
12 Nov 2024
We need to train #HDR
hydrodynamic recanalization
to find its role
in #hybridalgorithm
for #CTOPCI
@KambisMashayek1 @swissCTO
@JTiwanaMD @RhianEDavies1
@transradial @ptca5fr
@BongKiLee3 @dautov_MD @jedicath @AlexAchimMD @mornei2011 @anna_bortnick @SumitsujiS @mirvatalasnag
11 Nov 2024

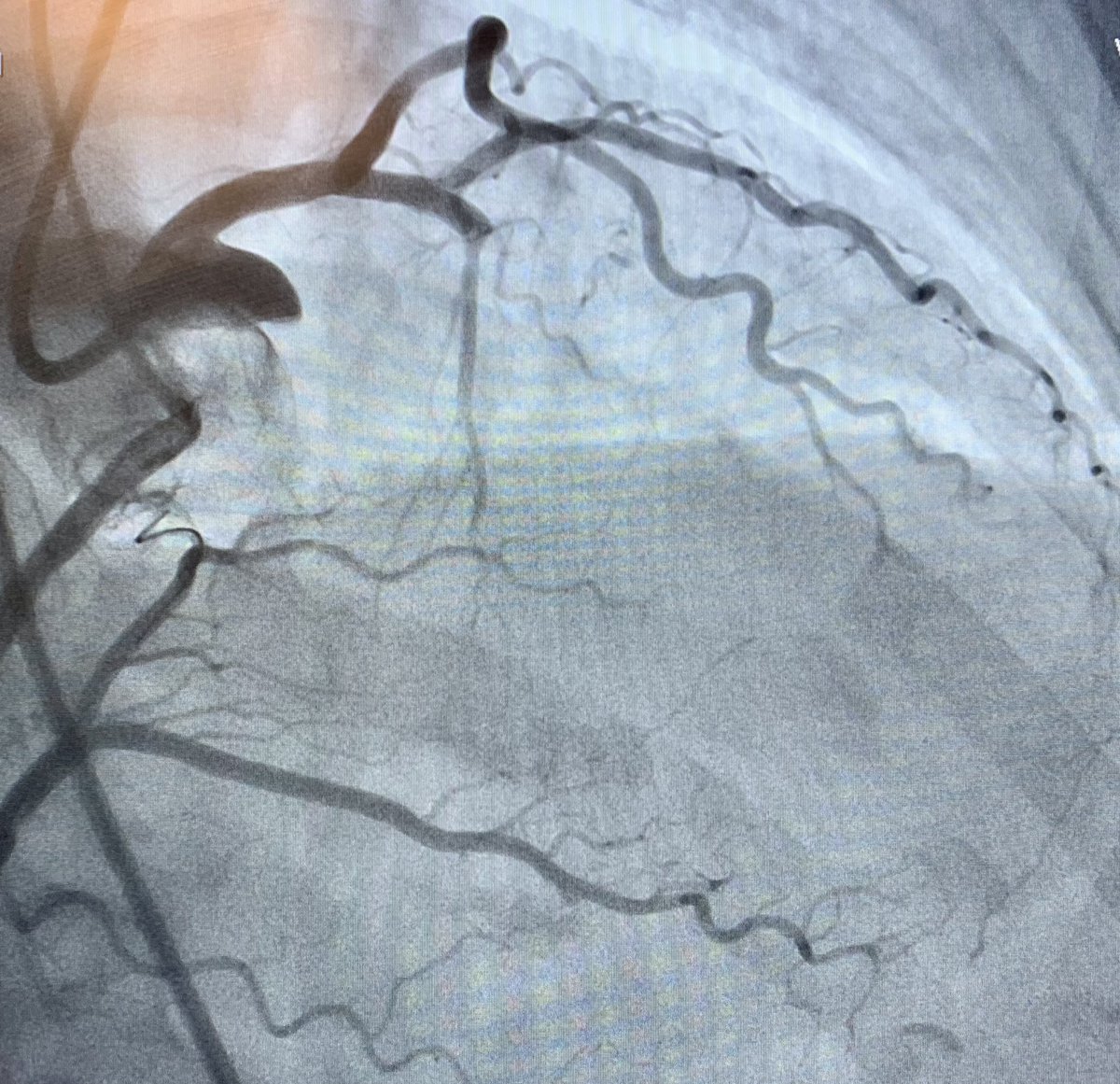
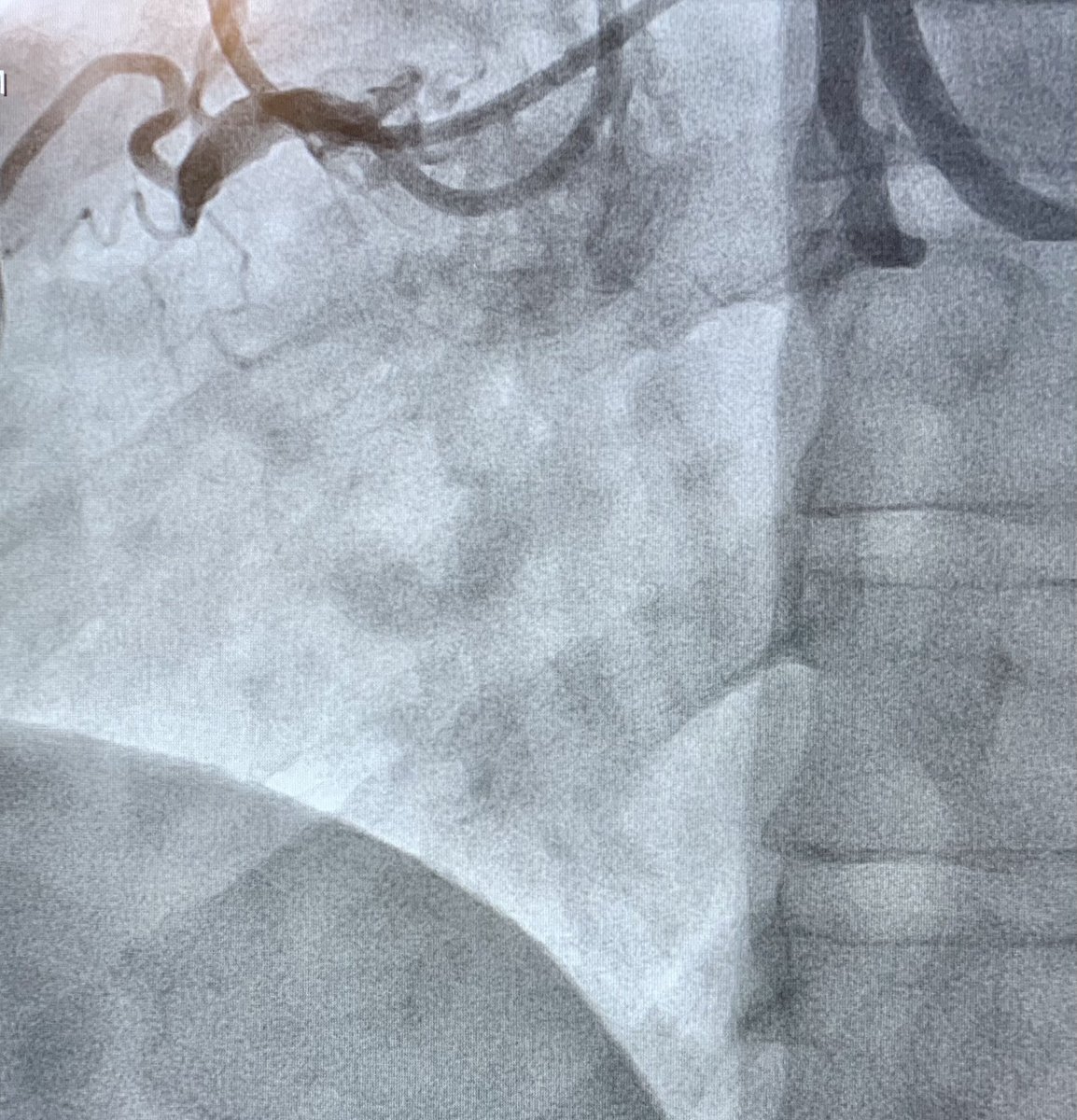
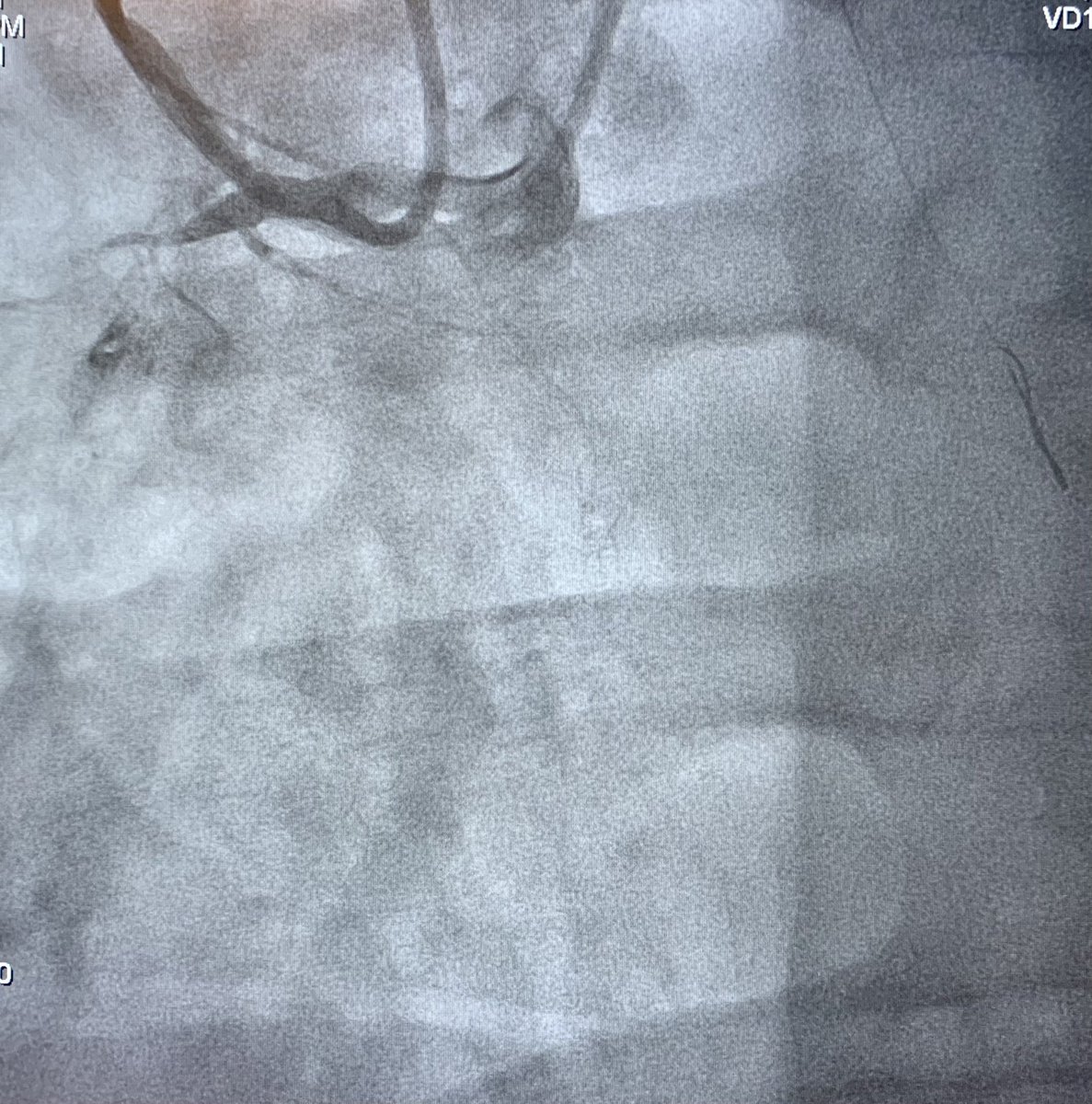
HDR is a new to concept to many of us. HDR in some ways challenges how we have been taught and currently practice CTO PCI. The use of contrast modulation is not new, but what is new is the move to using contrast first as “a first approach” for a CTO. There are my initial comments on this:
1. The strategies we currently use are AWE/ADR and RWE/RDR. The question is where HDR fits into the algorithm. But then HDR is not for every CTO. But that’s fine, as we know that no one strategy works for every CTO, and we often switch strategies as per the hybrid algorithm.
2. In post-CABG heavily calcified CTOs, where I have used a contrast injection to disrupt tough proximal cap, has a provided a natural means of testing this. HDR does not work for these CTO subsets in my experience. I think with time we will indeed learn more about this technique and the anatomies where it is likely to work.
3. The key question in most minds is : Should HDR always be the “first approach”? In most lesions where this may work, are the soft CTOs, which one may argue may be easily addressed with AWE. So the question is shouldn’t one try AWE first, before considering HDR. Although HDR may show the way for AWE, there is also a chance that HDR may disrupt the vessel unfavourably as such to reduce the likelihood of subsequent AWE, and then the need to switch to other strategies like ADR, which could have otherwise be avoided.
4. It is always important to try and learn new strategies and techniques. After all that’s how we grow and get better. There are no hard and fast rules. I am always welcome to trying new techniques.💪🙌
2
1
9
1,168

25 Sep 2022
#mdpienergies #highlycitedpaper
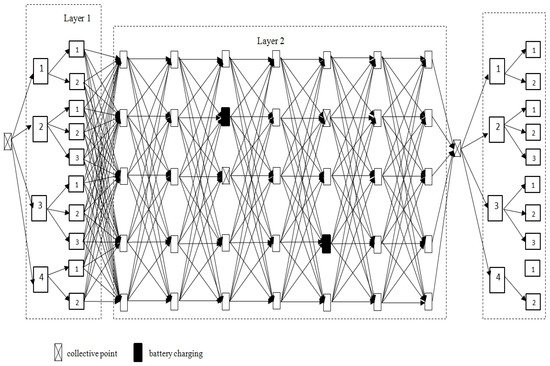
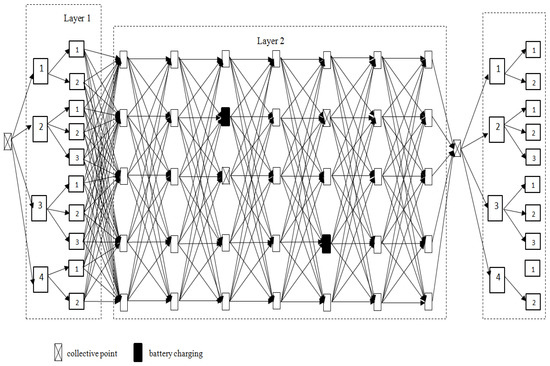
An Efficient Hybrid Algorithm for Energy Expenditure Estimation for Electric Vehicles in Urban Service Enterprises
👉mdpi.com/1996-1073/14/7/2004
@PW_edu
#electricvehicles #emobility #hybridalgorithm
2
24 May 2022
#mdpienergies #highlycitedpaper
An Efficient Hybrid Algorithm for Energy Expenditure Estimation for Electric Vehicles in Urban Service Enterprises
👉 mdpi.com/1996-1073/14/7/2004
@WUT_edu
#electricvehicles #hybridalgorithm #emobility
2

17 Sep 2021
Tools of the #HybridAlgorithm Trade!
17 Sep 2021

Another successful #CTOPCI using Crossboss and wire escalation for #ADR topped off with #IVL for a calcified blunt cap with excellent results. #PennsyInterventions @jcgeorgemd @GPAngioClub @ACVCPhila @PennCardiology @PennCVFellows @BSCCardiology @ShockwaveIVL

11

24 Jul 2021
Tale of 2 CTOs: dual simultaneous coronary injections, wire escalation, and antegrade dissection re-entry for successful revascularization. #hybridalgorithm @jcgeorgemd @GPAngioClub @ACVCPhila @PennCardiology @PennCVFellows
1
3

25 Jul 2020
Harvard scientists created a hybrid algorithm for NMR readings
@Harvard #QuantumComputer #HybridAlgorithm #research
techexplorist.com/hybrid-alg…
1
2

15 May 2020
I would fix the RCA first then stage the LAD. Since the LAD is a true CTO, bring the heavy artillery as @TheNarulaSeries says. 2 guides, be prepared for all aspects of the #hybridalgorithm. Nice case.
2
2

28 Apr 2020
[Article] Research and Study of the Hybrid Algorithms Based on the Collective Behavior of Fish Schools and Classical Optimization Methods
mdpi.com/1999-4893/13/4/85
#evolutionaryoptimization
#swarmintelligence
#fishschoolsearch
#gradientdescent
#hybridalgorithm
#algorithms

1
1

3 Dec 2019
Step-by-step #CTO #PCI 48 y.o female with familial Hyperlipidemia, chronic tobacco use and CAD, s/p MIDCAB and previous interventions to pRCA, pLAD presented w worsening angina despite aggressive medical therapy. Angio> RCA #CTO w L>R and R>R collaterals #CHIP #HybridAlgorithm
3
16
58

24 Apr 2019
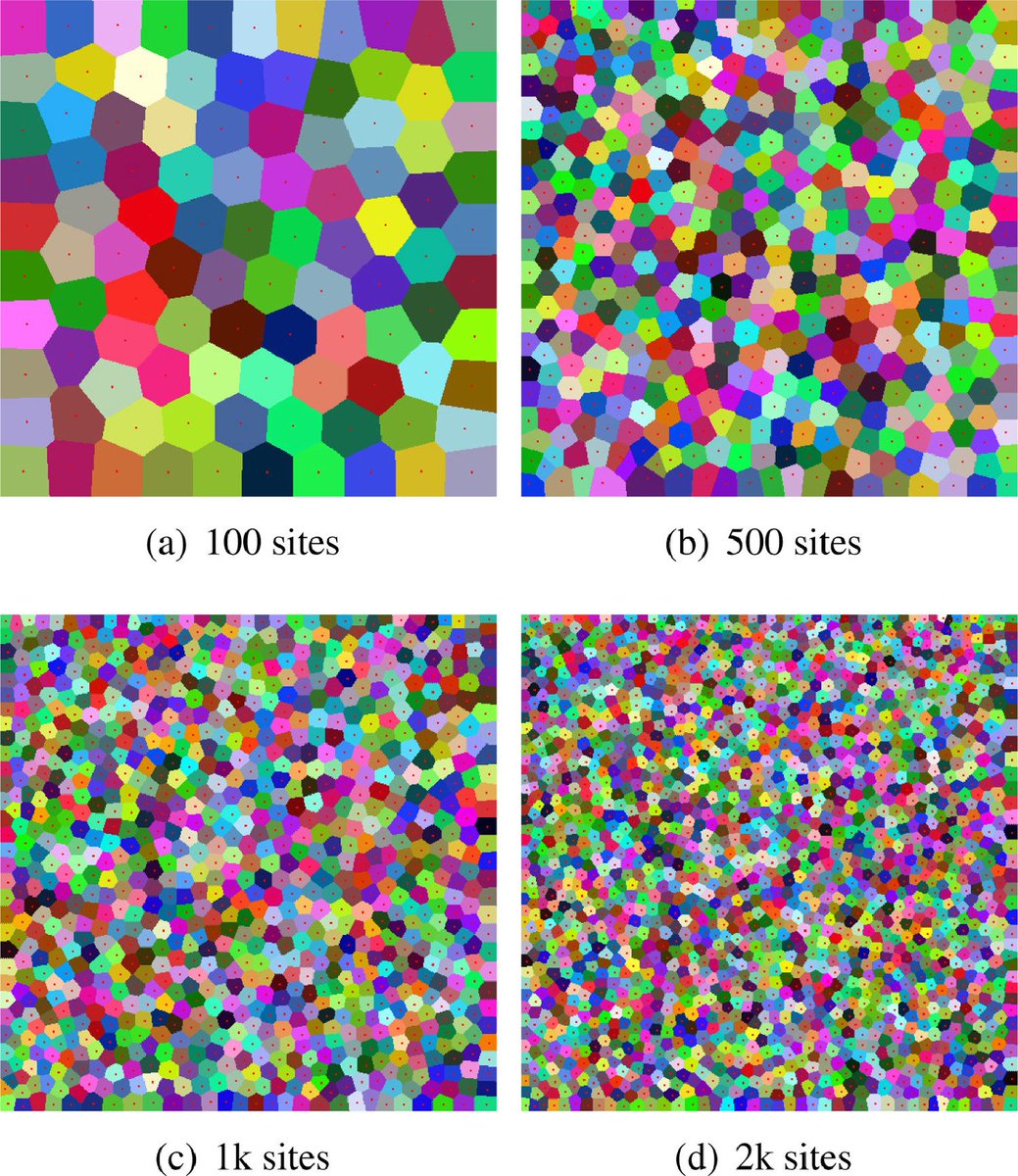
GPU-based efficient computation of power diagram
See more: bit.ly/2IkZ73y
Authors: Zheng, Gui, Cai, Fei, Zhang, Xu
#CagJournal #ComputerGraphics #GPU #computaion #diagram #efficient #geometrical #HybridAlgorithm #JFA #edges #magnitude
1
3