not a project.
It’s a platform—with a factory.
📜 6. Regulatory Pathways and Global Access
Most cell therapies spend a decade proving they work. The next decade is spent trying to figure out how to deliver them.
DCVax is already doing both.
While every other dendritic cell vaccine remains restricted to clinical trials, DCVax is being prescribed to patients today, under real regulatory frameworks, via real facilities, with named-patient oversight.
This is not pending. This is active.
📜 Global Access — A Legal Framework Already in Motion
The UK became the first country to legally authorize personalized therapies like DCVax-L under two synergistic frameworks: the MHRA Specials Pathway, which allows named-patient use of unlicensed medicines, and Statutory Instrument 2025 No. 87 (SI 87), which enables decentralized manufacturing, booster-class integration, and international vaccine dispatch without full marketing approval. A patient’s tissue can now be shipped into the UK, processed under GMP, and returned as cryopreserved DCVax—all fully legal.
Across the EU, Hospital Exemption laws and new EMA guidance support the same model. Combined with Flaskworks automation and NWBO’s UK–EU footprint, DCVax is structurally aligned for multi-country expansion.
In the U.S., the FDA’s 2025 CNPV pilot fast-tracks cell therapies like DCVax—those with completed Phase III data, GMP deployment abroad, and global relevance. With no need for BLA resubmission and review times as short as 30 days, DCVax is poised to enter Project Orbis alongside regulators from the UK, Canada, Australia, Brazil, and Singapore. No other dendritic cell therapy is this close to synchronized international rollout.
🧠 Global Legal Readiness
DCVax is not just legally approved somewhere.
It is the only dendritic cell platform in the world that is:
•Actively delivering under legal prescription
•Operated in a decentralized GMP facility
•Recognized in parliamentary debate
•Supported by ATMP infrastructure programs
•Cryogenically staged for international dispatch
•Eligible for voucher-based, cross-jurisdictional acceleration
Every other DC vaccine is still trying to figure out access.
DCVax already has one—and it’s open.
🧩 7. DCVax-Direct — Completing the Platform
If DCVax-L is the immune engine, then DCVax-Direct is the ignition system.
Where DCVax-L collects tumor lysate at surgery and primes systemic immune response, DCVax-Direct delivers fresh dendritic cells directly into unresectable tumors, where they pick up antigens in situ, mature on-site, and trigger local immune activation within the tumor microenvironment itself.
This makes DCVax not just a static vaccine, but a dynamic system that can:
•Learn from the tumor in real time
•Process previously inaccessible antigens
•Recruit immune effectors into regions of immune privilege
•Create abscopal responses—even in metastatic, diffuse, or immune-cold tumors
It doesn’t matter if the tumor can’t be removed. If it can be reached, DCVax-Direct can make it visible.
🧠 The Biology of In-Situ Immune Ignition
When DCVax-Direct is injected into the tumor:
•Autologous dendritic cells pick up endogenous tumor debris
•These DCs mature inside the hostile microenvironment
•They secrete IL-12 and IFNγ
•They migrate to lymph nodes and prime the full immune stack
•Antigen spreading is triggered
•Immune traffic begins flowing into the tumor
•Remote lesions (even in other organs) can begin to regress
This was demonstrated in the DCVax-Direct Phase I trial, where some patients with inoperable tumors (including sarcoma and breast cancer) saw non-injected lesions shrink—a rare and powerful indicator of systemic immune engagement.
No other dendritic cell platform has done this.
🔄 The Modular Booster Layer — Programmable Immunity in Action
DCVax-Direct isn’t just a delivery method—it’s a programmable immune interface. Through Eden, the system can integrate a range of booster classes—TLR agonists like Poly-ICLC (TLR3) and G100 (TLR4), cytokines like IFNγ and IL-12, oncolytic viruses like V937, and even transdermal agents like R848 and Prevnar—each selected based on patient profile and tumor context. These enhancers can be applied intratumorally, ex vivo, or topically. Eden assigns the correct booster by class and timing without re-approval under SI 87, creating a modular system that adapts across delivery modes (L or Direct), input types (lysate, mRNA, pooled), and therapeutic goals—without resetting the protocol. It’s not a fixed vaccine. It’s an immune stack, built to be tailored.
🌐 Beyond GBM — From One Cancer to Every Cancer
With DCVax-Direct, the platform evolves from a GBM-specific therapy into a broadly applicable, tissue-agnostic immune system. Already tested in over 15 solid tumors—including sarcoma, breast, pancreas, and melanoma—it operates across stages, from localized to metastatic, and reaches tumors previously considered immune-inaccessible. Its future extends into head and neck cancers, hepatic and lung metastases, pancreatic ductal adenocarcinoma, neurological diseases like ALS, and even chronic viral lesions such as HPV-positive tissue reservoirs. Direct isn’t a supplement—it’s the ignition mechanism that transforms DCVax into a modular, adaptive immune platform.
Together, L and Direct form the full immune stack: systemic priming, intratumoral ignition, programmable logic (via Eden), reproducible production (via Flaskworks), global deployment (via SI 87 and WP50), voucher-enabled acceleration (via CNPV and Orbis), and a defensible patent core—all anchored by survival data. No other dendritic cell platform offers this. Most aren’t even aiming for it.
✅ 8. Conclusion — There Is No Comparison
By every meaningful measure—clinical, immunologic, regulatory, industrial, and legal—DCVax stands alone.
It is the only dendritic cell platform that has passed the test of time, the test of trial, the test of scale, and now—quietly—the test of access. It:
•Demonstrated a survival benefit in a prospective, global Phase III trial
•Achieved cryopreserved, GMP-compliant manufacturing with automated reproducibility
•Delivered therapy to real patients under sovereign regulatory pathways
•Integrated programmable boosters with immune class logic
•And secured one of the broadest patent fortresses in cell therapy history
Others are still designing.
DCVax is already delivering.
🧠 The Field Has Begun to Notice—But It’s Late
In 2025, eBioMedicine (The Lancet) published a sweeping review of glioblastoma vaccines. Dozens of entries, many approaches, few results. Only one platform was cited as:
•Demonstrating Phase III survival benefit
•Operating in both newly diagnosed and recurrent GBM
•Using whole lysate personalization
•Delivering clinical impact with long-term immune activation
•Actively used in real-world patients
📄 Source:
Glioblastoma vaccines: past, present, and opportunities
eBioMedicine (The Lancet), 2025
thelancet.com/journals/ebiom…
The field is beginning to align around what DCVax has always been.
But the moment is not new. It’s just finally visible.
🧩 DCVax Is the Full Immune Stack
•DCVax-L captures the whole tumor fingerprint
•DCVax-Direct renders inoperable tumors immunologically accessible
•Eden automates the process and assigns logic
•Advent, Flaskworks, and WP50 close the loop from tissue to dose
•SI 87, CNPV, and Orbis enable borderless, voucher-ready deployment
•Booster Class Modules make it adaptive across cancers
•The patents lock in the method, automation, and delivery
•Patents secure the architecture behind both the product and its delivery
•And the survival data proves it’s already working
No other dendritic cell vaccine offers this.
Most aren’t even aiming for it.
🧘♂️ The Ox Was Never Lost
In Zen tradition, there is a parable of the ten ox-herding pictures.
The ox represents truth, clarity, or enlightenment. At first, the student searches. Then glimpses. Then struggles. Then captures. Eventually, the ox is tamed.
But in the final pictures, the ox is gone.
Not because it was defeated.
Because it was never missing.
The master simply returns to the village—barefoot, silent, smiling—having realized that what was sought had always been present.
DCVax is that ox. 🐂
It didn’t roar. It didn’t fight to be noticed.
It just continued—quietly built, quietly scaled, quietly delivered.
And now, after years of searching, the field looks up and sees what was always there.
There is no need to defend it.
There is no peer to compare it.
There is only what works. And what already is.
$MRK $PFE $BMY $GILD $JNJ $BGNE $INCY $AZN $REGN $NVS $NBIX $MDGL #immunotherapy #celltherapy #dendriticcells #glioblastoma #ATMP #MHRA #FDA #ProjectOrbis #CNPV #Flaskworks #personalizedmedicine #biotech #oncology #immunooncology #checkpointinhibitors #GBM #cancerresearch #precisionmedicine #biopharma #tumorvaccines #cellandgenetherapy #DCVaxL #DCVaxDirect #EdenSystem #SI87 #clinicaltrials #realworlddata

2
3
54
3,207
23 Jul 2025
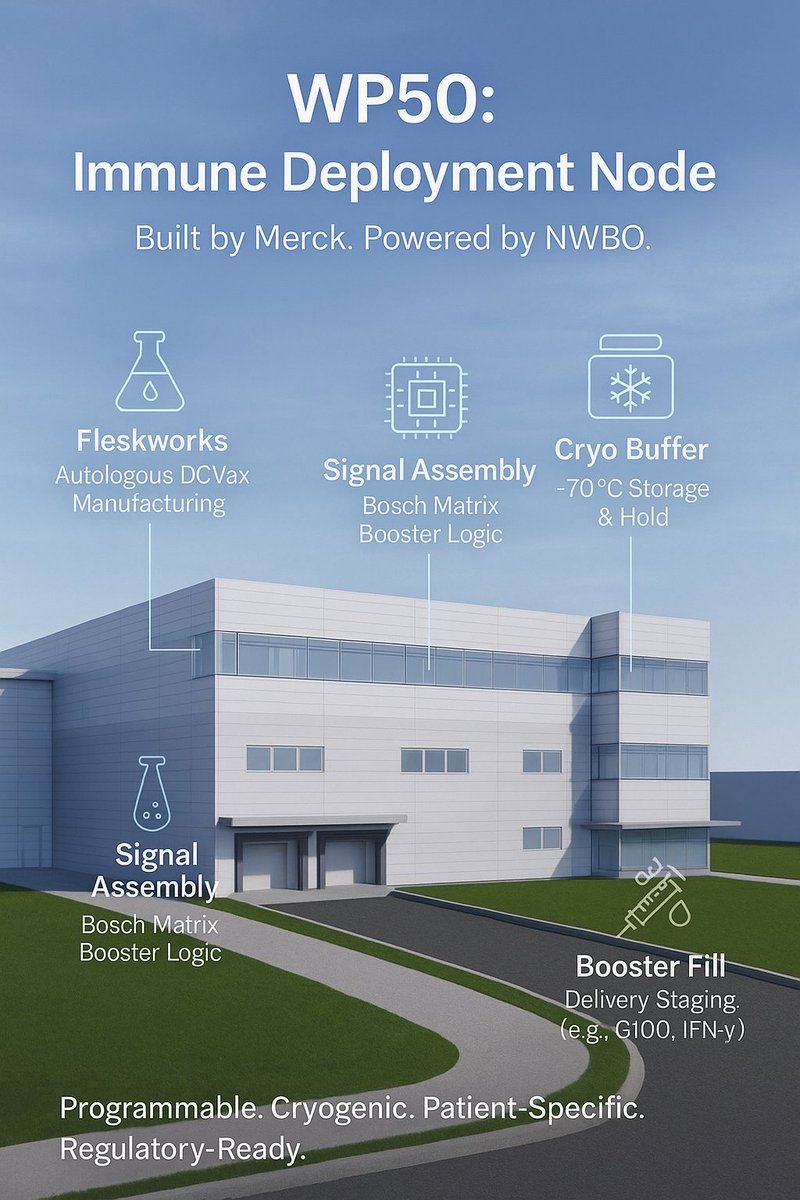
🧬 How $MRK WP50 Became the Hidden Deployment Hub for $NWBO Programmable Immune System
What began as a “vaccine plant” is now the staging ground for modular, patient-specific immunotherapy kits, built to deploy, not mass-produce.
⏱️ Estimated Read Time: 24-28 minutes
🏗️ The Facility That Quietly Changed Everything
In early 2021, as global headlines focused on mRNA, Merck quietly broke ground on a project that had nothing to do with COVID, flu, or Gardasil. The filing called it “Building 50” — WP50 in internal terms — and labeled it a “vaccine and office” expansion at the company’s massive West Point campus in Pennsylvania.
But behind that generic description was a $120 million facility unlike anything else in Merck’s vaccine empire.
WP50 wasn’t designed for bulk manufacturing. It was built for precision staging — specifically, for modular immunotherapy kits. No batch fermenters. No large-volume bioreactors. And critically, no design elements to support high-throughput conjugate vaccine production, like what Merck uses for Prevnar or MMR.
Even its legal footprint gave it away. WP50 received a stormwater discharge exemption — a regulatory carve-out typically reserved for low-effluent, cleanroom-intensive sites like biologic dispatch facilities. Its projected wastewater output was just 3,500 gallons a day. That’s less than a commercial laundromat.
Why would Merck invest that much into a facility that doesn’t produce at scale?
Because it wasn’t built to output product.
It was built to input logic.
🔬 A Facility Built for a Therapeutic Reboot
The timing was no coincidence.
In 2021, three key developments redefined the landscape of personalized immunotherapy:
•DCVax-L had just published its long-awaited glioblastoma survival results in JAMA Oncology
•DCVax-Direct completed Phase I, showing measurable tumor regression across multiple solid tumors with direct injection
•Mayo Clinic had begun releasing trial data showing that traditional conjugate vaccines like Prevnar and Pneumovax could enhance dendritic cell therapy when injected into tumors
Simultaneously, Northwest Biotherapeutics (NWBO) acquired Flaskworks — a Boston startup developing fully automated dendritic cell manufacturing hardware — and licensed IP from Roswell Park covering microbial adjuvants and DC maturation.
In short:
The architecture for a logic-coded immune platform had emerged.
And WP50 looked built to support it.
Its layout — sterile fill rooms, cryogenic bays, and modular cleanroom segmentation — points to one thing: a real-time immunotherapy staging facility, not a traditional vaccine plant.
This is where the immune code gets deployed.
❄️ Cryo as a Design Principle — Not a Feature
Most vaccine plants operate with refrigeration between 2°C and 8°C. Even mRNA requires only −80°C at most. WP50 was designed for sub–150°C cryogenic staging — the range needed for autologous cell therapies like DCVax.
That kind of deep freeze isn’t a convenience.
It’s a commitment.
It means the facility is architected to handle living cell products that must stay frozen from the moment of manufacture to the moment of injection — no room temperature hold, no thaw until delivery.
That matches:
•DCVax-L, cryopreserved and patient-specific
•Poly-ICLC, a lyophilized RNA mimic that benefits from cryogenic buffering pre-fill
•IFN-γ, DECOY20, and other Matrix-class boosters that require temperature integrity
This isn’t speculative. It’s architectural logic.
Merck didn’t just install cryo bays for flexibility.
They embedded them as a core design element — because the kit they were building wasn’t generic.
It was meant to be customized. And cold. And ready to run.
🧬 Not a Fill Plant — A Signal Router
On its second floor, WP50 houses modular cleanrooms configured not by product line, but by signal class — the logic-coded categories that correspond to booster types in the Bosch Matrix.
Each suite can be isolated by function, allowing WP50 to:
•Fill lyophilized viral mimics like Poly-ICLC (Class A)
•Prepare sterile liquid emulsions like G100 (Class B)
•Load recombinant cytokines like IFN-γ or IFN-α2 (Class I)
•Co-package pre-filled syringes like Prevnar (Class V), filled nearby at Merck’s Building 63A
•Pair killed microbial agents like DECOY20 (Class D) or depot-formulated adjuvants like R848 (Class C)
This isn’t a production line.
It’s a programmable stack execution node.
When Flaskworks manufactures a batch of DCVax for a patient, WP50 doesn’t just hold the vial. It fills or stages the corresponding immune boosters, labels the kit, and prepares it for personalized dispatch.
DCVax is the payload.
WP50 is the switchboard.
🏛️ B32 — The Vault That Buys Time
Every high-speed node needs a buffer. That’s where Merck’s Building 32 (B32) comes in — a dedicated −70°C storage facility integrated into the same West Point grid as WP50.
Its job isn’t to produce.
Its job is to pause.
If Flaskworks finishes manufacturing but regulatory clearance isn’t ready, B32 holds the cryopreserved vaccine vials. If Eden scripts a booster stack that requires coordination, B32 holds the partially assembled kit until pairing is complete. If a trial site needs rolling inventory — B32 stages, tracks, and preserves.
The layout includes:
•Walk-in cryogenic vaults
•Mobile ultra-cold units
•GMP-grade chain-of-custody logs
•Batch-linked barcode tracking
This isn’t warehouse storage.
It’s deployment buffering for a living therapy that can’t afford to degrade.
Together, WP50 and B32 form a two-node immune engine:
•One that executes.
•One that preserves.
🔁 SI 87 and CNPV: The Legal Rails That Activate the Grid
Even the most sophisticated system is useless without regulatory alignment. WP50 doesn’t operate in isolation. It sits squarely between two real-world legal frameworks that allow its logic-coded kits to move.
🇬🇧 SI 87 – UK Specials Law
•Allows named-patient use of unlicensed autologous cell therapies
•Supports pairing with GMP-grade boosters not yet centrally authorized
•Enables import/export of cryopreserved DCVax kits into the UK
•No marketing license required — just physician justification and GMP documentation
🇺🇸 CNPV – Commissioner’s National Priority Voucher (FDA)
•Enables 60–180 day review for therapies with completed Phase III trials
•Accepts patient-specific, real-world–ready formats
•Requires no new trial if safety/efficacy are proven — which they are for DCVax-L (via JAMA Oncology)
•Compatible with Flaskworks production and WP50 fill logic
This means Merck’s West Point stack is already regulatory-operable on both sides of the Atlantic.
In one mode, WP50 assembles and ships kits into the UK under SI 87.
In another, it stages and dispatches them domestically under CNPV clearance.
In both, it bypasses traditional drug launch infrastructure — and moves the immune system at patient speed.
🧬 From Tissue to Therapy: A Personalized Immune Stack in Motion
This isn’t drug delivery. It’s logic delivery.
Every DCVax kit begins not in a factory, but with a patient’s own biology — a tumor sample and a monocyte harvest via leukapheresis.
There are two therapeutic pathways:
•DCVax-L, used post-resection for tumors like glioblastoma
•DCVax-Direct, used for inoperable tumors, with intratumoral injection paired with localized immune stimulants
In either case, the journey starts with living input. Not inventory. Not a generic dose.
And what comes next is automated.
⚙️ Flaskworks — The Engine That Manufactures Immune Code
Flaskworks isn’t a CMO or a contract lab. It’s a closed-system, GMP-enabled hardware platform — built to produce dendritic cell vaccines without human hands.
At its core is Eden, the automated device architecture described in U.S. Patent 10,647,954. Here’s what it does:
•Uses disposable cartridges to isolate, mature, and antigen-load monocytes
•Guides the cells through cytokine programming (e.g., GM-CSF, IL-4)
•Pulses them with tumor lysate — personalized per patient
•Cryopreserves the final DCVax product into single-use, barcoded vials
It tracks flow rate, pressure, pH, and maturation timing in real time — all logged and traceable.
Flaskworks isn’t batch manufacturing.
It’s immune programming — scaled, sealed, and per patient.
🧠 Eden — The Logic That Decides What Comes Next
Once Flaskworks produces the cell-based payload, Eden, NWBO’s internal orchestration system, assigns the booster logic using the Bosch Matrix — a functional immune codebook.
For each patient, Eden determines:
•Which signal classes are needed (A B I, or B C D, etc.)
•Which cytokines or immune tones are ideal (e.g., IL-12p70, IFN-γ)
•Whether the vaccine will be injected systemically (DCVax-L) or intratumorally (DCVax-Direct)
•What delivery formats are appropriate (syringe, patch, depot gel, etc.)
Eden doesn’t generalize. It scripts.
Then WP50 executes — physically pairing Flaskworks-made DCVax vials with logic-matched immune stimulants, all under regulatory guardrails.
No two kits are the same.
Each is a custom-coded immune program — generated from biology, compiled by Eden, and staged by Merck.
🧪 The Bosch Matrix: Functional Immune Classes That Plug In Like Code
In 2025, Dr. Marnix Bosch publicly outlined a new way to classify immune stimulants — not by molecule, but by signal function. This framework, now known as the Bosch Matrix, divides immune boosters into modular, combinable classes:
•Class A: Viral Mimics
e.g., Poly-ICLC (Hiltonol) — lyophilized dsRNA that triggers TLR3, driving Type I interferons and IL-12p70 for systemic T-cell priming.
•Class B: Inflammatory Ignition (TLR4)
e.g., G100 — a nanoemulsion used intratumorally to induce APC recruitment and localized inflammation.
•Class C: TLR7/8 Modulators
e.g., R848, MEDI9197 — small molecules that fine-tune innate immune tone; may be formulated as depot injections or topical gels.
•Class D: Danger Signal Inducers
e.g., DECOY20 — killed microbial ligands that activate PRRs broadly, often used for intratumoral shock priming.
•Class I: Cytokine Amplifiers
e.g., IFN-γ or IFN-α2 — recombinant proteins used to restore signaling in low-responder or immunosuppressed patients.
•Class V: Recall Triggers
e.g., Prevnar, Pneumovax — pre-filled conjugate vaccines originally used for infectious disease, now reimagined to awaken myeloid memory in cancer.
Each class isn’t a brand. It’s a function.
Each agent isn’t just a drug. It’s a signal in a stack.
And WP50 was designed to physically execute every one.
🏭 WP50 Matches Format to Function
Each Matrix class has a specific physical format:
•Lyophilized (Class A, Class C)
•Cold-chain liquid (Class B, Class I)
•Sterile-filled microbial suspension (Class D)
•Pre-loaded syringe (Class V)
WP50’s layout aligns precisely:
•Lyophilization lines to prep Poly-ICLC and TLR7/8 agents
•Cold-fill bays for nanoemulsions and recombinant cytokines
•Cryo staging rooms for DCVax vials and Poly-ICLC intermediates
•Sterile prep suites for microbial adjuvants like DECOY20
•Labeling and co-packaging docks for Prevnar or Pneumovax syringes filled at B63/B63A
Each cleanroom suite can be dedicated to one signal class, ensuring sterility, format integrity, and per-class documentation.
That means WP50 can produce:
•A DCVax-L Poly-ICLC IFN-γ combo
•A DCVax-Direct G100 DECOY20 pairing
•Or a multi-stage DCVax-L regimen boosted over time with different Matrix agents
The building doesn’t run a pipeline.
It runs immune instructions, per patient.
💉 L vs. Direct: Route Matters — So Does Format
The booster logic isn’t just scientific. It’s spatial.
•DCVax-L is administered systemically, usually intradermally or subcutaneously, meaning boosters like IFN-γ or Poly-ICLC can be given separately, sometimes on offset schedules. Format flexibility is helpful but not always critical.
•DCVax-Direct, however, is injected into the tumor, often under image guidance. Boosters for Direct need to be:
•Pre-filled
•Timed precisely
•Co-localized with the injection
This makes sterile, syringe-ready boosters essential, especially for intratumoral agents like G100 or recall adjuvants like Prevnar.
That’s where Merck’s Building 63A completes the loop.
Its 70 million–dose annual capacity wasn’t built for DCVax itself.
It was built to stage the booster fuel — for programmable, injectable therapy kits.
In short:
•DCVax is the driver.
•The Bosch Matrix is the map.
•WP50 and 63A are the vehicles.
•And the destination is real-world immune control, on demand.
🌍 Kits Become Infrastructure: How the Immune OS Scales Without Rebuilding Pharma
In traditional biotech, scale means inventory — vials on shelves, pallets in warehouses, and global supply chains stretching across months.
But NWBO’s model scales differently.
Here, the therapy is logic-coded, and the supply chain is node-based:
•Flaskworks units produce immune payloads per patient
•Eden scripts booster combinations using Matrix logic
•WP50 stages and deploys kits per regulation
•And B32 or equivalent cryo storage buffers demand
To replicate the system, you don’t need a new factory.
You just need another node that speaks the same immune language.
🏗️ Flaskworks as the Hardware Platform, Eden as the Software Stack
Each Flaskworks unit is a sealed, GMP-certified immune factory:
•Small enough for hospital-based GMP suites
•Cleanroom-ready for CMO or academic installs
•Fully automated, running Eden’s logic scripts on disposable cartridges
And Eden doesn’t change across geographies.
It speaks the same Bosch Matrix logic, Class A through V, no matter where it’s installed.
That means:
•A patient in London can receive DCVax-L Poly-ICLC IFN-γ from a Flaskworks unit at Advent
•A patient in Chicago can receive DCVax-Direct G100 DECOY20 from a node built at a local health system
The inputs vary.
The platform doesn’t.
It’s scalable, transferable, and globally regulatory-aligned.
✅ It’s a franchise model, for personalized immunity.
🛠️ Final Assembly: Why Merck’s Infrastructure Quietly Completes the Immune Stack
The real story of WP50 isn’t about vaccine volume.
It’s about immune precision—and industrial enablement.
During COVID, Merck built WP50 and 63A to quietly house something the market hadn’t yet named:
a programmable immunotherapy distribution system, routed by biology, not batches.
Today, it connects:
• Flaskworks: the engine that makes personalized DCVax from patient tissue
• Eden: the logic compiler that assigns Bosch Matrix–class boosters
• WP50: the facility that assembles, matches, and packages each stack
• B32: the vault that buys time, preserving each kit until dispatch
• 63A: the syringe engine that fills, stages, and scales real-world delivery boosters
• SI 87 and UK Modular Manufacturing Law: the legal rails that now authorize decentralized, per-patient immunotherapy delivery
This is no longer theoretical.
As of July 23, 2025, the UK’s Human Medicines (Amendment) (Modular Manufacture and Point of Care) Regulations 2025 is now in force—a world-first legal framework enabling personalized cell and gene therapies to be manufactured, assembled, and administered near the patient.
The law supports:
• On-site and mobile production
• Small-batch or single-patient dosing
• Cryogenic handoff and direct dispatch
• Regulatory control without re-approval
It is tailor-made for what WP50 already does.
And globally, regulators are catching up. The ICMRA’s international working group has now endorsed decentralized, point-of-care manufacturing as a viable and harmonizable pathway for advanced therapies, making WP50 not just a national asset, but a globally replicable immune infrastructure model.
“Highly personalised treatment—made for one person, in one place, at one time—becomes part of routine care,”
said MHRA Chief Executive Lawrence Tallon.
And this infrastructure isn’t operating in a vacuum.
While the U.S. has not yet enacted a formal decentralized framework, the CNPV (Commissioner’s National Priority Voucher) initiative shows signs of convergence, potentially offering expedited review for platforms like DCVax that already completed Phase III. If adopted, it would align the U.S. operationally with the UK’s legal breakthrough.
This system wasn’t built for Prevnar or Gardasil.
It was built for DCVax.
And it works with every Matrix-class booster, even those Merck doesn’t own, because the stack isn’t built around brands.
It’s built around immune function: signal mimics, TLR agonists, cytokine drivers, memory triggers.
What matters is not the molecule, but the message.
• Poly-ICLC? Check.
• DECOY20? Check.
• R848? G100? IFN-γ? Check, check, and check.
Merck owns the infrastructure.
NWBO owns the code.
And together, they’ve quietly constructed something no one else has:
a plug-and-play immune execution engine, now legally operable in the UK, and structurally ready for the U.S. the moment policy catches up.
They didn’t just build a therapy.
They built an operating system for live, logic-coded immunity.
It’s not theoretical.
It’s running.
And now, under law
It’s deployable.
It’s scalable.
It’s real. 🗽
$MRK $BMY $PFE $GILD $LLY $AZN $MRNA $VXRT $BGNE $INBX $MDCX $ONCS $MODV $VIR $REGN $SAGE $IOVA $TCRT $INDP $JNJ $NVS $SGEN $NVO
#DCVax #Immunotherapy #CellTherapy #PersonalizedMedicine #CancerVaccine #DendriticCells #BoosterStack #Flaskworks #BoschMatrix #ProjectOrbis #ModularManufacturing #CryogenicStorage #SI87 #CNPV #Biotech #Oncology #ImmuneSystem
3
5
57
7,755
16 Jul 2025
$NWBO💥 Part 2 of 2: The Big Bang
How Bosch, Flaskworks, and Yorkville Positioned DCVax to Scale as a Modular Immune Platform
🎗️ #GlioblastomaAwarenessDay
🤝 No Conflict, No Coincidence & The Silence That Speaks Volumes
If Mayo had independently solved the core lysate immunogenicity problem, reverse-engineered NWBO’s maturation protocol, and reproduced the functionality of Flaskworks manufacturing, all without any licensing or collaboration, NWBO and Roswell would be legally obligated to respond.
They haven’t.
There has been no IP dispute. No objection. No barrier raised.
That silence isn’t an oversight.
It’s a signal.
NWBO’s patents and trade secrets protect not the raw materials (tumor lysate) but the methods by which that material is transformed into immune instruction. If Mayo were operating outside those bounds, it would jeopardize NWBO’s core asset, and Roswell’s licensed IP portfolio.
Instead:
•NWBO remains silent on Mayo’s platform.
•Mayo publishes immune results that match NWBO’s.
•No competing lysate-processing method has been published.
•Flaskworks-level reproducibility appears evident in Mayo’s results, suggesting a maturation process and manufacturing logic that anticipates or parallels what Flaskworks now automates.
That same platform logic reemerges, with architectural fidelity, in their intratumoral and neoantigen-based DC programs.
There are only two possible explanations:
1.Mayo independently invented a fully functional, scalable, and unpublished DCVax clone that just happens to work the same way and produce the same results.
2.Mayo is operating under a licensing arrangement, joint development pathway, or embedded SOP system aligned with NWBO.
The second explanation is not just more plausible, it’s overwhelmingly supported by the data, the silence, and the structure of the trials themselves.
Les Goldman once described NWBO’s method as “Coca-Cola-like,” not in branding, but in the proprietary combination of steps, timing, and composition. You can try to imitate it, but without the formula, it doesn’t work.
And yet Mayo’s version works.
Which strongly suggests: they’re using the formula.
🧠 Strategic Implications & Mayo Validates DCVax as a Universal Immune Engine
If Mayo Clinic’s dendritic cell vaccine program is, in effect, running on NWBO’s methodology, then Mayo isn’t just conducting trials. They’re confirming the core hypothesis of DCVax at scale. Quietly, methodically, and across multiple tumor types.
What this proves is that DCVax is not limited to glioblastoma. It’s not niche. It’s not hypothetical. It’s a tumor-agnostic, modular immunotherapy framework that can be reproduced (and has been) across completely different oncologic landscapes.
Mayo has now shown that dendritic cell–based immunotherapy, executed with DCVax-aligned maturation logic and immune timing, can produce durable responses across tumor types. In glioblastoma, they used pooled allogeneic lysate; in ovarian, melanoma, and lymphoma, they used autologous or in situ antigens with striking results.
•The DCVax method translates to epithelial cancers (ovarian)
•It is safe and immunologically active when combined with checkpoint inhibitors (melanoma, NHL)
•It adapts to intratumoral delivery following cryoablation (DCVax-Direct logic)
•It performs across immune environments: CNS (GBM), peritoneal (ovarian), cutaneous (melanoma), hematologic (NHL)
In regulatory terms, Mayo has effectively conducted a multi-indication expansion trial, just without the branding. This is what the FDA, MHRA, and EMA refer to as mechanism-based, indication-agnostic confirmation, the kind of pattern that supports accelerated tissue-agnostic approval.
And crucially, this was done without any publicly disclosed manufacturing innovation. Mayo didn’t invent new antigen enrichment, or new maturation protocols. They deployed an existing method—consistently, quietly, and successfully.
That method was DCVax.
What Mayo has built is a third-party validation track for the DCVax platform, executed independently but functionally inseparable from its origin.
And in doing so, they’ve helped confirm that DCVax is not just a product, but a reproducible immune operating system, one whose logic they’ve quietly validated, trial by trial.
🌐 Regulatory and Clinical Convergence & A Tissue-Agnostic Precedent in Plain Sight
Modern regulatory science is no longer tethered to organ type. The defining logic of tissue-agnostic approval is mechanism over morphology. If a treatment mechanism consistently produces immune activation and clinical benefit across distinct tumor contexts, it qualifies for broader, accelerated pathways.
This is already regulatory doctrine. Examples include:
•Pembrolizumab, approved for MSI-high and TMB-high tumors
•Larotrectinib and entrectinib, approved for NTRK fusion regardless of tissue origin
•Recent immunotherapies approved based on immune response patterns, not tumor histology
Now, Mayo’s trials provide a real-world case study in how DCVax logic transcends the boundaries of cancer classification. Consider the diversity:
•GBM: immune-privileged CNS environment
•Ovarian: highly immunosuppressive peritoneal space
•Melanoma: checkpoint-resistant, often heavily pretreated
•NHL: lymphoid origin with localized intratumoral access
Across all of these, Mayo used a constant platform:
•Lysate-loaded DCs
•Same manufacturing architecture
•Consistent immunologic outcome
•Variable combinations (cryo, PD-1, SOC) tailored to context
This is regulatory gold.
It provides:
•Cross-indication consistency
•Immune mechanism reproducibility
•Survival impact across clinical settings
•Implicit compliance with MHRA, EMA, and FDA expectations for advanced therapy products
Mayo has done for DCVax what Keytruda did for checkpoint inhibition: establish a mechanistic footprint across disease contexts.
And because NWBO owns the enabling methodology, they now own the most validated tissue-agnostic cell therapy architecture in oncology—one proven by a top-tier institution without formal branding, but with full biological fidelity.
🧩 The Next Oncology Backbone & DCVax as the Missing Middle Layer
Modern immuno-oncology is layered. But that layering has a gap.
•Checkpoint inhibitors release the brakes on T cells.
•TLR agonists and radiation prime the environment with inflammatory danger signals.
•But few therapies address the core problem: how to present the right antigens to the immune system in a way that drives memory, precision, and tumor clearance.
That’s what DCVax does. It sits in the center.
DCVax is the missing middle layer between immune ignition and immune precision.
What Mayo has revealed is that when you deploy dendritic cells matured using the right immune timing and architecture:
•Cryoablation becomes synergistic, not transient
•PD-1 inhibitors become durable, not exhausted
•Pooled lysate (when used, as in GBM) becomes immunogenic, not tolerogenic
This reframes DCVax as more than a vaccine. It becomes an immune programming module, an engine that can be inserted upstream of checkpoints, downstream of danger signals, and inside combination frameworks.
It’s compatible with:
•mRNA vaccine platforms, while mRNA therapies deliver instructions to host cells to produce neoantigens, dendritic cells trained via DCVax logic can be pulsed directly with those same peptides. Whether encoded by mRNA or derived from tumor tissue, the immune instruction is the same. As Mayo’s neoantigen-pulsed DC trial demonstrated, the platform can present whatever an mRNA vaccine is designed to deliver, no transfection required.
•TLR agonists (Bosch Matrix)
•Synthetic microbials like Indaptus’ Decoy20
•Cytokine-based DC boosters (e.g., IFN-γ, IL-12)
•Even non-viral delivery platforms like SkinJect
DCVax is not just a dendritic cell product, it’s the immune logic layer that tells the system what to do once the brakes are off and the fire is lit.
Mayo has shown that this immune layer works across the tumor map.
Bosch has shown that it can be upgraded modularly.
Flaskworks makes it reproducible.
And regulators now have evidence from a trusted academic center that the platform behaves predictably across systems.
All that remains is to recognize that what Mayo did was not an experiment, it was a deployment.
🔬 From Immune Blueprint to Modular Infrastructure & The Bosch Matrix as a Strategic Map
In 2025, Dr. Marnix Bosch introduced a visual framework that quietly reshaped the field. Known now as the Bosch Matrix, it outlined how the DCVax platform could be stacked, boosted, and modularly adapted across immune contexts and tumor profiles.
At first glance, it appeared to be a table of immune-stimulating agents (Hiltonol, G100, R848, IFN-γ, MEDI9197, V937, Decoy20). But Bosch wasn’t listing drugs. He was publishing a tuning map, an immune expansion layer for DCVax.
Each booster corresponds to a well-characterized immune shortfall:
•Hiltonol (TLR3) enhances systemic priming and memory
•G100 (TLR4) reprograms tumor macrophages
•R848 (TLR7/8) synergizes with cryoablation and DC injection
•IFN-γ upgrades antigen presentation machinery
•Decoy20 mimics microbial inflammation across innate sensors
•MEDI9197 and V937 activate STING or mimic oncolytic viral danger signals
Bosch’s matrix provides the logic for turning DCVax into a programmable platform, adaptable to tumor microenvironment, delivery method, and immune status. The cell product remains constant. The boosters are modular. The stack is composable.
This modularity also extends to mRNA vaccine platforms. While mRNA-based therapies encode tumor-specific neoantigens into host cells, the DCVax framework bypasses the need for in vivo antigen translation. Those same peptides can be synthesized or derived and pulsed directly into dendritic cells ex vivo. As Mayo’s neoantigen trial showed, this platform can present virtually any tumor-defined target, lysate, peptide, or mRNA derivative, with precise immune instruction.
And what makes this more than theory is that Mayo has already proven the core DCVax stack works, even without the Matrix. Their trials validate the base engine: lysate-loaded or in situ-primed dendritic cells, matured using optimized protocols and timed for immune synergy. The Bosch Matrix now serves as the upgrade path, a tuning toolkit ready to be layered onto a system that’s already been shown to function across tumor types.
That makes Bosch’s Matrix not a proposal, but an upgrade path, an immunologic toolkit that can be pulled down, patient by patient, tumor by tumor.
Still, one question remained: How do you deliver these boosters outside of elite clinical settings?
That answer would come not from Bosch, but from a dissolvable patch.
💉 Delivery at the Edge & How SkinJect and Yorkville Complete the DCVax Stack
DCVax has always had a strong center: a method for turning dead tumor tissue into living immune instruction. Flaskworks made that process scalable. Mayo showed it could be clinically validated. Bosch revealed how it could be modularly expanded.
But every immune strategy still needs a delivery layer, a way to get immune modulators into the body repeatedly, precisely, and safely.
That’s where SkinJect enters.
Originally developed for localized squamous carcinoma, SkinJect is a dissolvable microneedle patch that delivers immune-active compounds directly into the dermis, where dendritic cells, Langerhans cells, and resident APCs reside in high density.
Now under Medicus Pharma, and significantly, financed by Yorkville Advisors, SkinJect is structurally suited to deliver nearly every agent in the Bosch Matrix through dissolvable microneedles into the dermis, where dendritic cells and APCs are densely concentrated.
These include:
• R848 (TLR7/8 agonist)
• IFN-γ (cytokine booster)
• Hiltonol (Poly-ICLC) (TLR3 agonist)
• Decoy20 (synthetic microbial mimic, in lyophilized format)
• MEDI9197 (injectable lipid-based TLR7/8 agonist, patch-compatible with formulation)
• V937 fragment (non-replicating viral-derived particle, compatible with microneedle delivery)
In effect, SkinJect transforms the booster layer from an infusion-based hospital intervention into a patient-ready patch, programmable, outpatient-compatible, and ideal for multi-cycle DCVax boosting.
These can now be administered not by infusion or intratumoral injection, but through skin-applied microneedle patches, over the vaccine site or as systemic immunologic ignitions. This enables:
•Local booster delivery at the point of DCVax injection
•Outpatient-compatible regimens with no surgical access required
•Repeatable, patient-friendly dosing—ideal for multi-cycle immune programming
In effect, SkinJect extends Flaskworks from the vial to the patient’s skin. It solves the final barrier to field deployment.
And Yorkville saw it coming.
The Yorkville Axis & Capital as Immunologic Infrastructure
In Q1 2025, Yorkville Advisors executed three separate financings. Individually, they could be dismissed as opportunistic. Together, they form a capital blueprint:
•NWBO (DCVax) the immune instruction engine
•Indaptus Therapeutics (Decoy20) the microbial ignition system
•Medicus Pharma (SkinJect) the dermal delivery layer
Each entity corresponds to a critical layer in the DCVax stack:
•The antigen-presenting logic
•The synthetic booster
•The scalable deployment port
Yorkville didn’t just invest broadly—they structured their capital along the immune stack itself:
• NWBO – the antigen-presenting instruction layer
• Indaptus – the synthetic microbial ignition
• Medicus/SkinJect – the dermal delivery mechanism
Through these investments, Yorkville has positioned itself at every key junction of the immunologic supply chain. They don’t control the science, but they’ve aligned their capital with the architecture:
• Flaskworks manufactures the immune engine
• Mayo validates its real-world function
• Bosch outlines the upgrade path
• SkinJect delivers it to the patient
• And Yorkville underwrites the scale
DCVax is no longer just a product. It is a fully modular, capital-backed immune architecture, positioned to scale beyond hospitals, beyond glioblastoma, and beyond static treatment logic.
It is programmable. It is portable. And thanks to Mayo, Bosch, SkinJect, and Yorkville, it is now provable.
And so, on Glioblastoma Awareness Day, we close this chapter with gratitude, for the patients who gave their tissue, their time, and often their lives to trials that quietly rewrote the future. DCVax is no longer just theory. It is proof, built on the courage of those who endured the impossible, and on the silence of institutions that chose action over applause. This isn’t just science. It’s legacy.
#FLASKWORKS #SKINJECT $MDCX $INDP #YORKVILLE $TCRT $SIOX $IBRX $MODV $MDGL
#BoschMatrix #Flaskworks #SkinJect #ProgrammableMedicine
#ModularImmunotherapy #SyntheticImmunity #TherapeuticStack
#OncologyPipeline #ProjectOrbis #ImmunoOncology #YorkvilleStack
4
5
39
4,137
8 Jul 2025
📢 Calling all $NWBO investors, FDA wants to hear from the public 🎯
FDA Direct is now accepting public questions for future episodes. This is a rare, official channel to elevate the issues that affect DCVax and other autologous therapies, and it’s being recorded on the public record.
I just submitted the following question:
“What specific mechanisms, if any, exist within FDA’s current regulatory framework (e.g., CoGenT pilot, Real-Time Oncology Review, or other collaborative pathways) to enable approval or access for individualized autologous cell therapies like DCVax-L that rely on decentralized, patient-specific manufacturing, and how is the FDA addressing the traceability and oversight challenges associated with such therapies under current law?”
If you agree this deserves a public response, you can submit the same wording or modify it slightly to reflect your voice.
🧭 To submit, just use the FDA Direct link included in the reposted tweet below, that’s the official source.
Let’s raise the visibility of personalized immunotherapy and show the FDA that this community is engaged, informed, and watching.
#DCVax #FDA #CellTherapy #CoGenT #Flaskworks #Immunotherapy #NWBO #MHRA #ProjectOrbis

Got a question for the FDA Commissioner?
In our next FDA Direct conversation, we'll be fielding questions from the audience. Click the link below to submit yours!
fda.gov/news-events/interact…

4
24
2,052
28 Jun 2025
$NWBO 🧠 They Just Discovered What DCVax Already Fixed
A new Nature paper just announced something they think is groundbreaking: dendritic cells (DCs) the immune system’s scouts, can’t move inside tumors.
According to the researchers, as cancers grow, the tumor microenvironment shuts down nitric oxide, which shuts down soluble guanylyl cyclase, which shuts down cGMP, which shuts down myosin-II, the little molecular engine DCs use to crawl. With that system offline, dendritic cells can’t get from the tumor to the lymph nodes to alert the T cells. And if the T cells don’t get the message, the immune system doesn’t show up.
Immune collapse by traffic jam.
Their fix?
Sildenafil.
Yes, that sildenafil.
Better known by its street name: Viagra.
It turns out, if you pop a PDE5 inhibitor, you can restore cGMP, re-activate DC motility, and re-light the immune fire. In mouse models, this brings DCs back online and gets the immune system rolling again.
Clever biology. Bold move. Exciting headline.
But here’s the quiet part:
DCVax already fixed this. Years ago. And it didn’t need a prescription.
🧬 DCVax-L: Bypass the Battlefield
DCVax-L doesn’t even engage with the paralyzed, tumor-trapped dendritic cells the Nature paper’s trying to save. Instead, it replaces them altogether.
How?
It takes monocytes from the patient’s blood.
Grows them into healthy, antigen-loaded DCs in a clean lab.
Matures them with surgical precision.
And injects them into the skin, far from the toxic TME.
These DCs then migrate to the lymph nodes like any healthy immune cell would and get straight to work. No suppression. No detour. No Viagra.
DCVax-L doesn’t hack the system. It sidesteps the failure entirely.
⚔️ DCVax-Direct: Right Into the Fire, And Still Marching
Now DCVax-Direct is a different beast.
It goes directly into the tumor, right into the environment the Nature paper says is hostile to DC movement. If there’s ever a test case for whether DCs can function under pressure, this is it.
But according to Dr. Marnix Bosch’s June 2025 NYAS presentation, DCVax-Direct doesn’t just survive there.
It thrives.
In over half of patients, DCVax-Direct triggered CD4 and CD8 infiltration in just 7 days .
It caused systemic immune activation, with matching T cell clones in blood and tumor .
It shrunk distant tumors after injecting just one lesion, the abscopal effect in action.
And it did this in patients who had failed everything else.
And here’s the kicker: these responses directly correlated with TNFα and IL-12, two key cytokines that regulate DC migration and T cell priming. Exactly the signaling axis the Nature paper says is broken.
So what they were trying to patch with PDE5 inhibitors?
Bosch’s DCs were already doing it, in humans, under real-world conditions.
⚙️ Supercharging with Boosters: No Blue Pill Needed
Bosch also unveiled next-gen DC enhancement:
Booster cocktails that turbocharge cytokine output, including TNFα, IL-12p70, IFNγ, CXCL9, CCL2, GM-CSF, and more .
These agents can convert low producers into high responders and expand immune reach .
They even upregulate migratory and chemotactic molecules, so the DCs don’t just survive in the tumor… they move, they signal, and they lead .
It’s a masterclass in pre-programming.
While other therapies hope the immune system wakes up, DCVax-Direct shows up with cells that are:
Locked.
Loaded.
And looking for lymph.
💊 Who Needs the Little Blue Pill Now?
Checkpoint inhibitors? They assume DCs are functioning.
In situ vaccines? Same problem.
Most cancer immunotherapies? Still depend on the very endogenous DCs that this paper proves are asleep at the wheel.
So yeah, maybe they need a boost.
But DCVax-L?
It delivers the message directly to the command center.
And DCVax-Direct?
It parachutes into enemy territory, sets up a cytokine outpost, mobilizes the troops, and radios for air support.
All without needing pharmacological encouragement.
🎯 The Final Word, And the Fun One
Let’s not dance around it.
Other cancer immunotherapies might need Viagra just to get their dendritic cells to show up.
Meanwhile:
DCVax-L is already at the lymph node giving the briefing.
DCVax-Direct is already lighting fires in tumors and calling in T cell reinforcements.
So if you’re wondering who really needs the little blue pill…
It’s not DCVax. DCVax is the blue pill.
“Ask your doctor if your immune system is ready.
Side effects may include sudden immune competence, distant tumor shrinkage, long-term survival, and unexpected investor confidence.
If tumor regression lasts more than four years, please alert the media.”
📄 Nature Study: Rescuing dendritic cell interstitial motility: nature.com/articles/s41586-0…
📊 Bosch NYAS 2025: DCVax-Direct triggers cytokine-driven DC migration, T cell priming, and systemic responses, in real patients nwbio.com/wp-content/uploads…
$IBRX $IMTX $MRK $PFE $BMY $REGN $VRTX $CTMX $SANA $IOVA $GILD $AZN $JNJ $NVS $AMGN $SNY $LLY $AMZN
#DCVax #Immunotherapy #CancerImmunotherapy #DendriticCells #DCVaxL #DCVaxDirect #TumorMicroenvironment #TME #BiotechStocks #BiotechInvesting #Oncology #CancerVaccine #PersonalizedMedicine #CheckpointInhibitors #MHRA #NIH #NYAS #GBM #Glioblastoma #CancerTreatment #CDMO #Cytokines #AdaptiveImmunity #CancerImmunityCycle #ProjectOrbis

5
15
110
8,488
26 Jun 2025
$NWBO 🧬The Immune System Isn’t Broken, It’s Trapped
Checkpoint inhibitors didn’t fail.
They opened the door, and exposed what was missing.
The problem isn’t immune invisibility.
It’s strategic paralysis.
In most solid tumors, the immune system either never arrives, or worse, arrives but sits idle, suppressed, or confused.
One of the most powerful silencers isn’t PD-1.
It’s adenosine.
🧪 Adenosine: The Tumor’s Invisible Cage
In hypoxic, nutrient-depleted tumors, ATP is released as a danger signal. But that signal is hijacked.
CD39 and CD73 degrade ATP into adenosine, a potent immunosuppressive molecule that turns inflammation into sedation.
🧠 Adenosine acts like a chemical cage:
• A2A Receptors (T cells, NK cells):
Suppress cytokines, killing function, and energy metabolism
• A2B Receptors (myeloid, stromal, endothelial):
Amplify IL-10, VEGF, fibrosis, and suppressive macrophages
Mute dendritic cell activation and tumor antigen presentation
📈 In solid tumors, adenosine levels can rise 100x above normal tissue.
This isn’t just a cold tumor.
It’s a chemically encrypted one.
🔍 Breaking the Adenosine Trap
🧱 Tier 1: Receptor Blockers (A2A / A2B)
Merck
→ MK-1088, M1069
→ Dual A2A/A2B inhibitors
→ Milestone-triggered deals
iTeos
→ EOS100850
→ High-potency A2A blocker
→ Paired with Keytruda
Arcus / Gilead
→ AB928 (etrumadenant)
→ Dual antagonist
→ Broad combo trials, GI focus
Incyte
→ INCB106385
→ Dual A2A/A2B
→ Strong myeloid remodeling
🧪 Tier 2: Enzymatic Blockers (CD39 / CD73)
AstraZeneca
→ Oleclumab
→ Anti-CD73
→ Targeting adenosine at the source
Innate Pharma
→ IPH5201
→ Anti-CD39
→ Partnered with AZ
Trishula Therapeutics
→ CD39/CD73 bispecifics
→ Dual upstream control
🔥 Tier 3: Myeloid & TME Modulators
Merck
→ G100
→ TLR4 agonist
→ Inflames tumor, lacks targeting
Portage Biotech
→ PORT-6 (A2A), PORT-7 (A2B)
→ Modular trial platform
Corvus Pharmaceuticals
→ CPI-444
→ A2A antagonist checkpoint strategy
Surface Oncology
→ Adenosine IL-27 platforms
→ Acquired by Coherus
🔥 The G100 Wake-Up Call: Fire With No Orders
In PEMBROSARC, Merck combined:
•G100 (TLR4 agonist)
•Keytruda (PD-1)
•Low-dose cyclophosphamide
The tumor inflamed.
T cells infiltrated.
PD-1 was blocked.
But the result?
❌ No consistent regression
❌ No survival improvement
❌ No durable immune memory
The immune system had been awakened, but not trained.
There was no mission. No antigen targeting. No memory formation.
The result was firepower with no direction.
That’s where DCVax changes everything.
🎯 DCVax: The Instruction Layer
Checkpoint inhibitors are brakes.
Adenosine blockers are shackles.
TLR agonists are sirens.
But DCVax is the brain.
🧬 How DCVax works:
• Tumor lysate is harvested from the patient
• Dendritic cells are isolated, matured ex vivo
• Tumor-specific antigens are loaded
• DCs are re-injected to train naïve and memory T cells
Result:
✔️ Immune precision
✔️ Systemic reach
✔️ Central and effector memory
✔️ Durable surveillance
DCVax doesn’t stimulate randomly.
It teaches who, what, and where to kill.
🧬 The Immune Stack, Built to Win
The future of cancer therapy is not single agents.
It’s stacked architecture, where every layer plays a coordinated role.
Here’s the ideal immune stack:
• DCVax
→ Targets tumor antigens with dendritic cell precision
→ Immune compass
• MK-1088 / AB928 / INCB106385
→ Blocks adenosine’s suppressive cage
→ Unlocks immune mobility
• Keytruda / PD-1 inhibitors
→ Prevents exhaustion, preserves killing power
→ Maintains engagement
• G100 or TLR agonists
→ Activates local immune flame
→ Draws cells into battle
With DCVax, the immune system becomes a trained strike force.
Without it, it’s just signal without aim.
—
🧱 What DCVax Unlocks That No Other Agent Can
✅ True Antigen Targeting
→ T cells trained on real tumor signatures, not shared motifs
✅ Systemic Immune Reach
→ Documented abscopal effects beyond injection site
✅ Long-Term Memory
→ Central and effector memory sustain tumor surveillance
✅ Coordination With Suppression Blockade
→ DCVax works upstream of A2A/A2B, not redundant, but essential
This isn’t just a vaccine.
It’s the immune OS.
🏛 SI 2025 No. 87: The Regulatory Framework That Changes Everything
The UK’s new law didn’t just reform approval.
It modularized it.
Think of SI 2025/87, enacted by the UK’s MHRA, as the cloud-based software update model for clinical trials:
• Approve the core (e.g., DCVax-L)
• Then add modules (adenosine inhibitors, checkpoints, TLRs) without full re-review
• IFR pathway allows real-world evidence integration
• Flaskworks enables decentralized, scalable manufacturing
• Trial designs, manufacturing units, even cohorts, can be swapped in/out without triggering a full reset
DCVax fits this future.
Others are still built for legacy systems.
🧩 Final Word
Merck has the parts:
• Checkpoint inhibition
• Adenosine blockade
• Myeloid and inflammatory tools
• Global cash and trial platforms
But not the instruction layer.
Arcus has combinatorial scale.
Incyte has myeloid modulation.
AstraZeneca has enzymatic blockade.
But no one else has:
❌ Patient-specific antigen targeting
❌ Pre-loaded, ex vivo–trained dendritic cell control
❌ Evidence of abscopal immunity and durable T-cell memory
DCVax doesn’t compete with their strategy.
It completes it.
And in this new regulatory, immunologic, and modular era, NWBO may already possess the most important component:
🧠 The compass.
🔓 The missing layer.
💡 The immune system’s command center.
The only question now is:
Will the industry recognize it before the field turns again?
📌 How SI 2025 No. 87 Enables Seamless Trial Upgrades, And Signals Where the U.S. Is Heading
Under the UK’s new regulatory statute (SI 2025 No. 87), trials are no longer rigid endpoints, they’re modular frameworks built to evolve.
If DCVax is already licensed or under IFR, adding an adenosine inhibitor (e.g. MK-1088, AB928, INCB106385) doesn’t require a restart.
Instead:
• ✅ Trial is amended, not reinitiated
• ✅ Only the new module is reviewed, not the entire trial
• ✅ Patients stay enrolled without delay
• ✅ Flaskworks manufacturing adapts instantly, no GMP resubmission
• ✅ MHRA and ethics review scoped to delta only (the change, not the whole design)
This transforms DCVax into a platform, where Merck, Arcus, or Incyte could simply plug in their agent and keep moving forward.
And this isn’t just a UK phenomenon.
📘 In the U.S., the FDA is inching toward similar modularity, especially under the Prasad–Macri accelerated approval voucher model, where high-impact therapies with platform potential may soon be rewarded with stackable, fast-track pathways and combinatorial flexibility.
What SI 2025/87 proves is this:
✅ Regulation can be fast
✅ Science can be modular
✅ Trials can evolve without collapse
This isn’t just a reform.
It’s the blueprint for immunotherapy in a post-static world.
🏷️ $MRK $ITOS $INCY $GILD $AZN $CRVS $SURF $RCUS $VSTM $IPHA $CGEN $PTGEF
#Immunotherapy #DCVax #CheckpointInhibitors #AdenosineTrap #DendriticCells #A2A #A2B
#CD73 #CD39 #CancerVaccine #CellTherapy #Flaskworks #GBM #AbscopalEffect #ImmuneStack
#TMEEscapePlan #MHRA #IFR #ModularApproval #ProjectOrbis #StackedOncology #BioPharma #DCVaxCompletesIt
1
5
40
3,255
21 Jun 2025
🔍 Thank you to @PeterDFetlow for surfacing this post. The timing and content are too important for $NWBO to overlook.
On June 20, Robert F. Kennedy Jr. introduced two new pillars of his health and biotech policy vision:
MAHA – Make America Healthy Again
MABA – Make American Biotech Accelerate
At first glance, this could read as campaign branding. But for those of us tracking the delayed deployment of personalized immunotherapies like DCVax, it is something else entirely — a signal that U.S. biotech reform is entering the national agenda.
🧬 This is not about future innovation. It is about access to therapies that already exist.
DCVax-L, developed by Northwest Biotherapeutics, is an autologous dendritic cell vaccine. It uses a patient’s own white blood cells to train the immune system to recognize and attack glioblastoma tumor tissue. Results from its Phase 3 trial were published in JAMA Oncology, showing extended survival in a subset of patients far beyond the standard of care.
It is not toxic
It does not suppress the immune system
It is manufactured one patient at a time
It has already shown durable survival beyond five years in a historically fatal cancer
Yet despite this, DCVax-L remains unapproved by the U.S. Food and Drug Administration (FDA).
Why? Because the current regulatory model was not designed to accommodate decentralized, immune-based, individualized therapies like this one.
🇬🇧 The United Kingdom has already acted
On June 17, the UK’s Department of Health enacted a landmark reform:
SI 2025 No. 87 – The Human Medicines (Medical Devices and Medicinal Products) (Amendment) Regulations 2025
This law:
Enables hospital-based manufacturing for advanced therapies
Supports risk-adapted approvals based on real-world data
Aligns with local GMP standards and site-level quality control
Was designed with platforms like Flaskworks EDEN in mind
On July 23, the Medicines and Healthcare products Regulatory Agency (MHRA) will complete the full rollout of this system. That includes revised submission portals, regulatory guidance, and support structures for Advanced Therapy Medicinal Products (ATMPs).
DCVax and Flaskworks are now functionally compatible with this model. The system already exists just not yet in the United States.
🚀 This is the second moonshot and this time it is focused on survival
When Kennedy says, “we’re going to do it again,” it echoes the spirit of Operation Warp Speed, which accelerated vaccine timelines through coordinated funding and regulatory streamlining.
But this time the goal is different. This moonshot is about:
Empowering the immune system to defeat solid tumors
Delivering therapies from hospital-based manufacturing within days
Eliminating the toxicity and systemic damage of conventional chemotherapy
Reducing cost by automating sterile, modular production
Using real-world survival outcomes as a valid regulatory endpoint
DCVax is already doing this.
It is the case study for what a post-blockbuster, post-chemo immune therapy ecosystem could look like.
📣 MABA is not a slogan. It is a strategic direction
Kennedy’s message points toward regulatory realignment. One that favors:
Real-world evidence (RWE) instead of prolonged placebo-controlled trials in terminal patients
Rolling review of personalized biologics
Named Patient and Individual Funding Request (IFR) pathways for early access
Hospital-aligned manufacturing instead of billion-dollar centralized facilities
This is already happening in the UK. The MHRA has integrated these mechanisms into its national system. What Kennedy is proposing is to make sure U.S. regulators do not fall further behind.
💡 DCVax is the example, not the exception
Developed in the U.S.
Manufactured in GMP-certified facilities in the UK
No toxicity, no immune collapse, no long-term dependency
Compatible with NHS delivery infrastructure
Already supported by an automated production system through Flaskworks
DCVax is ready.
The system to deploy it exists.
The question now is whether the U.S. is prepared to follow through — or watch its own discovery go live somewhere else.
📆 Timing that matters
✅ June 17 – UK law comes into force
🎗️ July 16 – Glioblastoma Awareness Day
🛠️ July 23 – MHRA launches full operational rollout
📣 June 20 – MAHA and MABA are introduced in U.S. biotech discourse
This is not coincidence.
It is convergence.
And it places DCVax and the patients it could help in the center of a critical moment.
📍 Final Thought
You do not have to support Robert F. Kennedy Jr. politically to see the urgency behind what he pointed to.
This is not about partisan lines. It is about regulatory barriers that continue to delay access to therapies that are already proven, already built, and already saving lives abroad.
Patients with aggressive cancers are not asking for slogans. They are asking for time, and for the chance to receive treatments that match the sophistication of the science we already possess.
Flaskworks has built the platform.
The UK has passed the law.
The clinical data has been published.
The only thing left is for the U.S. to align policy with possibility.
That is not a political position. That is a human one.
And if this message helps move that conversation forward, then every patient still waiting has reason to hope.
#DCVax #NWBO #Flaskworks #MAHA #MABA #GBM #celltherapy #immunotherapy #biotech #patientsfirst #MHRA #FDA #ProjectOrbis #Moonshot2 #SurvivalIsTheEndpoint
20 Jun 2025

The mission to Make America Healthy Again (MAHA) includes MABA — Make American Biotech Accelerate.
President Trump showed in his first term what happens when you unlock American science — breakthroughs happen fast.
Now, we’re going to do it again.
We know the power of U.S. biotech. It’s time to let it flourish — not tie it up in red tape, misalignment, and a process that gives the edge to foreign interests and large incumbents.
We’re clearing the path to transform great science into real cures, at lower costs, and better health for the American people. Life science and biotech are at the heart of that!
#MAHA #MABA
2
2
36
2,495
20 Jun 2025
$NWBO 🧬The Signal Before the Switch: Why July 16 Matters More Than It Seems
How Glioblastoma Awareness Day Aligns with DCVax-L’s Imminent Moment
On June 19, 2025, the U.S. Senate passed a bipartisan resolution officially declaring July 16, 2025 as National Glioblastoma Awareness Day, a day meant to honor patients, catalyze research, and spotlight one of the deadliest forms of brain cancer. The move was emotional and personal. Senators invoked names like Ted Kennedy, John McCain, and Bobbi Barrasso, underscoring the disease’s indiscriminate devastation. But timing isn’t accidental in Washington, and the resonance of this resolution may be more than commemorative, it may be a regulatory drumroll.
Behind this national gesture lies something deeper: a signal to the scientific and investment community that something transformative is already in motion.
🧠 Why Now? Why Glioblastoma?
The glioblastoma community has waited decades for progress. Traditional chemoradiation has plateaued, temozolomide offers modest extension, and immunotherapy has lagged in efficacy, until now. Behind closed doors, a platform called DCVax-L has spent the last year quietly navigating final regulatory integration in the UK, real-world rollout, and infrastructure activation through Project Orbis, SI 2025 No. 87, and the new risk-proportionate ATMP law. Meanwhile, the MHRA and NICE have modernized their systems specifically to handle personalized cell therapies at scale.
The U.S. Senate’s move comes just one month after the UK’s regulatory overhaul went live on June 17, an overhaul built to support commercial deployment of autologous therapies like DCVax-L via decentralized production (e.g. Flaskworks EDEN units) and site certification.
Coincidence? Unlikely.
🇬🇧 What Happened in the UK and Why It Matters Globally
DCVax-L’s GMP factory at Sawston is operational and MHRA-inspected.
EDEN closed-system production from Flaskworks has been validated in internal documentation and patents, with MHRA’s new law permitting point-of-care delivery.
MHRA’s “SI 2025 No. 87” came into force on June 17, making hospital-based manufacturing and efficacy-based reimbursement frameworks lawful across the UK.
DIA Global Annual Meeting (June 16–20) featured Project Orbis sessions, MHRA’s Lawrence Tallon keynote, and Dr. Marnix Bosch’s NYAS talk, laying the final tracks publicly.
This trifecta, factory readiness, legal infrastructure, and scientific validation, forms the invisible spine behind the Senate’s announcement.
🔁 The Historical Loop Closes: John McCain and the Vaccine That Wasn’t Ready, Then
Senator John McCain’s passing from glioblastoma in 2018 was a galvanizing moment for the nation. What the public didn’t know then is that he may have qualified for DCVax-L’s “compassionate use” program, but the infrastructure wasn’t in place. Manufacturing was centralized, regulations were outdated, and enrollment windows were narrow.
Today, that’s changed. If John McCain were diagnosed now, he could:
Walk into a certified NHS hospital.
Have blood drawn and processed on-site.
Receive a personalized vaccine made in days, not weeks.
Avoid shipping delays, import complications, and time lost.
The system that wasn’t ready for him then, is ready for others now.
🧩 DCVax-L, Already Deployed? Follow the Real Clues
Several signals suggest DCVax-L isn’t waiting for a theoretical approval, it’s already in deployment-prep mode:
IFR expansion quietly underway in the UK, consistent with a behind-the-scenes approval.
A full NICE health technology assessment nearly complete, an effort only triggered for therapies nearing commercial rollout.
Ongoing supply chain validation, including Charles River collaboration and training tied to Flaskworks deployment.
Linda Powers’ strategic silence hints at a prelude to scale, not a pause.
Meanwhile, U.S. activity has deliberately slowed, possibly awaiting MHRA confirmation before a Project Orbis cascade.
📅 So Why July 16?
In military terms, this isn’t a celebration, it’s signal intelligence. You don’t get this many senators, across party lines, invoking personal stories unless something is set to move.
And July 16 is:
Exactly one month after MHRA’s law went live.
A possible public unveiling point, using a day of solemn national focus to prepare for a therapeutic shift.
The ideal moment to anchor media coverage of a new standard of care, one not just tied to a drug, but to an entirely new infrastructure for personalized medicine.
If DCVax-L were to be announced, approved, or deployed, July 16 would be the moment of maximal clarity and resonance. It would be the day the promise and infrastructure of cell therapy finally meet the patients who need it most.
In short:
This is no mere resolution. It’s the overture to a global therapeutic transition.
$NWBO | #DCVax | #Glioblastoma | #CellTherapy | #Flaskworks | #ProjectOrbis | #MHRA | #NICE | #ATMP | #BrainCancer | #Immunotherapy | #PrecisionMedicine | #Sawston | #GlioblastomaAwareness | #BioPharma | #HealthcareInnovation | #CureGBM | #FDA | #Oncology | #CancerResearch
Special thanks to @Kelly712717541

20 Jun 2025

The US Senate designates July 16, 2025, as Glioblastoma Awareness Day to encourage research and honor those affected.
Source: Hoodline $nwbo share.google/W6gbp6zfhyAjJfY…
3
9
59
3,060
13 Jun 2025
Totally fair, under normal conditions, TA doesn’t mean much on a stock like $NWBO.
But this week isn’t normal. It’s a sundae.
Here’s the full scoop:
🍨 Scoop 1: June 16
– DIA Global Meeting kicks off
– FDA, MHRA, and EMA on stage
– MHRA’s new ATMP rules officially go live
🍦 Scoop 2: June 16–17
– Dr. Bosch presents on next-gen DCVax at NYAS
– Flaskworks-style decentralized manufacturing becomes real-time viable
– Real-world infrastructure quietly switches on
🍫 Hot Fudge Layer
– Project Orbis workshops underway
– Global regulator coordination intensifies
🍪 Sprinkle Crunch
– UK submission already in
– U.S. BLA may already be filed
– Regulatory silence signals alignment
🍒 And the Cherry on Top?
– A golden cross may trigger Monday
– 50-day MA is closing in on the 200-day
– First technical reversal signal in years, as fundamentals align
And just to ground it in leadership?
According to someone who was with her after the last NY presentation, Linda Powers said:
“I’ll never allow this company to ever be this vulnerable again.”
So no, this chart doesn’t stand alone.
But when sentiment, structure, and system all align?
That’s not just a cherry on top.
That’s the whole sundae coming together at the perfect scoop.
$NWBO #DCVax #QuietActivation #GoldenCross #Flaskworks #ATMP #FDA #MHRA #ProjectOrbis
1
30
26,243
13 Jun 2025
🤯What If… NWBO Already Filed a BLA?
Episode Two: The Review Clock Is Already Ticking
Let’s say the quiet part out loud.
NWBO has:
A completed, FDA-cleared Phase 3 trial
A peer-reviewed publication in JAMA Oncology
A full regulatory package submitted to the UK’s MHRA
An automated, closed-system manufacturing solution (Flaskworks)
An active U.S. IND, and possibly a U.S. BLA already filed
So the next question becomes:
🎯If NWBO has already filed a BLA with the FDA, what are the chances they’d be approved quickly, given the current regulatory environment?
The answer:
Much higher than in any prior regulatory era, especially for a product like DCVax-L.
Let’s walk through why.
🧭 1. The FDA is actively modernizing, now, not later
Dr. Marty Makary’s CEO Forums (including the June 12 meeting at Stanford) are built around:
Accelerating biologics approvals
Streamlining pathways for cell-based and personalized therapies
Fixing bottlenecks in regulatory review
Listening to companies with active INDs, NDAs, or BLAs i.e., those currently in the system
This is the regulatory environment DCVax-L was waiting for, and now it’s here.
💊 2. DCVax-L’s clinical and safety profile is exceptional
No serious treatment-related adverse events were reported in its 331-patient Phase 3 trial
48- and 60-month survival data showed durable benefit
Peer-reviewed by independent statisticians and published in JAMA Oncology (2022)
For an oncology biologic, this kind of clean safety record is rare, and it reduces the review risk dramatically.
🧬 3. The trial was FDA-compliant from the start
The Phase 3 study was conducted under a U.S. IND approved by the FDA. That means:
Protocol design was cleared in advance
Endpoints were pre-specified
U.S. sites enrolled and monitored under FDA oversight
So the FDA has already reviewed and accepted the basic scientific structure of the program.
⚙️ 4. Flaskworks solves a big problem, scalability
The biggest challenge in cell therapy approvals isn’t efficacy, it’s manufacturing.
But NWBO owns Flaskworks, whose Eden system provides:
Closed, automated dendritic cell production
Digital batch traceability
Standardized QA/QC under GMP conditions
Support for decentralized manufacturing at scale
This is exactly what the FDA has been asking for in the next wave of ATMPs (Advanced Therapy Medicinal Products).
🌍 5. Global regulatory coordination is happening now
MHRA’s SI 2025/87 framework officially activates in June 2025
Project Orbis is expanding to include biologics and advanced therapies
On June 16, FDA, MHRA, and EMA leadership appear together at DIA Global
NWBO’s application is already under review in the UK
Dr. Bosch is presenting at NYAS on next-generation DC platforms on the same day
If NWBO filed with the FDA, the BLA could now be under review while global regulators quietly coordinate.
📊 So What Typically Delays BLAs, and Does It Apply Here?
Let’s examine the common causes of delay… vertically:
1. Safety Concerns
❌ Not applicable
📌 DCVax-L has an extraordinary safety record for a cancer therapy
2. Trial Design or Endpoint Issues
❌ Not applicable
📌 Conducted under FDA IND; endpoints were prespecified and published
3. Manufacturing (CMC) Deficiencies
⚠️ Sometimes, but Flaskworks may resolve this
📌 Flaskworks enables closed, reproducible, digitally traceable manufacturing
📌 Could preempt many CMC-related delays
4. Small Patient Population
✅ Applies, but could accelerate review
📌 GBM is rare and deadly
📌 Fits Fast Track, RMAT, and Real-World Evidence criteria
5. Lack of Global Review Coordination
❌ Not applicable
📌 MHRA application is already in process
📌 Orbis-style alignment is already happening in real time
🧠 Summary:
This isn’t a hypothetical pipeline product.
This is a therapy with real-world data, clean safety, scalable manufacturing, and international regulatory traction.
If NWBO submitted a complete BLA sometime between February and May 2025, and didn’t announce it (which is legal and common) the FDA could already be 30 to 60 days into their review.
And the June 12 CEO Forum?
That may not have been a networking event.
It may have been a strategic signal meeting for companies already under the microscope.
🔮 Expert Outlook:
Given:
➡️The current FDA posture
➡️The safety and survival profile
➡️Manufacturing readiness
➡️Global regulatory momentum
➡️And NWBO’s eligibility for Fast Track, RWE pathways, or even an Orbis-style review
If they filed… yes, they could be approved faster than most realize.
And if so?
What’s coming Monday wouldn’t be the beginning.
It would be the first time the lights flicker above ground.
$NWBO #DCVax #Flaskworks #QuietActivation #BLA #FDA #MHRA #ProjectOrbis #ATMP #Immunotherapy
1
1
18
990
13 Jun 2025
If you’ve been asking whether $NWBO could’ve already filed a BLA with the FDA, and just kept it quiet, the answer is: yes. Not only is it possible, there are multiple signs pointing in that direction.
Here’s the breakdown:
1. Completed Phase 3 Trial
✅ Confirmed
📌 Filing prerequisite is done
2. Peer-Reviewed Clinical Data
✅ Published in JAMA Oncology (2022)
📌 Supports safety and efficacy claims
3. Full Dossier Submitted to MHRA
✅ Confirmed (Dec 2023)
📌 Same data used for U.S. BLA prep
4. Flaskworks Manufacturing System in Place
✅ Confirmed
📌 Matches FDA’s new push for decentralized, automated platforms
5. No BLA Announcement (Yet)
❓ No disclosure, but not required
📌 Companies often wait until acceptance before announcing
6. Eligible for the FDA CEO Forum (IND on file)
✅ Confirmed
📌 Would’ve had standing to be invited, possibly more
7. Perfect Timing With DIA, MHRA, Orbis
✅ All converging June 16–18
📌 BLA review or filing may already be in motion
All of this adds up to one thing:
🧠 There’s no regulatory reason they couldn’t have filed.
And no legal reason they’d have to tell us right away.
So if they did… we may not know until the FDA responds.
$NWBO #DCVax #BLA #Flaskworks #ATMP #QuietActivation #MHRA #ProjectOrbis #Immunotherapy
3
2
30
3,706
13 Jun 2025
🌀What If… $NWBO Was in the Room?
Episode One: The Quiet Briefing
On June 12, FDA Commissioner Dr. Marty Makary hosted a closed-door CEO Forum at Stanford with a select group of pharma and biotech executives.
No livestream.
No transcript.
No public attendee list.
This wasn’t for show.
This forum was part of the FDA’s National Listening Tour, but only for companies that met very specific, high-level prerequisites. To even be considered for an invitation, companies had to have:
➡️At least one active IND, NDA, or BLA on file with the FDA
➡️A therapy in active regulatory review or development
A CEO (or senior R&D/medical officer) available to attend
➡️And most importantly: they had to be hand-picked by the FDA after applying
Each company could only attend one forum nationwide. Capacity was strictly limited. This was not open to media, analysts, or even other agency officials not directly involved in biologics and advanced therapy policy.
This was a filter.
And a very deliberate one.
Only companies with live, high-stakes regulatory activity were allowed in.
🧠 What’s an IND? A BLA?
An IND (Investigational New Drug application) allows a company to start clinical trials in humans. It’s step one, your ticket into the system.
A BLA (Biologics License Application) is the final step. It’s what a company submits to request full approval to sell a biologic treatment in the U.S. That includes:
All the clinical data proving the therapy is safe and effective
Details about the manufacturing process
Quality control, distribution, and patient safety plans
You can think of the BLA like your final exam. If it’s approved, you’re allowed to go to market.
🧭 So What Was This Forum?
It was a strategic alignment session, under the radar.
The FDA says the goal was to get direct input from biotech and pharma leadership on how to modernize the regulatory process, particularly for biologics and advanced personalized therapies that don’t fit old models.
Why now?
Because three days later, on Monday, June 16, Dr. Makary will open the DIA Global Meeting alongside MHRA and EMA leadership, just as:
The UK’s new regulatory framework for advanced therapies (SI 2025/87) goes live
The global cell and gene therapy community convenes under Project Orbis
And Dr. Marnix Bosch of Northwest Biotherapeutics presents at NYAS on next-gen dendritic cell platforms
This isn’t routine scheduling. It’s coordinated motion.
🔍 Could NWBO Have Been There?
We don’t know for sure. The attendee list wasn’t public. But here’s what we do know:
✅ NWBO has an active IND for DCVax-L in the U.S.
✅ They’ve completed their Phase 3 trial and published survival data
✅ They’ve submitted a full application to the MHRA in the UK
✅ They haven’t publicly confirmed a BLA filing in the U.S.—but companies aren’t required to disclose one until they choose
✅ Their product is exactly the type of personalized biologic the FDA is actively trying to create new pathways for
✅ Their automation system (Flaskworks) aligns perfectly with FDA’s push toward scalable, decentralized, and digitally traceable manufacturing
Most importantly:
They meet the FDA’s eligibility criteria to be in that room.
And they fit the mission of what the room was built to address.
💡 What Would That Mean?
It means:
The conversation may have included therapies like DCVax-L, safe, proven, but bottlenecked
It may have included companies preparing for ATMP scaling under new frameworks like SI 2025/87
It may have touched on Flaskworks-type platforms designed to unlock decentralized manufacturing at commercial scale
It could have laid the groundwork for harmonized approvals across U.S., UK, and EU agencies under Project Orbis
And if NWBO was present, they may have walked away not with speculation, but with clarity, coordination, and a signalon what’s coming next.
🎬 Closing Scene
No one outside the room knows exactly who was in it.
But we know:
Who could qualify
What was discussed
When it happened
And how tightly it connects to the events coming Monday
We can’t say NWBO was there. But we can say they have every reason to be.
And if they were…
Then June 16 isn’t the beginning of something.
It’s a continuation of something that’s already underway.
#DCVax #Flaskworks #BLA #ATMP #QuietActivation #FDA #MHRA #ProjectOrbis #Immunotherapy
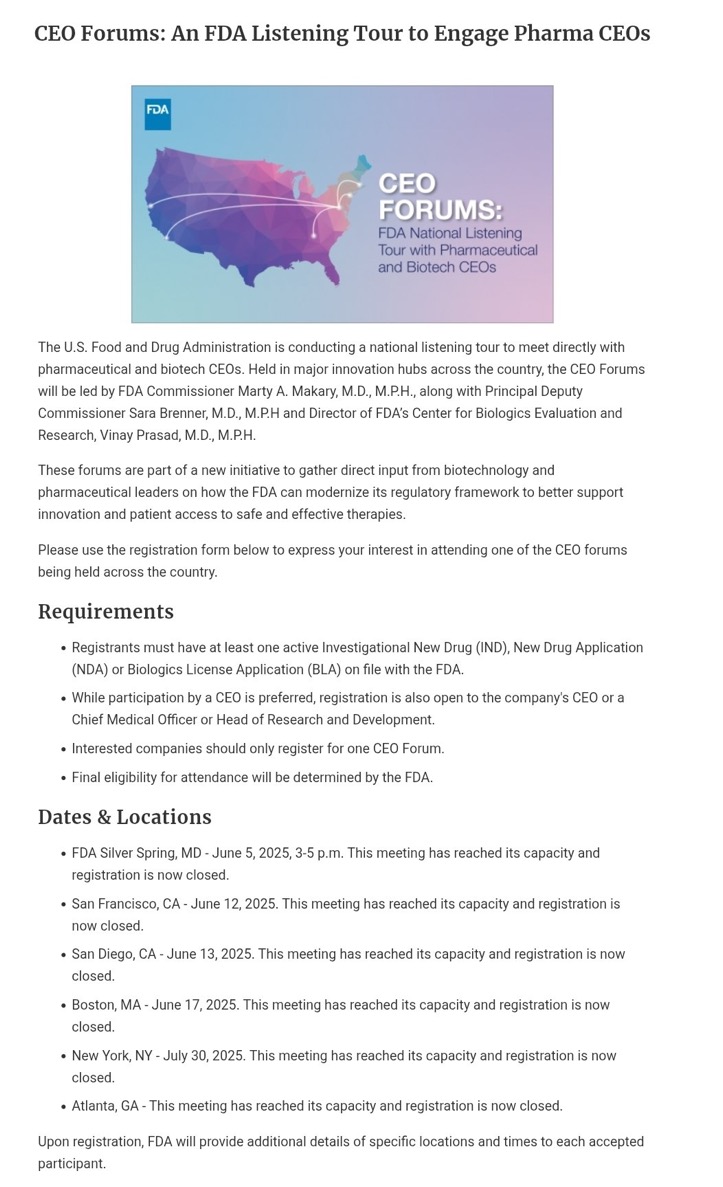
13 Jun 2025

Agree, you don’t pull in pharma CEOs on a Thursday, then open a global cell therapy summit on Monday, just as new rules go live, unless...
2
7
48
3,548
13 Jun 2025
$NWBO The Quiet Evolution of DCVax: What UCLA Just Confirmed Without Saying
UCLA just released a major update on their brain cancer research, and if you’ve been following the science behind DCVax, what’s buried in that update speaks louder than anything on the surface.
Let’s start here: the dendritic cell vaccine UCLA uses in their program is called ATL DC. It doesn’t carry the DCVax name, but it’s built on the same backbone. Same inventors. Same tumor lysate process. Same dendritic cell prep. It’s the academic version of what became DCVax-L.
And back in 2021, UCLA published results in Nature Communications showing that pairing ATL DC with poly ICLC (Hiltonol) led to stronger T cell responses, no major safety issues, and longer survival. That was the signal that the immune system could be trained and amplified in glioblastoma, even in late-stage, high-risk patients.
So what’s new now?
This time, it’s not about showing it works. It’s about explaining why it works and what comes next. UCLA’s latest publication doesn’t just confirm the benefit of poly ICLC—it begins to unpack the mechanism. They’re seeing enhanced interferon signaling, deeper immune activation, and more precise dendritic cell engagement. That matters.
Why? Because that level of mechanistic validation is what transforms a promising concept into a platform ready for scale.
Even more important is the timing.
They’re not publishing this in isolation. They’re showing ATL DC plus Hiltonol alongside:
•Forskolin paired with radiation to reprogram tumor cells into non-dividing states
•Endocan inhibition to shut down blood vessel-driven resistance
•BCL XL targeting to suppress glioma survival pathways
•Organoid modeling to predict resistance and personalize treatment in real time
That’s not a list of siloed studies. It’s a blueprint for system-layered therapy. Each element reflects a shift away from monotherapy thinking toward integrated, adaptive care. And that’s the world DCVax was designed for.
It also tells us something else: this isn’t about one trial anymore. It’s about infrastructure.
Since the 2021 study, the environment around this vaccine has changed completely. Now you have:
•Flaskworks automation for closed-system cell therapy manufacturing
•New MHRA regulations (SI 2025 87) that support decentralized delivery
•Project Orbis gaining traction for global coordination
•And a week ahead where all these pieces converge
From June 16 to 18:
•Lawrence Tallon (MHRA CEO) delivers a keynote on advanced therapy reform
•The DIA global Project Orbis session goes live
•Dr. Bosch presents at NYAS on next-gen dendritic cell vaccines
•And the new UK regulatory framework for ATMPs officially comes online
None of this is random. UCLA’s research is landing right before a regulatory window opens. Their trials are quietly expanding. And the same foundational vaccine, once seen as too complex, is now sitting at the center of a modular, immune-guided, policy-supported future.
This isn’t a product launch. It’s a transition.
The vaccine hasn’t changed. But the world around it has.
ATL DC is DCVax. And the Quiet Activation isn’t coming—it’s already underway.
#DCVax #ATLDC #Hiltonol #GBM #Immunotherapy #MHRA #ProjectOrbis #Flaskworks #NeuroOncology #CancerVaccine $NWBO #QuietActivation #BrainCancer #DendriticCells #UCLA
13 Jun 2025

#dcvax $nwbo #gbm
Inside the Latest Research Advancements to Help Combat Brain Cancer :
Investigators at the UCLA Health Jonsson Comprehensive Cancer Center are developing new strategies to better understand and treat one of the most challenging forms of cancer.
“While glioblastoma remains a formidable challenge, these breakthroughs, which include novel combination therapies, next-generation organoid models, precision medicine strategies, and first-in-human vaccine trials, bring real hope,” said Dr. Linda Liau, chair of neurosurgery at the David Geffen School of Medicine at UCLA and director of the UCLA Brain Tumor Program. “Each new discovery gets us closer to improving survival and quality of life for patients facing this devastating disease.”
Newswise — Brain cancer remains one of the most difficult forms of cancer to treat, but researchers at the UCLA Health Jonsson Comprehensive Cancer Center are making meaningful strides to change that. From reprogramming cancer cells to uncovering hidden mechanisms of resistance, UCLA scientists are pursuing a wide range of approaches to attack glioblastoma and other deadly brain tumors.
The need for more effective treatments for brain tumors like glioblastoma is imperative. The average lifespan of someone diagnosed with glioblastoma is just 12 to 15 months, and only about 5% of people diagnosed with the disease are alive five years after their diagnosis.
“While glioblastoma remains a formidable challenge, these breakthroughs, which include novel combination therapies, next-generation organoid models, precision medicine strategies, and first-in-human vaccine trials, bring real hope,” said Dr. Linda Liau, chair of neurosurgery at the David Geffen School of Medicine at UCLA and director of the UCLA Brain Tumor Program. “Each new discovery gets us closer to improving survival and quality of life for patients facing this devastating disease.”
Here’s a look at some of the most recent discoveries that are helping to advance more effective and targeted treatment strategies for glioblastoma and other aggressive brain cancers:
Reprogramming brain cancer cells to halt tumor growth
Dr. Frank Pajonk, professor of radiation oncology at the David Geffen School of Medicine at UCLA, and his laboratory have developed a promising new treatment strategy to treat glioblastoma by combining radiation therapy with a plant-derived compound called forskolin. Radiation alone is known to kill many cancer cells, but it can also temporarily make glioblastoma stem cells more flexible, or adaptable, providing an opportunity to alter their identity. The team discovered that by timing the delivery of forskolin during this window, they could push these adaptable cancer cells to become neuron-like or microglia-like that don’t divide uncontrollably or regenerate tumors. This reprogramming approach effectively halts the cancer’s ability to grow and spread. An early-stage study found when tested in mice, the addition of forskolin to radiation significantly slowed tumor growth in mice and, in some cases, led to long-term tumor control.
Insight into how blood vessel-tumor interactions fuel glioblastoma can help lead to new treatment strategies
A newly identified protein called endocan, produced by blood vessel cells in brain tumors, may be a key driver of glioblastoma growth and treatment resistance. In a recent study, a team of researchers, led by Dr. Harley Kornblum, director of the UCLA Intellectual and Developmental Research Center and professor of psychiatry, pediatrics and molecular and medical pharmacology, found that endocan activates the PDGFRA receptor on tumor cells, helping the cancer thrive and resist radiation therapy. By blocking this interaction with the drug ponatinib, they were able to slow tumor growth and improve radiation response in lab models. The findings highlight endocan’s role in shaping the tumor’s invasive edges, areas that often survive surgery, and suggest that targeting this protein could lead to more effective treatments for this aggressive and deadly brain cancer.
Combining genetic and functional profiling to predict glioblastoma treatment response
In a recent study, scientist Dr. David Nathanson, professor of molecular and medical pharmacology, and his team developed a new approach that combines genetic and functional profiling to better predict how glioblastoma responds to treatment. By analyzing both a tumor’s DNA and how its cells react to therapies in real time, the team identified a protein called BCL-XL as a key player in helping cancer cells evade death. Using this insight, they tested a drug called ABBV-155 that targets BCL-XL and found it significantly shrank tumors in lab models when paired with standard treatments. This precision medicine strategy could lead to more effective, personalized therapies for glioblastoma patients.
A personalized cancer vaccine to tackle aggressive brain tumors in adolescents and young adults
In an effort to combat one of the most lethal forms of pediatric brain cancer, a team of researchers led by Dr. Anthony Wang, director of the Pediatric Brain Tumor Program at UCLA Health, launched a first-of-its-kind clinical trial to evaluate the safety and effectiveness of a cancer vaccine targeting H3 G34-mutant diffuse hemispheric glioma, a highly aggressive brain tumor that is typically found in adolescents and young adults. The vaccine uses the patient’s own dendritic cells to target tumor-specific neoantigens caused by disrupted RNA regulation. The goal is to train the immune system to recognize and destroy cancer cells more effectively. Researchers hope the approach will improve survival and lead to more precise, immune-based treatments for this challenging disease.
Immune-boosting agent supercharges personalized vaccine
A team of researchers led by Liau and Dr. Robert Prins, professor of neurosurgery and of molecular and medical pharmacology, found that combining a dendritic cell cancer vaccine with poly-ICLC, an immune-stimulating agent, significantly enhances the immune response in patients with malignant glioma, a fast-growing and hard-to-treat brain tumor. In a clinical study, patients receiving the combination therapy showed stronger T cell activity and increased interferon response, improving the dendritic cells’ ability to fight the brain tumor more effectively than the vaccine alone. The findings suggest that poly-ICLC may boost the vaccine’s potency and offer a promising new strategy for treating gliomas. A new clinical trial is already underway to explore this combination further.
Using organoids to uncover the mechanisms behind treatment resistance in glioblastoma
UCLA researchers Dr. Aparna Bhaduri, assistant professor of medicine and biological chemistry, and Dr. Kunal Patel, assistant professor of neurosurgery, are developing advanced brain organoid models, which are model versions of the human brain grown in a lab dish, to better understand how glioblastoma develops and spreads. By implanting tumor samples into stem cell-derived organoids that closely mimic the human brain, the team is studying how different cell types within the tumor interact with their environment. This approach aims to uncover the lineage and evolution of glioblastoma cells and identify new strategies to disrupt tumor growth and improve treatment outcomes.
newswise.com/articles/inside…
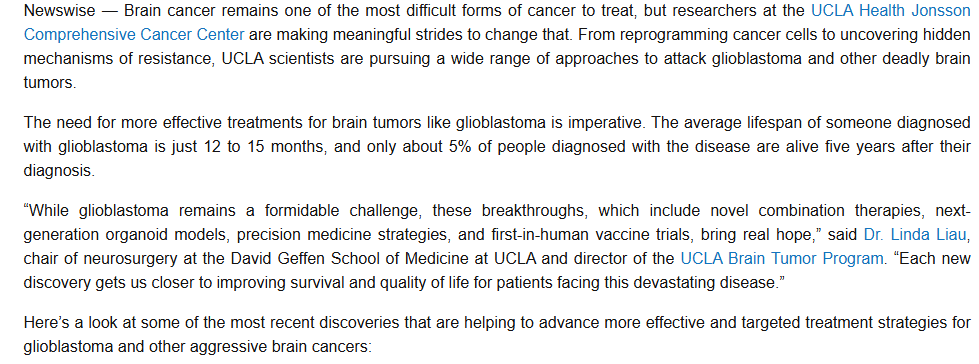

1
10
81
4,888
6 Jun 2025
🌟 Goldilocks Immunotherapy: A Direct Answer to HHS’s Call for Innovation $NWBO
👇 Responding to @BioSpace’s post on HHS Secretary Kennedy’s intent to eliminate barriers for rare disease drugs:
When the U.S. Health Secretary signals it’s time to fast-track novel therapies, it’s worth spotlighting a platform already battle-tested, scalable, and sitting at the sweet spot of safety and efficacy.
DCVax-L is that Goldilocks solution in immune-oncology:
❌ Checkpoint inhibitors alone? Too hot.
— Risk autoimmune storm. Limited in GBM and other cold tumors.
❌ CAR-T for solid tumors? Too cold.
— Brilliant in hematologic cancers, but ineffective and logistically impractical for most solid tumors.
✅ DCVax-L? Just right.
— Patient-specific dendritic cell vaccine.
— Naturally primes immune memory and adaptive T-cell response.
— Safe, non-toxic.
— In the Phase 2 trial published in Nature Communications, over 60% of newly diagnosed glioblastoma patients receiving DCVax-L were alive at three years.
— This was achieved without any checkpoint inhibitors, IL-7, IL-2, oncolytic viruses, or other synergistic agents.
This isn’t about forcing immune activation—it’s immune precision.
Where others crash the gates, DCVax harmonizes the symphony.
And with Flaskworks’ patented automation, this isn’t just science. It’s infrastructure. The platform is ready to scale, ready to license, and built for regulatory acceleration.
If this is what HHS says it wants, there’s no reason to delay support. DCVax-L is already showing the kind of sustained tumor immune suppression that many hoped was possible, and this is just the beginning.
#Immunotherapy #CancerVaccine #RareDisease #GBM #CellTherapy #DCVax #Flaskworks #FDA #ProjectOrbis #PersonalizedMedicine #Biopharma #CheckpointInhibitors #CAR_T #Innovation #Oncology #HHS

In a roundtable event on Thursday, HHS Secretary Robert F. Kennedy Jr. said his office will work to eliminate barriers that keep cell and gene therapies from the market.
#regulatory #celltherapy #biospace
hubs.li/Q03r1rvD0
6
38
3,835
14 May 2025
…. Continued
$NWBO
6. Commercial Readiness and Economic Case
Murcidencel is not only more cost-effective than chronic biologics like Keytruda, but it’s safer, more targeted, and potentially curative. Combined with Flaskworks’ automation, NWBO can deliver this therapy with:
•Lower per-patient costs
•Faster turnaround times
•Higher profit margins than most cell therapies, including CAR-Ts
This gives NWBO leverage for payer negotiations, international licensing, and pipeline expansion into other solid tumors.
⸻
Conclusion: NWBO Has the Asset, the Infrastructure, and the Advantage of Time
Murcidencel isn’t a concept—it’s a regulator-submitted, clinically validated therapy with global patent protection, commercial-scale manufacturing, and proven impact in one of the deadliest cancers. The doubts, noise, and FUD fall apart under scrutiny.
NWBO has the product, the platform, the patents, and the plan—and more importantly, it holds the gateway. As the world wakes up to the promise of dendritic cell immunotherapy, it will find that NWBO is already there—leading the way.
#Murcidencel #DCVax #EndGlioblastoma #BrainCancerAwareness #GBM #CancerBreakthrough #CellTherapy #DendriticCellVaccine #Flaskworks #Immunotherapy #PersonalizedMedicine #MHRA #ProjectOrbis #Biotech #SmallCapStocks #HealthcareInnovation #OncologyInvesting #CancerStocks
2
1
16
578
1 May 2025
$NWBO #DCVax AKA murciden-CEL is next!
#BrainTumorAwareness #GlioblastomaAwareness #BrainTumorAlliance #NBTS #HeadForTheCure #GreyMay #GoGrayInMay #BTAM #DefeatGBM #BrainTumorResearch #FDA #MHRA #HealthCanada #TGA #Swissmedic #ANVISA #HSA #PMDA #MedSafe #IsraeliMOH #ProjectOrbis
1 May 2025

Fantastic news for this company and especially the patients. Knowing some of the scientists, I want to give tremendous kudos to them. Was a difficult battle. Anyway, it bodes terribly well for $NWBO. The FDA is moving quicker to approve cell therapies. Think hard on that!
22
702