
Physician anesthesiologist | Cofounder & Executive Director, Opioid Free America | 33 yrs in healthcare—zero tolerance for the status quo.
Joined November 2008
- Tweets 21,911
- Following 4,983
- Followers 3,928
- Likes 7,645
365 Photos and videos











Matt McCord retweeted

Jun 15
“He's at least ten years ahead of everyone else as far as making satellites, as far as making rockets, as far as building networks,” says @RonBaronAnalyst of @elonmusk following the $SPCX IPO. “They have opportunities that are changing lives.” cnb.cx/3Qirmom
28
42
266
28,423
Matt McCord retweeted

Jun 15
“You have thousands of moments ahead of you. The important thing isn’t to get them all right; it’s to find a way to keep moving forward.”
Sundar Pichai, MS ’95, CEO of Google and Alphabet, addressed the Class of 2026 at Stanford’s 135th Commencement ceremony.
Watch the full speech at the link: stanford.io/4e8weWd
73
610
2,872
497,453
Matt McCord retweeted

Jun 14
The recent impressive drug (daraxonrasib) success vs pancreatic cancer may presage a much broader set of wins.
gift link @TheEconomist
economist.com/science-and-te…

7
147
619
34,644

Jun 15
Salient points from @drbruggeman. The devil is in the details.
MSOs are being sold as a lifeline for independent medicine — but the math only works if physicians retain their owner-stakeholder position. That ownership is what keeps docs engaged in care delivery and advocating for their patients. An MSO, by definition, relinquishes some of that.
And here's what rarely gets said: the negotiating problem isn't solved by MSOs — it's structural. When 97% of commercial insurance markets are highly concentrated and a single insurer controls 50% of premiums in nearly half of metro areas, small physician groups — even MSO-backed ones — are still outgunned. Only hospital systems have the leverage to negotiate in these markets.
The "good MSO" path Dr. Bruggeman describes is real. So is the bad one. The difference lives in contract terms most physicians don't have time to read. Until we address insurance monopoly power directly, we're asking independent docs to fight a structural battle with operational tools. ♻️
Jun 15

MSOs: A Necessary Part of Healthcare Delivery?
Independent medicine is not disappearing because physicians stopped wanting to practice independently. It is disappearing because the infrastructure required to survive in modern healthcare has grown far beyond what most small groups can build alone.
Value-based care contracts require data analytics, population health platforms, and care coordination teams. Prior authorization compliance requires dedicated staff and software. Revenue cycle management has become a specialty in its own right. Credentialing, HR, real estate, IT, and EHR optimization haven’t become easier as payers and health systems grow larger.
The negotiating environment has become structurally hostile to small independent groups. The AMA's 2024 Competition in Health Insurance report found that 97% of commercial health insurance markets at the metropolitan level are now classified as highly concentrated under federal merger guidelines, with HHI exceeding 1,800. In 47% of metro areas, a single insurer holds at least half the commercial market. Physician practices are negotiating contracts against counterparties that, in nearly every local market in the country, face no meaningful competitive pressure to offer fair terms.
The GAO reported in September 2025 that at least 47% of physicians were consolidated with hospital systems by 2024, up from less than 30% in 2012. The AMA's own practice benchmark data shows that only 42.2% of physicians were working in private practice as of 2024, down from 60.1% in 2012.
The Management Services Organization model has emerged as one of the most debated structures in healthcare. An MSO is a separate legal entity that contracts with a physician-owned professional entity to handle administrative, operational, and financial functions like billing, coding, HR, technology, facility management, credentialing, and strategic business development. Physicians retain ownership of the clinical practice and, in theory, exclusive control over clinical decisions. The MSO handles the business infrastructure the practice cannot efficiently build or maintain on its own.
While the concept is good, the execution varies enormously. The difference between an MSO that strengthens an independent practice and one that quietly absorbs it often lives in contract terms that physicians never had time to read carefully.
That is what this week is about. Independent physicians need operational support, capital, and negotiating scale. The question is what kind of partnership delivers those things without trading away the clinical autonomy that makes independent medicine worth fighting for.

1
100
Jun 15
Popular joint supplement glucosamine linked to faster Alzheimer’s progression | ScienceDaily sciencedaily.com/releases/20…
19
Jun 15
Signs of Breast Cancer Could Be Spotted 3-6 Years Before Diagnosis Using AI Screening, Shows Massive Study goodnewsnetwork.org/signs-of…
24
Matt McCord retweeted

Jun 13
I bought a Tesla thinking I was buying a car. Turns out I was buying a front-row seat to the first guy on earth to hit a trillion dollars.
Elon crossed it yesterday when SpaceX went public. He got there building something people line up to buy at a price posted before they walk in.
The hospital that owns my town got rich the other way. Buy the only competitor for fifty miles, hide the price, mail the bill later.
*My license plate is GZELLIG for the great Dutch feeling of gezelligheid.

10
11
160
4,225
Matt McCord retweeted

I showed my son this.
Show yours, too.
55
562
4,262
169,163
Matt McCord retweeted

Jun 12
Elon just created 4,400 millionaires in a single day.
400 of them are now worth over $100 million.
These aren't VCs. They're SpaceX employees, and the list includes welders, technicians, and cafeteria staff, because for two decades the company paid every level of the workforce in stock instead of higher salaries.
Juan Hernandez immigrated from Mexico and took a $28 an hour contractor welding job in 2015. He says he didn't even know what SpaceX was. The company gave him a $10,000 equity grant and let him buy more shares through payroll deductions. That stake is now worth $880,000.
Trevor Hise's parents wanted him to take a stable job at General Electric. He picked SpaceX instead, stayed 12 years, and accumulated over 100,000 shares. At the $135 listing price that's $13.5 million. He's 37 and semiretired. His words: "The magnitude of this has been ridiculous."
The most telling detail came before the listing. Over 100 employees quietly banded together and negotiated a group wealth management deal covering up to $5 billion, because none of them had ever needed a wealth manager before.
Software IPOs have minted millionaires for 30 years. This is the first one where the money went to the factory floor.
3,279
25,639
142,082
7,497,186
Matt McCord retweeted

I charge $350 for a new patient visit. This includes a number of procedures (nasal endoscopy, laryngoscopy, ear microscopy) if necessary.
Here’s why I don’t take insurance. This plan believes that visit is worth $13.96. I honestly don’t know how any doctor can afford to take insurance.

341
381
3,036
126,375
Matt McCord retweeted

Jun 11
Sepsis kills more people in American hospitals than heart attacks. 350,000 deaths a year, and the reason is brutally simple: the early warning signs are almost invisible.
A slightly elevated heart rate. A small temperature shift. A lab value drifting in the wrong direction. Each one looks like noise on a busy ward. By the time the pattern is obvious to a human, the patient is hours into a cascade toward organ failure, and every hour of delayed antibiotics raises mortality.
Tampa General built a system on Palantir's Foundry that watches roughly 1,000 inpatients continuously. Vitals, labs, medication records, clinician notes, all scanned in real time for the pattern no single nurse can see across 12 beds at 3am. When risk crosses a threshold, a rapid response team gets paged. Humans still make every treatment decision. The software just compresses detection from hours to minutes.
The results since 2022: overall sepsis mortality cut in half, 48-hour deaths down 68%, length of stay down 30%, roughly 900 lives saved. At one hospital.
Now run the national math. There are about 6,100 hospitals in the US. If even the 500 largest matched these numbers, you'd be looking at tens of thousands of lives a year from a single use case. The treatment for sepsis hasn't changed. Antibiotics and fluids, same as decades ago. The entire gain comes from starting them earlier.
The hardest problem in medicine was never the cure. It was noticing in time.
Jun 10

JUST IN: Florida hospital reveals Palantir software has cut sepsis deaths by more than half since it was installed.
180
1,560
9,950
1,407,416
Jun 10
Daily Activity and Positive Mood Form a Continuous Loop - Neuroscience News neurosciencenews.com/daily-a…
6
Jun 10
A very important point. A real marketplace in American healthcare for all but catastrophic events would make it much more efficient and effective.
Jun 8

LASIK isn’t covered by insurance. Neither is most cosmetic surgery.
Both got cheaper and better every single year for two decades.
The one corner of medicine where patients pay cash and see prices.
Funny how the “market failure” vanishes the second the market’s allowed to exist.
Friedman called this in 1980. The tape doesn’t lie.
1
1
25
Matt McCord retweeted
Jun 9
The first participant to receive partial cellular reprogramming for eye disease (advanced glaucoma) in a pilot study of 12 patients was treated. Using 3 of the 4 Yamanaka stem cell factors to potentially achieve cellular rejuvenation @Nature
nature.com/articles/d41586-0…
17
126
579
98,426
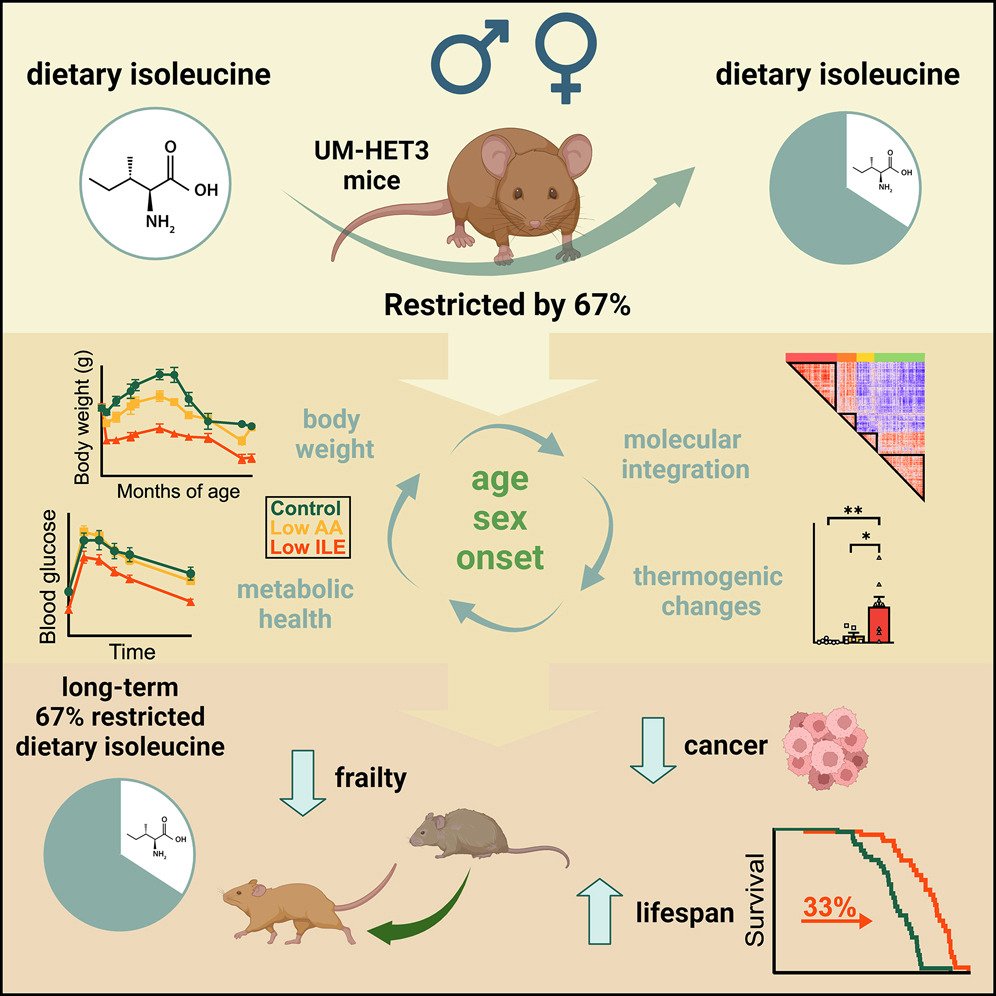
Matt McCord retweeted

I’m very familiar w/the mouse paper that motivated this, mechanistic rationale and the hurdles for it to “work”… but if it does, it’s historic as retinal neurons are CNS (effectively “brain”). Best of luck @davidasinclair & team. nature.com/articles/d41586-0…
41
143
950
179,905
Matt McCord retweeted

I'm a cardiologist. I've held dying hearts in my hands in the cath lab at 3 AM. And I need to tell you something that changes everything about how we prevent heart attacks.
For decades, the entire field was built on one target: lower LDL cholesterol. Statins save lives — that's settled science. But too many of my patients did everything right — took their statins, hit their numbers, lived clean — and still ended up on my table with a ruptured artery.
We were treating the smoke while the fire kept burning.
The fire is inflammation. And the evidence is now overwhelming.
The CANTOS trial proved it first — lowering inflammation independent of cholesterol reduced cardiac events. But the newer data is what keeps me up at night.
AI-enhanced CT angiography can now detect inflamed arteries by measuring changes in the fat surrounding your coronary vessels — the perivascular fat attenuation index. Higher inflammation in the fat around even one artery independently predicts cardiac death. When multiple arteries show inflammation, the risk multiplies dramatically — even in patients whose cholesterol looks perfect.
This isn't theoretical. This is measurable. Right now. On a scan you can get this month.
Low-dose colchicine — a drug that's been around for centuries for gout — is now FDA-approved specifically for reducing cardiovascular events. It works by quieting the inflammatory cascade that destabilizes the plaque sitting in your arteries. A pill that costs pennies is saving lives the statins couldn't reach.
And the next wave is already in Phase 3 trials. Ziltivekimab — an IL-6 inhibitor — targets the central inflammatory pathway driving atherosclerosis. Phase 2 data showed a 90% reduction in hsCRP. The ZEUS cardiovascular outcomes trial is enrolling now, with results expected late 2026 into 2027. If positive, anti-inflammatory therapy will become standard in managing heart disease alongside lipid-lowering. The era of inflammation-targeted cardiology is arriving.
But it goes deeper than drugs. AI is now predicting heart failure and cardiac events 5 years before symptoms — integrating CT imaging, electronic health records, and genetic data with accuracy that jumps far beyond traditional risk calculators.
And polygenic risk scores — a simple genetic test that flags inherited cardiovascular risk — are now formally recognized as a risk-enhancing factor in the 2026 ACC/AHA guidelines. A single blood draw can reveal risk that's been silently building since birth. Decades before the first chest pain.
Here's what this means for you right now — today:
Ask your doctor for a high-sensitivity CRP test. It's cheap, routine, and measures the systemic inflammation that standard cholesterol panels completely miss. You can have perfect LDL and inflamed arteries that are quietly preparing to rupture.
If your hsCRP is elevated, discuss low-dose colchicine with your physician. It's FDA-approved for exactly this.
Push for a coronary CT angiography with AI plaque and inflammation analysis if you have risk factors. This isn't the stress test your parents got. This is 3D visualization of your actual arteries — with AI quantifying not just how much plaque you have, but what kind it is and whether the surrounding tissue is inflamed.
Consider polygenic risk score testing — especially with a family history of early heart disease. It's now guideline-supported.
And the foundation that never changes: move daily, eat real food, sleep 7-9 hours, manage stress, and know your numbers — ApoB, Lp(a), hsCRP, fasting insulin.
I left Iran as a child with nothing. I rebuilt everything in a country that gave me the freedom to become a physician. I've spent twenty years watching patients get second chances.
The ones who haunt me aren't the ones who died on my table. They're the ones who survived but never acted on what the science was telling them — years before the event that didn't have to happen.
You can have perfect cholesterol and still have a heart attack. Inflammation plus genetics can drive plaque rupture in arteries that look "fine" on a standard panel.
The myth that normal cholesterol means you're safe has cost more lives than I can count.
We now have the tools to detect the fire — not just the smoke. AI to see it. Genetics to predict it. Drugs to quiet it. And the ancient basics — movement, real food, sleep, purpose — to prevent it from starting.
Prevention is the new cure. And the science to make it real is no longer coming.
It's here.
466
2,059
12,002
4,012,899
Matt McCord retweeted

Physicians are not burned out because medicine is hard.
Medicine has always been hard. That is not new.
We are burned out because the things making it harder have nothing to do with medicine.
Fix the system. Keep the physicians.
96
538
2,163
116,806
Matt McCord retweeted
Jun 9
10
60
220
35,341

