Hercules 55 retweeted

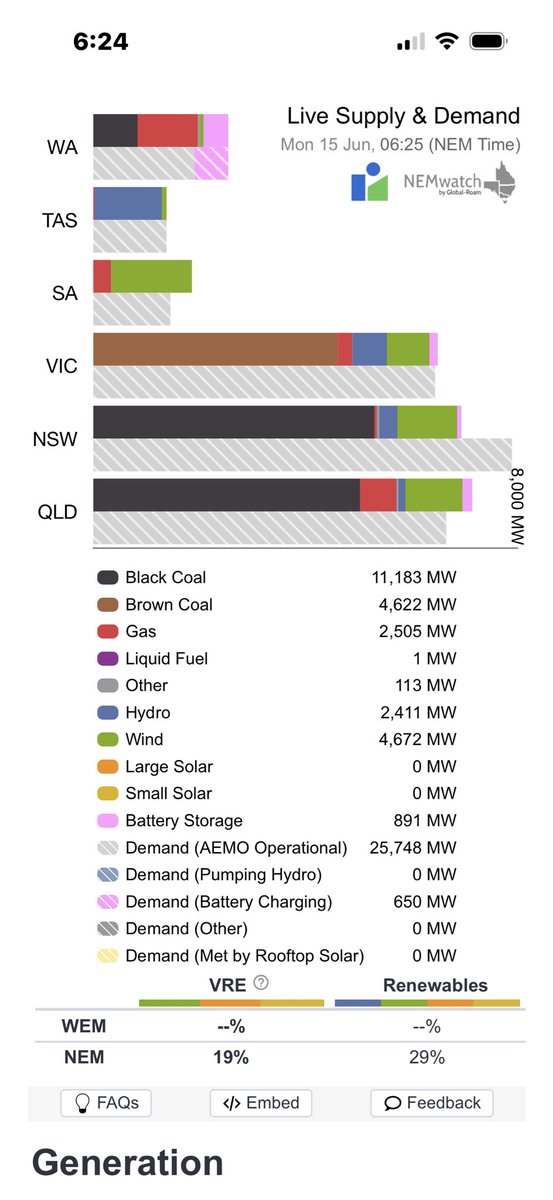
Good morning Australia 6-25 am AEST 15 June 2026
Variable renewable energy is not supplying 81.62% of your current electricity needs ( 26.63 GW )
@AlboMP @PMalinauskasMP @LilyDAmbrosioMP #auspol
3
23
56
231

La loi peut être, mais l'exigence d'assimilation à la France voudrait qu'une mahométane dans un conseil municipal ne se bâche pas ainsi de la tête aux pieds. Le problème est que ça ne lui traverse pas l'esprit ! 🤔
Ou la laïcité à géométrie variable des mairies communistes... 🙃

2
ZalinskySilverworks retweeted

Jun 13
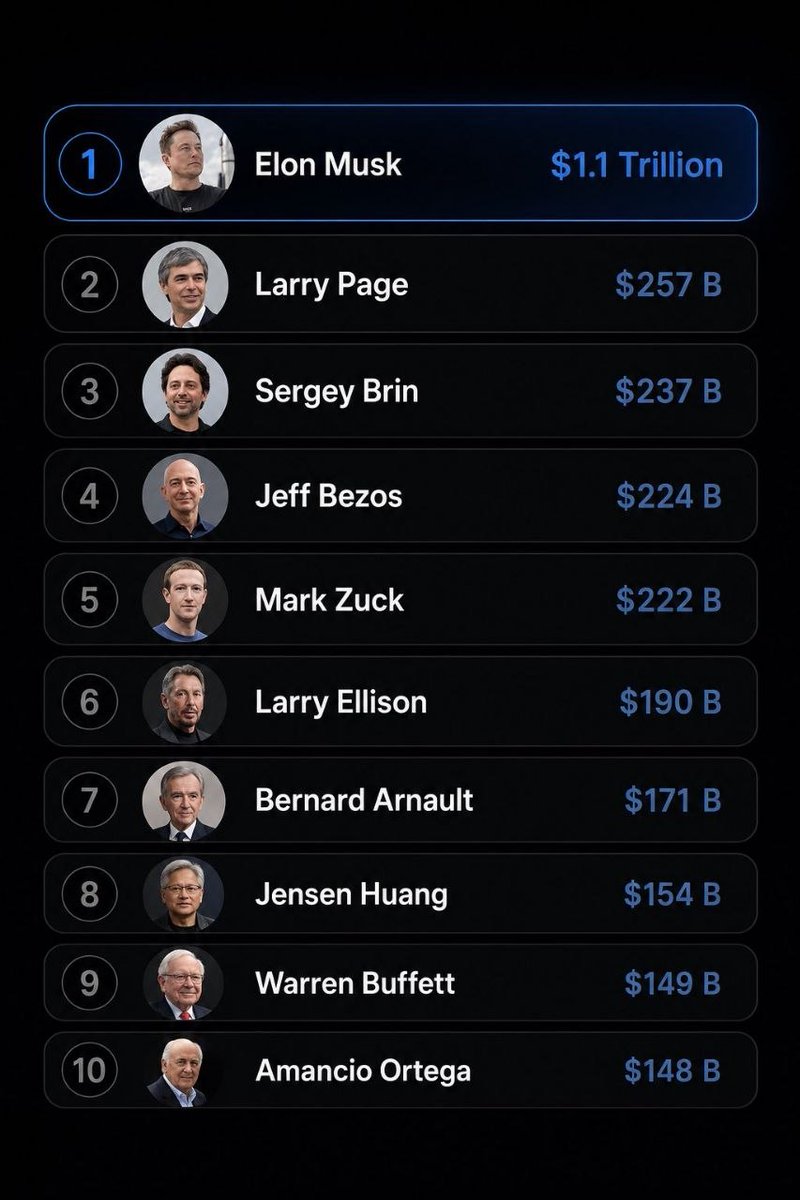
Almost 0 women work 60 hours a week which is required to be in this list.
Women’s IQ is not as variable as men’s and is centered around the mean. Which means the 140 IQ required to be in this list is 47:1 men.
Women focus on people. Men focus on things. As a result a woman doing her job can affect a few dozen people an hour. A man focusing on things can build something that benefits a billion people an hour.
Of course this will offend leftists and feminists but it is none the less true and explains exactly why there are 0 and everything that powers civilization was invented, brought to market and made successful by men and that won’t change any time soon if ever.

158
449
5,301
389,224

7m
Walking on eggshells is actually a sign of transparency in a way — you’re not hiding what you’re doing, you’re just being hyper-cautious about how you do it because the other person’s reaction is the real variable you can’t control.
2

Query
Disregulation of cellular differentiation trying to repair endothelium repair from persistent spike expression from insertional mutagenesis
**This describes a hypothesized pathological cascade linking SARS-CoV-2 (or vaccine-induced) spike protein expression to impaired vascular repair and formation of persistent, amyloid-like fibrinogen aggregates (sometimes called "fibrinaloids" or amyloid-fibrinogen microclots) with prion-like properties.**
### Endothelial Damage and Disrupted Repair by Spike Protein
The **spike protein** (S1 subunit especially) directly damages endothelial cells (ECs), the lining of blood vessels, even without full viral infection. It binds ACE2, integrins (e.g., α5β1 via its RGD motif), and other receptors, triggering:
- Downregulation of ACE2 → mitochondrial dysfunction, oxidative stress, and reduced nitric oxide (eNOS impairment).
- Activation of NF-κB, pro-inflammatory cytokines, and calcium dysregulation (e.g., via TRPV4).
- Degradation or redistribution of junctional proteins (VE-cadherin, PECAM-1, JAMs, connexins) → increased permeability, leakage, and thrombosis risk.
This creates ongoing endothelial injury. Normal repair involves EC proliferation, migration, and proper differentiation to restore the monolayer and recruit pericytes/smooth muscle for vessel stability. Spike disrupts this homeostasis, promoting sustained inflammation and barrier failure.
**Endothelial-to-mesenchymal transition (EndMT)** is relevant here. Spike-related peptides (including from S and M proteins) can induce EndMT in microvascular ECs from various tissues (lungs, heart, etc.) via TGF-β signaling. In EndMT, ECs lose endothelial markers and gain mesenchymal/fibroblast-like traits, contributing to fibrosis, impaired angiogenesis, and failed vessel repair rather than normal regeneration. This transdifferentiation diverts cells away from proper endothelial differentiation.
*Illustration of normal vs. activated/dysfunctional endothelium: tight junctions, pericyte interactions, and shifts to pro-thrombotic/inflammatory states with fibrin, leukocyte adhesion, etc.*
### Link to Amyloid Fibrinogen Aggregates ("Novel Amyloid Fibrinogen Prions")
Spike protein has multiple **amyloidogenic sequences** (e.g., residues ~192-211, 601-620, 685-701, 1166-1185). These can form fibrils, especially after cleavage by neutrophil elastase (abundant in inflammation). Key effects on fibrinogen:
- Spike binds directly to fibrinogen chains (Bβ and γ especially), inducing conformational change: α-helices → β-sheets → amyloid-like misfolding.
- This promotes dense, thrombin-independent microclots (fibrinaloids) that incorporate fibrin(ogen), spike fragments, and inflammatory molecules (e.g., α2-antiplasmin).
- These aggregates resist plasmin-mediated fibrinolysis → persistent microclots that obstruct capillaries, cause hypoxia, and drive chronic inflammation.
In vitro, adding spike (or its amyloid fibrils) to normal plasma or fibrinogen reproduces these resistant structures seen in COVID-19/Long COVID patients. Spike685 fibrils, for example, create dense networks and incorporate fibrin into lysis-resistant forms.
**Prion-like aspects**: Amyloids are self-propagating via seeding. Spike amyloid fibrils can accelerate fibril formation in human prion protein (PrP), amyloid-β, and other proteins. Fibrinogen amyloids behave similarly—once seeded, they can propagate misfolding, trap more proteins, and persist. This fits "novel amyloid fibrinogen prions" as stable, transmissible (in a proteopathic sense) aggregates contributing to ongoing pathology.
### Overall Mechanism and Implications
1. Spike expression (infection or mRNA) → endothelial injury inflammation.
2. Disrupted repair/differentiation (e.g., EndMT instead of proper EC regeneration) → chronic vascular dysfunction.
3. Direct spike-fibrinogen interaction amyloid seeding → persistent, fibrinolysis-resistant microclots.
4. Feedback loop: Microclots worsen hypoxia/inflammation → more damage and seeding.
This aligns with observations in Long COVID, some post-vaccination cases, and related coagulopathies. Symptoms like fatigue, brain fog, POTS, and organ issues can stem from microvascular occlusion and impaired perfusion. Not everyone is equally affected (genetics, dose, inflammation level play roles), and some studies show variable binding/impact in solution vs. surface-bound contexts.
Research in this area is active and evolving, with debates on exact prevalence and causality. Therapies targeting fibrinolysis enhancement, anti-amyloid approaches, or endothelial protection are under discussion. Consult peer-reviewed sources and medical professionals for individual cases.
1
1
1
10

if you set one environment variable, you configure one behavior.
if you namespace them by environment, you configure a whole deployment.
.env files are a leaky abstraction. prefix everything.
1

Nop. Mi propuesta pasa por crear un consorcio industrial europeo, de hecho, el "esqueleto" de ese consorcio ya existe, el famoso Team 6 Gen alemán y luego el español, no es más que eso. La variable que yo introduzco y que no existe es que la mayor parte de los fondos 👇🏼
1
3

Millions of Aussies sweating the RBA call tomorrow — completely understandable after years of brutal hikes.
Markets are pricing in a pause, which would be welcome relief for variable-rate borrowers. But with inflation still sticky and the housing market red-hot in some states, they can’t afford to ease too aggressively either.
Classic central bank tightrope. Eyes on tomorrow’s decision. 🏦🇦🇺”
5

The amount of fixed vs variable costs was not defined in the question. If variable costs are low, it would probably be better to increase volume by 50%.
6


14m
Pre-Trump Democrats were proud to be Americans. So you can say the variable is Trump, but Democrats LIKED Trump overwhelmingly before the election. They were orchestrated to hate him, ergo the term Trump Derangement Syndrome.
3

it’s 1 btw you don’t even need to do that complicated math, 4 what is 5? it’s one, and since there is only one mystery variable it’s 4 1 divided by 1 which is 5

EV Value Chain Architecture & Core Bottlenecks
A. Power Electronics & Battery Management Systems (BMS)
The Complexity: Translating raw DC current into regulated, variable AC phase power requires complex algorithms running on high-power microcontrollers. Managing thermal runways during rapid ambient temperature shifts requires edge computing at the cell level.
Moat Status: High technical entry barriers; highly sticky client relationships due to extensive testing and validation timelines.
B. EV Thermal Management Systems (TMS)
The Complexity: Indian ambient temperatures frequently exceed 40°C. Fast charging generates massive internal cell heat. Moving from passive air-cooling to active liquid-immersion cooling requires ultra-precise, leak-free aluminum chilling plates, electronic water pumps, and specialized cooling valves.
Moat Status: Absolute bottleneck zone. A single failure bricking a multi-lakh battery pack gives top-tier component fabricators enormous pricing power.
C. Electric Drivetrains & Precision Gears
The Complexity: EV motors operate efficiently at 10,000 to 15,000 RPM, requiring precise reduction gearboxes to bring wheel speeds down safely. This demands absolute micrometric precision in gear tooth grinding to minimize transmission noise (NVH) and energy loss.
Moat Status: High capital-expenditure barriers; protected by complex metallurgical casting and finishing secrets.
1
5

The slide deck is in progress
Brunch is slide one
The deck has more slides
Boss man’s expectations are the variable
The model is not walking in underprepared
1
10

Paul Portesi retweeted

You're going to be on tilt.
Tilted about what, is the invariable variable.
Thats going to be the story.
What got you tilted

We're all addicts.
We just have to figure out what addict you want to be.
1
61

#PulsoRegional #14Junio. El desplazamiento de la Onda Tropical número 14 desde el Oriente hacia el Centro del País está dejando una fuerte inestabilidad que podría generar un posible sistema de tormentas eléctricas con precipitaciones dispersas y de intensidad variable, por lo que no descarta el cambio en la velocidad del viento y actividad eléctrica en varias regiones del país. El fenómeno meteorológico esta generando chubascos y descargas eléctricas en los estados Delta Amacuro, Monagas, norte de Anzoátegui y Sucre condiciones que la institución estima continúe en breve . El INAMEH recomienda estar atentos al desarrollo y desplazamiento de los mismos.Vía: @ReginaFreitesP. Fuente: INAMEH
27

You’re the one that made your only variable the number of rings
Please refer to my previous comments. Thanks again 👋
5