

Apr 25
ControlSwitch - THE FINALS 605.5 - #1
@xuddley forced me at gunpoint to post this
@StellarAiming
1
1
8
365



Feb 18
Controlswitch #33
did this with 34cm, honestly i could try a slower sens and get a slightly better score but nah
@yaoi_aimers
19
400

Feb 5
🔴TARGET SWITCHING:
🔵ARC Snitchswitch: Speed switching scenario featuring disk-shaped targets flying above the player with a low time-to-kill. Trains fast target acquisition and aiming at awkward angles, while resembling the Snitch enemy from ARC Raiders. Player movement is disabled to keep the focus on raw switching speed.
🔵ARC Smoothswitch: A target switching scenario with several gently flying targets surrounding the player. Compared to most switching scenarios, this one leans more toward tracking due to its higher time-to-kill. It also includes health regeneration, meaning targets must be fully eliminated before moving on to the next one. Player movement is enabled but optional.
🔵ARC Controlswitch: A target switching scenario featuring evasive flying targets around the player. It is even more tracking-oriented due to the targets' more erratic, yet still readable, movement patterns. Like Smoothswitch, it uses health regeneration, requiring full eliminations before switching targets. Player movement is enabled but optional.
⬇️
1
3
167
Jan 5
🔴SMOOTH SWITCHING:
🔵Smoothswitch OW: A target switching scenario with several gently flying targets surrounding the player. Compared to most switching scenarios, this one leans more toward tracking due to its higher time-to-kill. It also includes health regeneration, meaning targets must be fully eliminated before moving on to the next one. ADS and player movement are optional.
🔵Controlswitch OW: A target switching scenario featuring evasive flying targets around the player. It is even more tracking-oriented due to the targets' more erratic, yet still readable, movement patterns. Like Smoothswitch, it uses health regeneration, requiring full eliminations before switching targets. ADS and player movement are optional.
⬇️
1
4
426
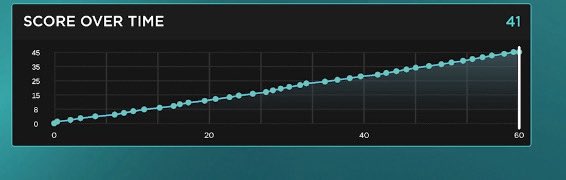
controlswitch intermediate - 46.20
1
4
77
27 Dec 2025
🔴360° SWITCHING:
Important note: In all three of these tasks you can move if you want to. Movement does not affect scoring, but it makes the task feel more game-like and helps players better understand how movement correlates with aim.
🔵Horizontal Switch BF6: Target switching scenario featuring several humanoid targets. Trains quick horizontal flicking in a 360° arena. Headshots deal more damage. ADS and player movement are optional.
🔵Smoothswitch BF6: Target switching scenario featuring several gently flying targets around the player. A more tracking-focused scenario compared to the previous ones, meant to introduce a smoother, more controlled playstyle rather than only flashy flicks. The scenario also features health regeneration, which means the player must fully eliminate a target before moving to the next one. ADS and player movement are optional.
🔵Controlswitch BF6: Target switching scenario featuring several evasive flying targets around the player. This is the most tracking-focused scenario in the routine. It also features health regeneration, meaning the player must focus on fully eliminating each target before switching. ADS and player movement are optional.
⬇️
2
2
243

2 Nov 2025
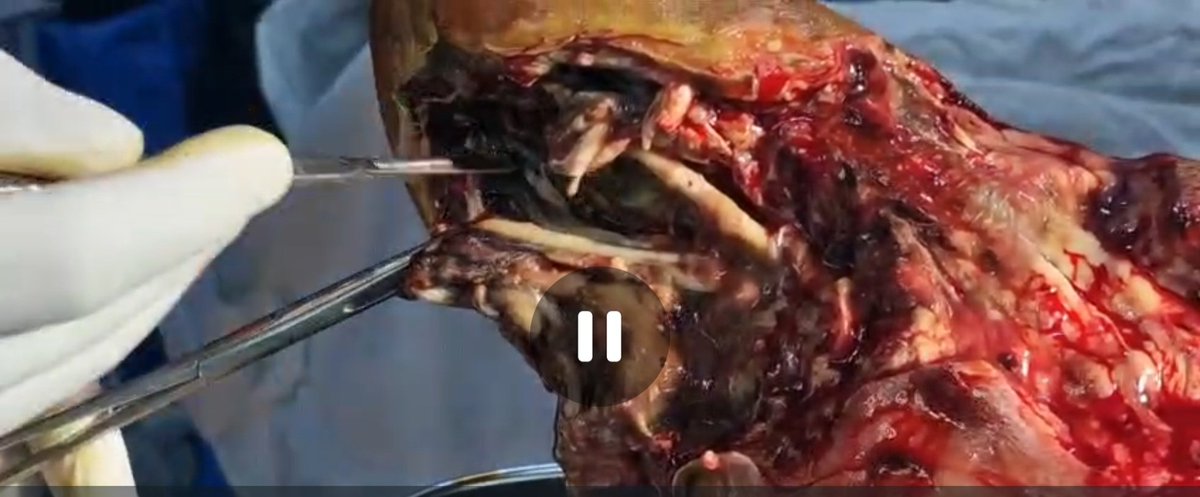
A bad diabetic foot is a metabolic emergency!
Case by Dr Vinay Dhandhania, Diabetologist, Ranchi
Patient: Male, 66 years
Diabetes: 20 years, poorly controlled (HbA1c = 9%)
Presentation:
Admitted with severe diabetic foot infection (left foot)
Underwent surgical debridement 3 days ago
Right foot is also high-risk
Background of peripheral vascular disease (PVD) and likely neuropathy
Images provided:
Left foot shows extensive necrosis, slough, and exposed tissue, compatible with infected wet gangrene / necrotizing fasciitis post-debridement.
Right foot shows digital ischemia, atrophic skin, and deformity—a neuro-ischemic diabetic foot at imminent risk.
Surgical video suggests deep fascial and tendon involvement, possibly extending to bone (osteomyelitis).
⚕️ Stepwise Clinical Analysis
1. Pathophysiology
This is a classic case of long-standing Type 2 diabetes with peripheral neuropathy, PVD, and superimposed infection leading to:
Ischemic necrosis → gangrene
Secondary bacterial infection → suppuration, tissue liquefaction
Systemic metabolic stress → poor wound healing, anemia, renal strain
2. Immediate Priorities
DomainKey Actions
Glycemic controlSwitch to IV insulin infusion or basal–bolus regimen; target glucose 140–180 mg/dL in hospital. Avoid SGLT2i.
Infection controlBroad-spectrum IV antibiotics (e.g., piperacillin–tazobactam ± clindamycin ± vancomycin) until culture results.
Wound managementSerial surgical debridement; remove all necrotic tissue; consider negative-pressure wound therapy (NPWT) after infection control.
Vascular assessmentDoppler / CT angiography to assess perfusion; if possible, angioplasty or distal bypass before deciding amputation level.
Supportive careOptimize nutrition, treat anemia, manage fluids, avoid nephrotoxins, and provide analgesia.
3. Surgical Perspective
Extent of involvement: Muscle and tendon necrosis likely → radical debridement justified.
Post-op monitoring: Ensure adequate drainage, aseptic dressing, glycemic control.
Amputation consideration: If vascularity poor or infection uncontrolled → below-knee amputation may become life-saving.
Multidisciplinary approach: Endocrinologist Vascular/Plastic surgeon Orthopedic Infectious disease Physiatrist.
4. Right Foot (High-risk Limb)
Findings: Clawing, muscle wasting, dry skin, absent hair, digital darkening → ischemic neuropathy.
Preventive strategy:
Off-loading footwear / customized orthosis
Daily inspection & hygiene
Nail and callus care
Avoid barefoot walking
Maintain foot warmth and moisture balance
5. Investigations to Review
X-ray / MRI foot: look for gas, osteomyelitis, Charcot changes
Vascular Doppler: ABI, flow velocity
Culture & sensitivity of wound
Renal function (many have concomitant CKD)
CBC, CRP, procalcitonin for infection severity
6. Prognosis
Guarded, depending on vascular status and infection control.
High amputation risk if:
Gas in tissue,
Osteomyelitis,
Persistent sepsis despite adequate surgery,
Poor perfusion on Doppler.
7. Long-term Goals
1. Secondary prevention:
Strict glycemic, BP, and lipid control.
Smoking cessation.
2. Foot care education:
Regular podiatric visits and footwear compliance.
3. Rehabilitation:
Early prosthesis / mobility training if amputation occurs.
4. Follow-up:
Periodic vascular reassessment and infection surveillance.
Key Take-home Clinical Pearls
A bad diabetic foot is a metabolic emergency—requires swift infection control, vascular evaluation, and glycemic stabilization.
PVD and neuropathy together predict limb loss more than infection alone.
HbA1c ≥ 9% indicates chronic neglect—intensify systemic management, not just local wound care.
Never delay revascularization decisions—a dead foot can cost a living life.
Dedicated multidisciplinary diabetic-foot teams dramatically reduce amputation rates


2
1
8
922

14 Jun 2025
Controlswitch - 53 - #1 [WR]
evasive switching my beloved
3
2
77
3,528



7 Nov 2024
WHITE-RODGERS SWITCHING RELAYS LOT 90-340 90-342 90-370 90-341 91-902 FURNAS ebay.com/itm/296790627570?mk… #eBay via @eBay #HVAC #Contractor #HeatingCooling #homerepair #DIY #controlswitch #plumbing #Business #Industrial #heating #Tech #electrical #repairman #winter #AC #cooling
8
5
102
6 Oct 2024
ICM Controls Delay-On Break Timer Relay Lot ICM102 ICM203 ebay.com/itm/235767498997?mk…… #eBay via
@eBay
#electric #Electrical #Business #industrial #ControlSwitch #Tech #Technician #electrician

7
4
56
3 Oct 2024
ICM Controls Delay-On Break Timer Relay Lot ICM102 ICM203 ebay.com/itm/235767498997?mk…… #eBay via
@eBay
#electric #Electrical #Business #industrial #ControlSwitch #Tech #Technician #electrician

14
5
161

1 Oct 2024
Check out ICM Controls Delay-On Break Timer Relay Lot ICM102 ICM203 ebay.com/itm/235767498997?mk… #eBay via @eBay #electric #Electrical #Business #industrial #ControlSwitch #Tech #Technician #electrician

30
16
209

5 Aug 2024
Have you discovered the much-awaited NEW additions to the Click Scolmore collection? Discover them here 🔗 ow.ly/I44X50SRlFY
#Scolmore #ScolmoreGroup #Click #Ireland #ClickLitehouse #GarageBoard #ConsumerUnit #ToothbrushCharger #ControlSwitch #UnswitchedSocket
2
24

10 May 2024
Question: In your experience, what are some of the key factors to consider when troubleshooting a control switch that’s exhibiting abnormal behavior or error conditions?
Please let’s know your answer in the comment below 👇
#ControlSwitch #EngineeringTech
1
4
40
