
RN educator, clean air & precautionary principle enthusiast.❣️creativity, arts & humanities 4health care ed. Find me upstream. Posts=mine, she/her #GoodTwitter
Joined May 2012
- Tweets 5,393
- Following 2,247
- Followers 656
- Likes 77,268
351 Photos and videos












Pinned Tweet

10 Jun 2023
Good timing for this reminder in my home province of Alberta. #CovidIsAirborne & this poster by @schmutzparty a reminder to protect the most vulnerable people in essential places.
ALT This 1930’s inspired poster depicts a person in profile wearing a respirator. Text at top says: Do No Harm. Bottom reads Keep Masks in Healthcare. smaller print reads: Wearing a mask is harm reduction. Protect your community. Art by @schmutzparty
3
11
27
2,494
Jocelyn Lehman retweeted

This is an astonishingly misinformed take by @VaughnPalmer, who seems to have little understanding of harm reduction or what's actually happening with the toxic drug crisis.
Overdose deaths have been declining across North America, including in many places that don't have supervised consumption sites, safer supply, or the harm reduction services available in B.C. To suggest B.C.'s retreat from harm reduction is responsible for the decline is pure speculation.
What's being ignored is that we're seeing more overdose events than ever, but fewer people are dying because people are being revived. Naloxone, supervised consumption sites, outreach workers, peers, and first responders are keeping people alive.
That's what HARM REDUCTION does.
Using a decline in deaths to argue that harm reduction isn't working is like using a decline in traffic fatalities to argue against seatbelts.
The real question is: how many more people would be dead if nobody was there with naloxone? If supervised consumption sites didn't exist? If outreach workers weren't responding? If people were left to use alone?
The people alive today because of those interventions aren't statistics, they're the evidence that harm reduction works.
Jun 16

Vaughn Palmer: Dropping opioid death toll hints B.C. NDP retreat on harm-reduction may be working vancouversun.com/opinion/col…

23
59
127
8,163
Jun 11
Great news ⬇️

😷 BREAKING🚨
Canada launches a new National Advisory Committee on Preventive Health Services.
It will be chaired by Dr. David Keegan, a leading advocate for masks in healthcare and on airplanes who filed human rights litigation on both fronts.

ALT 3M Aura
1
20
Jocelyn Lehman retweeted

There are plenty of world-class L0ngC0vid experts far smarter than I am.
But I bring something they don’t: I’m a CV surgeon and endovascular specialist. I’ve had hearts, lungs, arteries, and other organs literally in my hands. I’ve seen their insides, healthy and ravaged, with my own eyes.
That gives me one brutal, irreplaceable edge: I can take the science and translate it straight into the living, bleeding reality of human anatomy.
And what I see coming is ugly.
You, personally and as a society, are in for one hell of a shock.
Read this 🧵👇
If you keep minimising SARSCoV2, refuse to protect yourselves, and keep swallowing the lies of pseudo-experts chasing money or psychiatrists salivating over a fresh FND goldmine… you’re walking straight into disaster.
Tell every last one of them to f.ck off!
Then follow the hard, unfolding science.👇
Your organs don’t care about opinions. They only care about damage. And the damage is already stacking up, be it momentarily maybe still clinically "silent"! #AvoidSars2 #AvoidReinfections

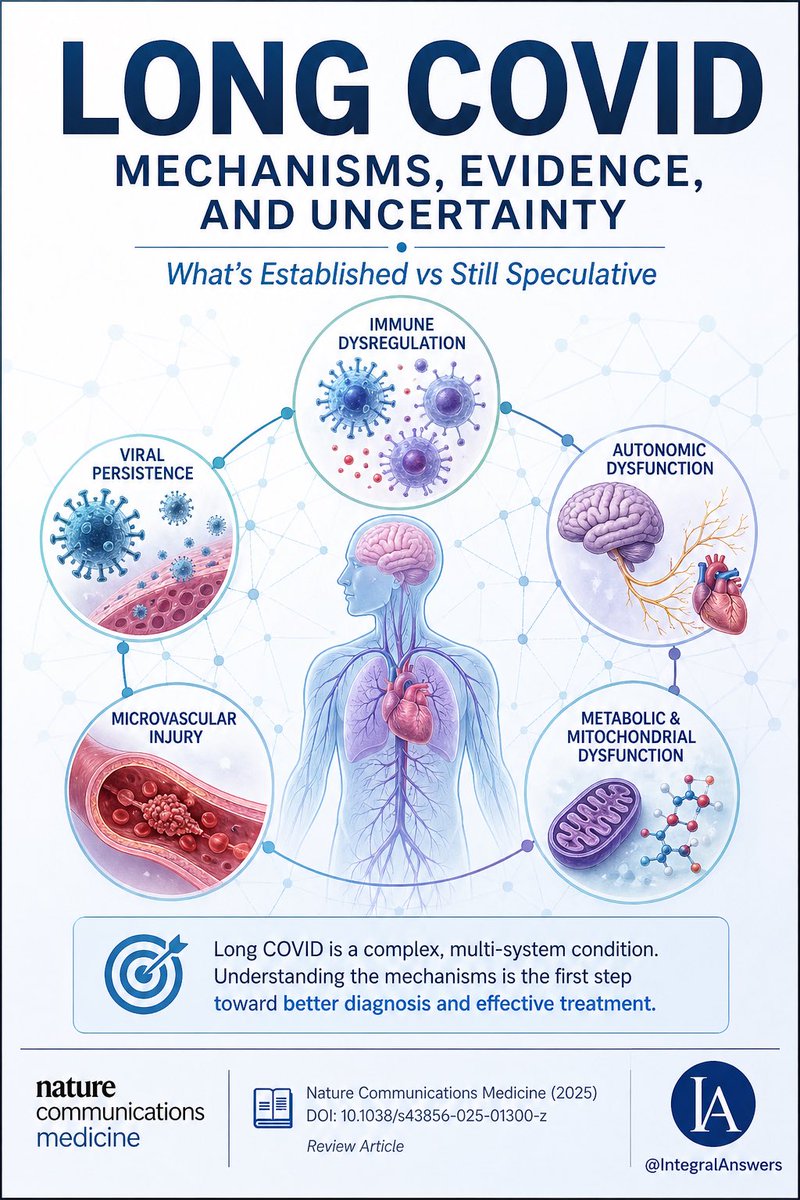
1/ Long COVID is one of the most complex post-infectious syndromes ever studied.
A new review in Nature Communications Medicine attempts to unify the biology.
Here’s what’s established, what’s emerging, and what’s still speculative. 🧵
38
506
1,127
34,883
Jun 3
🎯 From grace to disgrace doesn’t take long 😔
Jun 3

Sooner or later, almost every colleague, expert, institution, and idol disappoints us on this issue.
They almost have to.
Because accepting that COVID still poses meaningful risks would force a painful audit of years of assumptions, interpretations, and decisions.
It would require changing behavior.
It might require admitting mistakes.
It might require changing identity.
That’s a heavy lift.
Denial is lighter.
And that’s why it’s so popular.
2
2,463
Jun 2
“These countries maintain approximately 3.8 to 4.2 acute care beds per 1,000 population. Alberta has approximately 1.76 beds/1000, less than half.
This capacity gap, combined with blocked patient flow, is Alberta's fundamental healthcare challenge…Access is the problem.”
⬇️
Jun 1

Activity Based Funding Alone Will Not Fix Alberta's Healthcare Crisis:
Alberta is moving forward with Activity Based Funding (ABF), where hospitals and surgical facilities are paid according to the number and complexity of procedures they perform.
Let's start with an important point: this is not inherently a bad idea.
When properly designed, Activity Based Funding can improve efficiency, increase transparency, reward productivity, and reduce wait times for procedures such as cataracts, hip replacements, knee replacements, and day surgery.
High performing healthcare systems in Australia and Scandinavia have successfully incorporated versions of ABF into their funding models.
But those same jurisdictions teach us an important lesson.
They do not rely on Activity Based Funding in isolation. They pair it with robust investments in primary care, prevention, home care, rehabilitation, assisted living, long term care, community-based services, and significantly greater acute care capacity.
These countries maintain approximately 3.8 to 4.2 acute care beds per 1,000 population. Alberta has approximately 1.76 beds/1000, less than half.
This capacity gap, combined with blocked patient flow, is Alberta's fundamental healthcare challenge.
After 35 years in the front lines, I can say with confidence that once Albertans gain access to care, they generally receive world-class care. Access is the problem.
Every day, sick Albertans sit in crowded emergency department waiting rooms wondering why the system is failing them.
Many assume the problem starts in the emergency department. It does not.
The emergency department is where the failure becomes visible.
For decades, Alberta's population has grown faster than its healthcare capacity. Our population is aging, chronic disease is increasing, and medical care is becoming more complex.
At the same time, hundreds of patients who no longer require acute hospital care remain in hospital beds because they are waiting for home care, rehabilitation, transition units, assisted living, or long-term care.
Hospitals are designed to treat acute illness, not to house patients waiting for the next level of care.
Healthcare is fundamentally a flow system and we have a major flow problem, especially in the Edmonton zone.
Patients enter through primary care, emergency departments, and ambulance services. They move through hospitals and, when ready, back into the community through home care, rehabilitation, assisted living, and long-term care. When any part of that flow becomes blocked, the entire system slows down.
That is exactly what Albertans are experiencing today.
Hospitals function best at approximately 85% occupancy. Above that level, delays increase, flexibility disappears, and patient flow slows. When hospitals routinely operate at 100-110% capacity, they do not become more efficient, they become less safe.
The consequences are predictable and preventable.
Emergency departments back up. EMS crews wait to transfer patients into care. Admitted patients board on stretchers waiting for inpatient beds. Surgeries are delayed or cancelled. Patients may be discharged earlier than ideal because of bed pressures, increasing the risk of complications and readmissions.
Most concerning, the risk of medical errors rises when healthcare professionals are forced to work in overcrowded, high-pressure environments for prolonged periods.
Chronic overcrowding contributes to burnout, moral distress, absenteeism, staff turnover and less efficiency. Asking healthcare workers to function indefinitely in crisis mode is neither sustainable nor safe.
Public hospitals managing complex admissions, emergencies, and Alternate Level of Care patients cannot fairly compete in a pure activity-based funding model against facilities focused primarily on lower-complexity elective procedures.
Changing the funding formula will not solve these structural issues.
If Alberta is serious about improving access and reducing wait times, our priorities should be clear:
1. Retain, recruit, and support healthcare workers.
2. Expand acute care capacity, particularly in Edmonton, which serves a vast and underserved northern region.
3. Move Alternate Level of Care patients to the appropriate level of care within 24-48 hours whenever possible.
4. Expand home care, rehabilitation, transition units, assisted living, and long-term care.
5. Strengthen primary care, prevention, and community-based services.
The single most important performance measure in healthcare is not the number of procedures performed. It is how quickly patients receive the right care, in the right place, at the right time.
A patient who requires admission should move from the emergency department to an inpatient bed within six to eight hours, 90% of the time.
Even in the middle of summer, many Edmonton patients are waiting four to six hours simply to be assessed by a physician. Another respiratory virus season is only months away.
Activity Based Funding may improve surgical efficiency and deserves a fair evaluation. But Albertans should not mistake a funding reform for a healthcare solution.
Until we fix the bottlenecks at both the entry and exit doors of our hospitals, our emergency departments and inpatient wards will remain overcrowded and inefficient regardless of how hospitals are funded.
The biggest bottleneck in Alberta healthcare is not the operating room…It's patient flow…It's the hospital entry and exit door.
@ABDanielleSmith @nenshi @PfParks @JMeddings @raghu_venugopal @TheSGEM @TheBreakdownAB @RealTalkRJ @cspotweet @BradenMannsYYC @UCPCaucus @abndpcaucus
1
2
108
Jocelyn Lehman retweeted

I woke up this morning to see that my most recent Letter to the Editor was published in today's Edmonton Journal.
I you cannot read the font in the picture, here it is:
Saturday's letters: Referendum a waste of public money
This UCP government’s decision to pursue /2

47
126
319
8,262
Jocelyn Lehman retweeted

May 21
“Premier Danielle Smith and her party are beholden to the separatists who put them in power. Everything they do is subservient to that debt - without consideration for laws, Treaty obligations or the wellbeing of future generations.”
Treaty 6 would like a word.
#abpoli #cdnpoli
7
131
265
4,198
May 21
🎯 Thank you for highlighting facts
twisted = UCP failing to ‘remind’ folks that Forever Canadian exceeded the 10% burden based on the # of signatures required at the time.
🇨🇦 Citizens following closely were 💯 aware of intent
🌪️ UCP forever twisting to please the seppies

I’ll break it down:
1. Lukaszuk checked the POLICY box
2. He did not check the referendum box. 3. That’s the legal mechanism under the Citizen Initiative Act
4. He knew the UCP would violate the law
5. He added a caveat to protect Albertans
6. The UCP twisted his caveat.
2
24
Jocelyn Lehman retweeted

May 18
People who fear solutions should not be in charge of solutions.
6
37
211
1,921
Jocelyn Lehman retweeted

No “calm-mongering” by Dr. Donald Vinh, medical microbiologist & ID physician at McGill.
Bonus points for naming it, Andes hantavirus “spreads from person to person through droplets & aerosols”.
ctvnews.ca/video/2026/05/17/…
14
193
528
8,998
Jocelyn Lehman retweeted

Long COVlD "experts" giving unmasked testimony on the dangers of Long COVlD are as effective as thoracic oncologists warning of lung cancer while smoking cigarettes.
19
181
717
15,393
May 10
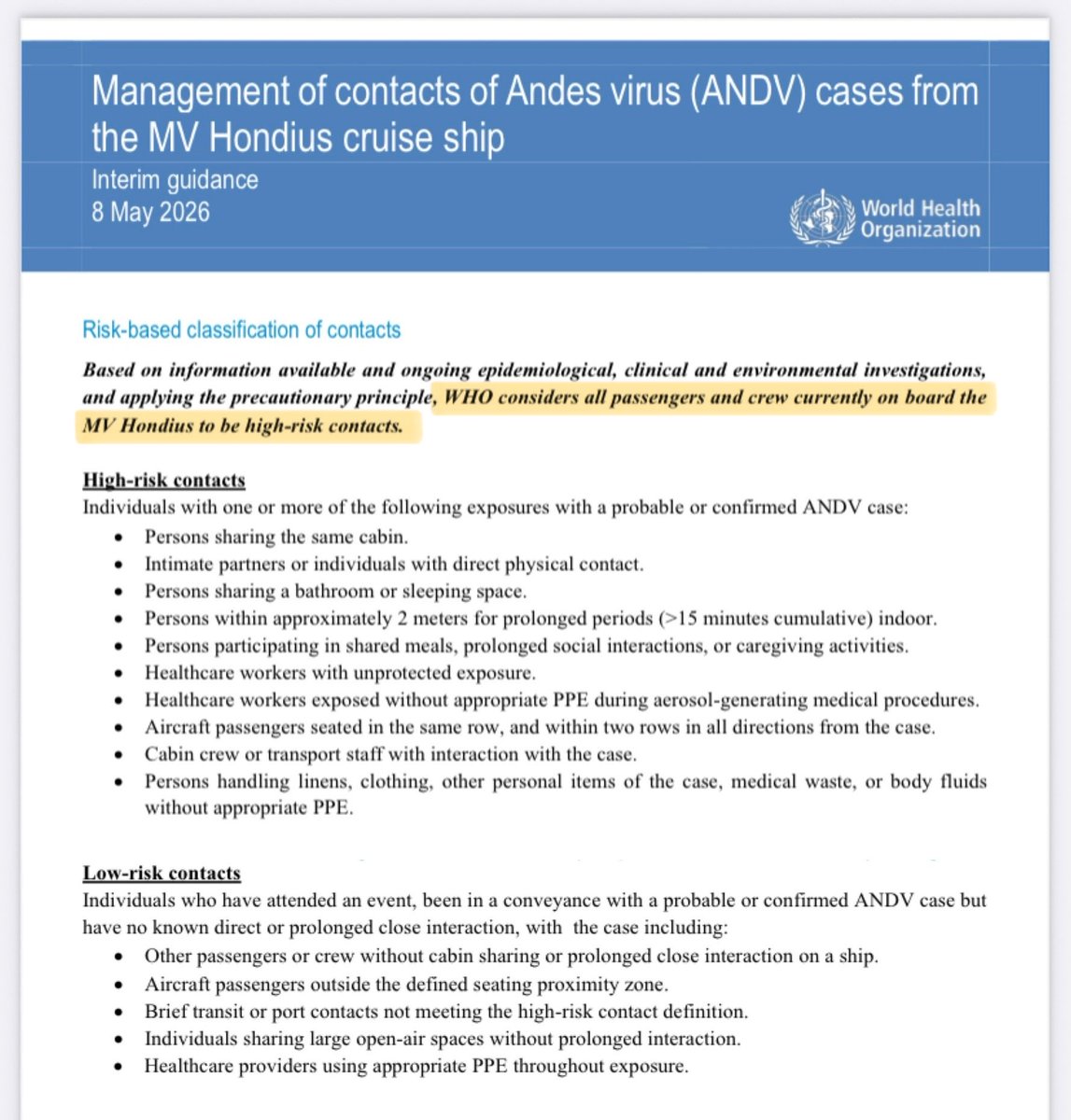
Better late than never ⬇️
High risk needs to be paired with ➡️accountability for those already put at risk on flights
➡️very clear guidance about protection for flight crew and HCPs monitoring repatriated high risk contacts

HANTAVIRUS OUTBREAK
Following my thread yesterday which criticised aspects of the WHO’s strategy, I’m pleased to see they’ve done a 180° turn in the updated guidance published today:
who.int/docs/default-source/…
EVERYONE from the ship will now be treated as HIGH-RISK contacts…
🧵
1
35
May 10
🚩 Apply precautionary principle to address lack of coordinated int’l response to evidence about: mode of H to H transmission; a variable incubation period & infectious phase that begins before symptoms. Expert PH overview on 🇦🇷 2018:
cbc.ca/listen/live-radio/1-5…
Read🧵@_CatintheHat
Final final point…
This is a virus with a case fatality rate of 30-50% - ie. up to HALF of those who catch it will die…
…and there are NO vaccines or specific treatments.
If those leading the response get this wrong, the implications will be fatal.
ukhsa.blog.gov.uk/2026/05/05…

35
May 10
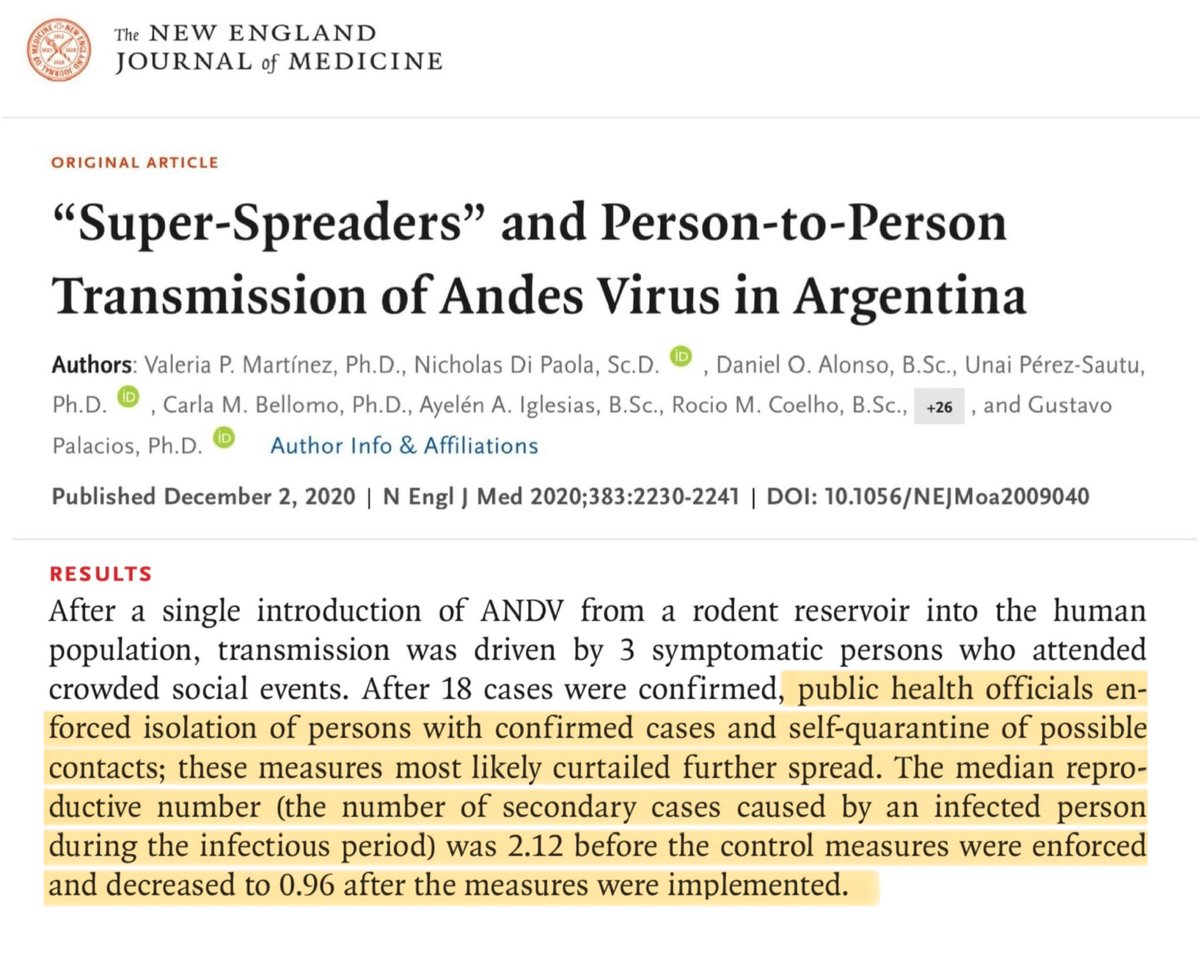
Demonstrating that there are choices between complacency & panic.
⬇️
Application of the precautionary principle
The lesson from the Argentina outbreak is not panic but precaution.
Their containment strategy (rigorous contact-tracing, isolation of all possible contacts, & use of N95 masks) successfully reduced the estimated R0 from 2.1 to below 1 and brought the outbreak under control.
20
Jocelyn Lehman retweeted
Clearly lessons from SARS2 have not been learned by PHAC. @GovCanHealth
Precautionary principle (PP) means until proven otherwise, assume all modes of transmission are possible including AIRBORNE.
PP means until proven otherwise, assume “infectious” even if asymptomatic!

Greatly appreciate all of my colleagues from across the Public Health Agency of Canada who expedited this Rapid Risk Assessment for Andes virus👇
canada.ca/en/public-health/s…
6
93
249
4,493
Jocelyn Lehman retweeted

People keep trying to frame every outbreak as the next COVID instead of recognizing what’s actually happening.
Ecosystems are being bulldozed apart and pathogens are exploiting the gap.
This Hantavirus outbreak is a case study in what happens when deforestation, habitat disruption, climate pressure, and human expansion shove rodent reservoirs directly into human environments
24
348
1,679
29,026
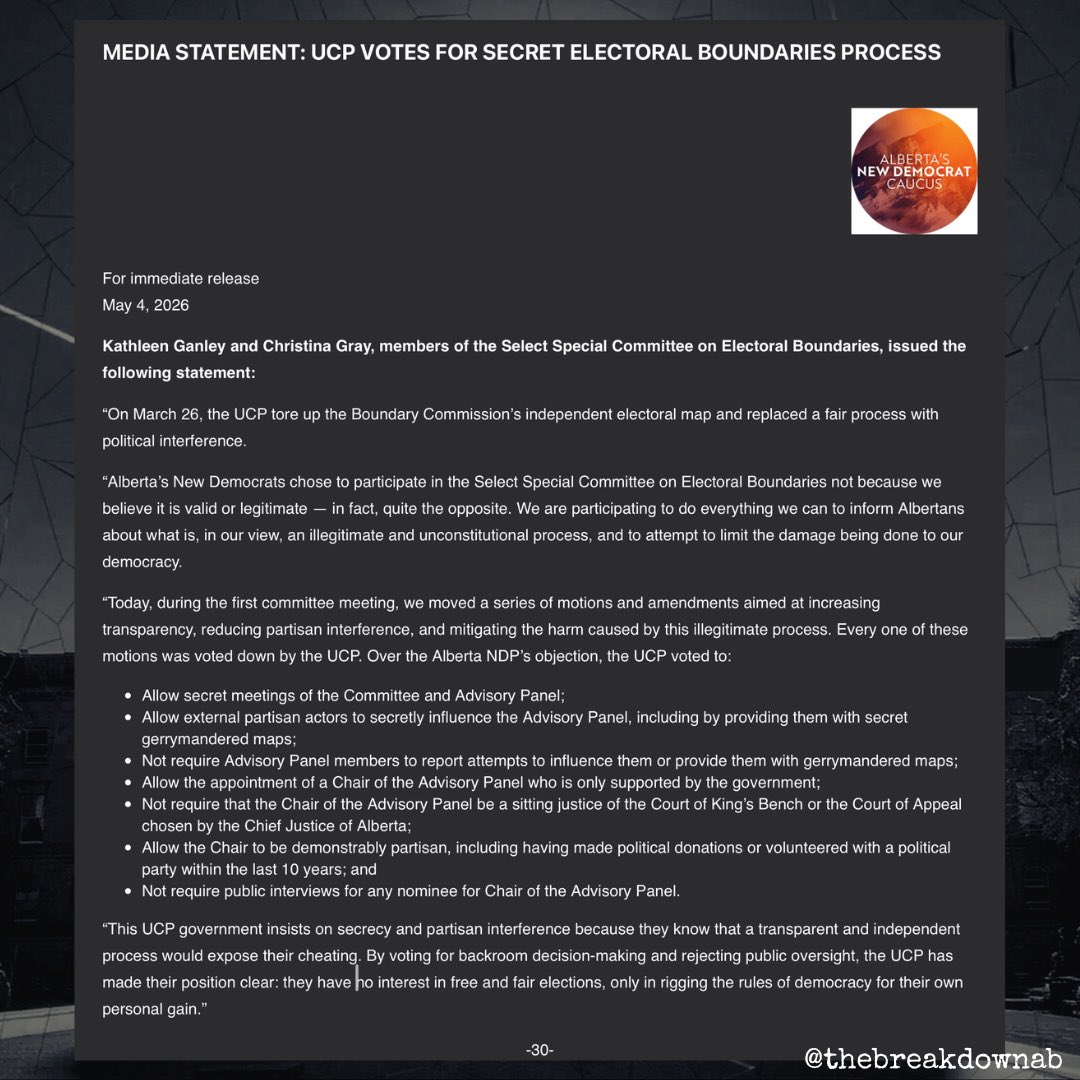
May 5
Read it, weep for the loss of fair & democratic processes and share widely.
May 4

🚨BREAKING!🚨
Never to let a good crisis go to waste, the UCP are clearly taking advantage of the separatist data breech scandal to run the table on electoral boundaries.
Secret meetings?
Secret Maps?
Every Albertan should read this!
#abpoli #ableg #cdnpoli
1
13
Jocelyn Lehman retweeted

May 4
The only possible way that the separatist petition should even be considered by @ElectionsAB is if every single signature is personally verified with every single signee.
Full Stop.
If you agree please repost.
114
823
1,454
15,506
Jocelyn Lehman retweeted

If you follow me, it's probably because I followed you first, and you followed back. So I know you are active.
But give a shout if you know that #CovidIsNotOver

ALT Man wearing black respirator mask.
May 2

The reason I’m interested in doing this because people overestimate how many of the followers are still active, especially if they grew in a prior era (e.g., COVID, etc)
169
167
1,779
27,236
Apr 30
I like the suggestion to print it and share w/ PCP to try and move the needle on getting research to practitioners.
Apr 30

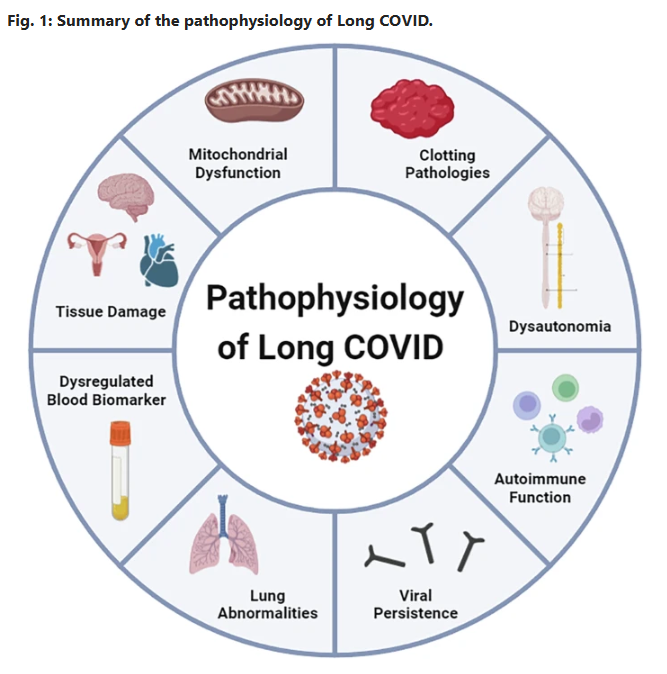
Current status and future perspectives on the mechanistic and pathophysiological understanding of long COVID
🚨JUST DROPPED YESTERDAY and rips open the black box of Long COVID:
Viral persistence up to at least 24 months. Fibrin microclots that laugh at fibrinolysis. Autoimmune storm. Mitochondrial sabotage. An up-to-date full mechanistic map is finally here!
No more guessing. This changes everything, let’s dig into this overview👇, better yet…..read it yourself!! #MustRead
➡️Global Impact & Context:
- Long COVID (PASC) affects >400 million people worldwide, incurring >$1 trillion in annual economic costs,
- Core symptoms, debilitating fatigue, cognitive dysfunction (“brain fog”), sleep disturbances, and post-exertional malaise (PEM) in 50–80% of cases, persist months to years’ post-infection, with a mechanistic overlap to ME/CFS,
➡️Core Mechanisms:
1. Immune Dysregulation:
- Persistent systemic inflammation features elevated cytokines (IL-6, TNF-α, IL-1β) detectable up to 14 months, driving T-cell exhaustion (reduced CD8 IFN-γ/TNF-α production) and monocyte activation (COX-2, IL-8Rβ, CXCR6),
- Autoantibodies (anti-GPCR, anti-PITX2, anti-FBXO2, ANA/ENA) persist 12–14 months and correlate directly with fatigue, dyspnoea, palpitations, and cognitive impairment with molecular mimicry, gut dysbiosis and latent herpesvirus reactivation (EBV, HHV-6) amplifying autoimmunity,
2. Viral Persistence & Reactivation:
- SARSCoV2 RNA, spike protein, and antigens remain detectable in brain, muscle, gut and plasma up to 14–24 months in ~60% of cases, fuelling chronic low-grade inflammation,
- EBV/CMV reactivation signatures are common with spatial transcriptomics highlighted as a possible next tool to map tissue reservoirs,
3. Endothelial/Microvascular Pathology:
- Glycocalyx shedding (elevated SDC-1), capillary rarefaction and endothelin-1 elevation create a pro-thrombotic state,
- Platelet hyperactivation releases vWF/FVIII, forming anomalous fibrin(ogen) microclots that resist fibrinolysis and these circulate and fragment during exertion, causing hypoxia, ischaemia-reperfusion injury, and PEM,
4. Autonomic Dysfunction:
- Present in ~50% of patients (POTS predominant), driven by hypovolaemia (70%), small-fibre neuropathy (20–40%), vagus-nerve damage and microclot-induced compensatory tachycardia with 4-fold norepinephrine spikes,
5. Mitochondrial Impairment & Neuroinflammation:
- Skeletal-muscle biopsies show reduced respiration, cytochrome c oxidase activity and WASF3-mediated supercomplex disruption, producing rapid lactate rise and PEM within 48 h,
- Systemic cytokines breach the blood–brain barrier, sustaining microglial activation and cognitive sequelae,
➡️Diagnostic & Therapeutic Gaps:
- No validated biomarkers or subtype-specific criteria exist.
- Graded exercise is contraindicated.
- Observational promise exists for IVIg, low-dose naltrexone and apheresis, but large RCTs are urgently required.
➡️Future Priorities:
Calls for subtype-specific research, large-scale RCTs, advanced techniques (spatial transcriptomics, proteomics), and interdisciplinary collaboration to develop precision diagnostics and therapies.
‼️This exceptional review delivers a masterful, evidence-based roadmap that not only clarifies Long COVID’s complex pathophysiology but stimulates the scientific community toward urgently needed mechanistic breakthroughs and effective, patient-centred interventions.
‼️Bottom line: Long COVID is not a single disease but a complex, multisystem condition that can impact your life seriously!
#AvoidSars2 #AvoidReinfections
A huge thanks to all authors, @DrMark_Faghy @DavidJoffe64 @PutrinoLab @DaniBeckman @resiapretorius @Sunny_Rae1 are only some of them!👏👏
nature.com/articles/s43856-0…
1
36