
🔬MD Pathologist | Big fan of Dunning-Kruger | Interests : Oncopath and BST | Give me a bone slide and make my day | T/Rt = educational 🚫 medical advice
Joined August 2017
- Tweets 285
- Following 442
- Followers 378
- Likes 466
97 Photos and videos





Pinned Tweet

17 Dec 2023
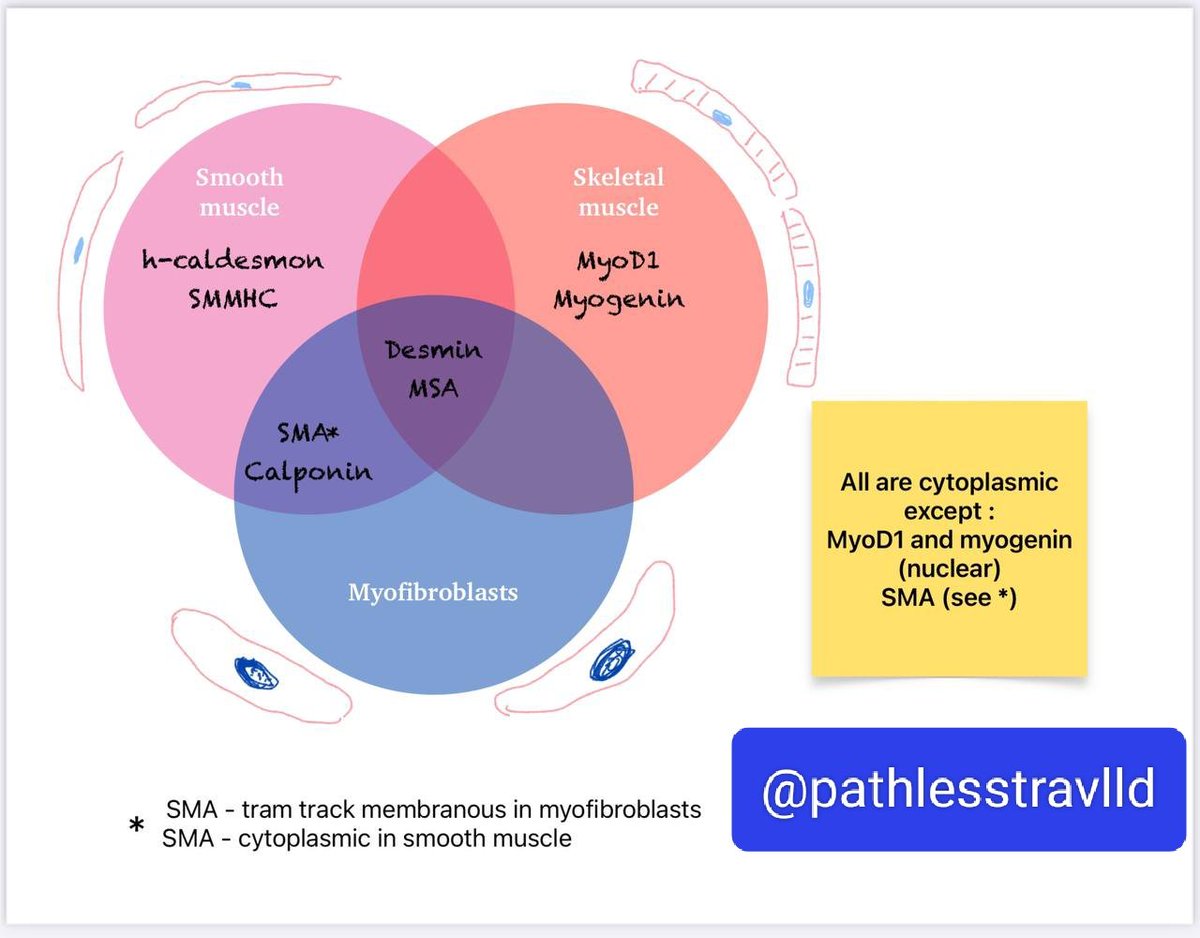
I always thought #IHCPath would be so much simpler with the help of Venn Diagrams
#bstpath #pathology #pathX #pathtwitter
5
26
76
6,644
Dr Ashish Kawthalkar retweeted

1 Apr 2025
Summary of conversations on social media, including Twitter (X), Facebook, and LinkedIn, which have evolved over the past 72 hours April 1 2025
Reimagining WHO Tumor Classifications: A Global Call for Equity
This piece summarises conversations on social media, including Twitter (X), Facebook, and LinkedIn, which have evolved over the past 72 hours. It is incomplete but offers a snapshot for those who may not have followed the full conversation.*
A growing conversation has erupted in the pathology community online, catalysed by concerns about equity in global cancer classification. Prompted by a tweet from Dr. Vikram Deshpande, this conversation critiques the growing reliance on molecular diagnostics in the WHO Blue Books and its impact on the vast majority of the world that lacks access to such resources. What began as a singular concern quickly unfolded into a global debate about representation, access, and the mission of the WHO.
Their collective insight has shaped a chorus of perspectives challenging the practicality of a classification system whose implementation depends on expensive, inaccessible molecular tests. These are not critiques of science or innovation but call for a balanced approach that values practicality and equity alongside advancement.
Central to the discussion is the concern that WHO tumour classifications, while intended to standardise cancer diagnosis globally, are increasingly aligned with high-resource settings. This misalignment creates a two-tiered system: one where wealthy institutions can implement precise, genomics-informed diagnoses, while much of the Global South is left behind, often defaulting to ambiguous "NOS" (not otherwise specified) labels due to the lack of infrastructure.
Dr. Deshpande and others argue that this contradicts the founding principles of the WHO, which was established in 1948 to promote global health equity. The WHO Constitution affirms that health is a fundamental human right and that unequal health development is dangerous to all. Yet the books meant to standardise cancer care may unintentionally deepen disparities.
Many contributors, including those with long experience in pathology across both resource-rich and resource-limited contexts, emphasised that their critique is related to structural issues in the IARC. Several noted that although some pathologists from the Global South have been added to WHO editorial committees, they remain underrepresented relative to the global cancer burden. As of the latest count, only 4 out of 20 WHO Standing Editorial Committee members are from the Global South, even though approximately 85% of the world's population lives there. This ratio has improved from the previous edition, which had just one member from the Global South but remains imbalanced.
Another key theme was the overreliance on molecular diagnostics, often without clear therapeutic implications. Contributors questioned whether creating finer subtypes based solely on genetic profiles meaningfully improves outcomes. For many cancers, these distinctions remain academic, especially in countries where even essential chemotherapy is hard to access. As several participants put it, "A diagnosis delayed is a diagnosis denied," pointing to the real harm caused by waiting weeks or months for complex tests that often don’t change management.
Alternatives were proposed. One idea that gained traction was reimagining the WHO Blue Books in a tiered structure: a primary volume focused on diagnostic features that can be assessed with H&E stains and basic IHC, accessible in most countries, and an annexe or supplemental volume incorporating advanced molecular classifications. This approach would allow for global standardisation without sacrificing equity.
Artificial intelligence was also raised as a potential equaliser. AI models trained on digital pathology slides may be able to predict mutations or tumour types from morphology alone, offering high diagnostic accuracy without molecular assays.
Further complicating matters is the price of WHO Blue Books themselves. A $109 annual subscription may be reasonable in the U.S., but it is unaffordable in countries like India or Nigeria when adjusted for purchasing power parity. Ironically, the pathologists least able to implement the classifications are paying disproportionately more to access them.
Several participants stressed the need for authors and editors of WHO chapters to spend time in low-resource settings before drafting guidelines. "Until you sign out cases in a district hospital with no access to molecular testing," one tweet said, "don’t write another chapter." Others emphasised the importance of humility and listening, particularly when creating documents that function as global standards.
Finally, many emphasised that these discussions are not meant to hinder scientific progress. The WHO’s role is not to document the latest science; its mandate is to promote health equity. That distinction matters deeply when publishing documents that shape cancer care in every country.
Critics of this position also made their voices heard. Some argued that advocating for simplified, resource-conscious classifications risked "dumbing down" pathology and hampering scientific progress. They warned that instead of slowing down to meet current limitations, the focus should be on raising global capabilities, expanding infrastructure, and investing in training. One widely shared concern was that limiting advanced classifications could risk entrenching a two-tiered system by perpetuating inequality rather than solving it. They argued that progress should not be impeded but made more inclusive and accessible.
In sum, this thread reflects a collective realisation: if WHO classifications are to fulfil their mission, they must prioritise global applicability over academic perfection. The time to act is now before further editions deepen the divide. As one pathologist tweeted, "Perfect classification is an illusion. Equity shouldn’t be."
These discussions will continue, both online and in formal academic venues. The hope is that with more inclusive authorship, practical frameworks, and a renewed focus on the WHO’s core mission, tumour classification can serve everyone—not just the privileged few.
1
12
38
3,128
Dr Ashish Kawthalkar retweeted

23 Feb 2025
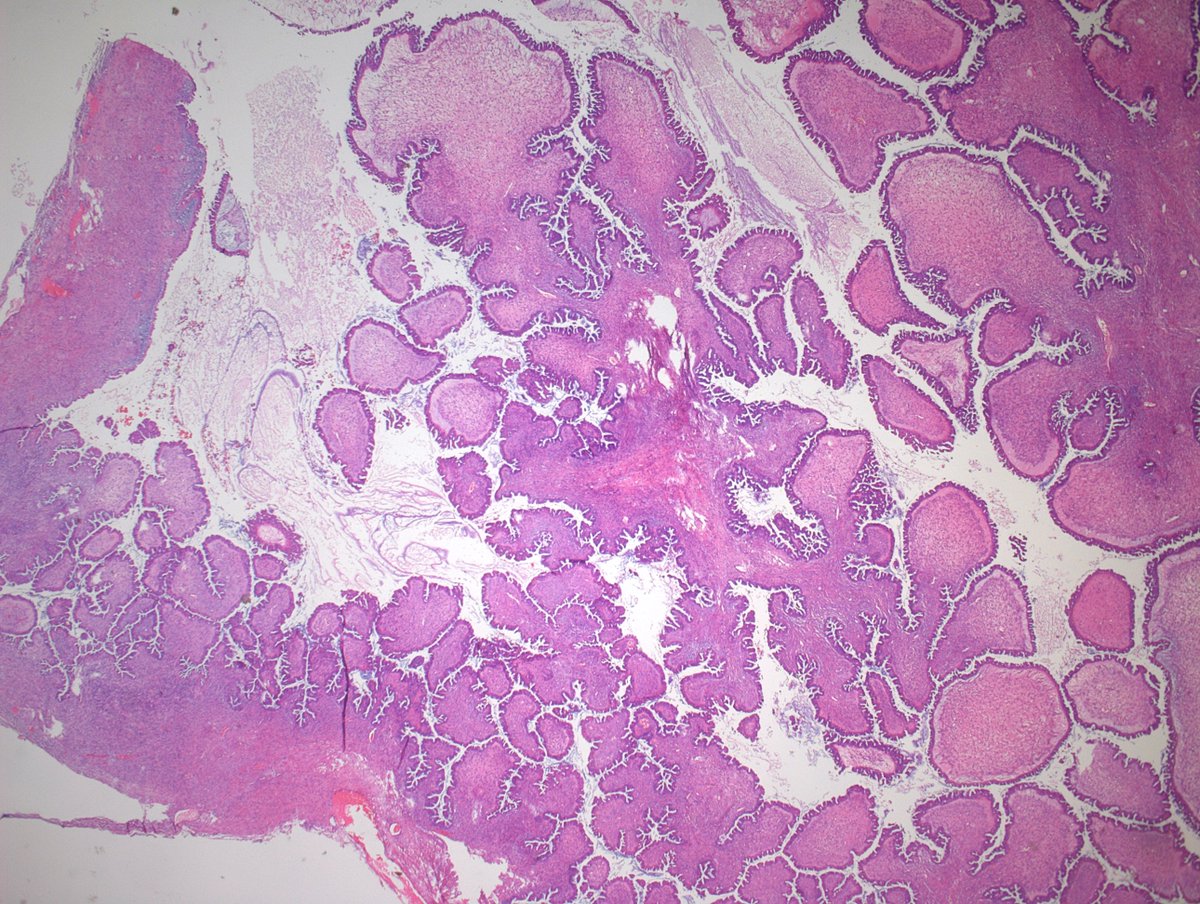
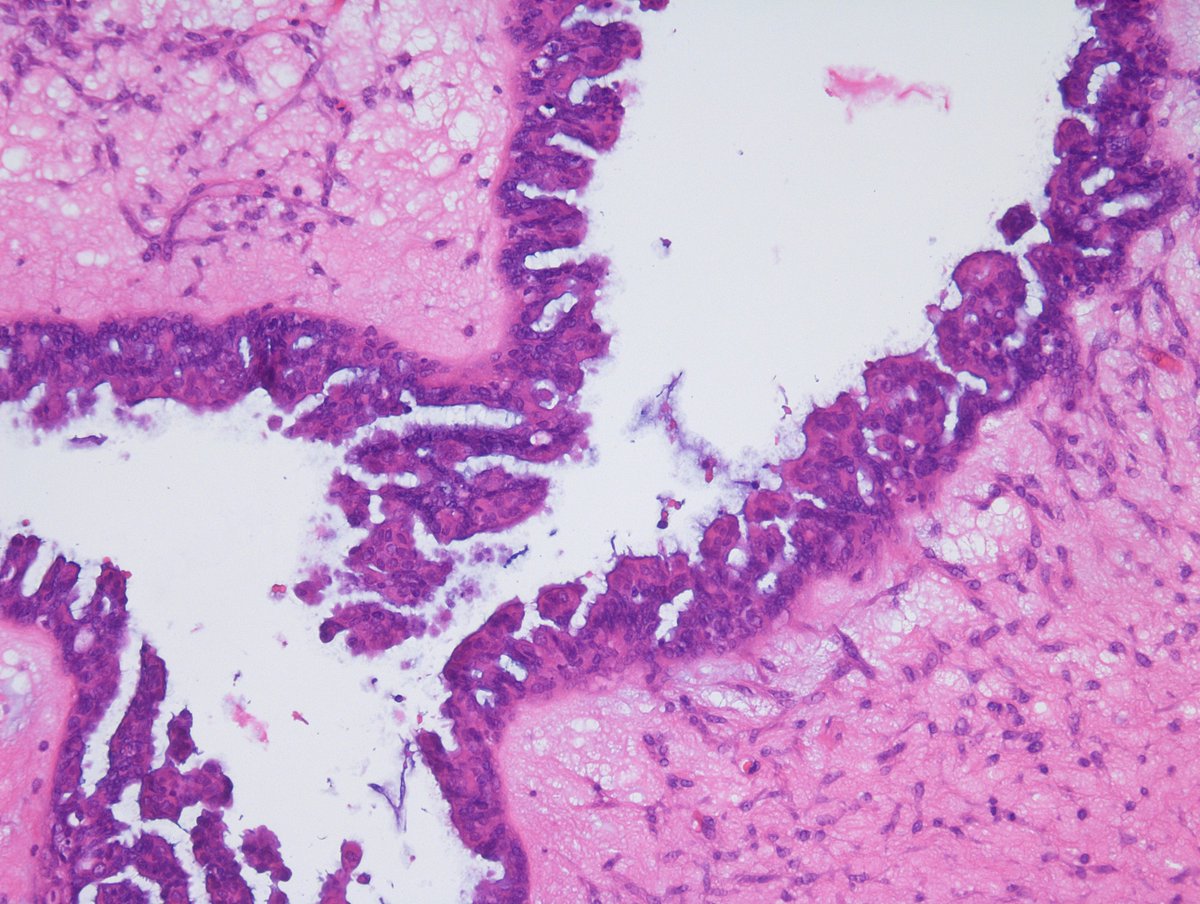
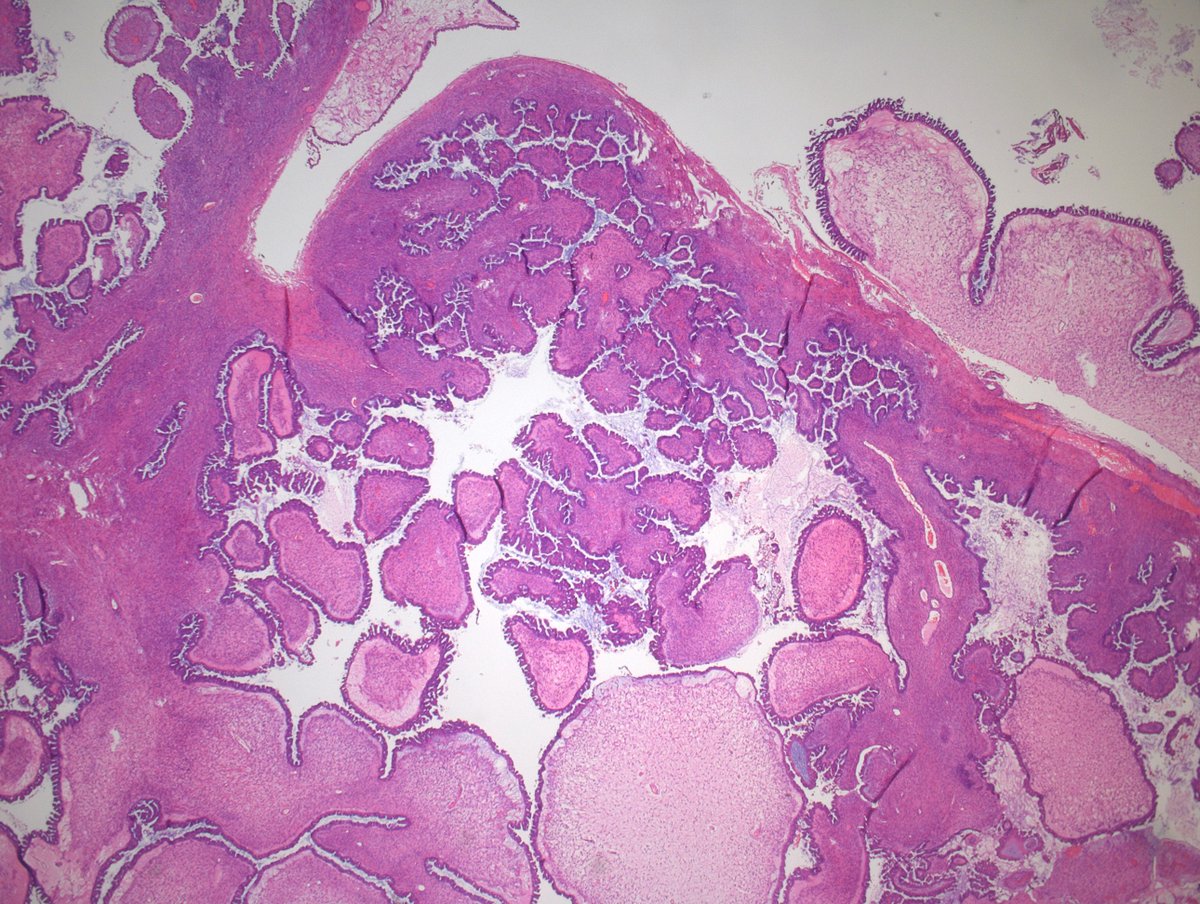
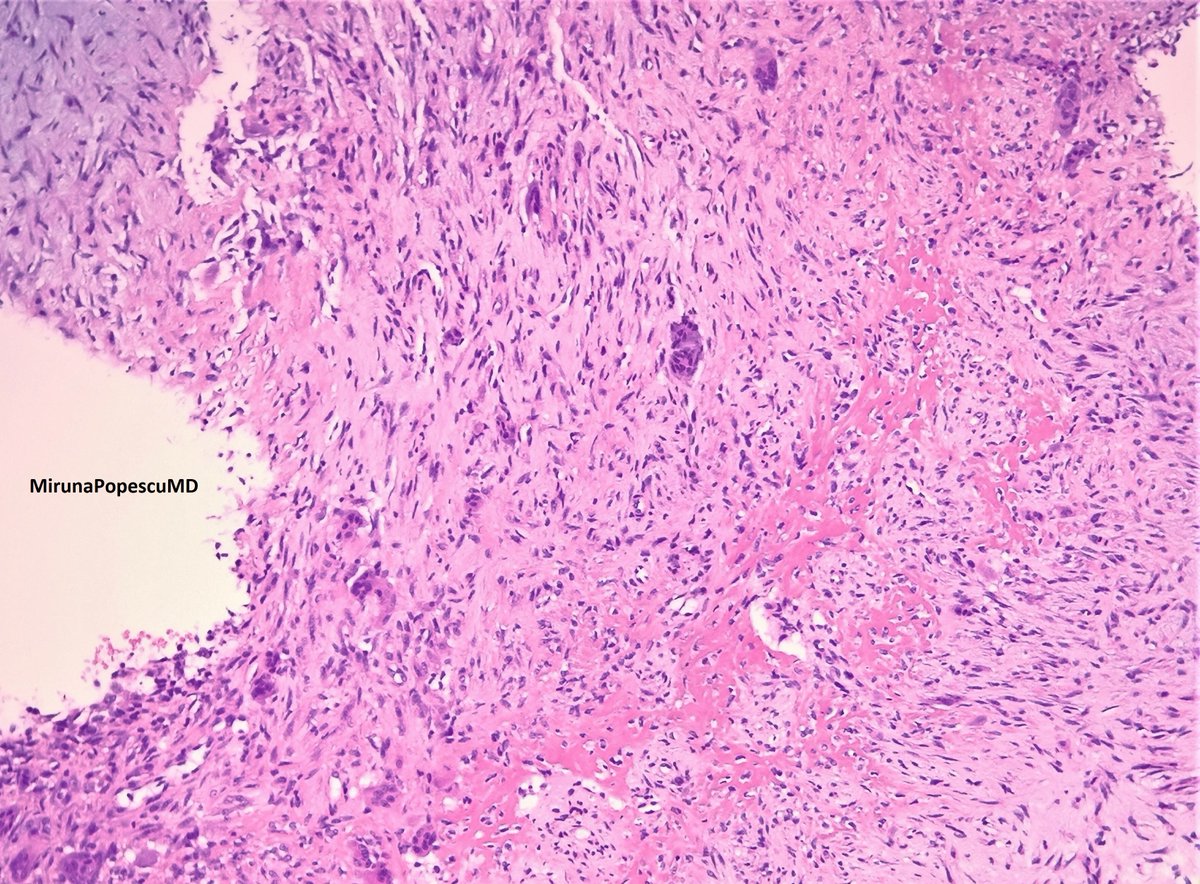
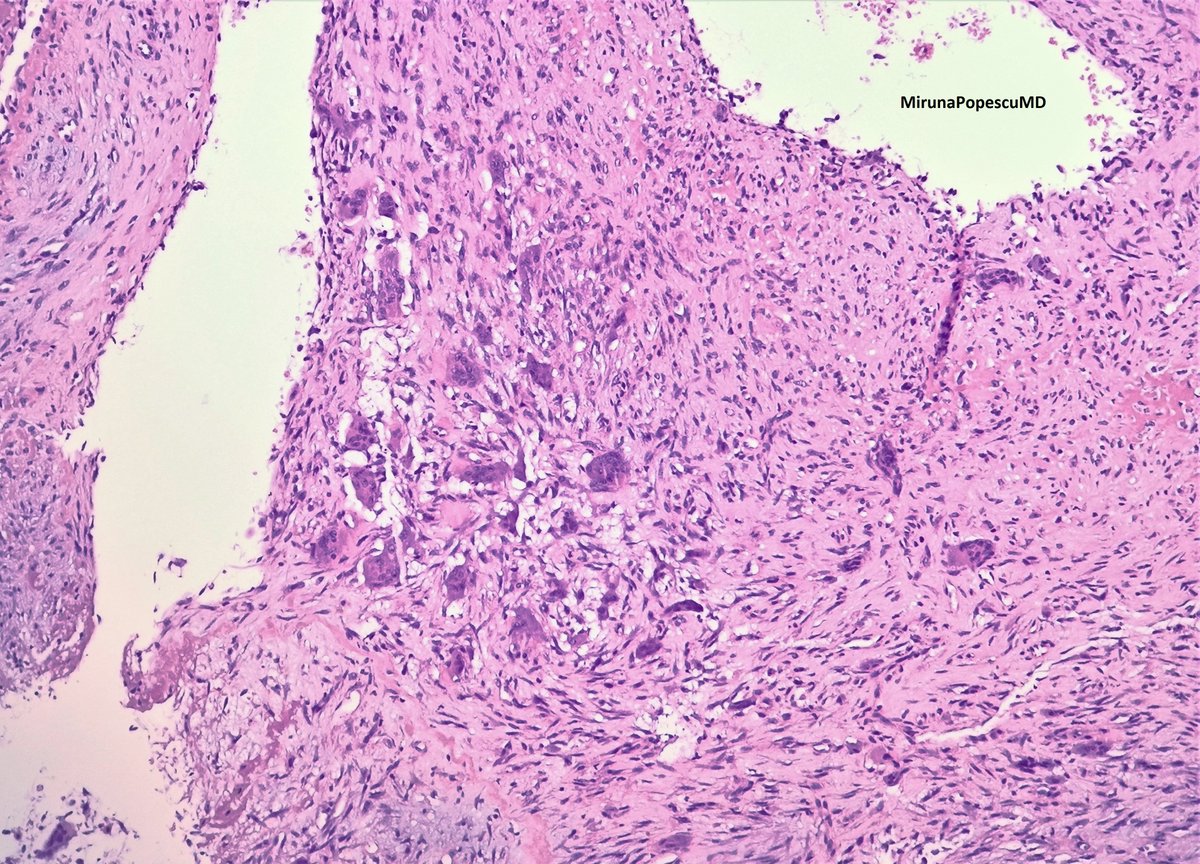
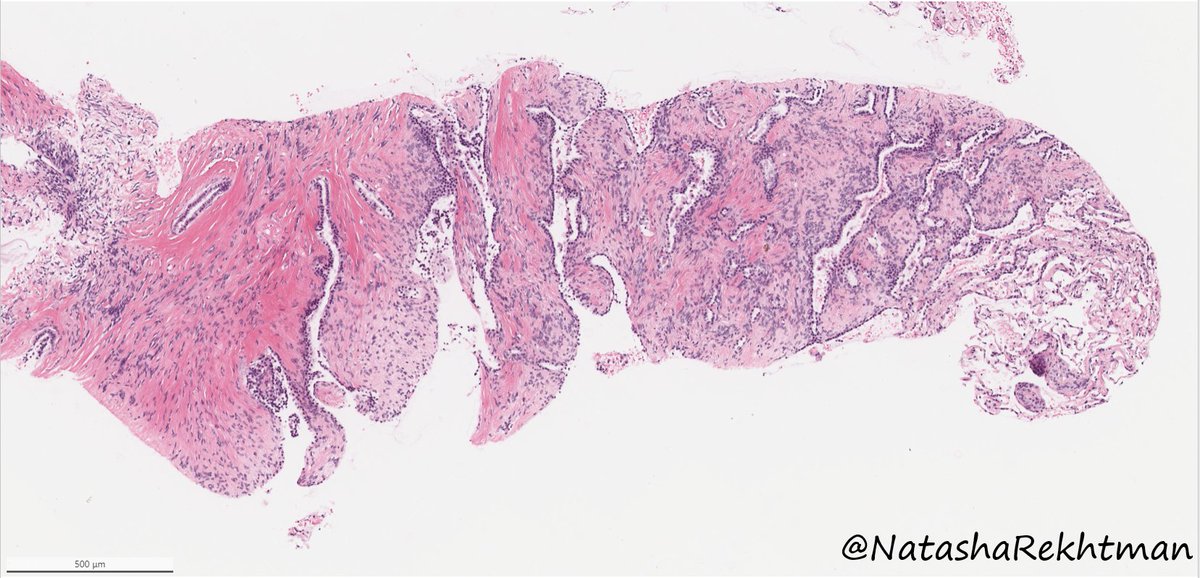
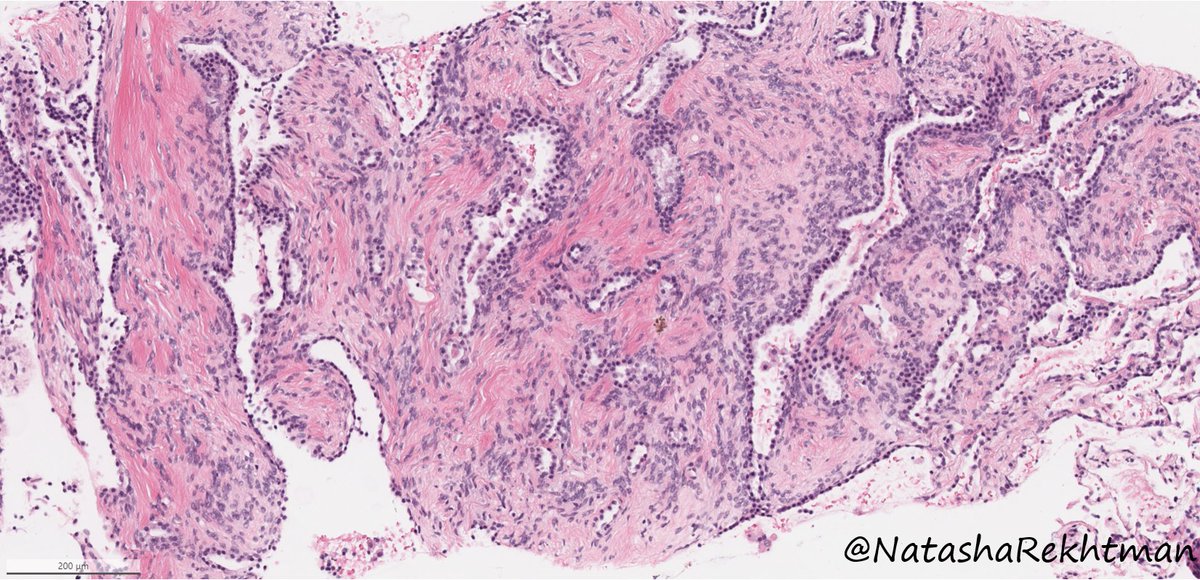
Ovarian serous borderline tumour (SBT)
3 essential features:
- hierarchical branching pattern
- papillae with fibro-myxoid core
- pseudostratified ciliated cells with tufting and exfoliation
photo credit: @MirunaPopescu13
#PathTwitter #gynpath #pathresident #pathoutpic
15
53
2,205
Dr Ashish Kawthalkar retweeted

11 Jul 2024
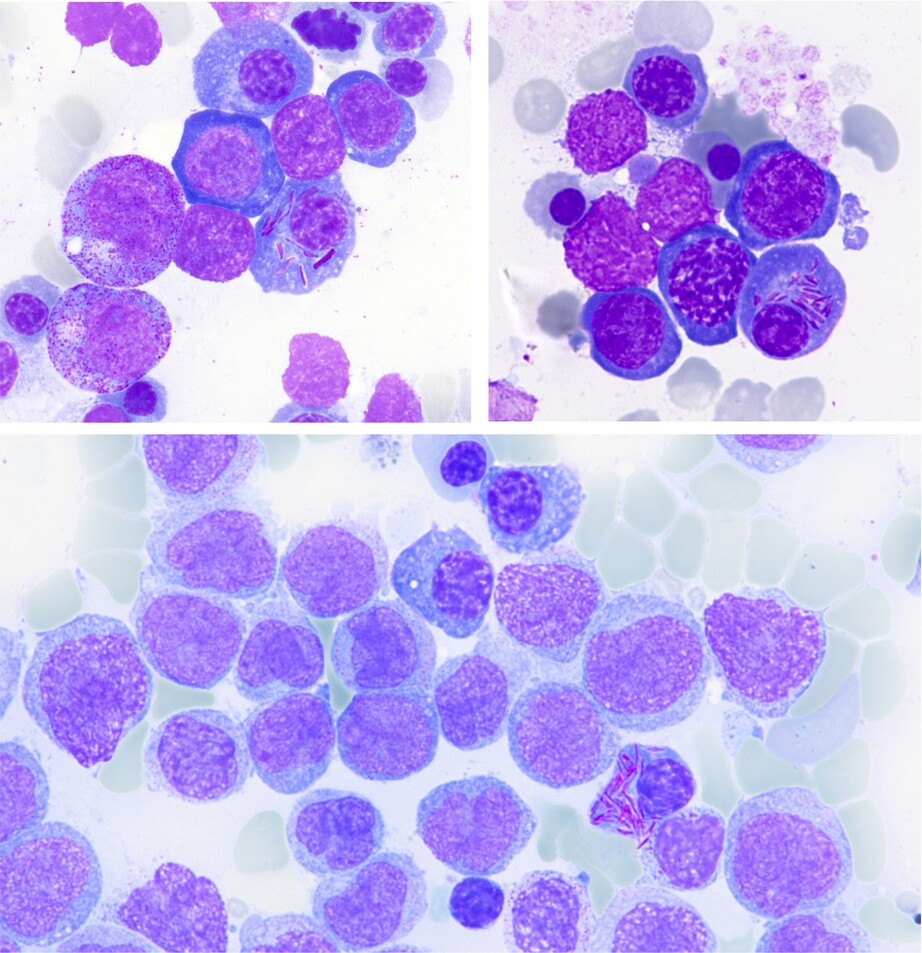
Plasma cells with Auer-rod-like inclusions in a patient with MGUS and acute myeloid leukaemia with NPM1 mutation |British Journal of Haematology | Wiley Online Library onlinelibrary.wiley.com/doi/…
1
52
133
9,725
Dr Ashish Kawthalkar retweeted

7 May 2024
@slusagar hats off, sir! 💯nailed it
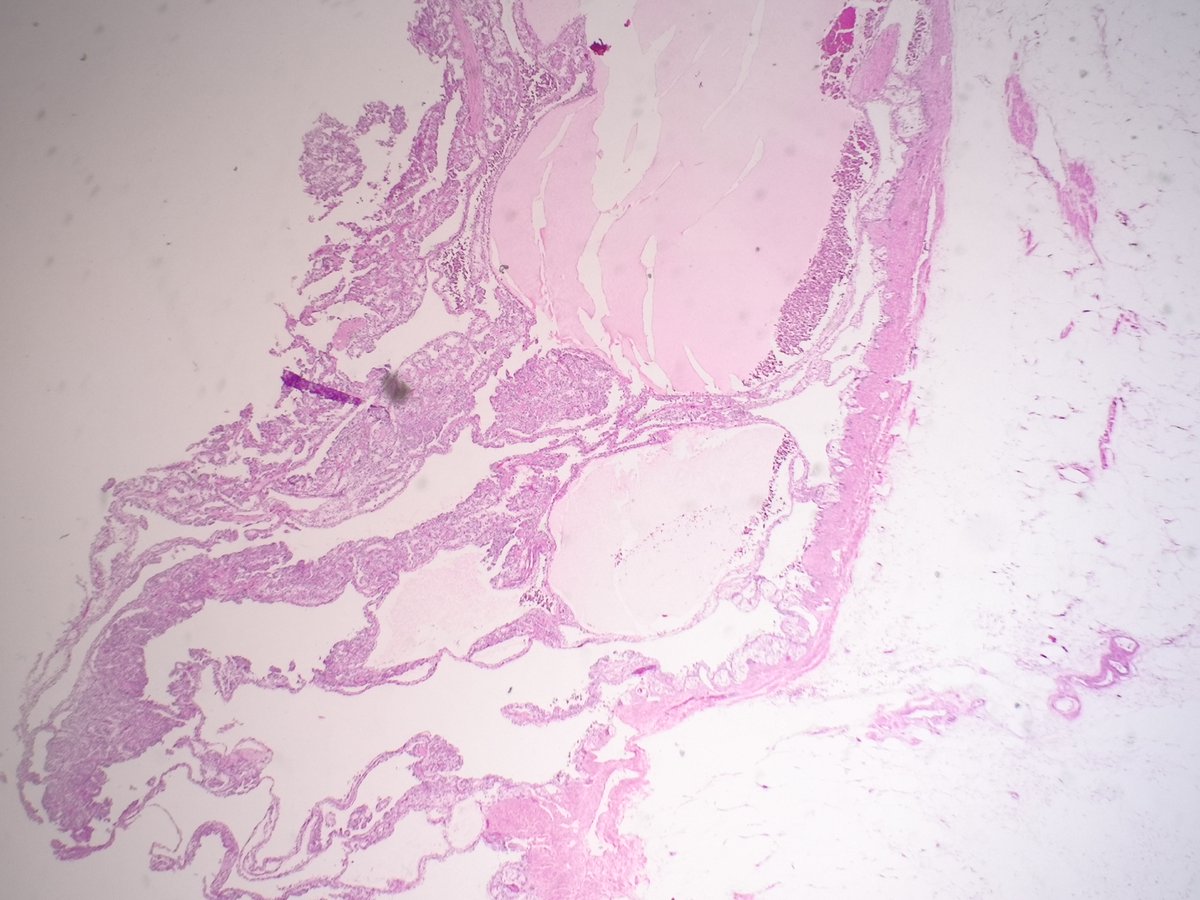
✅MED15::TFE3 RCC
Majority 👉🏼multilocular cystic
Mimicker of MCNLMP (PMID: 36997032), CCPRCT, and cystic CCRCC.
Like CCPRCT & other TFE3-rearr. cousins (NONO::TFE3, SFPQ::TFE3) shows 🎹apical oriented nuclei.
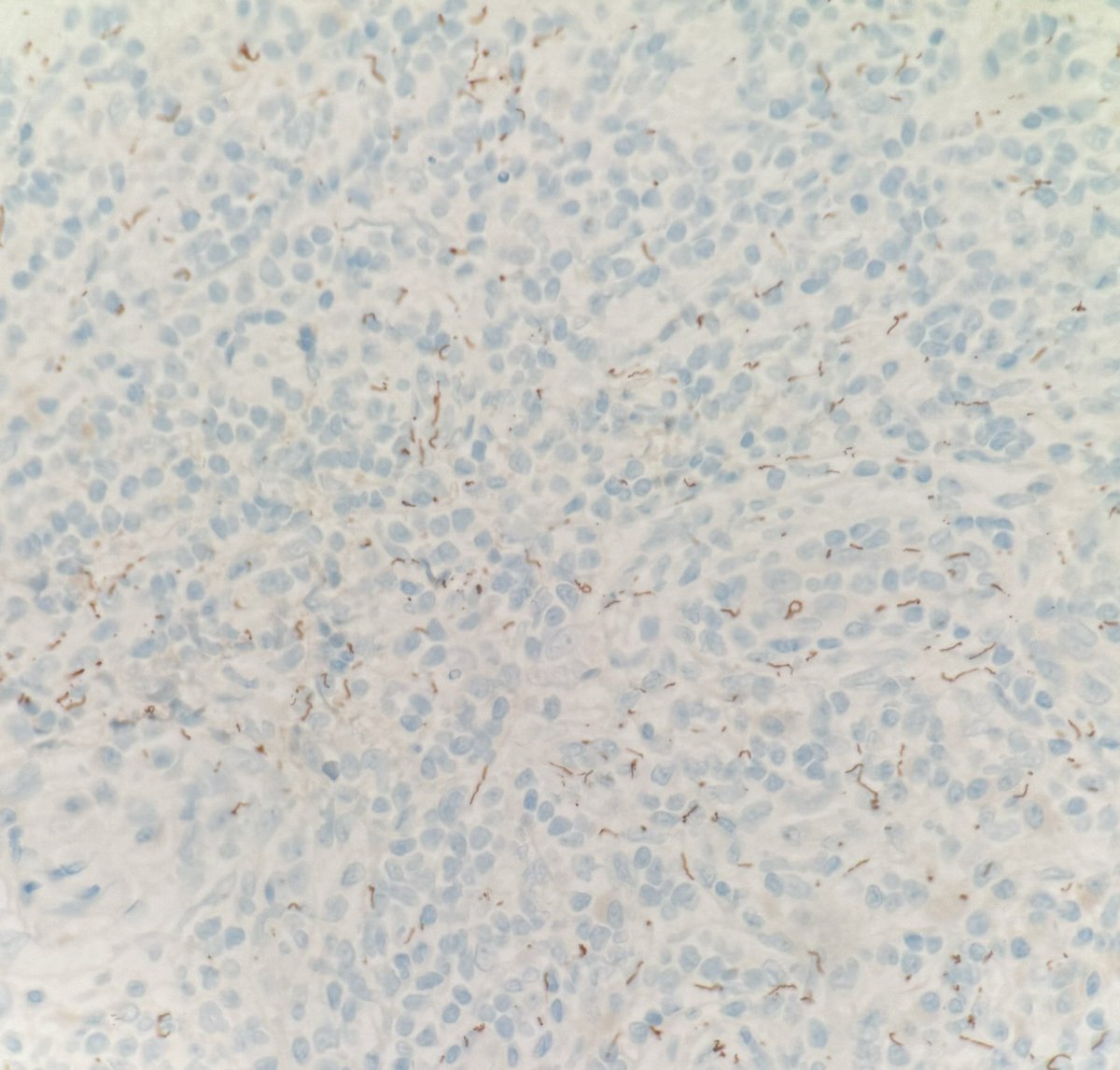
TRIM63 👉🏼specifically ⬆️expressed in majority of MiTF-RCC.
Combo TRIM63 RNA-ISH TFE3/TFEB FISH improves detection of MiTF-RCC, including FISH false-neg. paracentric inversion fusion variants RBM10::TFE3, RBMX::TFE3, NONO::TFE3.


5
9
45
2,780
Dr Ashish Kawthalkar retweeted

10 Apr 2024
Everyone is spot on. Treponema IHC is stunning. We now have enough control tissue for years.
10 Apr 2024

Elderly male with lesion on foreskin and glans. Not all inflammation is BXO! Great diagnosis by Dr Capleton while I was at USCAP/Hols! What one IHC do you want? Answer later!!!
1
7
28
5,127
Dr Ashish Kawthalkar retweeted

31 Mar 2024
Which fungus🍄 = crushed🏓⚪️?
A) Pneumocystis
B) Blastomyces
C) Cryptococcus
D) Coccidioides
🖼️🙏Dr. Carol Farver
#CrittersOnTwitter #PathBugs #PathTwitter #PathResidents #PulmPath

3
13
49
7,369
Dr Ashish Kawthalkar retweeted

5 Dec 2022
Picture this:
A young boy presents with mononucleosis, and you find this 👇 on your evaluation.
Why (and how) is this happening? 🤔
🧵 1/8

ALT Icteric tongue
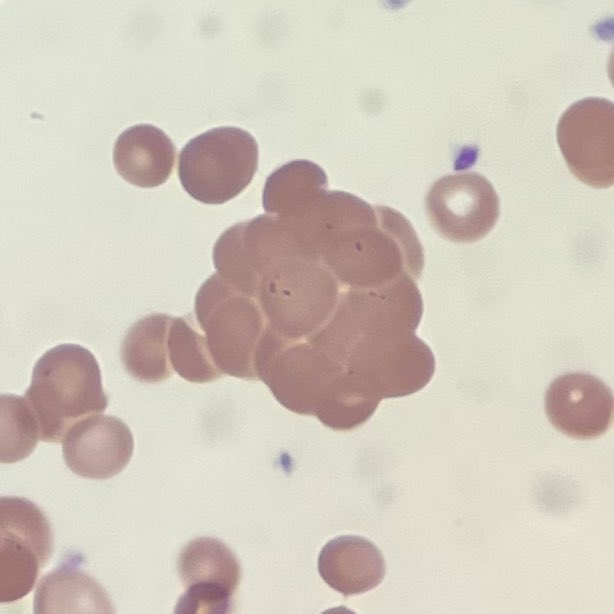
ALT Red blood cell agglutination
11
151
935
Dr Ashish Kawthalkar retweeted
21 Jan 2023
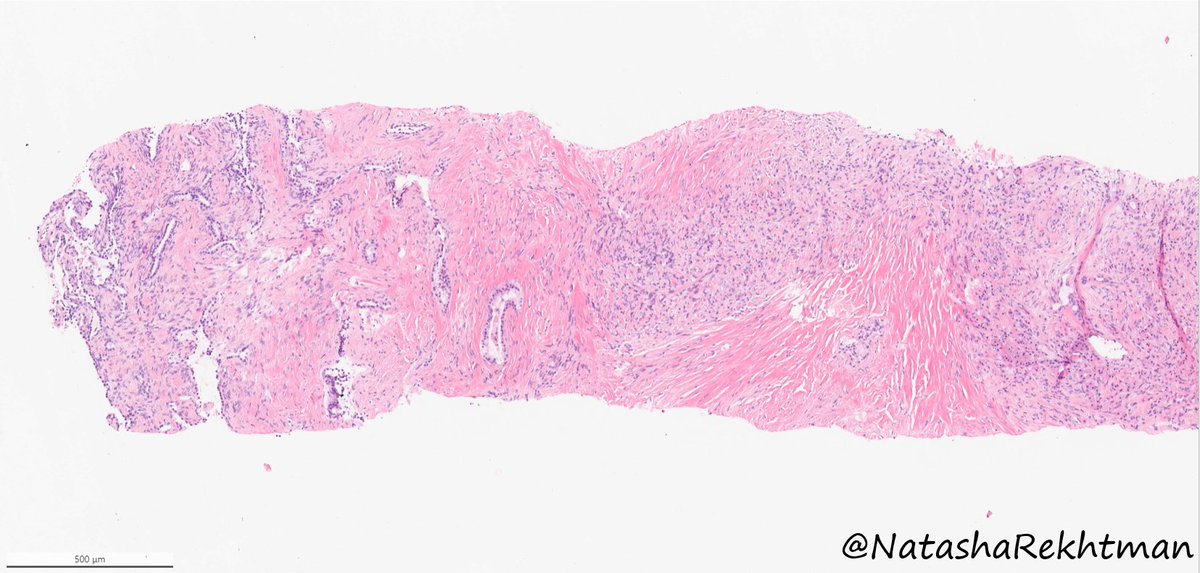
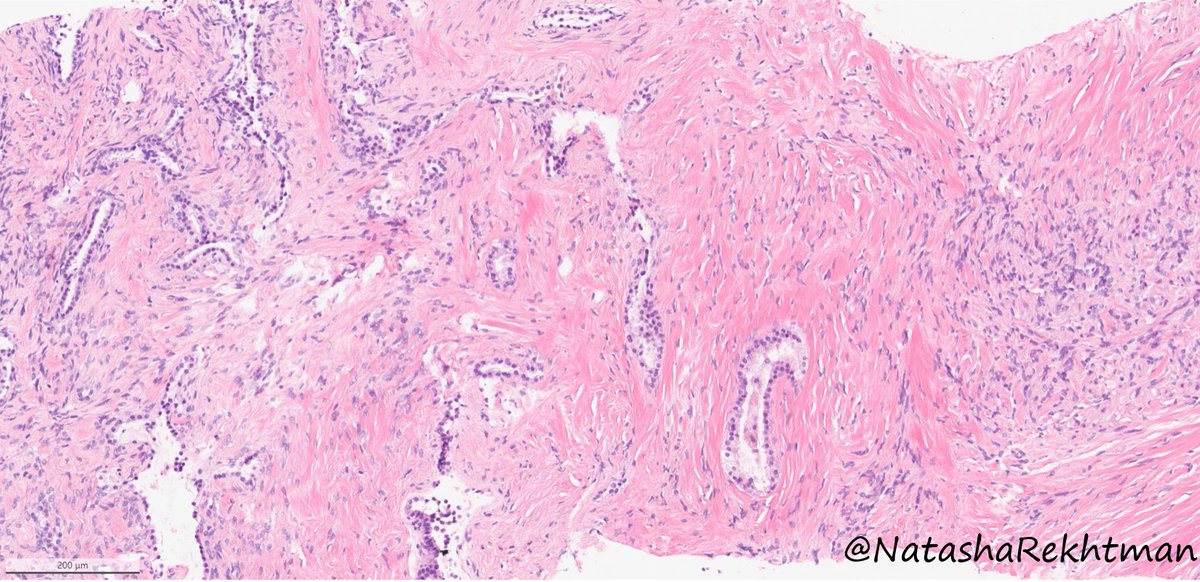
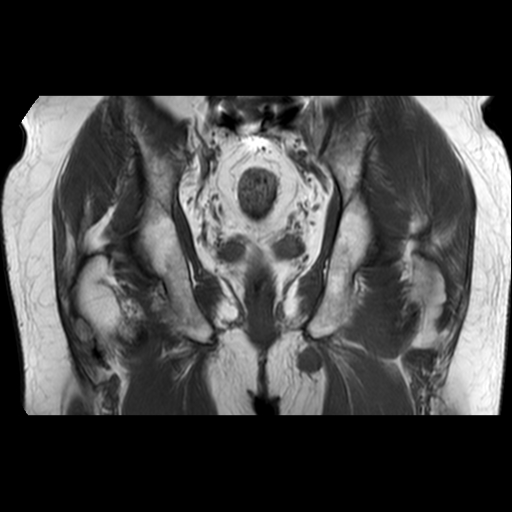
(1/10) 15 y/o M -> Rx: well-circumscribed lytic expansile mass, metaphysis of distal femur 🦴
MRI: fluid-fluid levels.
Your diagnosis on these 2 high power images?
Follow the 🧵👇🏽 for a poll & a short tweetorial.
#BSTPath #PathTwitter #bstpathpodcast #pathresidents #pathfellows
3
50
121
18,254
Dr Ashish Kawthalkar retweeted

6 Dec 2023
Hi #pathology friends,
Anyone up for a #PulmPath #NatPathPuzzler? Excited to share this one.
Lung nodule. Adult. No prior history. No tricks. Sent to us as a consult asking: what is this??
16
65
163
29,611
Dr Ashish Kawthalkar retweeted

20 Feb 2024
It's calcified, it's chondroid, it's mesenchymal...what's not to like? #BSTpath
pubmed.ncbi.nlm.nih.gov/3710…
3
19
54
7,391
Dr Ashish Kawthalkar retweeted

6 Oct 2021
Cauda equina tumor - we don't see this one very often. Can you guess the diagnosis? @UTSW_Pathology
18
45
160
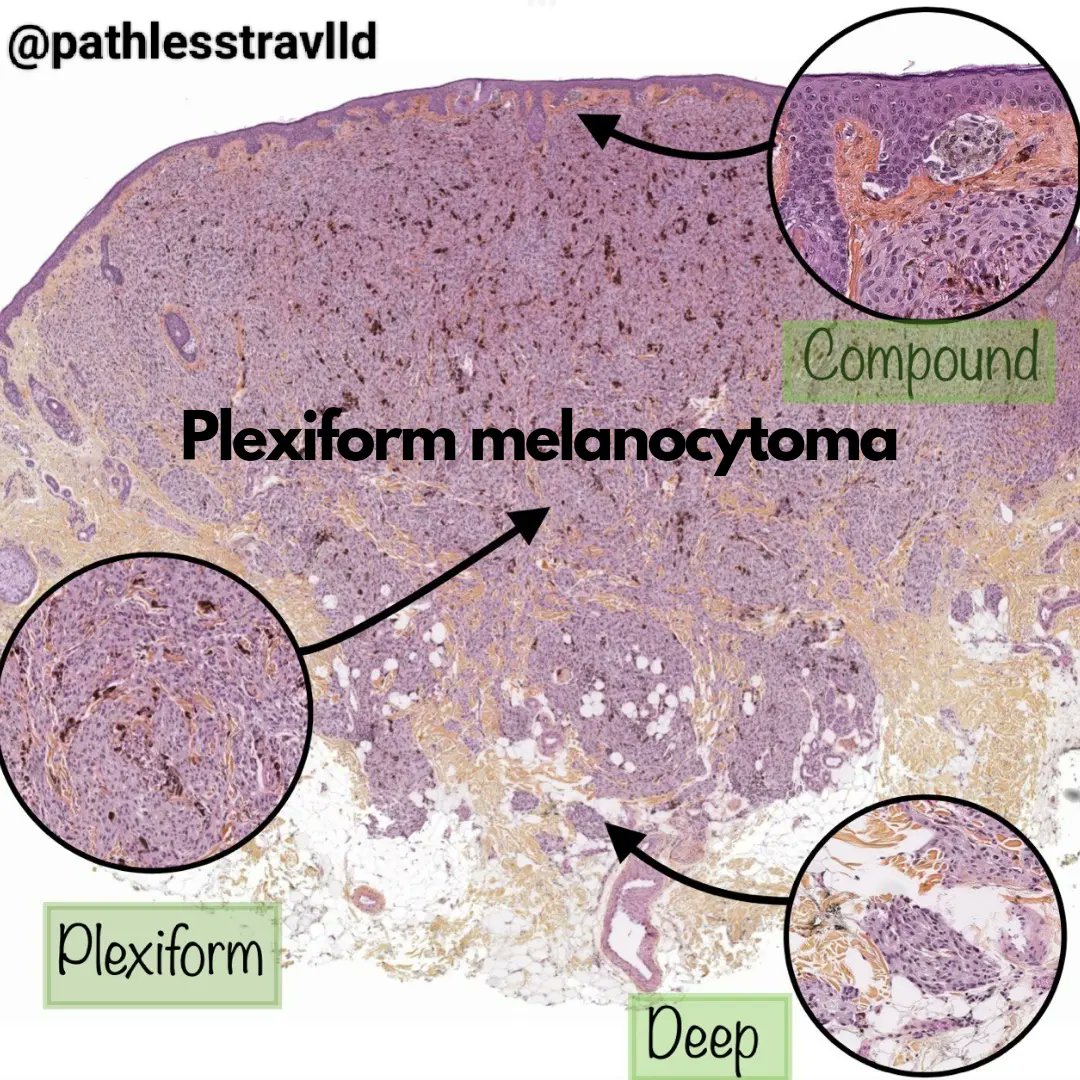
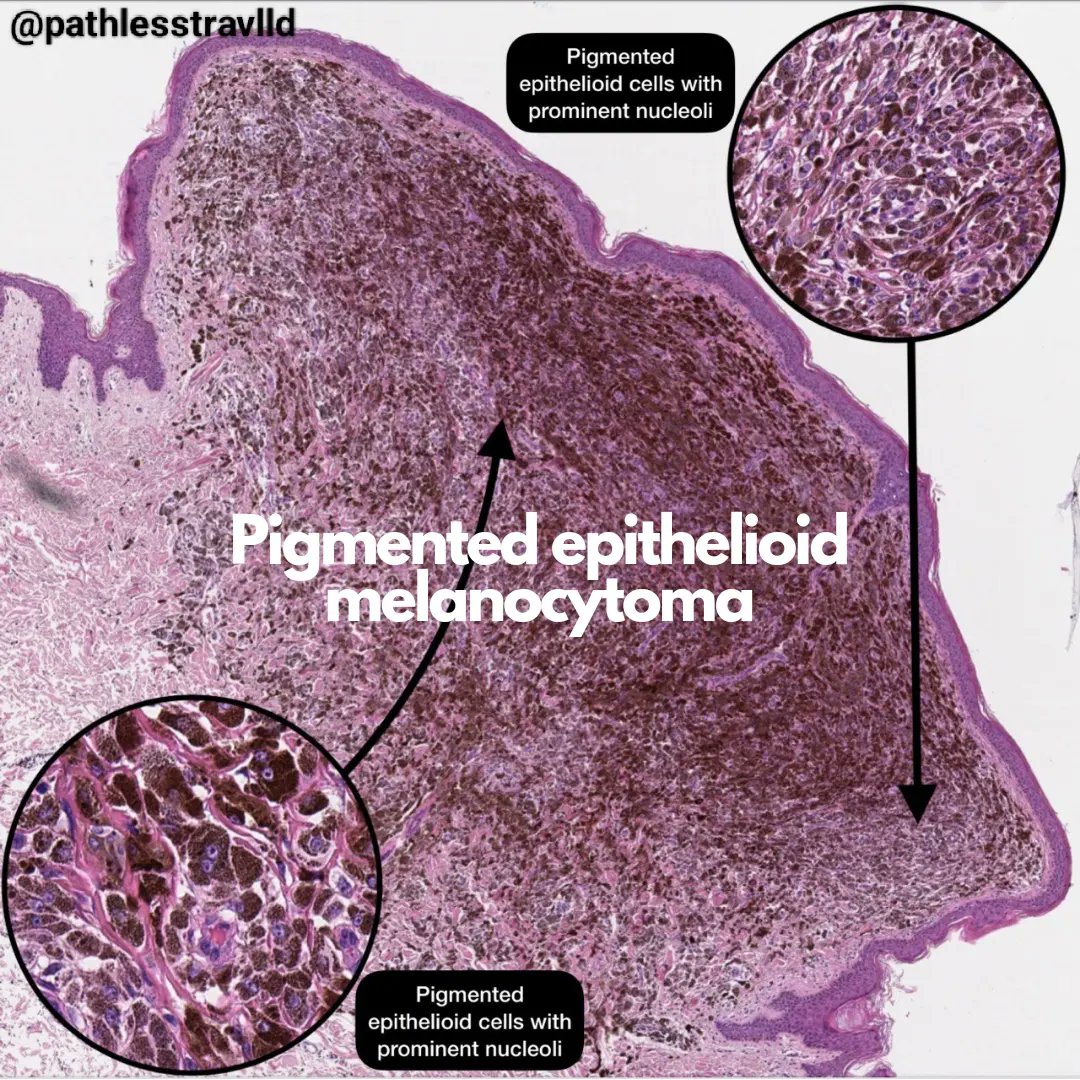
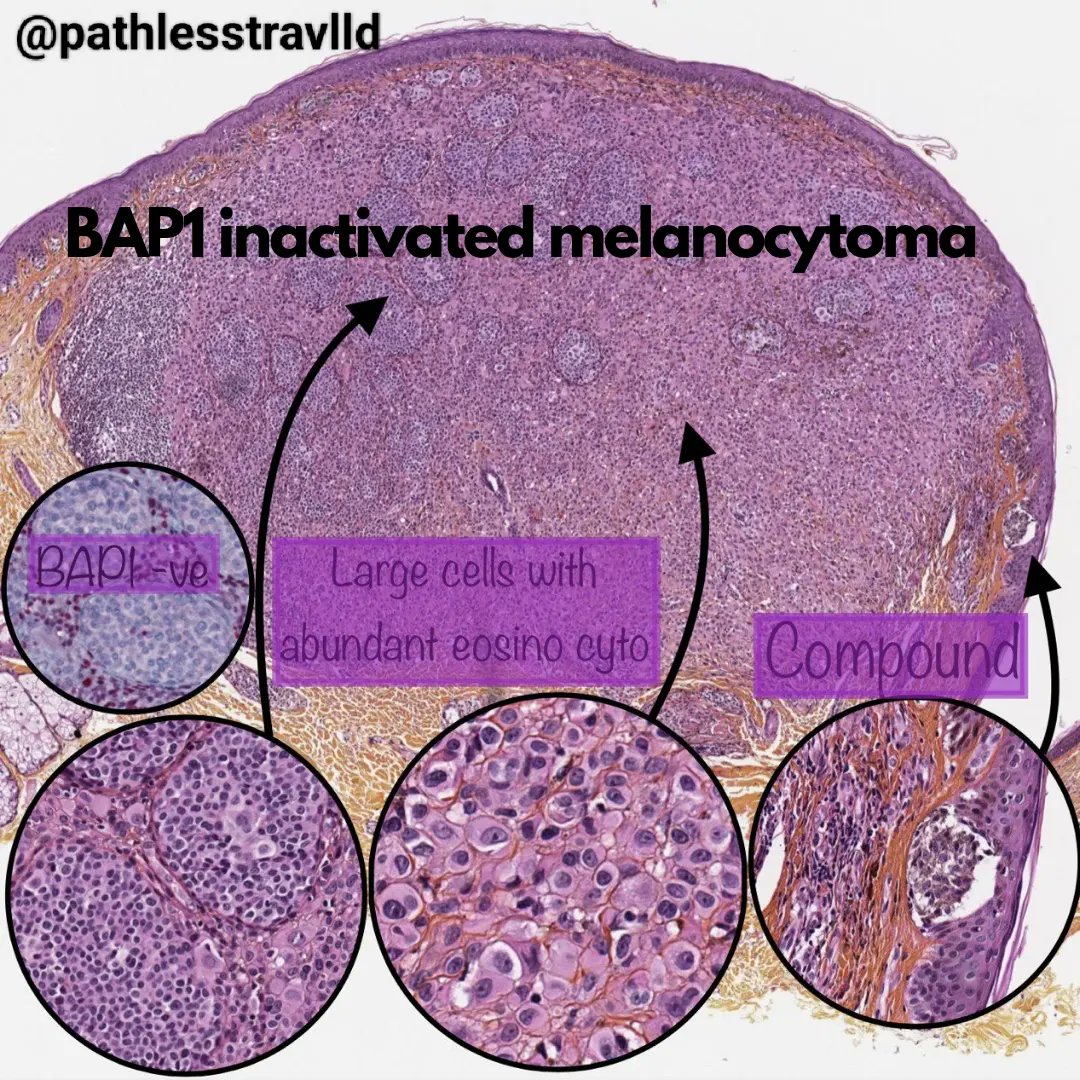
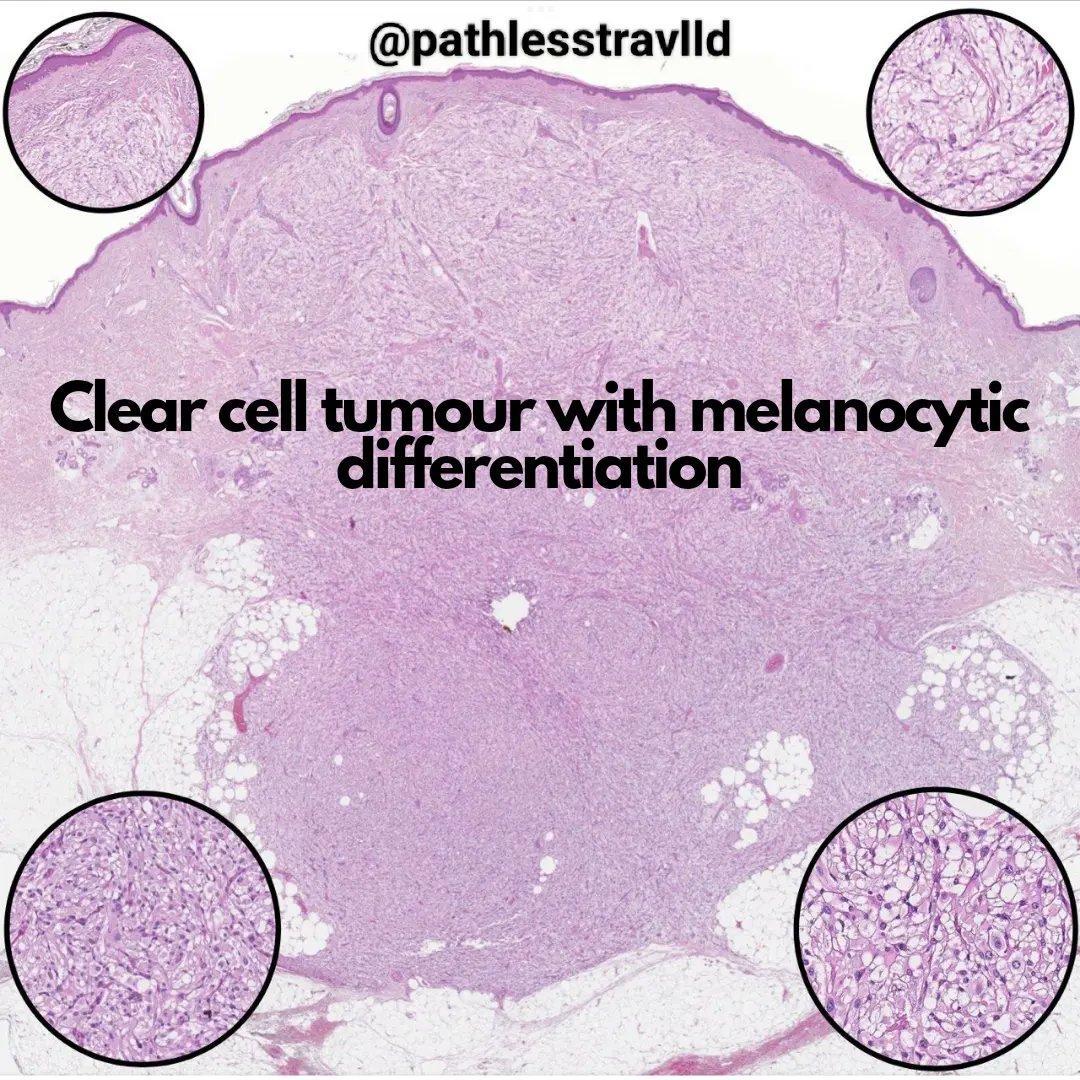
15 Feb 2024
Melanocytomas sourced from WHO 5th ed skin tumours - a pictorial👁️ view.
🔬 credit: 1, 3, 4 : WHO class. of tumours online, 5th ed
2 : Leeds Virtual Public Slide Deck
#DermPath #pathX #pathTwitter #dermatology #melanoma
1
8
28
1,439
Dr Ashish Kawthalkar retweeted
8 Feb 2024
1
15
44
6,255
Dr Ashish Kawthalkar retweeted

1 Feb 2024
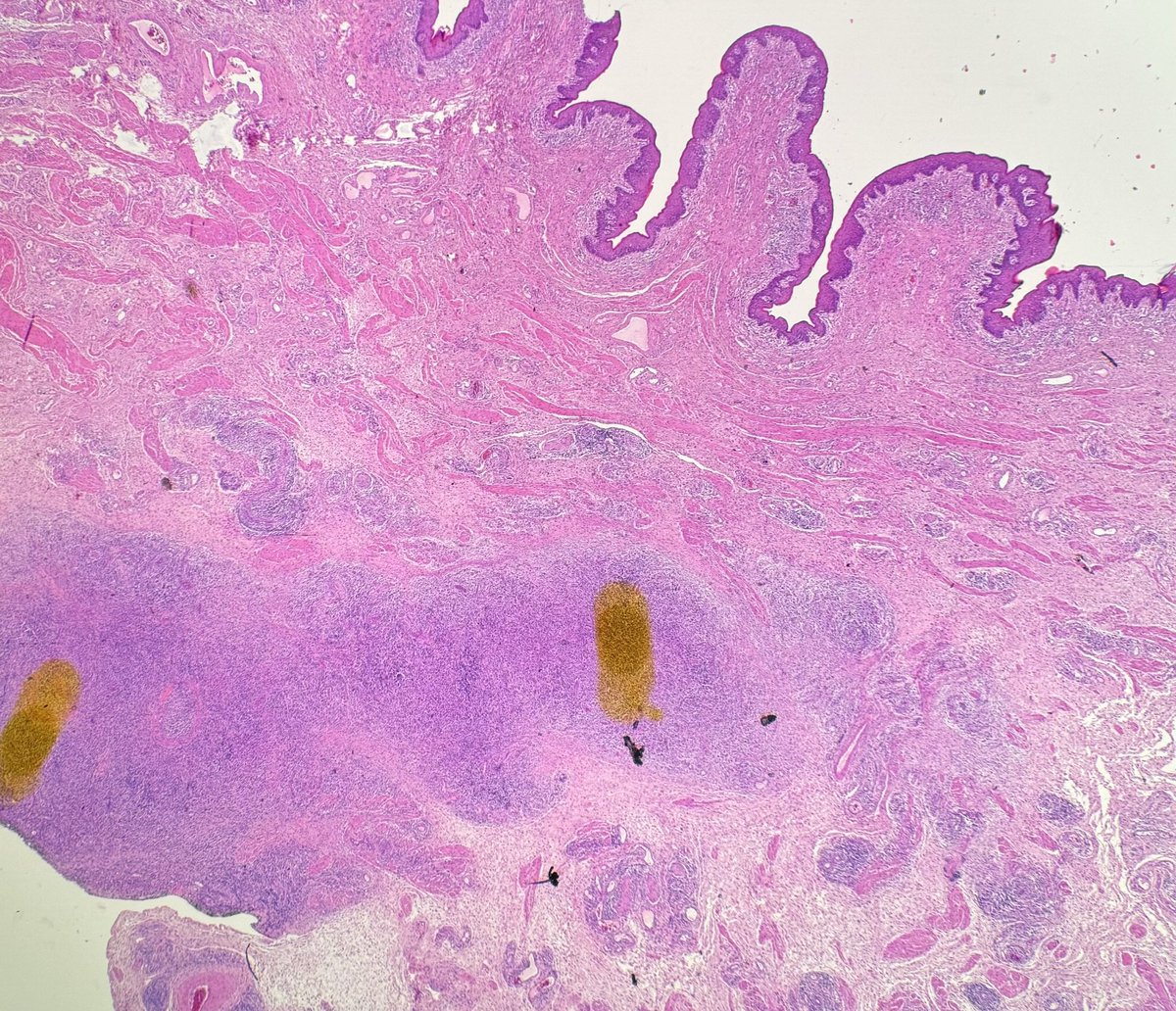
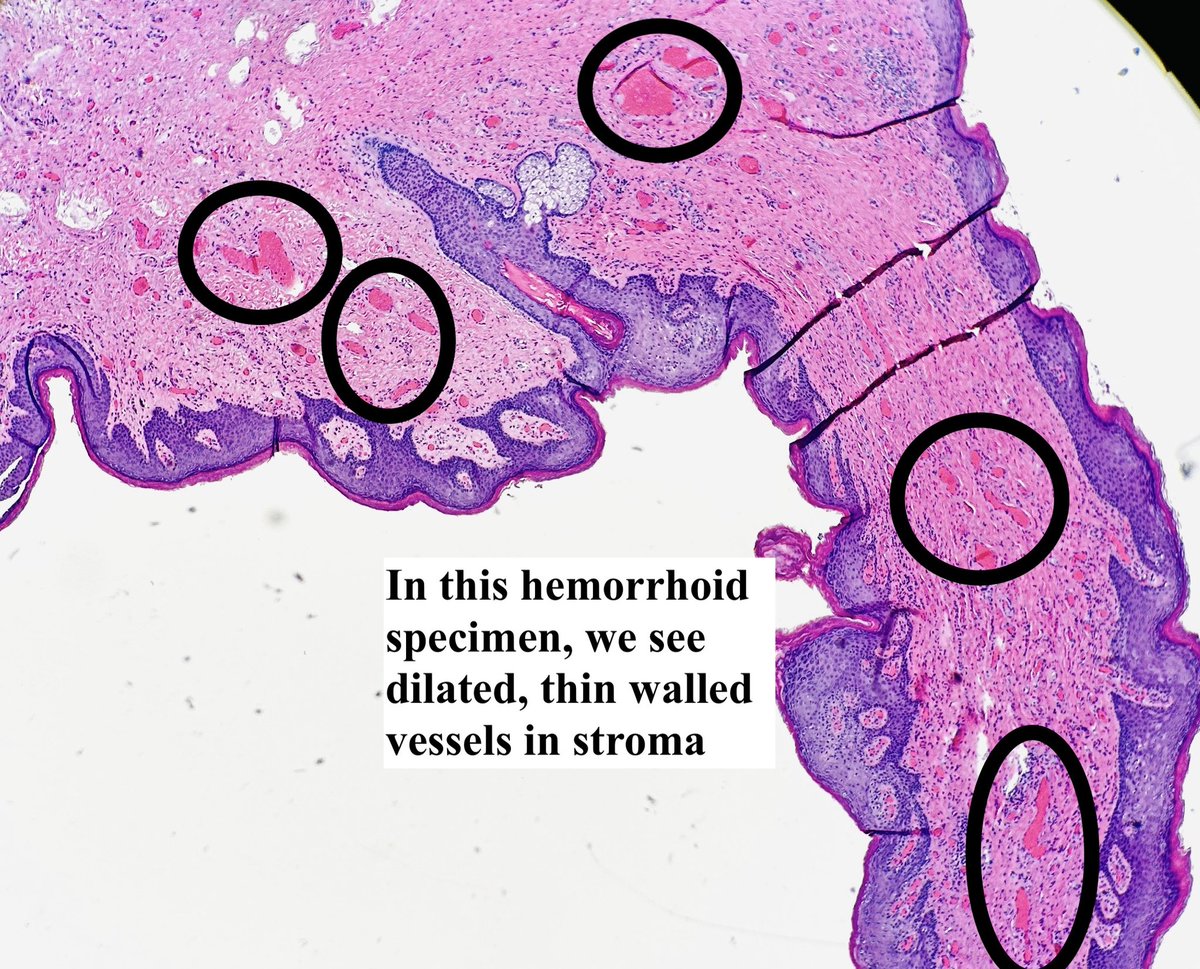
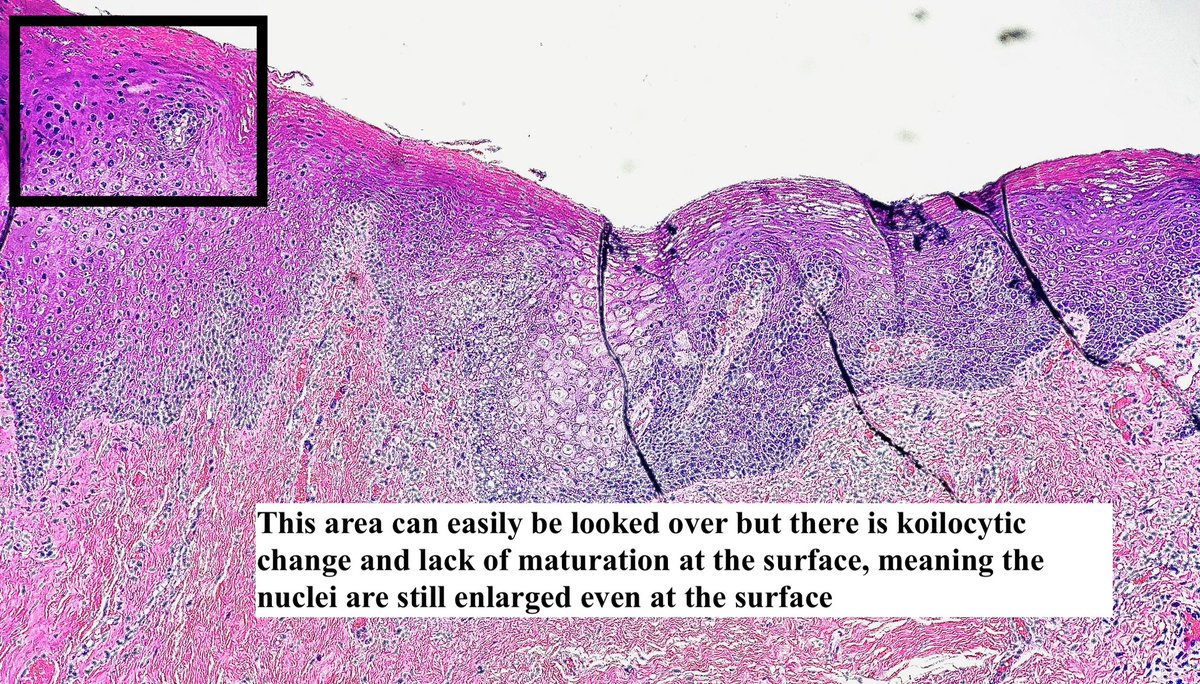
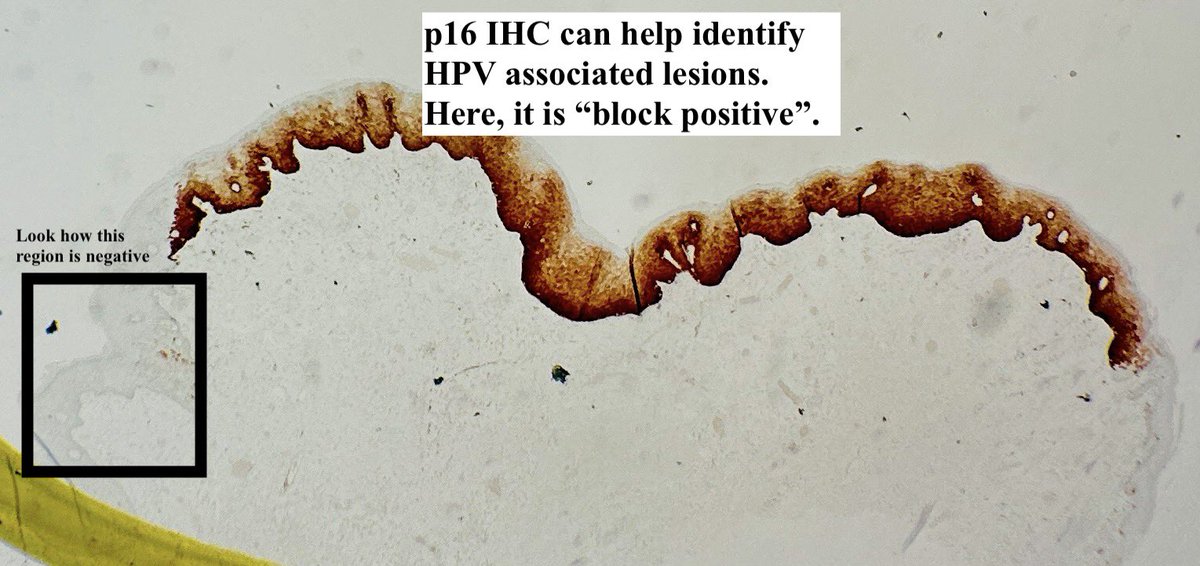
Hemorrhoids are “Easy” to Read by Pathologists.
Easy to Read, however, also sometimes mean Easy to Miss 😰😨
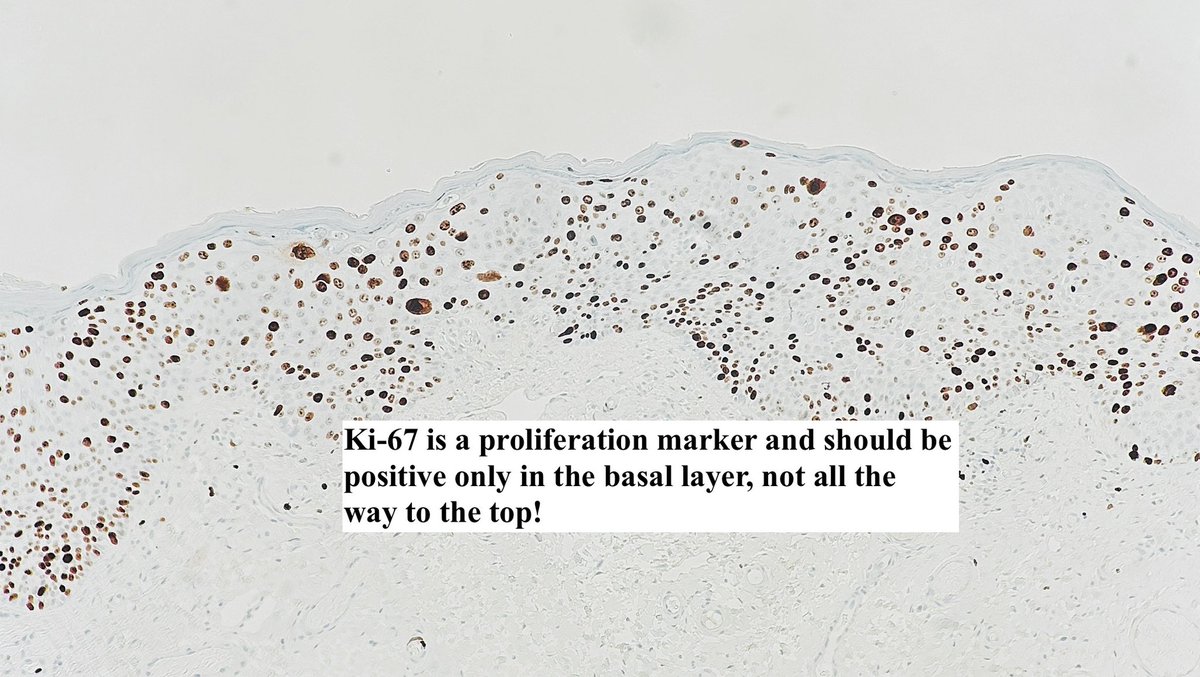
Here’s an HSIL involving a hemorrhoid.
Credit: Michelle Williams, MD
#pathagonia #pathx #gipath #obgyn #gynpath #hpv #medstudent #gensurg #surgpath #surgery #medx
1
36
115
5,776
2 Feb 2024
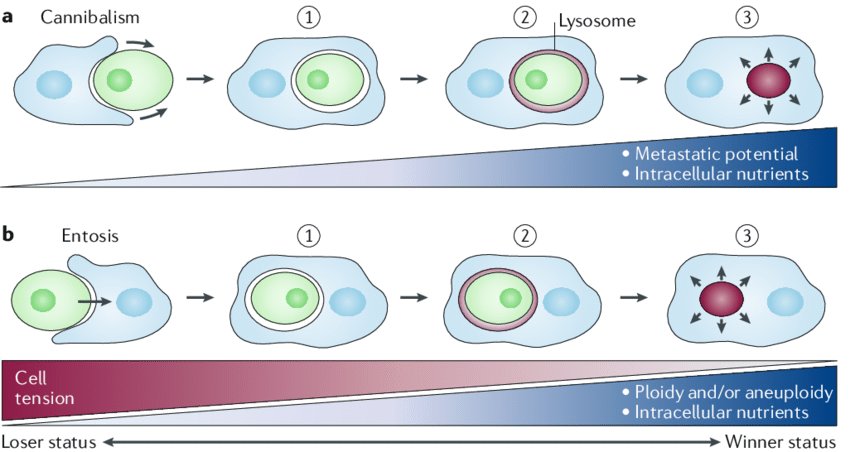
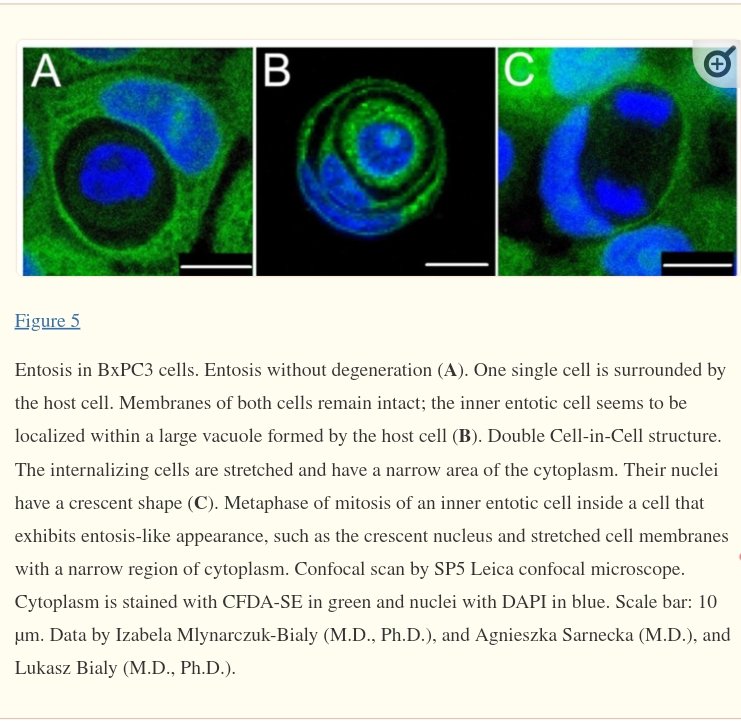
🚨An interesting form of cell death☠️ : Entosis and cannibalism often look similar on light microscopy🔬
@DanGrahamMD @MirunaPopescu13 and #pathTwitter what do you think? Entosis vs cannibalism?
...More in the tweet below👇🏻
#celldeath #pathX #cytology
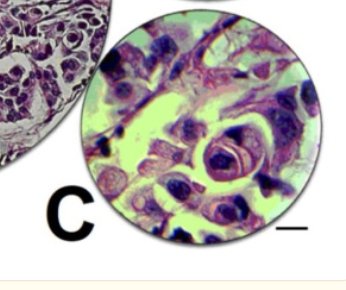
2 Feb 2024

The phenomenon seen here is cell cannibalism aka‘‘bird’s-eye
cell’’. Bird's eye cell is a tumor cell with in a tumor cell in such a way that smaller tumor cells are found in the cytoplasm of the larger tumor cells with crescent-shaped nuclei.

3
1
654
2 Feb 2024
1 : Entosis vs Cannibalism
2&3 : Entosis
Sources :
nature.com/articles/s41568-0…
ncbi.nlm.nih.gov/pmc/article…
51
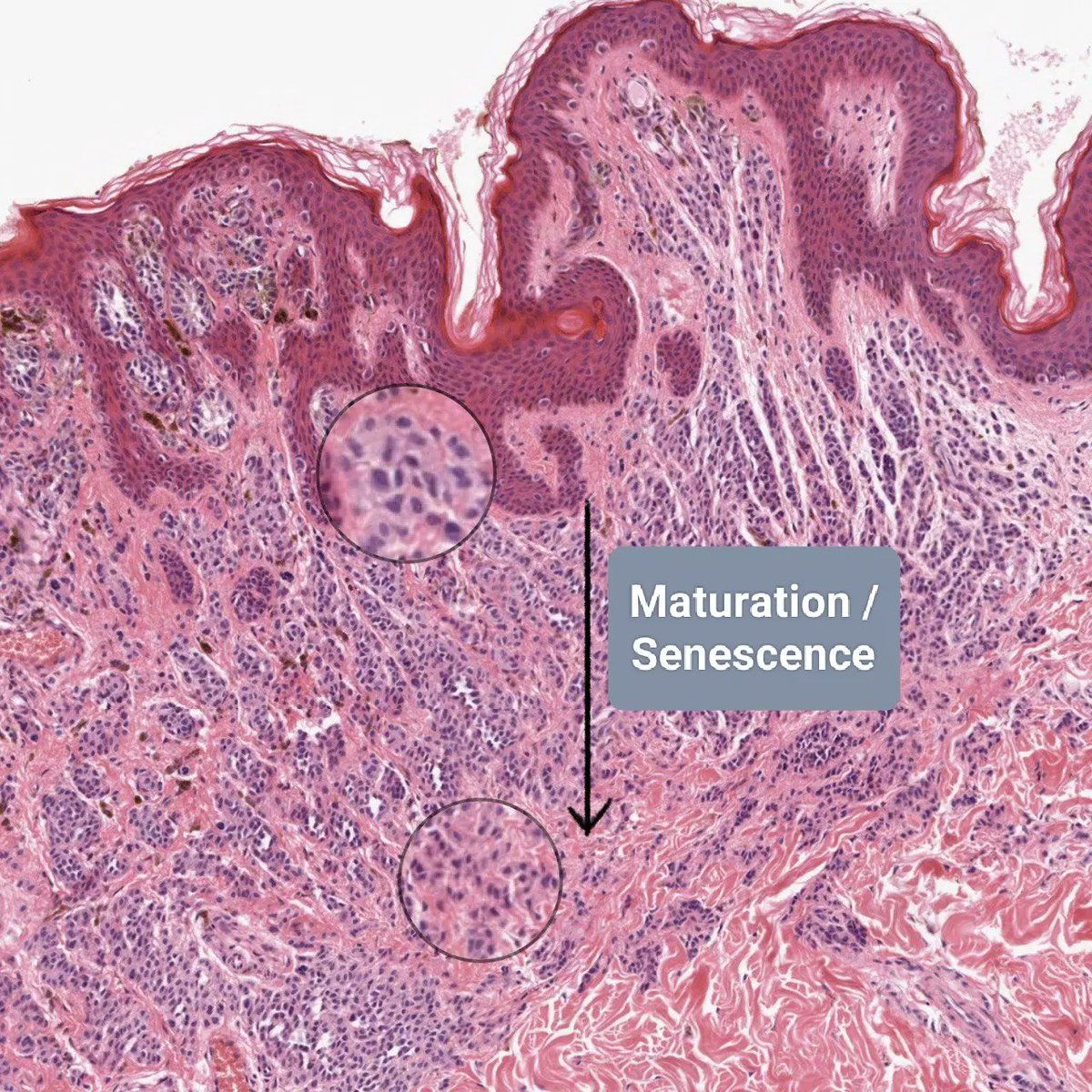
31 Jan 2024
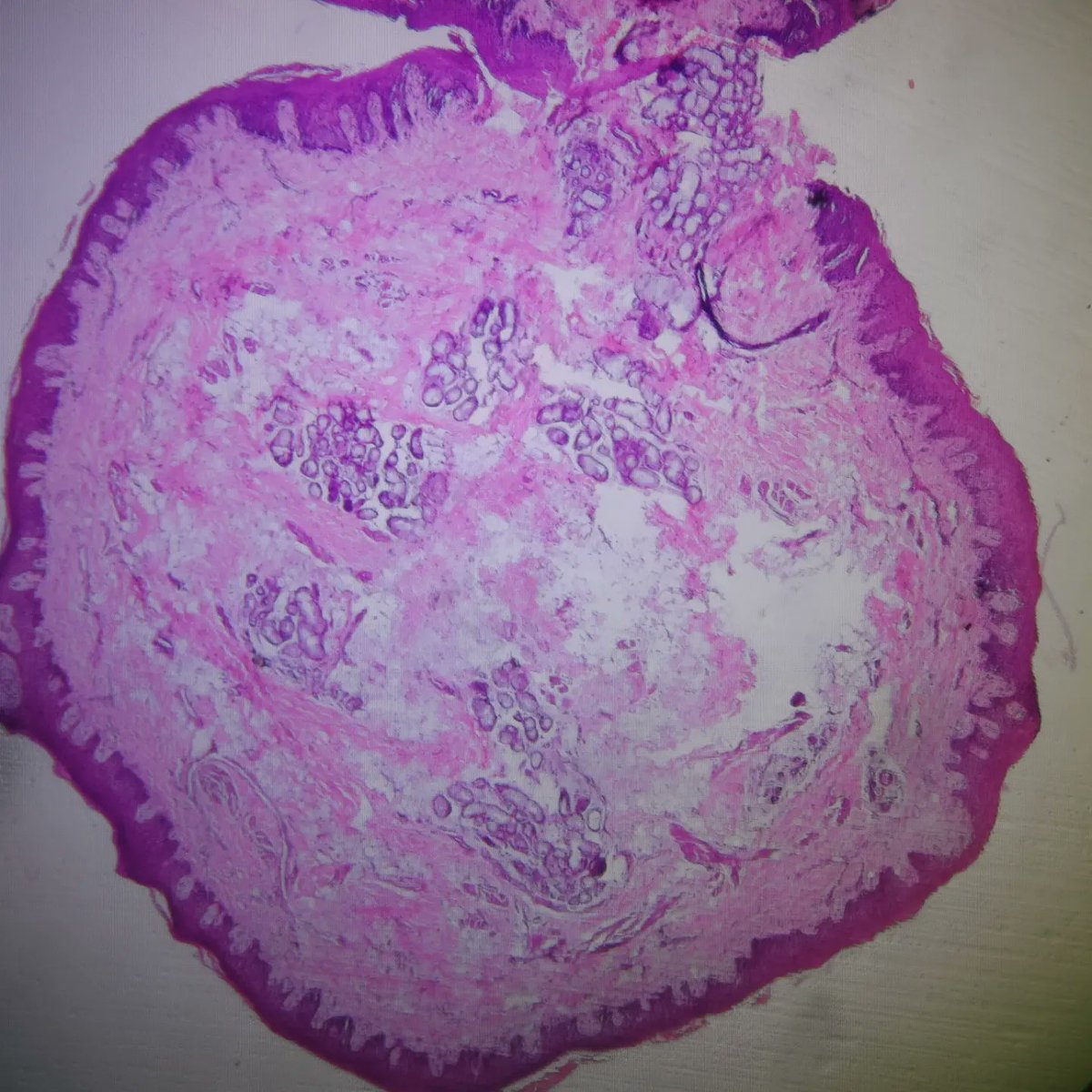
Naevus maturation : is it really?
Schwannization or neuronization as we go deep? Or Epithelioidization as we go superficial?
Slide cred : Leeds Virtual Public Slide Deck
#pathX #DermPath #pathTwitter #pathresident
2
192
Dr Ashish Kawthalkar retweeted

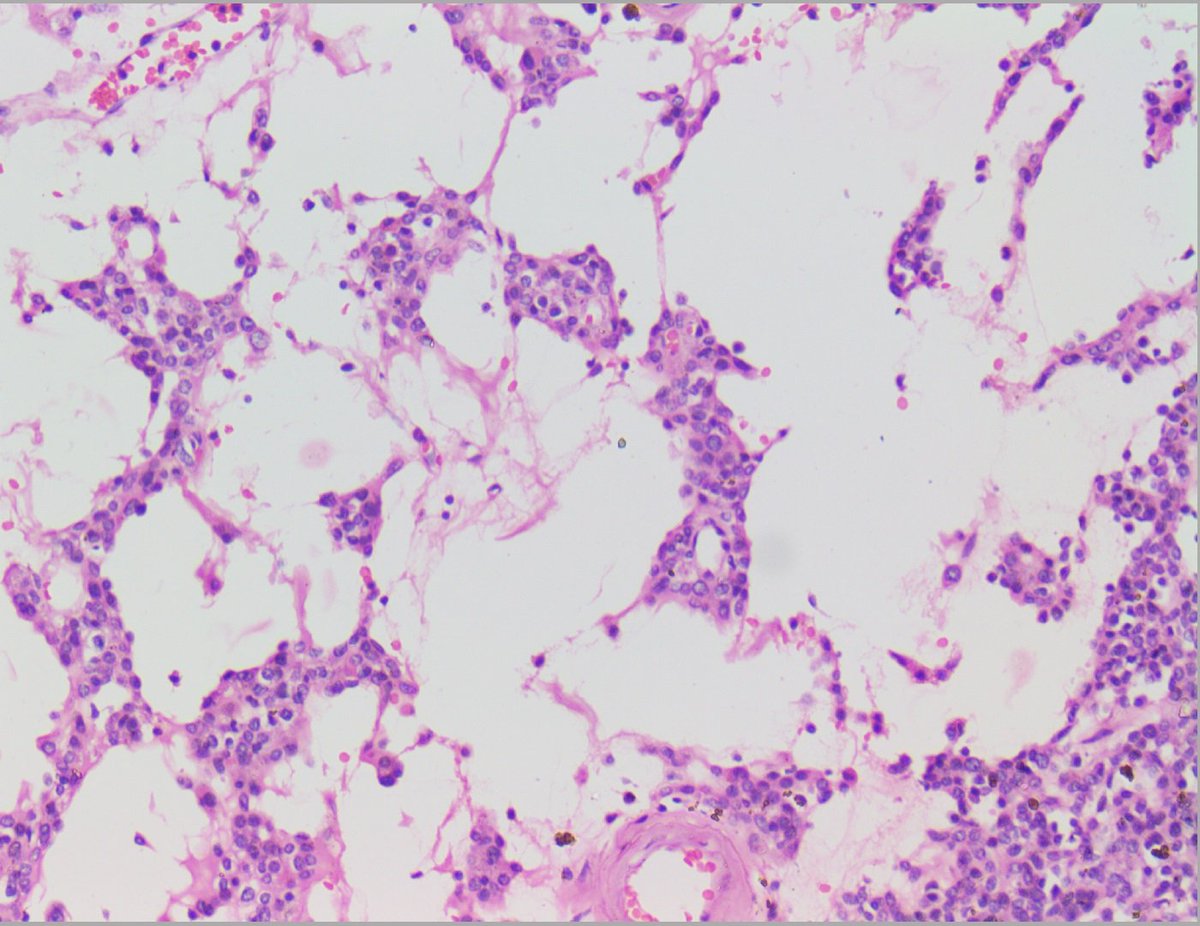
27 Jan 2024
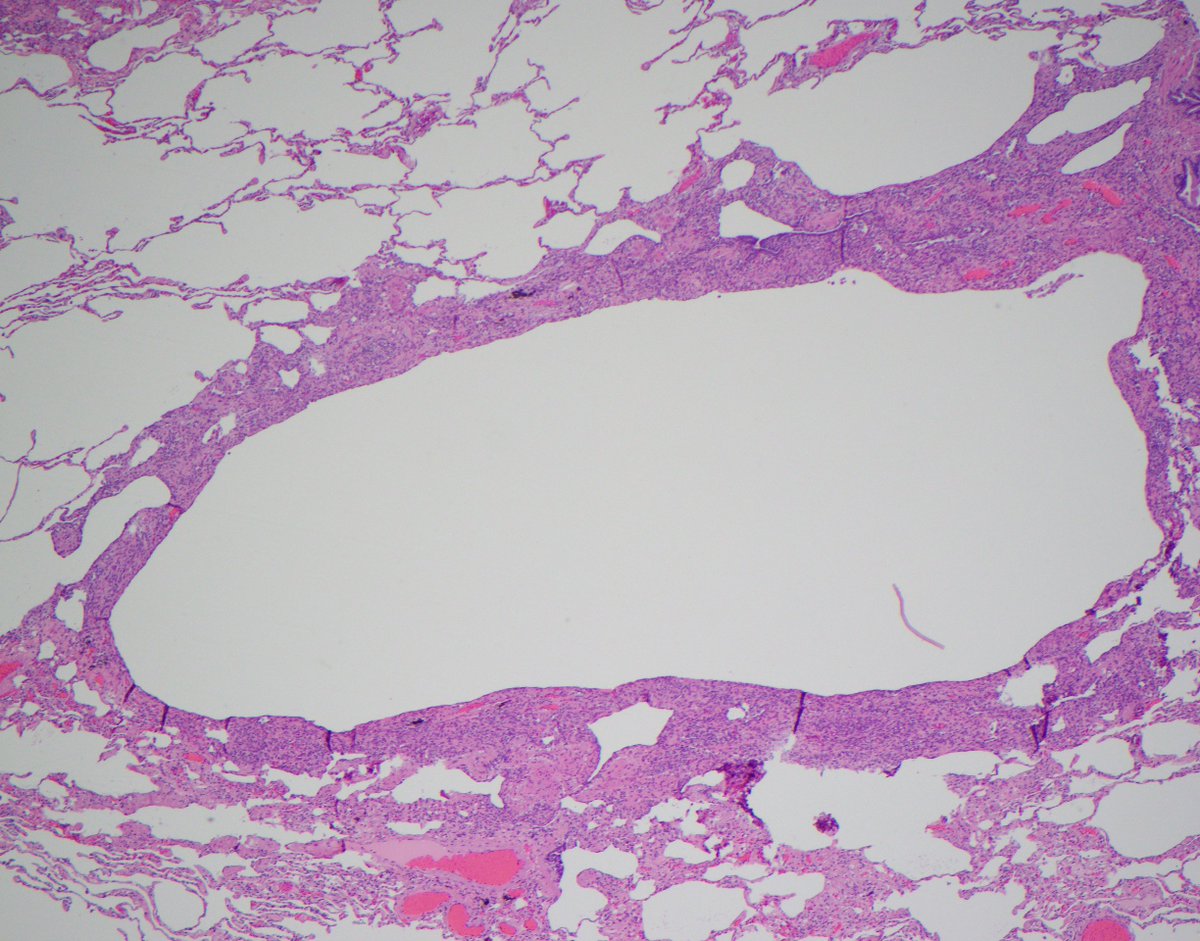
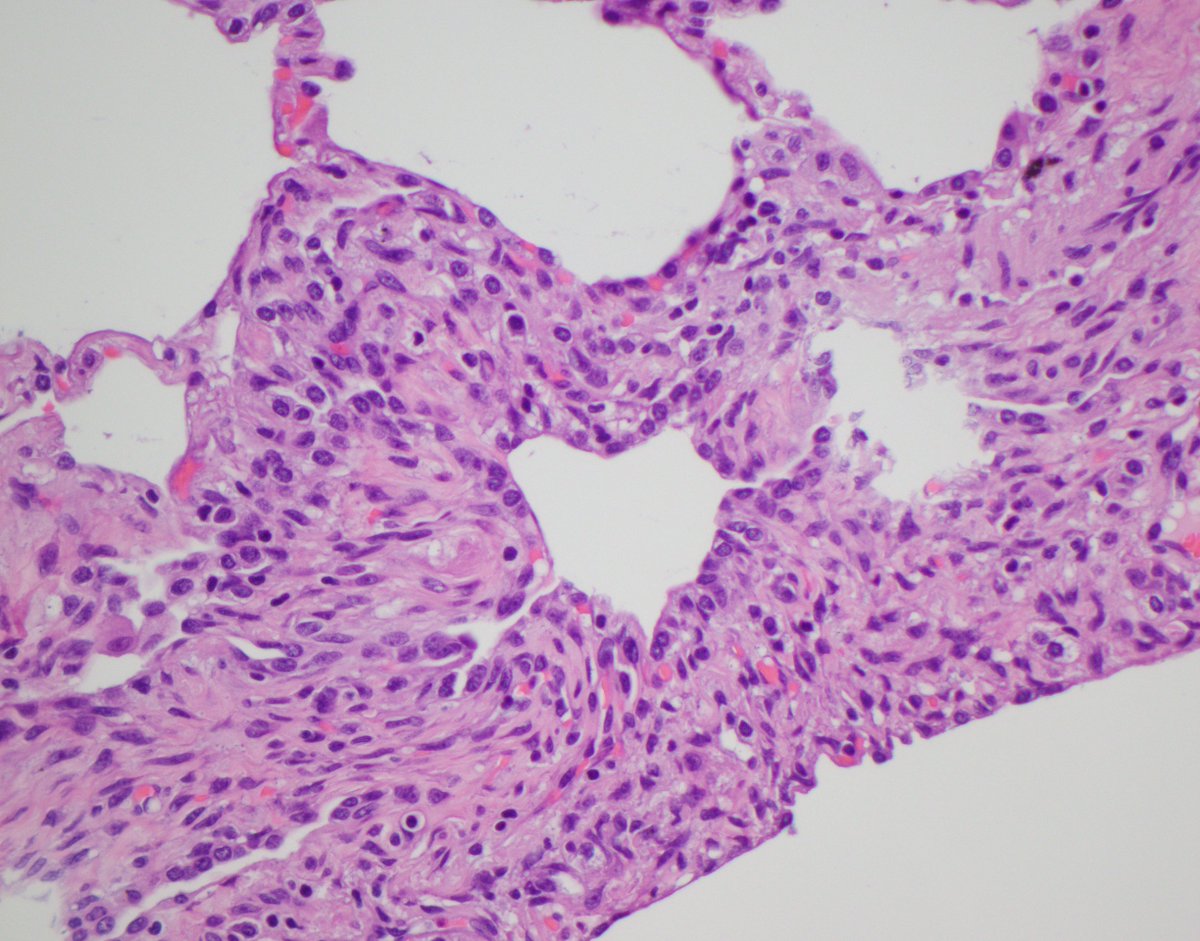
My approach to those bits of lung pathologists receive after surgical treatment of pneumothorax . . .
We commonly get wedges of lung generated during surgical treatment of pneumothorax.
Overwhelming I sign these out as 'PULMONARY APICAL CYSTIC DISEASE' by which I mean the sort of blebs and bullae that tall/lean young people sometimes get and cause spontaneous pneumothorax (and sometimes older smokers get too). It's just a neat four word summary for this phenomenon that can go on the bottom line and means there are no other important underlying pathologies.
However there are a few underlying pathologies that are very important not to miss.
These include:
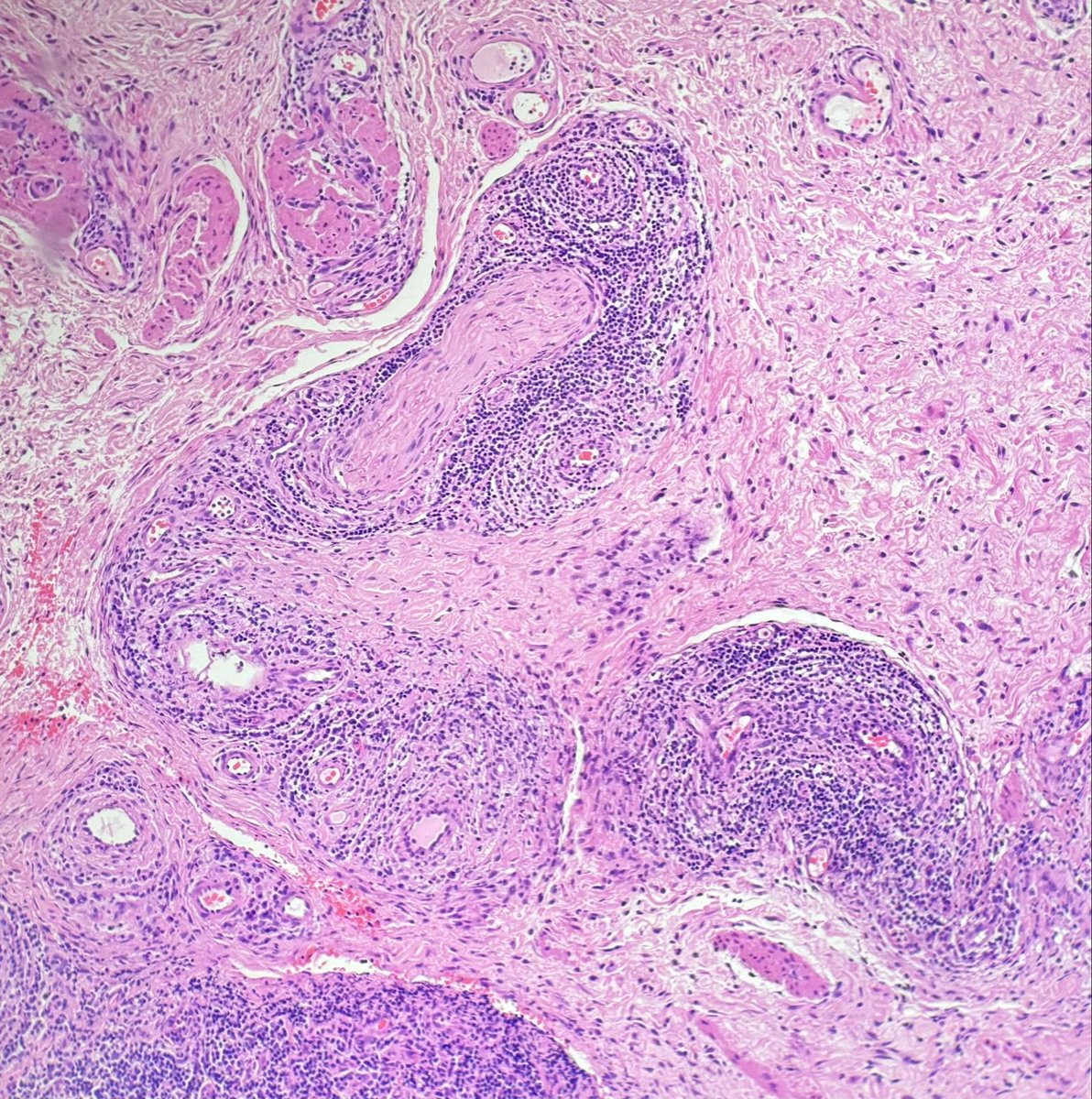
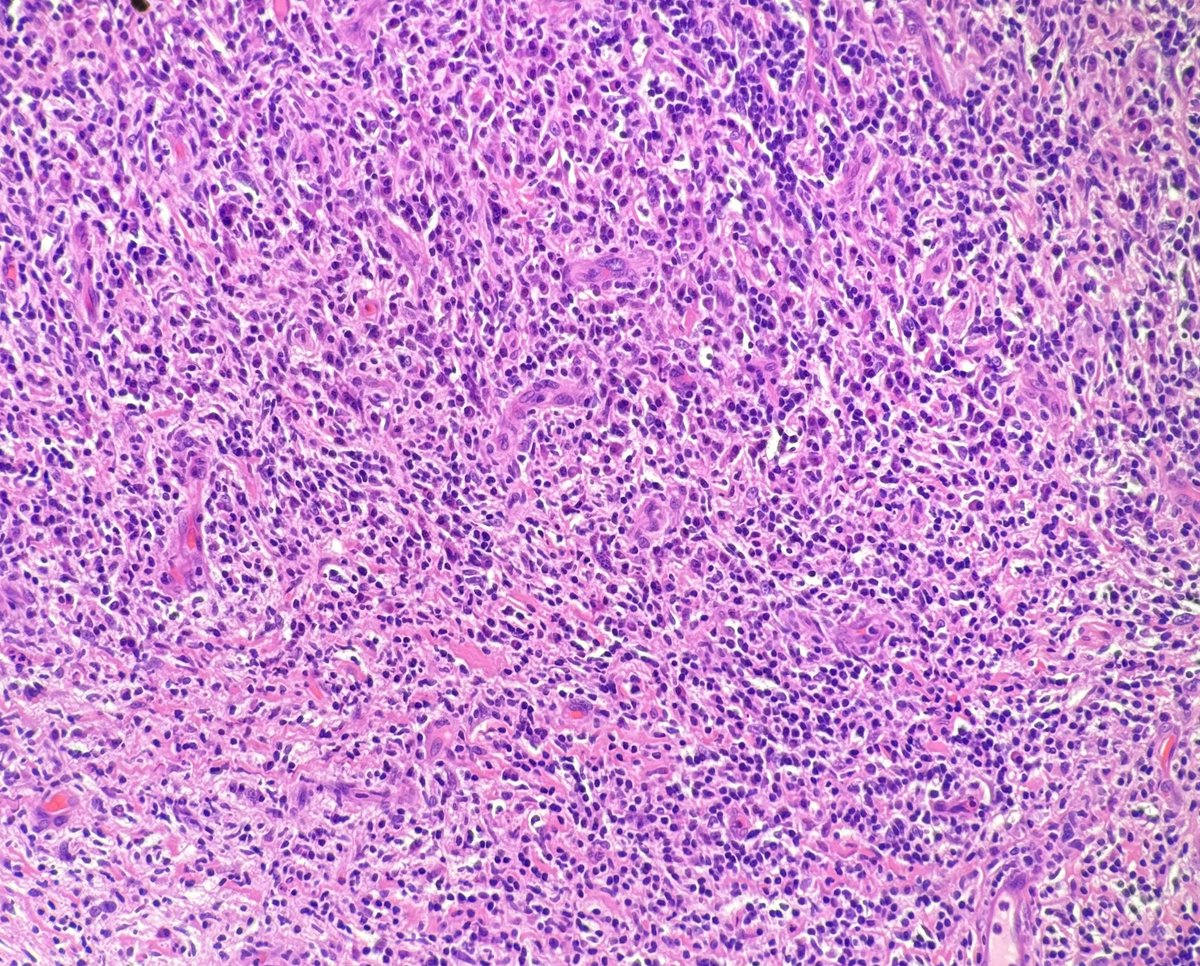
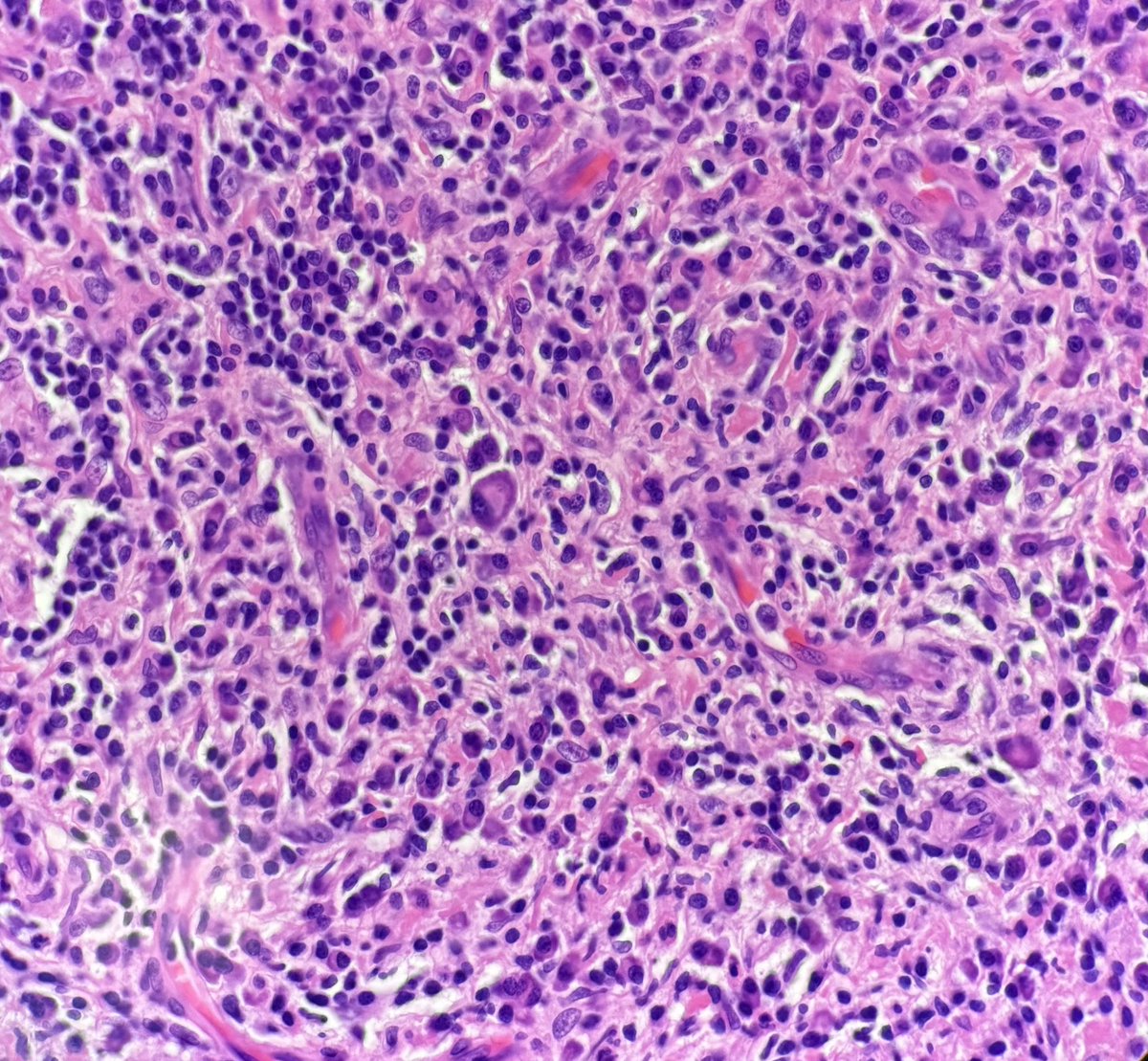
1. Langerhans Cell Histiocytosis.
2. Pneumocystis pneumonia (pretty rare now to present as pneumothorax but in the olden days before widespread uptake of HAART we used to see quite a bit)
3. What we called 'Bong Lung' in 2005 in Am J Surg Path:journals.lww.com/ajsp/citati…
(clue to the diagnosis of Bong Lung - they often present late in the evening to the emergency department)
4. Birt-Hogg-Dube syndrome (good luck diagnosing this on pathology alone, but on imaging look from the proximal/non-apical cysts and other disease associations (renal tumours and facial skin lesins)
5. Personally I've never seen a vasculitis or connective tissue disease presenting with pneumothorax (or at least if I've seen it then I have missed it) - but people say it happens
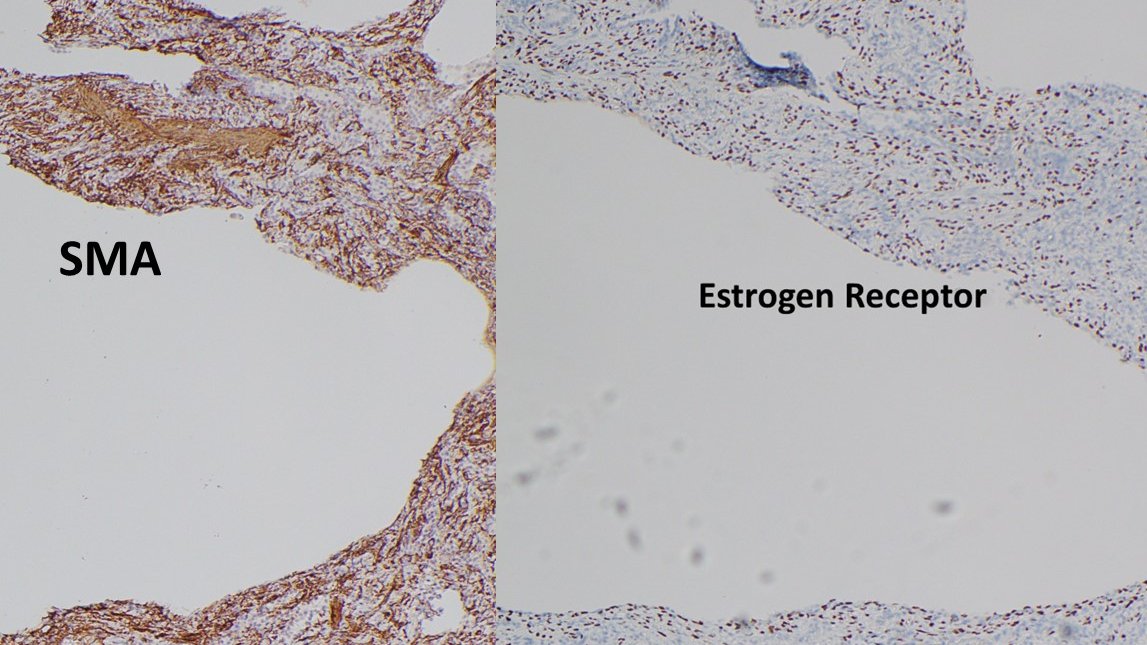
6. And of course - this entity illustrated below. What do you think?

6
22
75
12,305
Dr Ashish Kawthalkar retweeted

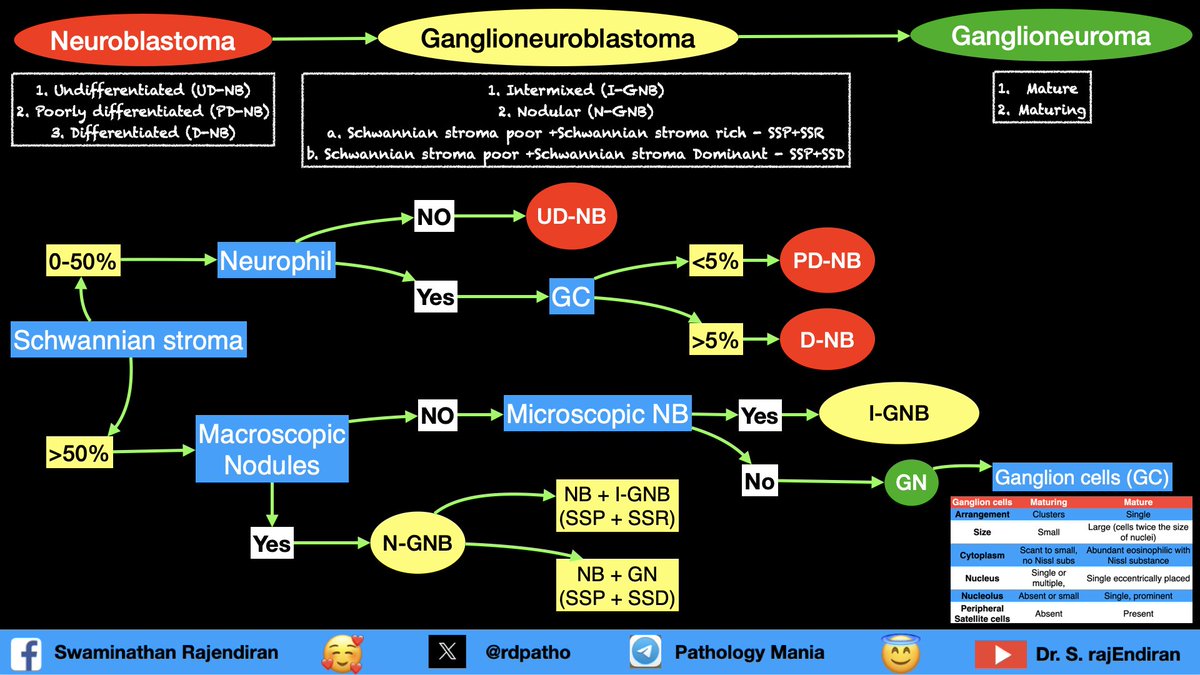
25 Jan 2024
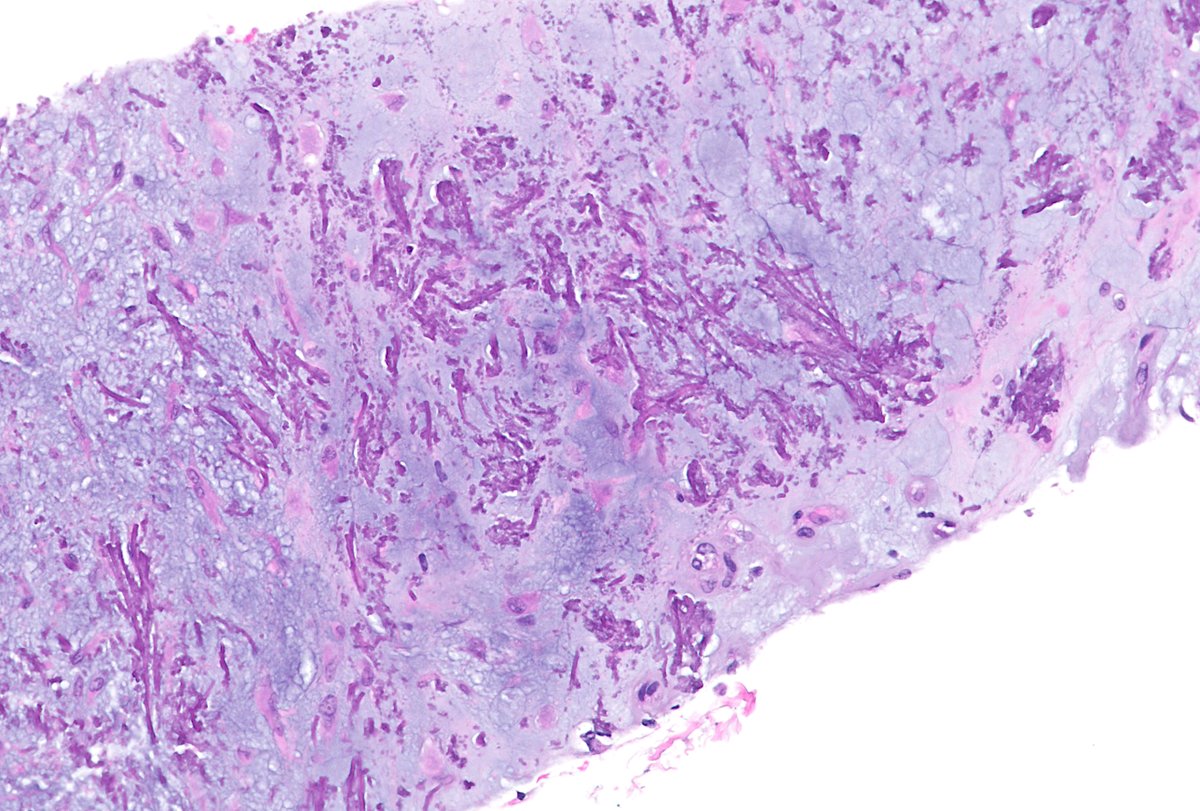
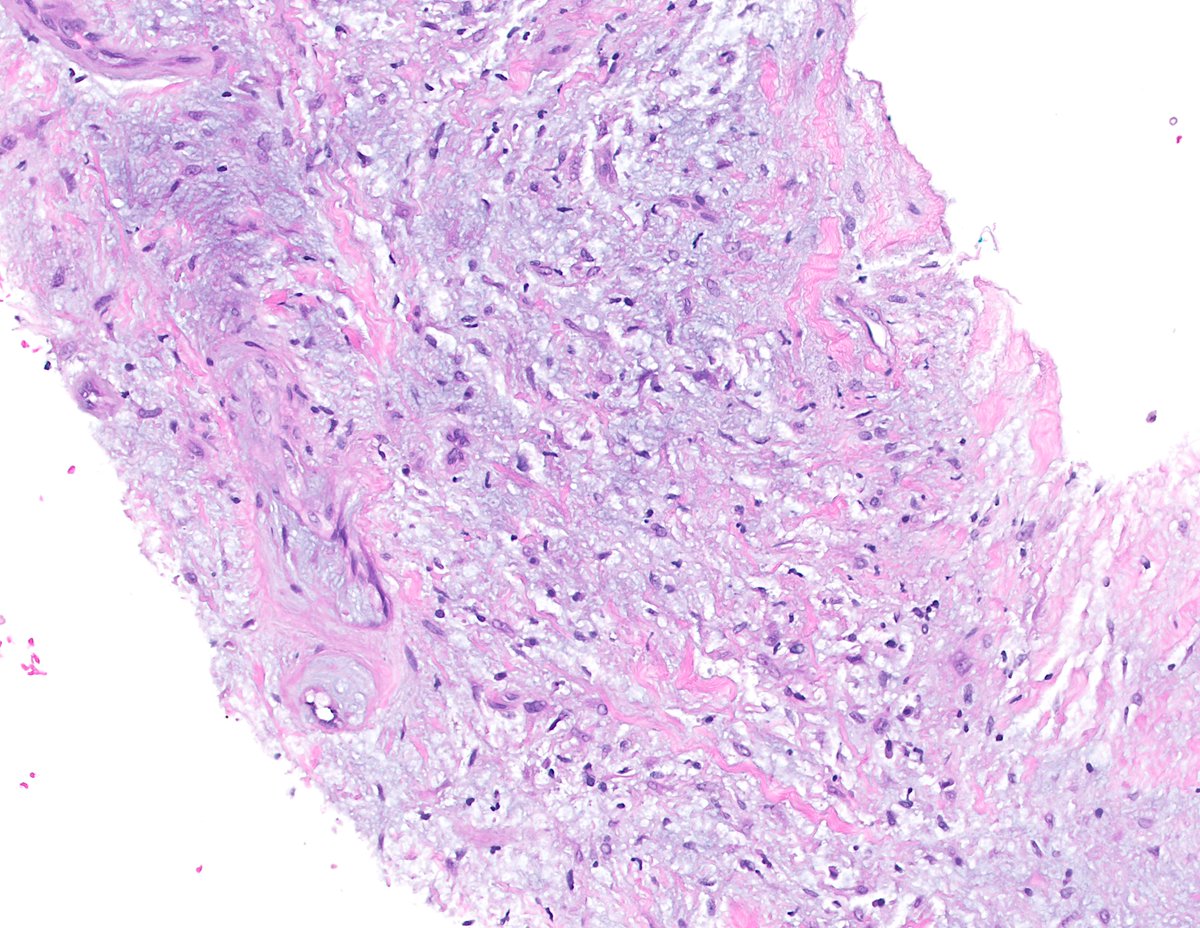
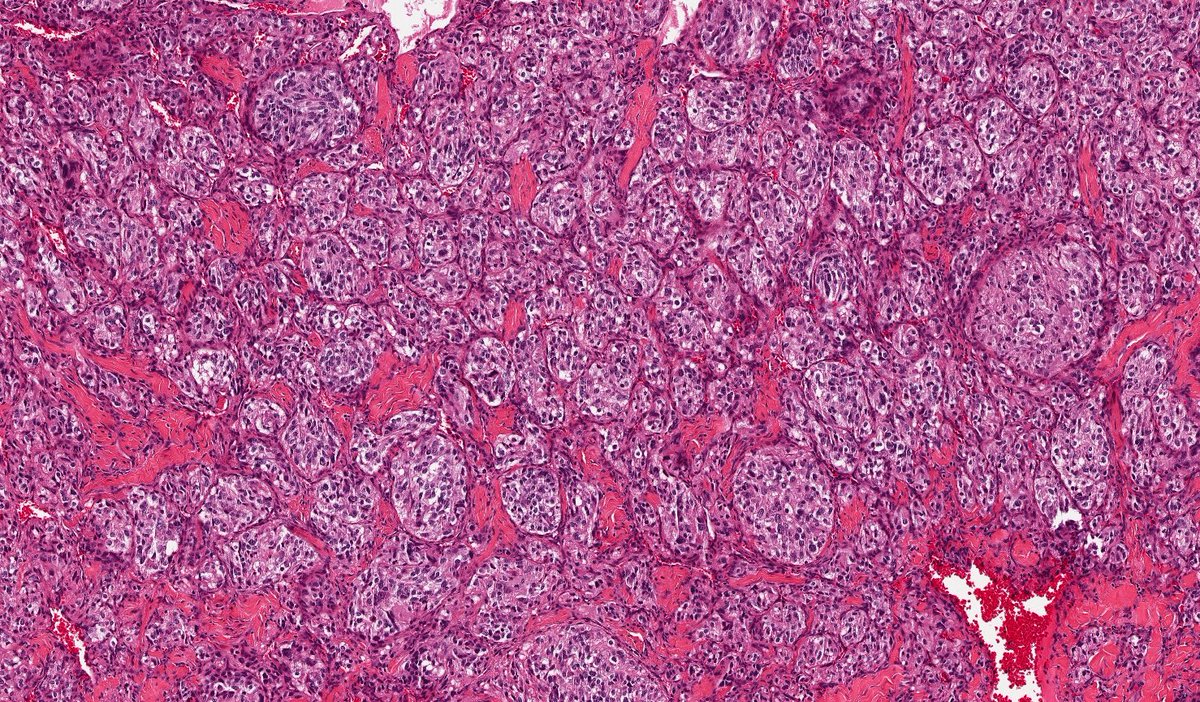
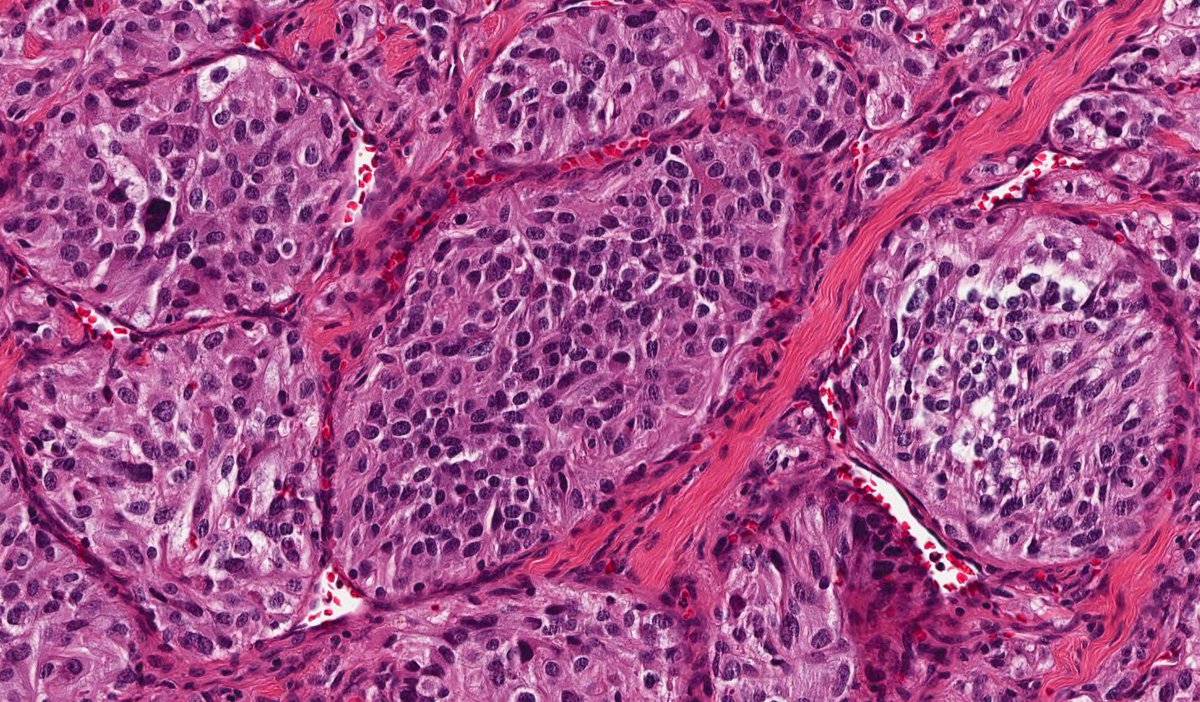
Just finished a discussion of Neuroblastoma and its spectrum ..... sharing the wall hangers .... here ... some of them are already shared .... but i want all in one place and hence repeating .....👏🏻👏🏻
10
32
1,627
Dr Ashish Kawthalkar retweeted
23 Jan 2024
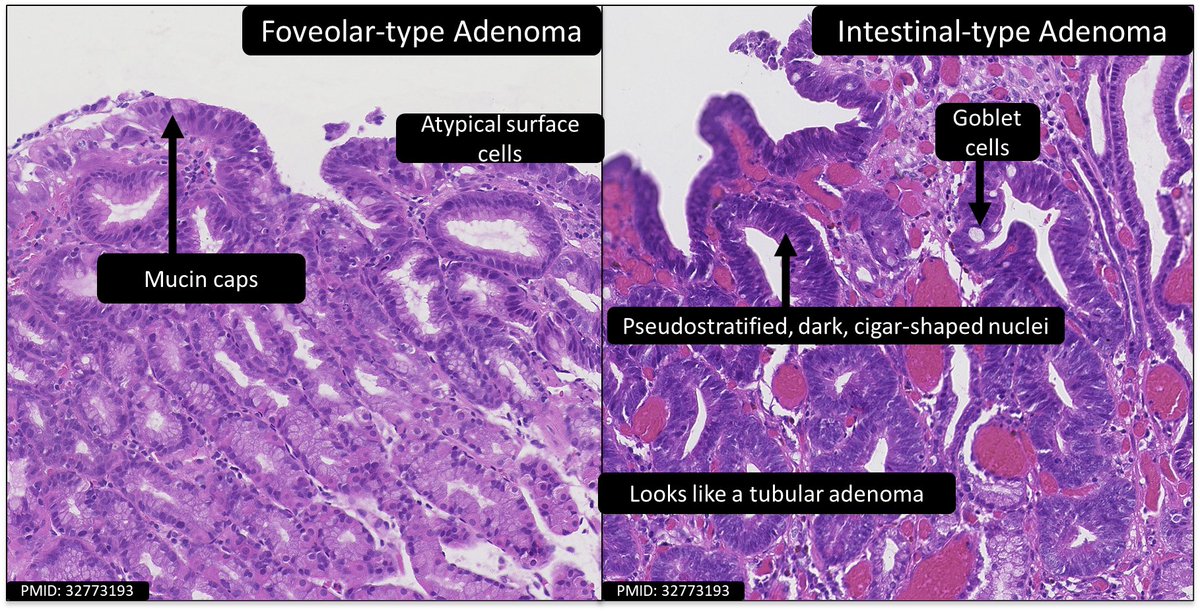
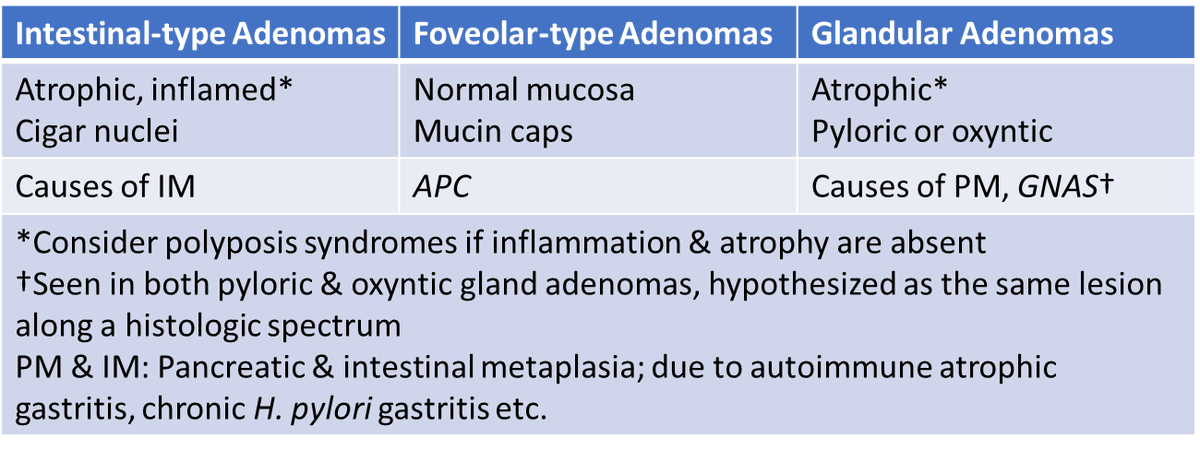
Foveolar-type adenomas are aw FAP (APC)
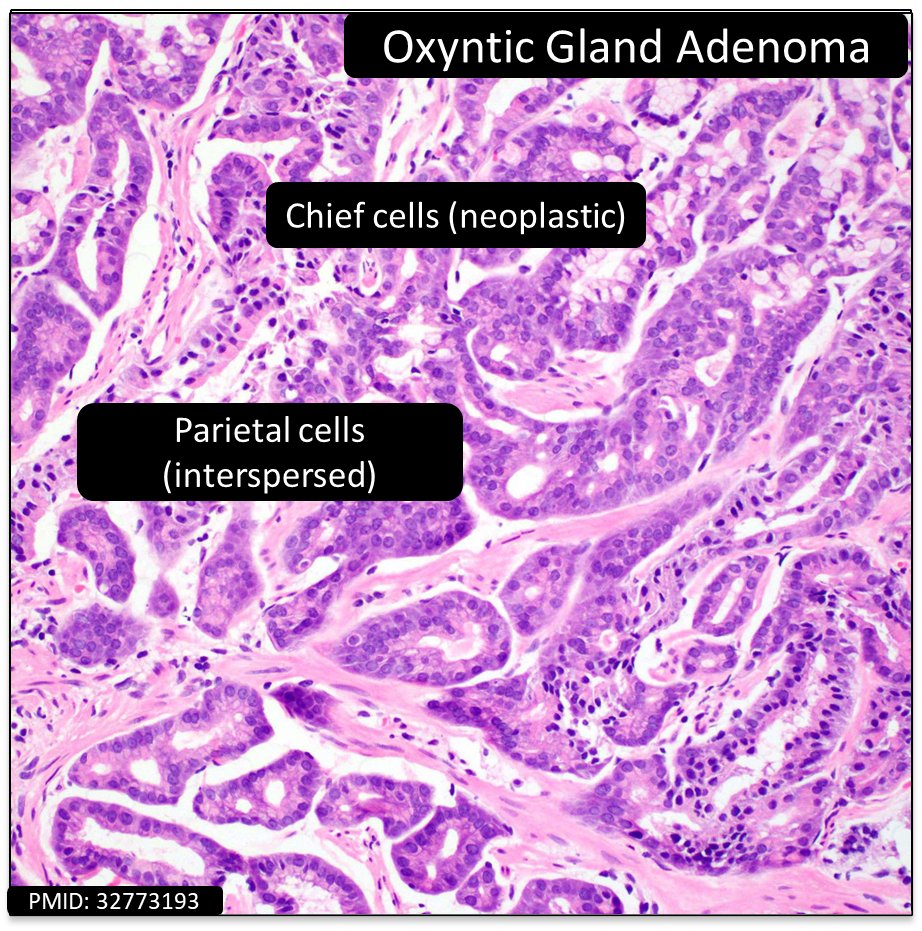
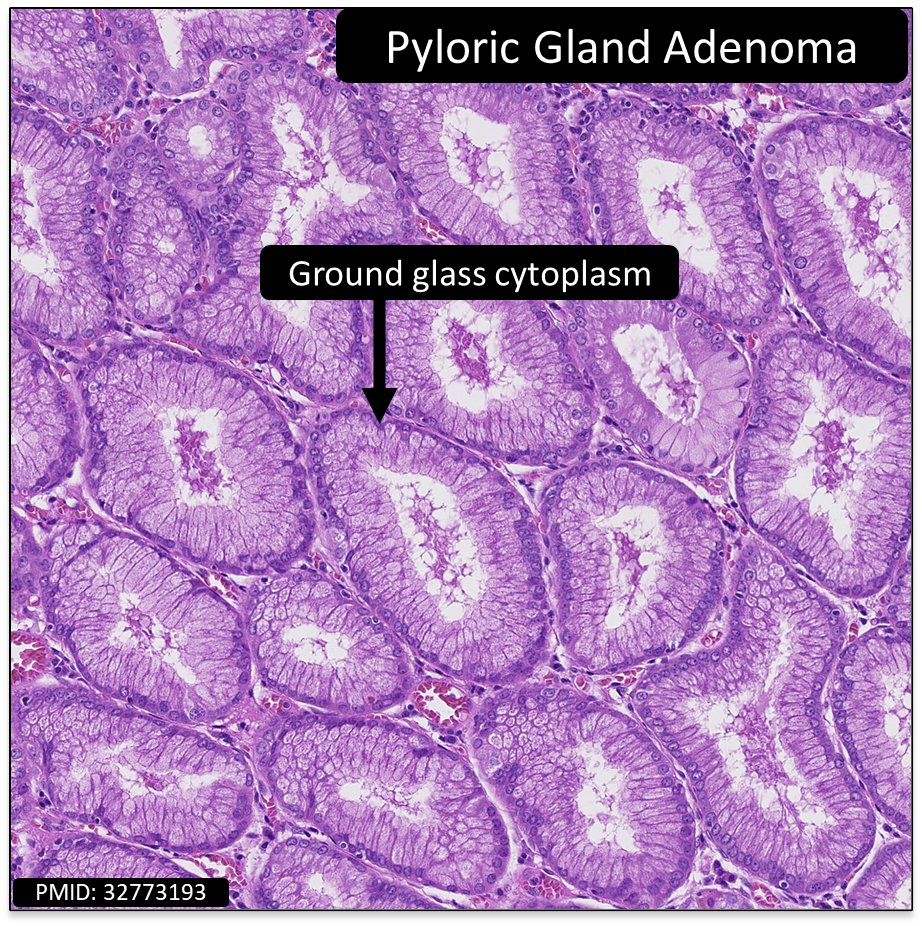
No GNAS, as seen in adenomas with glandular diff (ie oxyntic & pyloric)
Dysplasia in an uninflamed, non-atrophic stomach → consider polyposis syndrome
#GIPath #PathTwitter #PathResidents
surgpath.theclinics.com/arti…
✅foveolar, APC
19
55
1,687