
Joined September 2013
- Tweets 2,990
- Following 6,053
- Followers 11,457
- Likes 4,821
575 Photos and videos






Pinned Tweet

Apr 12
Proud to present our latest article - now available for free download @AJSPjournal
Please retweet and download the article.
Synopsis:
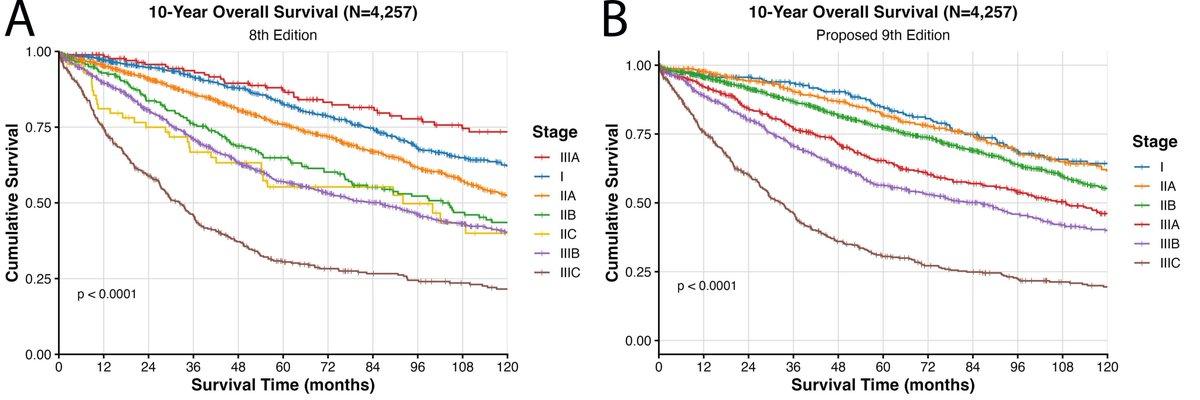
The AJCC ninth edition staging system for colon cancer is not yet current, but there are significant changes proposed. These changes aim to both get rid of the stage 3A paradox (under the eighth edition patients with Stage 3A actually disease do better than Stage 1 and 2) and also to better integrate discontinuous Tumour Deposits (TDs) into staging.
What are these proposals and do they work?
Free download:
journals.lww.com/ajsp/fullte…
12
20
1,988
Anthony J Gill retweeted

Jun 8
As shown in previous CRC studies, ctDNA positivity captures relapse risk very well. However, ALTAIR does not show that we can meaningfully and durably modify this risk with FTD/TPI.
Therefore, in this setting, ctDNA does not appear to function as a predictive tool for treatment selection, but rather as a strong MRD/prognostic enrichment marker.
Trying to treat MRD with conventional chemotherapy may not be the most rational approach. The biology of circulating tumor cells or molecular residual disease may differ from that of established tumor deposits in tissue.
We need treatment strategies designed specifically around MRD biology, rather than simply moving standard cytotoxic agents earlier into the molecular recurrence setting.
nature.com/articles/s41591-0…
3
20
45
4,841
Jun 8
I am deeply saddened by the passing of a great individual @ProfRAScolyer. Richard truly demonstrated the power of a single person who was passionate to influence so many.
A lot has been written about his research achievements and his advocacy in melanoma and brain cancer (which are truly phenomenal and globally recognized).
Beyond these achievements which are so well known and appreciated by the wider community, I want to emphasize that he was also a great advocate for high quality anatomical/surgical pathology. In his farewell letter he emphasized his pride in helping to start the world's largest melanoma tumour bank and his publications not just in melanoma but in melanoma pathology. He truly understood the role pathology plays in a patient's cancer journal and advocated at all levels for the specialty. He spent so much of his time teaching and promoting the discipline of surgical pathology; and he truly mentored so many.
As he wrote:
"A terminal cancer diagnosis does however provide clarity as to what truly matters. It shines a spotlight on the importance of relationships, on true friendship and on selflessness. Whilst cancer may not define us, our ability to empathise with and have compassion towards others does. That is true in all facets of life, and I am confident those traits will continue to guide Australians towards acceptance and support for all."
Also . . . he was also tremendous fun and entertaining in the social setting. This is from a party 25 years ago.
1
27
151
2,943
Jun 8
No words! There's nothing I can say - other than what a great person he was to work with and know.
smh.com.au/national/i-d-be-d…
4
1
14
421
Anthony J Gill retweeted

May 30
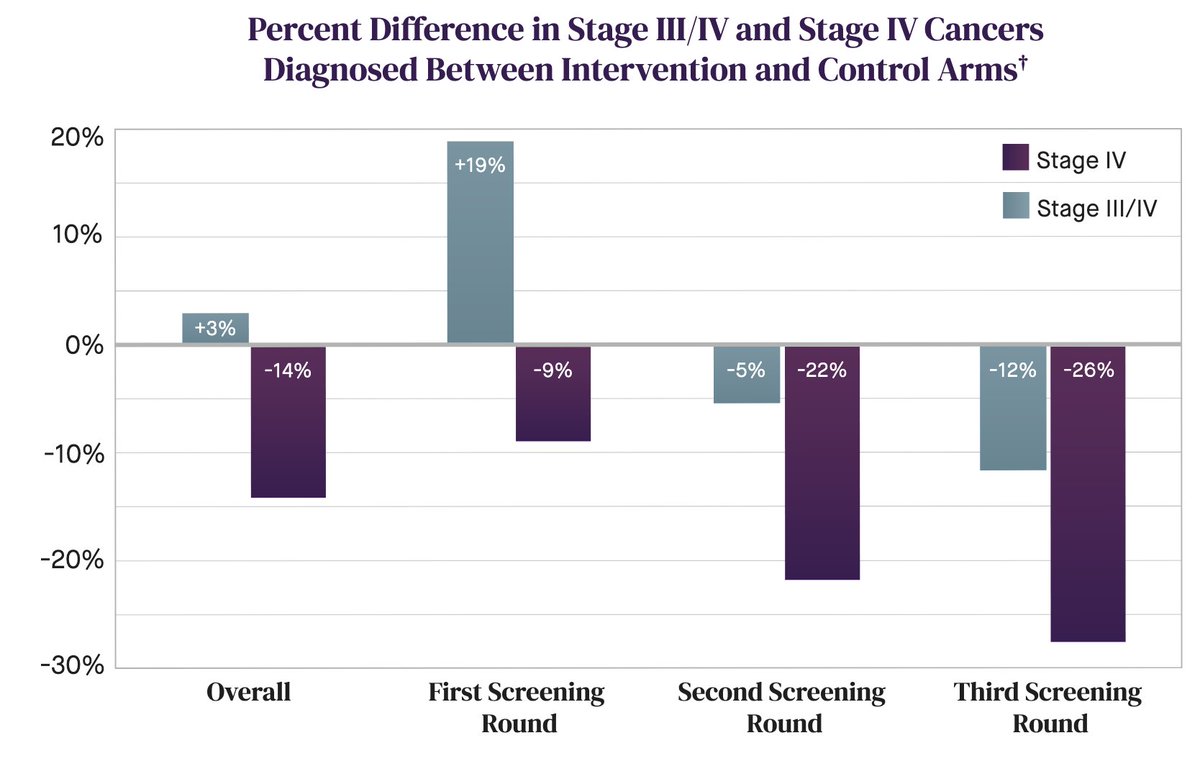
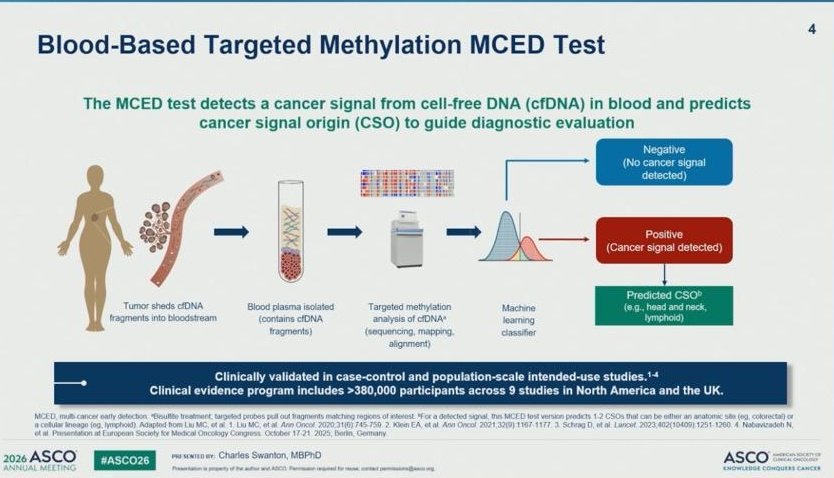
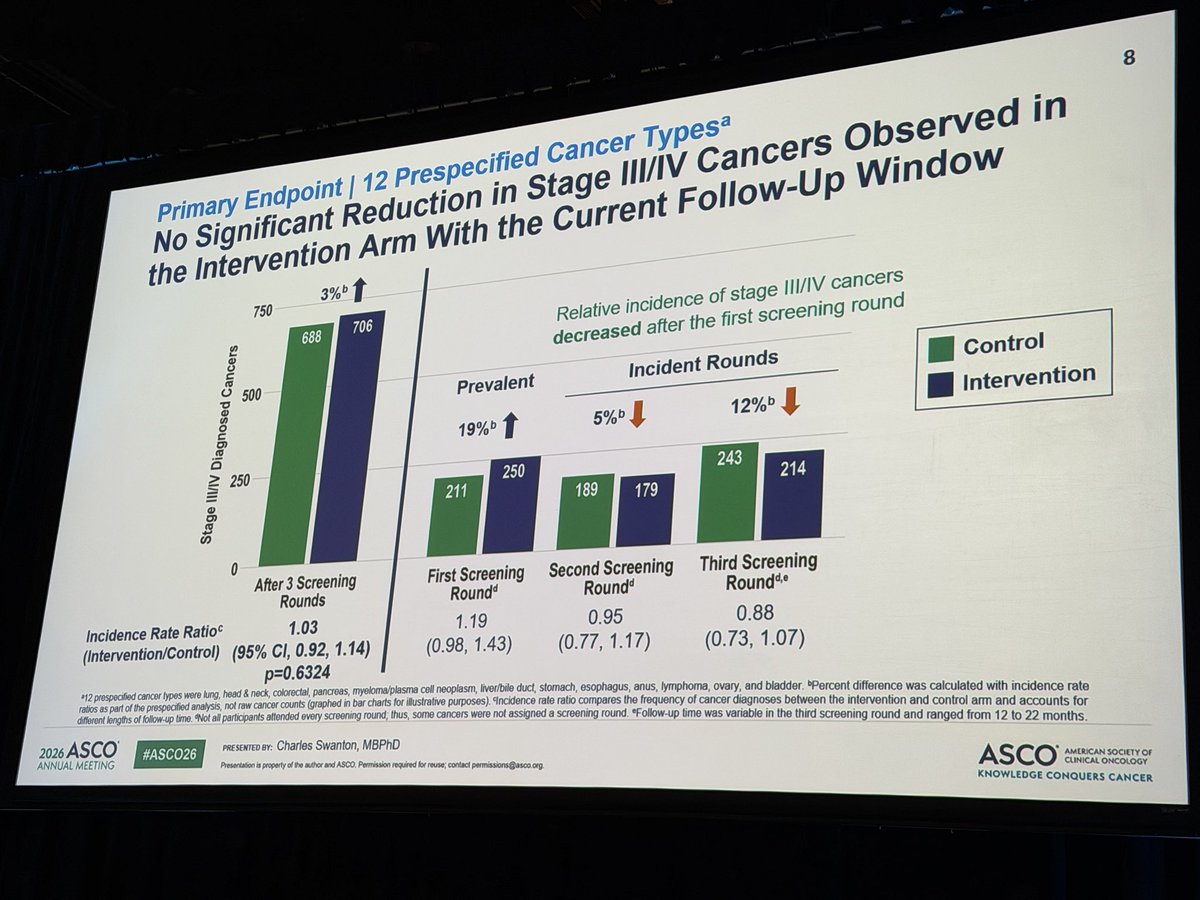
The full NHS GALLERI randomized trial data has been released at #ASCO26 by @GrailBio.
142,000 adults provided 3 blood samples over 2 years, for prevalent (baseline) & incident cancers. The trial did not meet its primary endpoint. Lots more data below:
mma.prnewswire.com/media/299…
10
16
3,280
Anthony J Gill retweeted

May 30
#ASCO26
Outstanding session on #ctDNA 🩸
🗣️ Great talk @CharlesSwanton
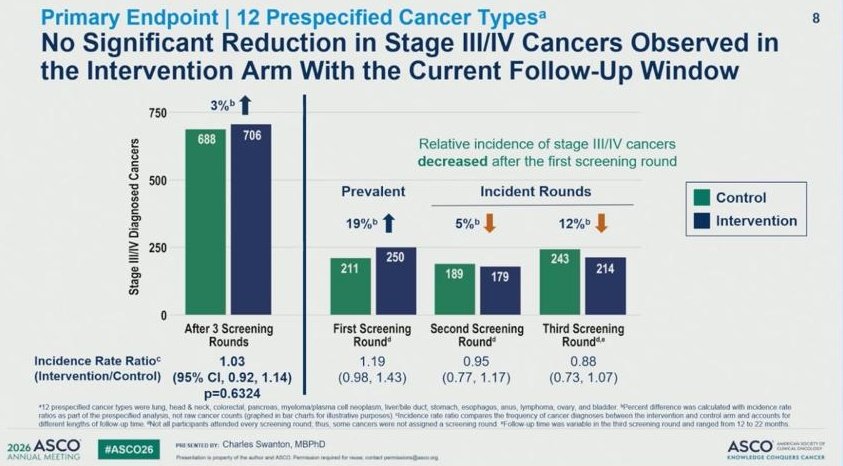
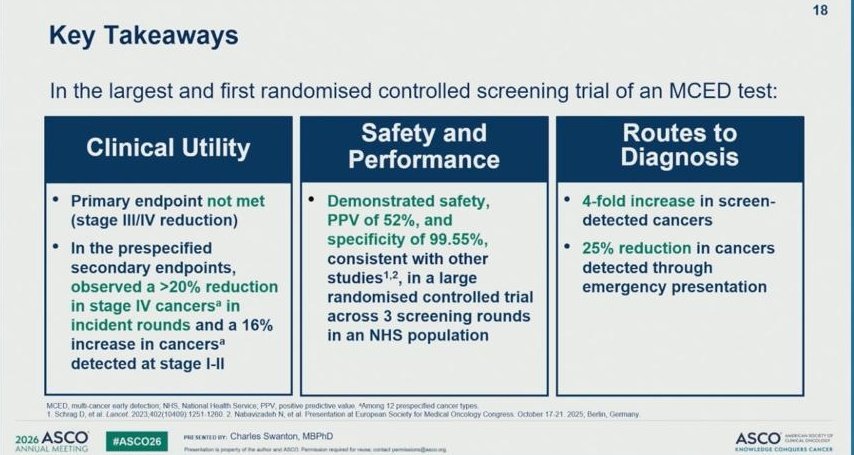
❌ Primary endpoint not met: Not increase of stage III/IV detection
📌 However:
✅ > 20% reduction in stage IV cancers
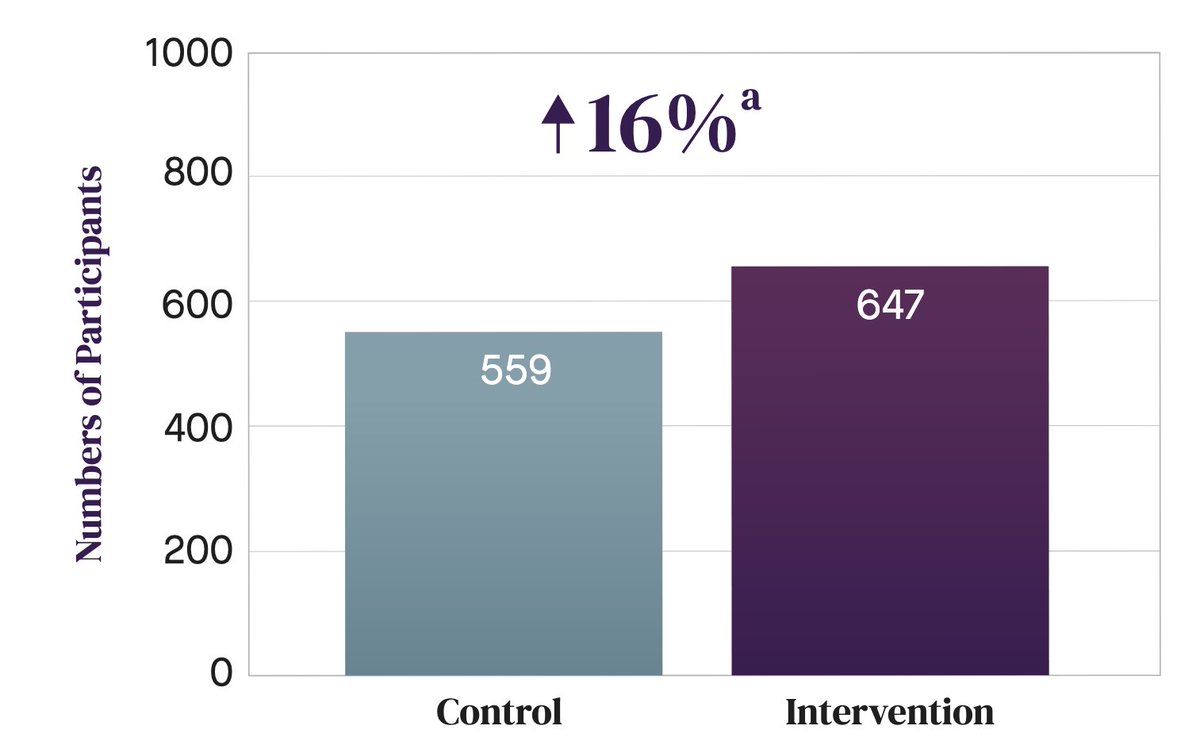
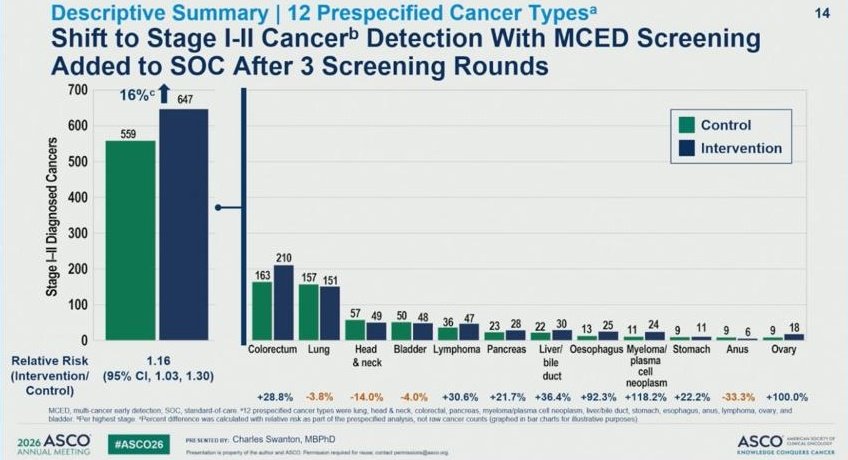
✅ 16% increase of stage I/II detection
✅ 4-fold ⬆️ in screening
@OncoAlert @EORTC @ASCO
1
15
30
2,796
Anthony J Gill retweeted

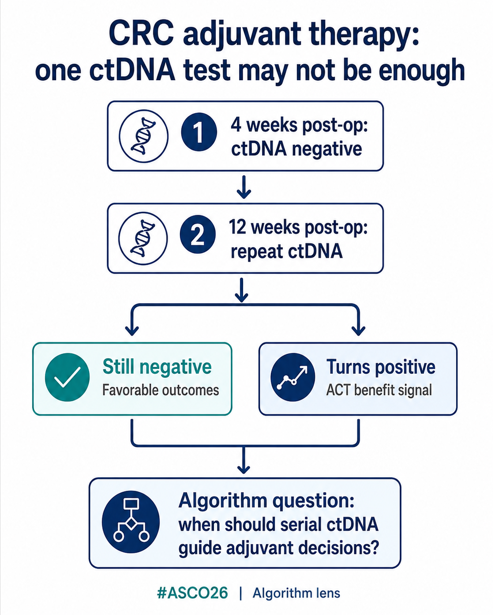
#ASCO26 through an algorithm lens
Abstract 102 | GALAXY / CIRCULATE-Japan
ctDNA dynamics at 4 and 12 weeks after resection in colorectal cancer
This is not just a “ctDNA-positive vs ctDNA-negative” story.
It is about timing.
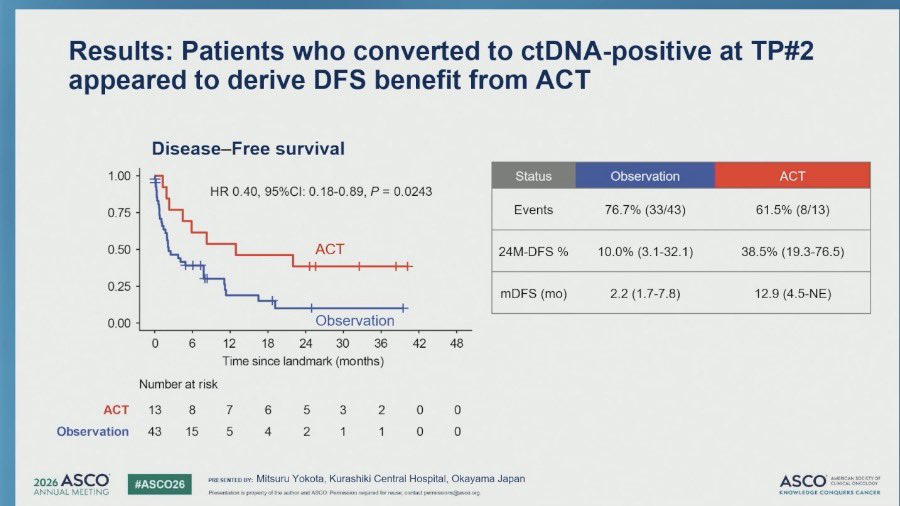
In resected stage I–IV CRC, patients who were ctDNA-negative at ~4 weeks but converted to ctDNA-positive at ~12 weeks appeared to derive benefit from adjuvant chemotherapy.
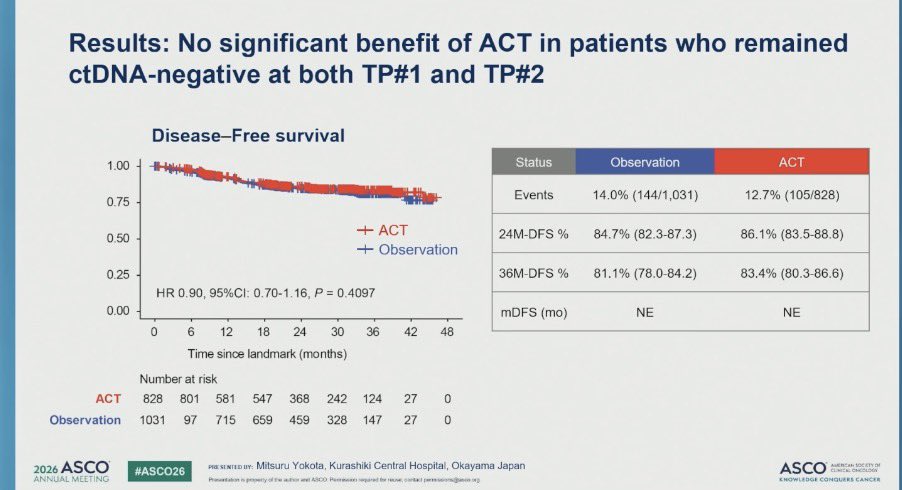
By contrast, patients who remained ctDNA-negative at both timepoints had favorable outcomes regardless of ACT.
Algorithm lens:
One postoperative ctDNA result may not be enough.
Serial ctDNA testing could help identify:
• patients who may safely avoid unnecessary treatment
• patients who need delayed or intensified adjuvant therapy
• patients whose molecular relapse emerges before clinical recurrence
Important caveat: the converted-positive subgroup was small, and this should not yet be used as a standalone rule. Clinical risk, pathology, timing, assay access, and prospective validation still matter.
Bottom line:
ctDNA may be most clinically useful not as a single test, but as a dynamic decision tool.
@mgfakih @drallysonocean @MPishvaian @GIMedOnc @YJanjigianMD @glopesmd
#ColorectalCancer #CRC #ctDNA #ASCO26
4
6
365


Anthony J Gill retweeted

May 30
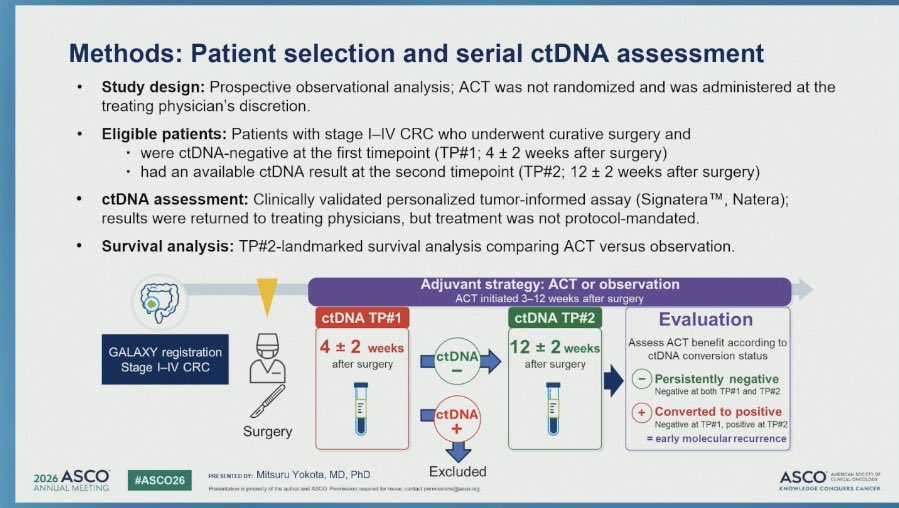
Early serial ctDNA dynamics resected stage I-IV CRC
➡️observational data GALAXY; tumor informed
➡️1915 pts ctDNA-ve at 4wks
✅persistent -ve:24mth DFS ~85%
➡️~3% ve (n=56) at 12wks -benefit chemo; more stg 4
✅serial ctDNA early prognostic info
#CRC #ASCO26 @ASCO @OncoAlert

13
18
1,588
Anthony J Gill retweeted

May 30
‼️ Big news in the early detection world: Galleri (a methylation-based multi-cancer detection test) failed to meet its primary endpoint of reduction of stage III/IV cancer diagnosis in a large prospective randomized trial with the NHS. #ASCO2026
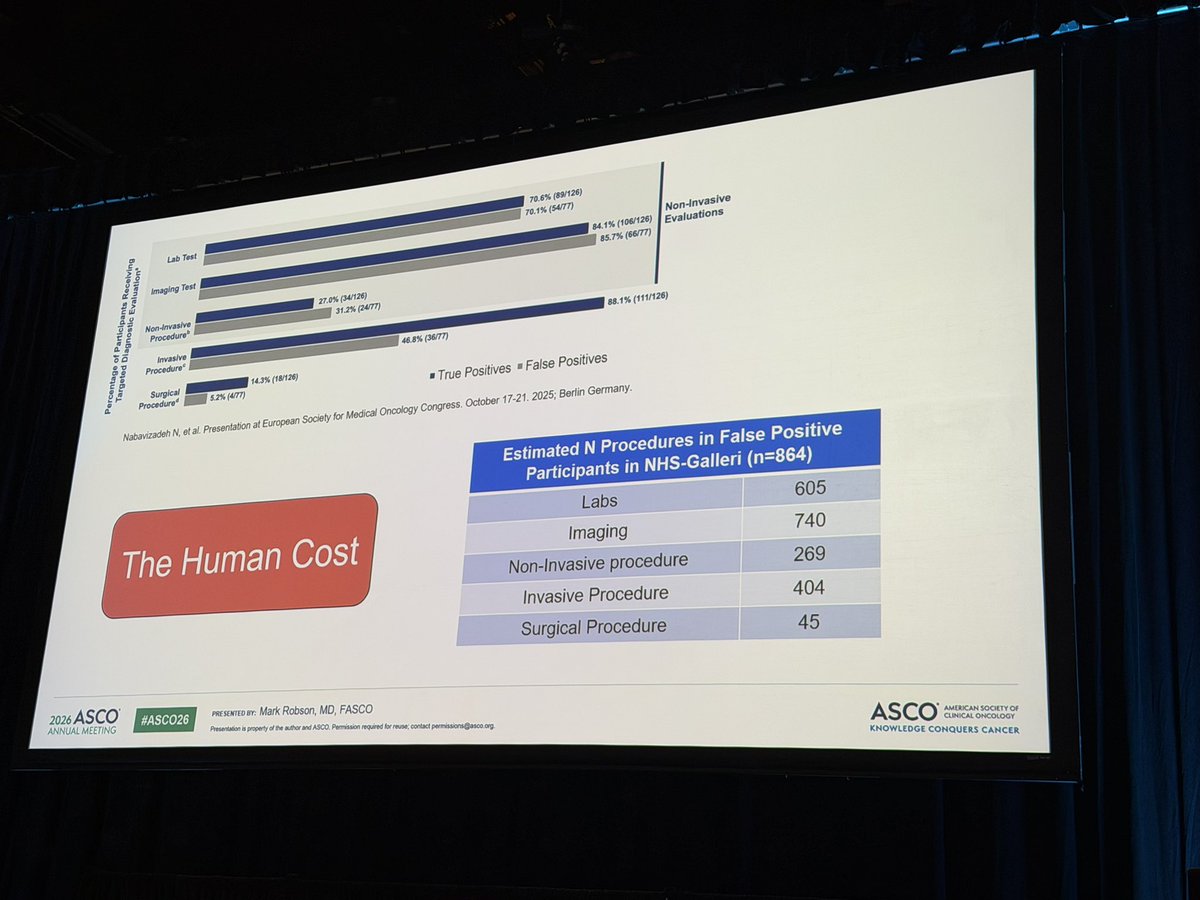
- PPV ~50%, and among the false positives, about half (n=404) underwent invasive procedures as part of their workup. 😬
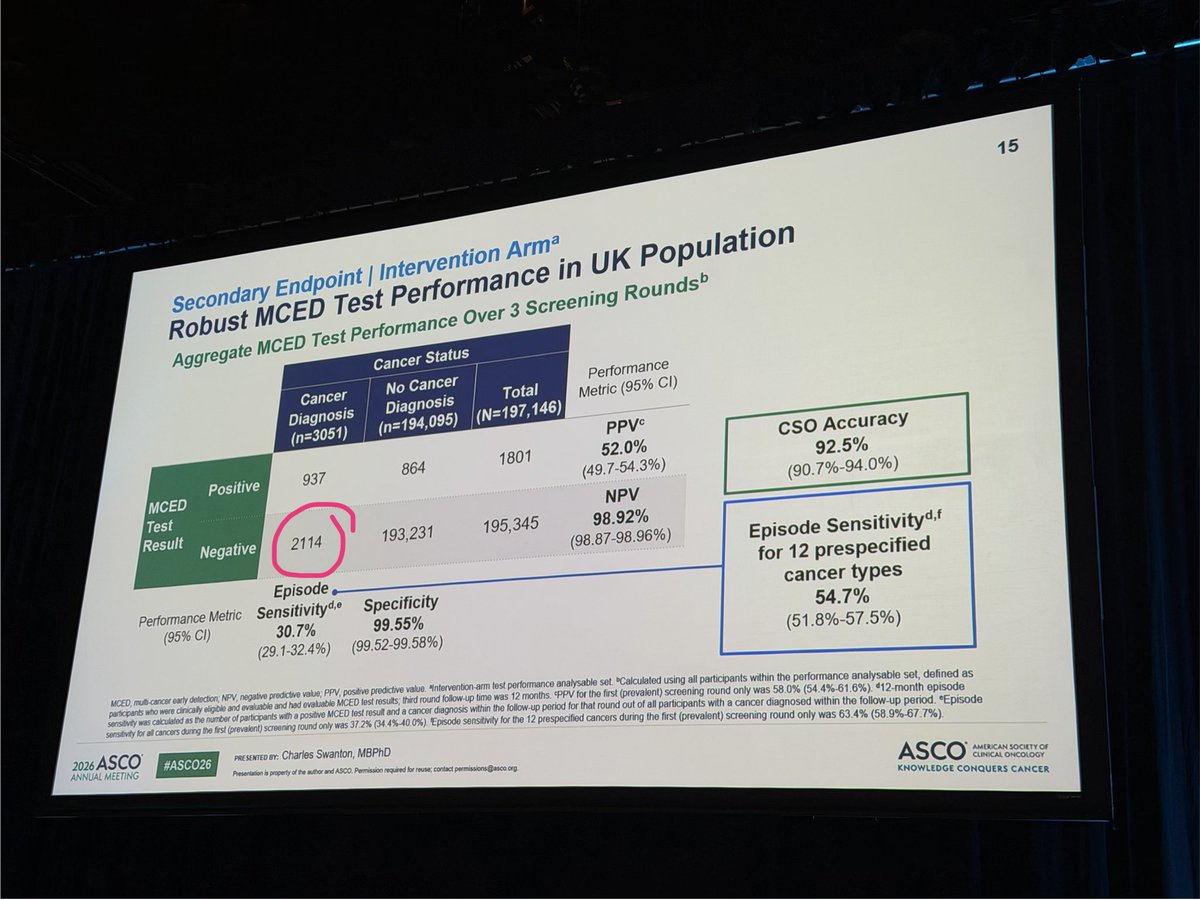
- ~2/3 of people diagnosed with cancer had a negative Galleri test (false negative)
- Some early signals of greater benefit in certain cancers but overall not powered for that.
- Galleri arm detected more cancers, but the clinical benefit of this is not yet clear.
- Important to remember that surrogate endpoints (stage III/IV diagnoses and stage IV diagnoses) do not correlate well with survival in all cancer types.
⭐️ My take: I think this type of cancer detection assay will have clinical value in some context(s), but we still have a ways to go before we know how to use it. Use in higher risk patients? Limit assay to detect only certain cancers? Lots of work to be done. 💪

1
6
1,291
Anthony J Gill retweeted

1
22
45
3,337
Anthony J Gill retweeted

May 28
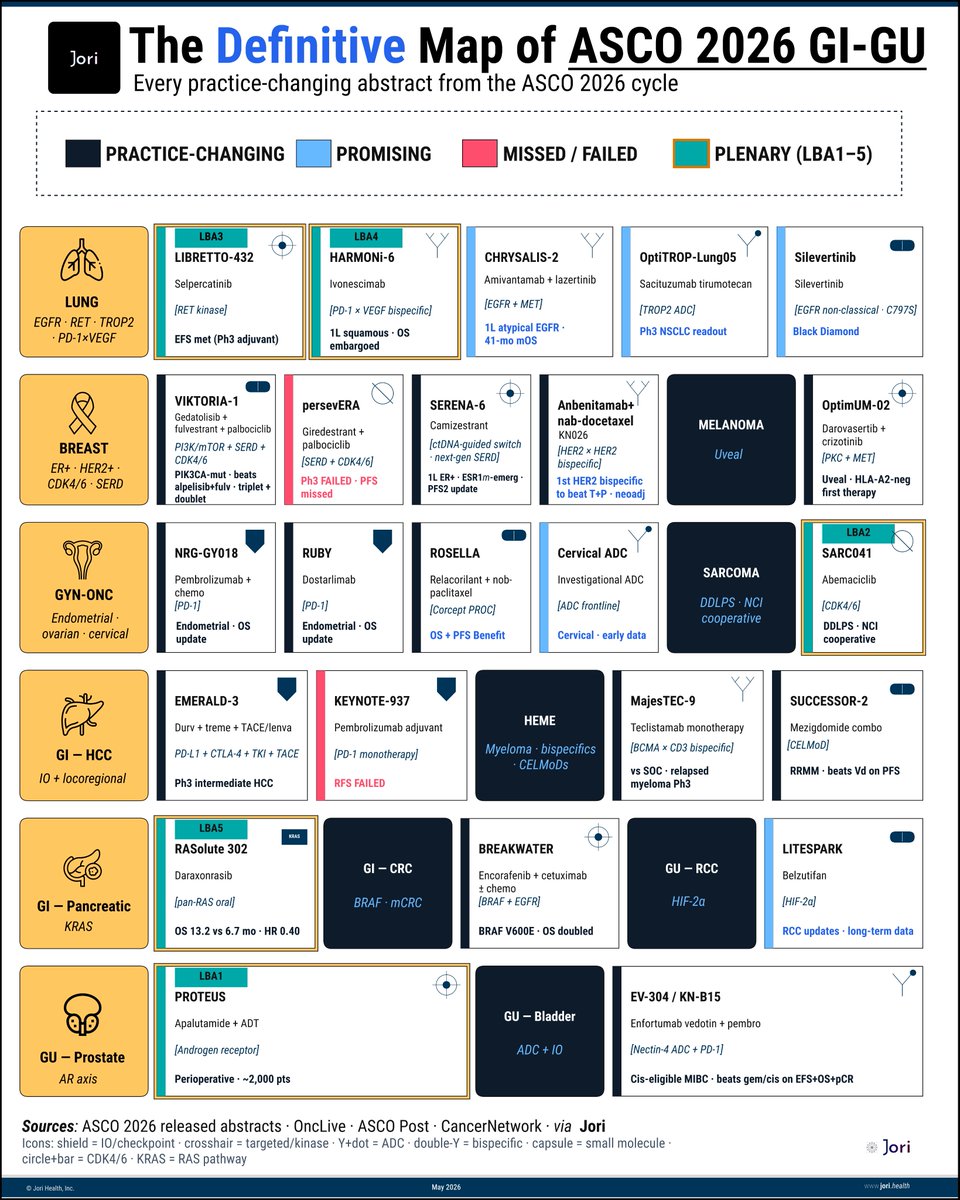
The Definitive Map of ASCO 2026
(peer-reviewed edition).
No single human alive can/has read all 7k abstracts.
That is precisely why this map needs to exist.
First version (below) had errors. 20 world-class oncologists reached out (private DMs, pointed corrections, public critiques).
We then did 23 rounds of revision in 48 hours.
Posting this to correct the record.
This new map is the result of machines & experts coming together.
Changelog v2 -> v1:
▫️SERENA-6: relabeled from "2L" to 1L ESR1m ctDNA-guided switch (trial's actual innovation)
▫️ ROSELLA: fixed drug (relacorilant, not mirvetuximab) and icon (small molecule, not ADC)
▫️ Silevertinib: corrected geography (Black Diamond/US, not China) and lead indication (non-classical EGFR)
▫️ CHRYSALIS-2: updated to Cohort C 1L atypical EGFR, 41-mo mOS
▫️ Anbenitamab nab-doc: promoted to practice-changing (1st HER2 bispecific to beat T P head-to-head)
▫️ EV-304: sharpened — beats gem/cis on EFS OS pCR (a 40-year SOC, displaced)
▫️ VIKTORIA-1: PIK3CA-mut, beats alpelisib fulv, triplet AND doublet
▫️ Scope widened to the full ASCO 2026 cycle (GI · GU · Annual)
💡Machines can extract patterns from 7k abstracts in 15 mins. But, it takes real human expertise closes the last mile.
To every oncologist who sent a fix: this map belongs to all of you.
<3 @Jori_health
ps, if you spot an error, holler at us
x.com/mukundiyngr/status/205…
May 26

ASCO this year has 5,000 abstracts.
But maybe 24 will actually change practice. This is that map.
(ERRATA: this plot fixes an error on VICTORIA which reflected incorrect data, thnx @Dr_RShatsky)
Map spans 12 disease areas, 24 critical readouts, 5 plenaries & 2 confirmed misses already on the board.
Few things jump out immediately:
▫️Pancreatic cancer gets the headline.
Daraxonrasib: 13.2 vs 6.7 months.
▫️Sarcoma gets a plenary because public science funded what pharma would not.
▫️Lung cancer remains the most crowded battlefield in oncology:
RET adjuvant, bispecific OS, post-osimertinib, next-gen EGFR.
By next week, some of these cells will become new standards of care.
This is your cheat sheet to keep score in real time.
- - - - -
Sources: @asco @OncLive @CancerNetwrk via @Jori_health
- - - - -

2
17
45
3,961
Anthony J Gill retweeted

@cancerNSW is proud to award $7.5 million to new Translational Program Grants led by Professor Paul Keall (@paul_keall) and Professor Anthony Gill (@CaDxPath) from @Sydney_Uni.
➡️ Find out more: cancer.nsw.gov.au/what-we-do…

1
1
5
390
Anthony J Gill retweeted
Apr 12
Proud to present our latest article - now available for free download @AJSPjournal
Please retweet and download the article.
Synopsis:
The AJCC ninth edition staging system for colon cancer is not yet current, but there are significant changes proposed. These changes aim to both get rid of the stage 3A paradox (under the eighth edition patients with Stage 3A actually disease do better than Stage 1 and 2) and also to better integrate discontinuous Tumour Deposits (TDs) into staging.
What are these proposals and do they work?
Free download:
journals.lww.com/ajsp/fullte…
12
20
1,988
Anthony J Gill retweeted

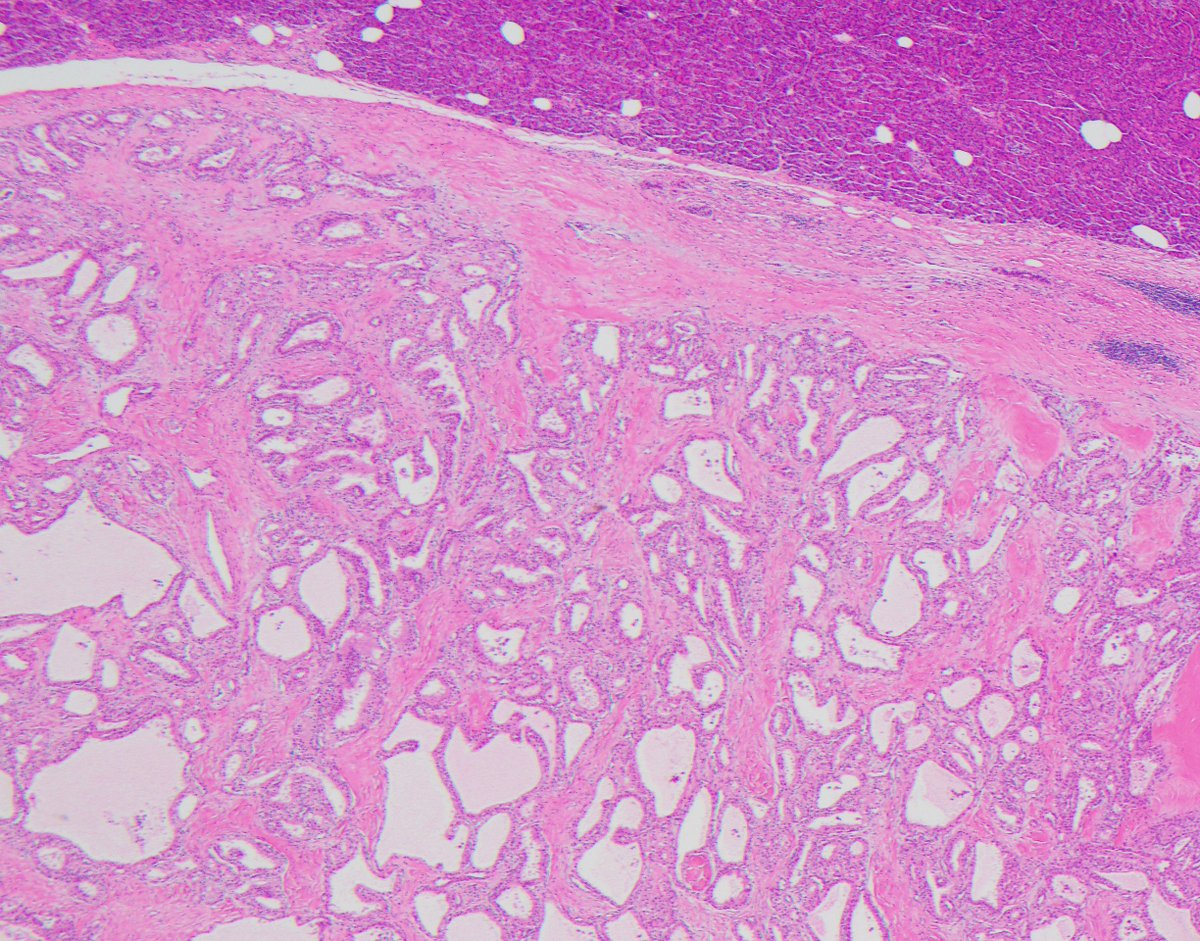
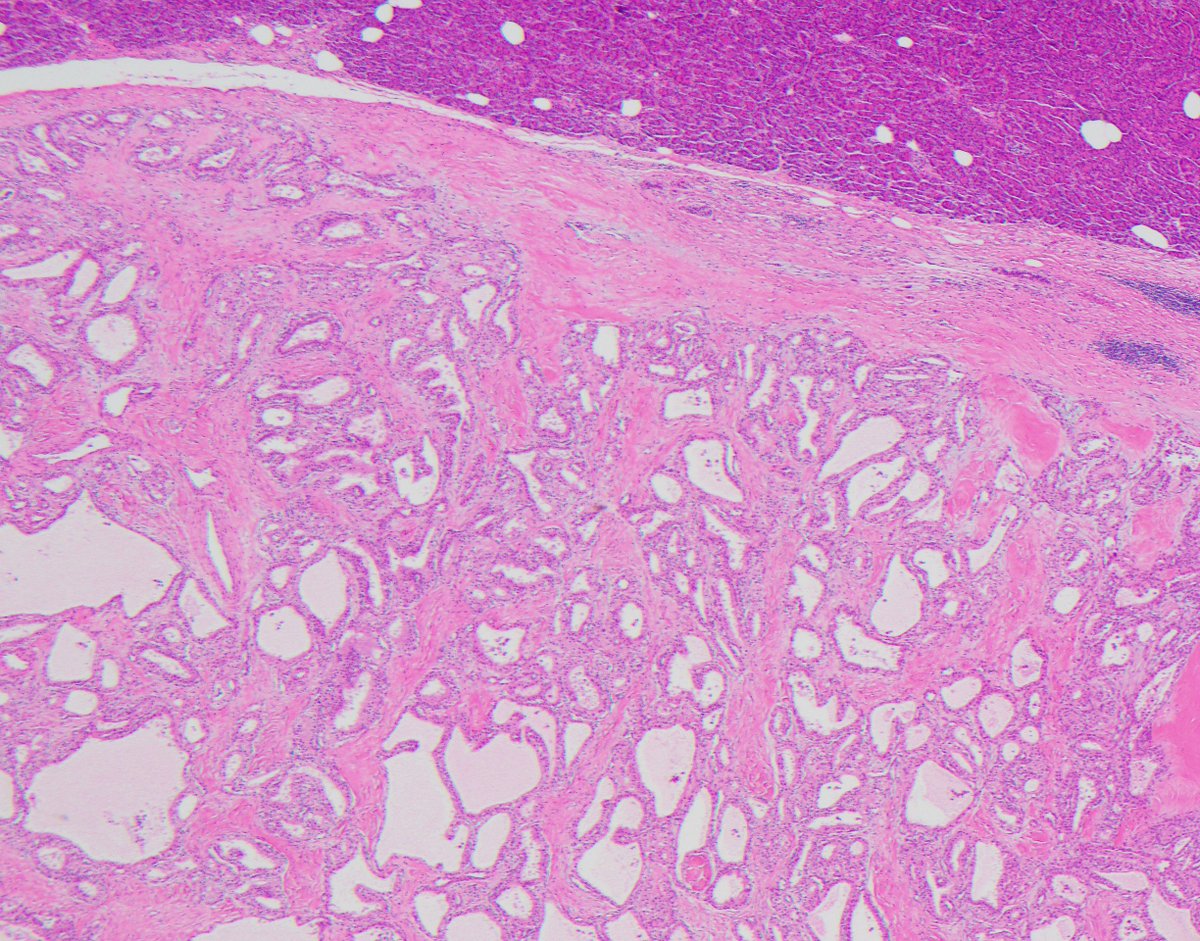
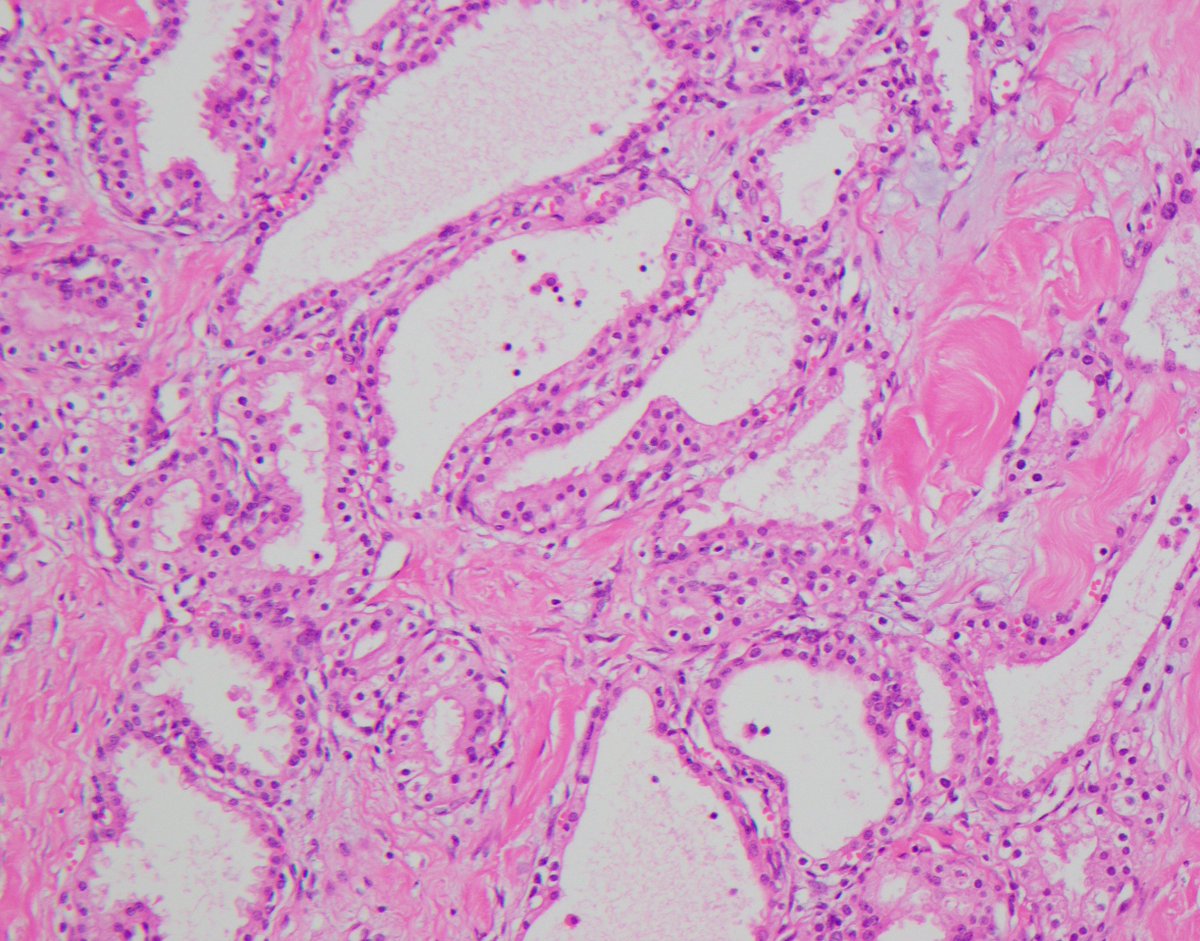
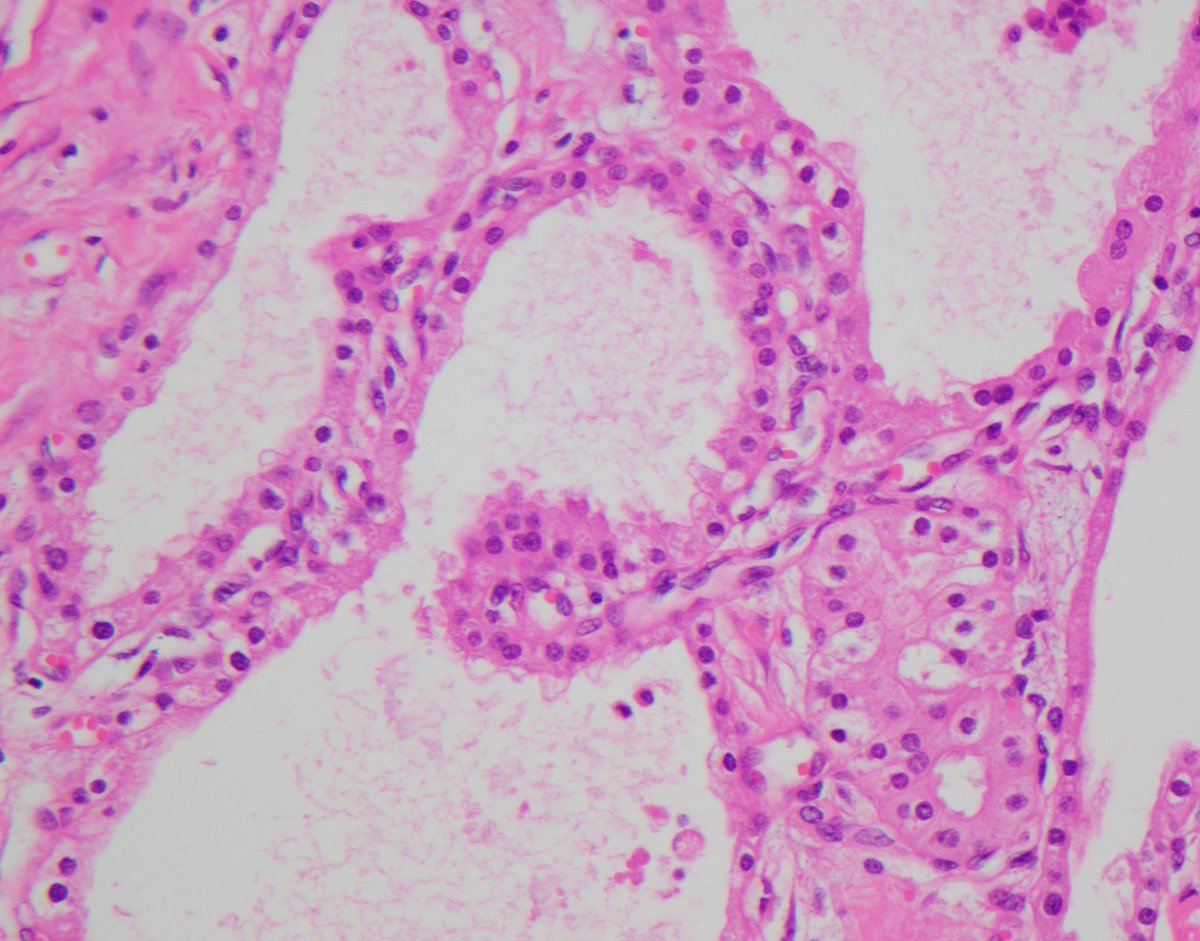
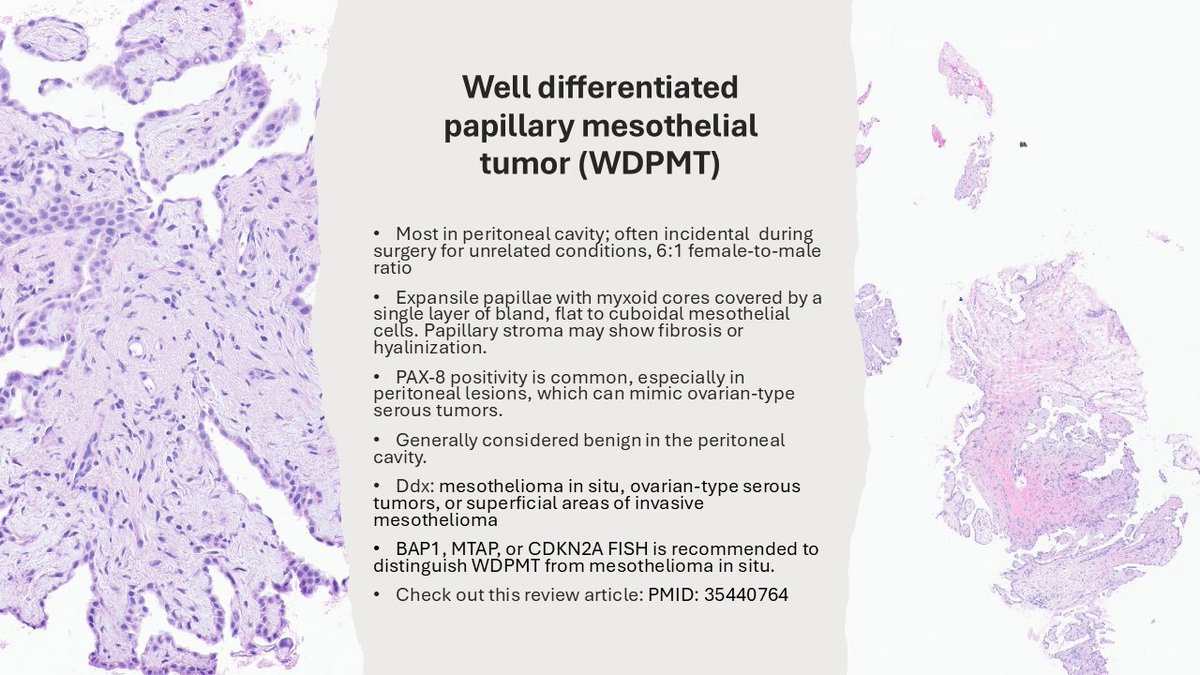
Well Differentiated Papillary Mesothelial Tumor (WDPMT) #TheJPCNCR #PathTwitter
1
20
42
1,661
Anthony J Gill retweeted

It was a wonderful to hear that an important clinical trial using neoadjuvant combination immunotherapy in selected glioblastoma brain patients has commenced in the USA. The pioneering work, led in Australia by my colleague Prof Georgina Long and the trial team formation led by Dr Jim Whittle, together with an extensive talented team, deserves huge congratulations for their work and initiating the development of the trial! The first patient, based in the USA where the study is led by Professor Mustafa Khasraw, has commenced trial participation. I hope patients in Australia can participate soon. Well done to everyone from the excellent teams involved. I hope the trial is positive for brain cancer patients!
Details of the information available can be found through a link to the Sydney Morning Herald with an article written by Garry Maddox.
#glioblastoma #braincancer
@ProfGLongMIA @MelanomaAus @WEHI_research @carriesB4BC @BrainCancerCtr @gmaddox @smh @NthSydHealth @COBLH @Sydney_Uni @BickmoreCarrie
9
92
629
11,810
Anthony J Gill retweeted

1/ Just out in @ModernPathology
New study from our group: A distinct variant of aggressive lung carcinoma with peculiar pathologic features.
We called these tumors “SAGA” (solid and granular adenocarcinoma) .. sorting them out was in fact a long and winding saga that led to some unexpected insights. 👇
modernpathology.org/article/…
pubmed.ncbi.nlm.nih.gov/4158…

3
44
87
8,898
Feb 2
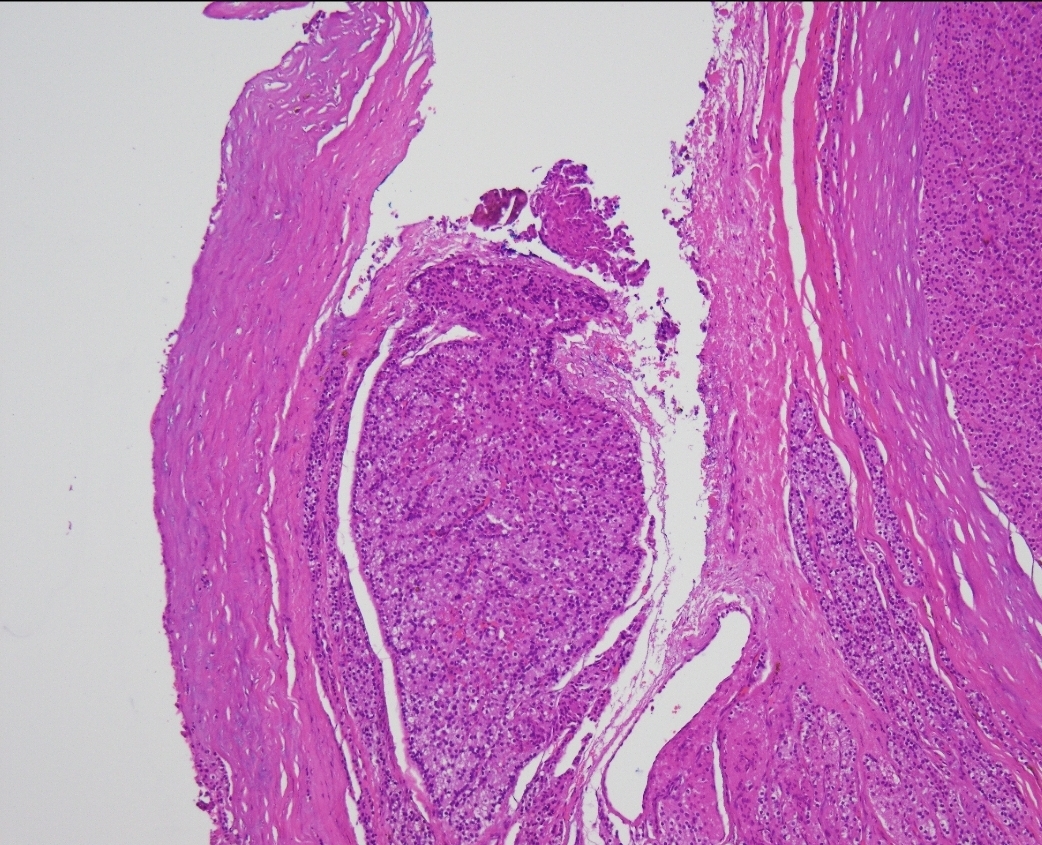
Great Article on this not uncommon problem. I think after reading the article:
authors.elsevier.com/a/1mWXy…
pathologists may have different ideas about whether it is benign or malignant.
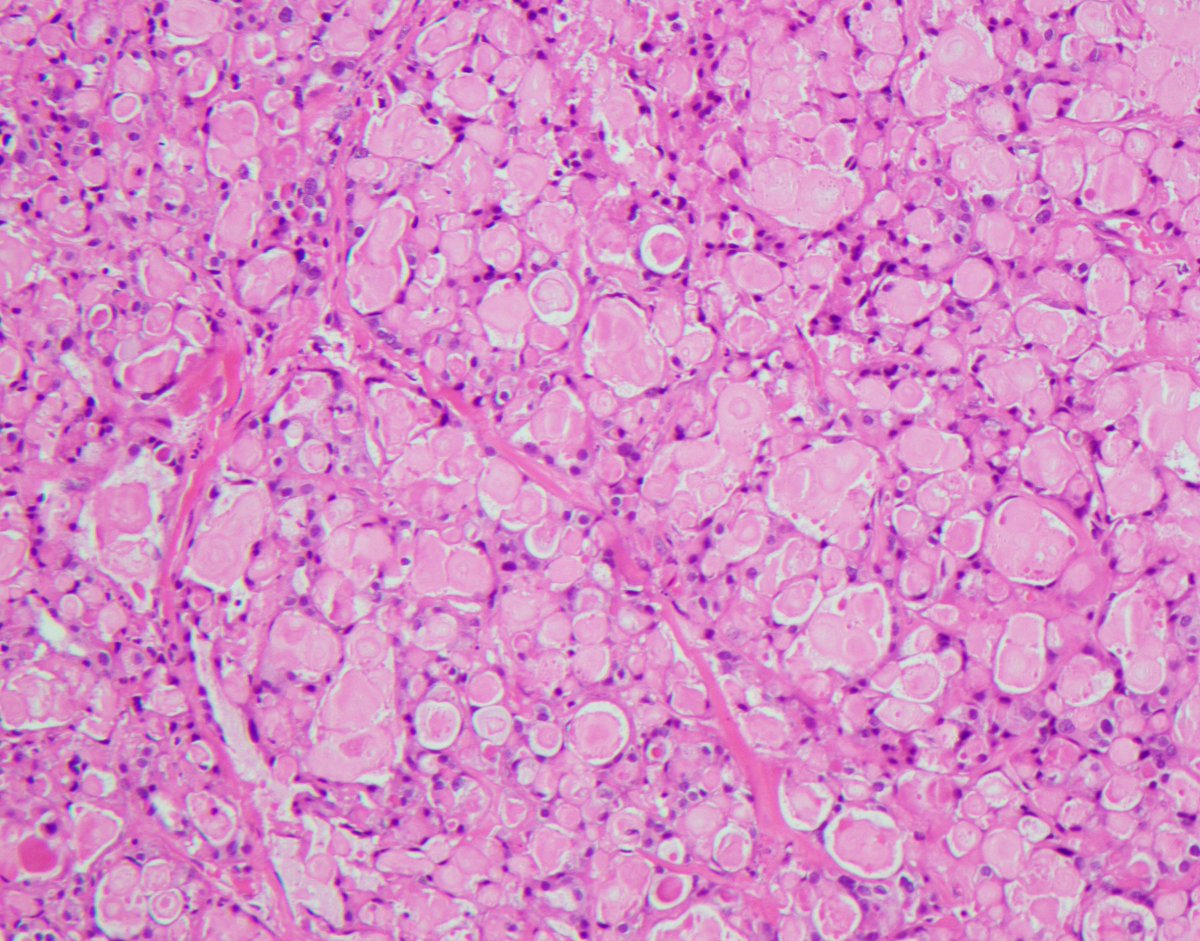
Feb 2

Would you diagnose this lesion as parathyroid carcinoma in a patient with chronic renal failure? Find out here - authors.elsevier.com/a/1mWXy…
7
1,161