
Primary care NP, lover of balanced glucagon agonism, incretin nerd, photographer, mountain lover, coonhound rescuer
Joined October 2021
- Tweets 3,583
- Following 231
- Followers 1,010
- Likes 7,517
611 Photos and videos

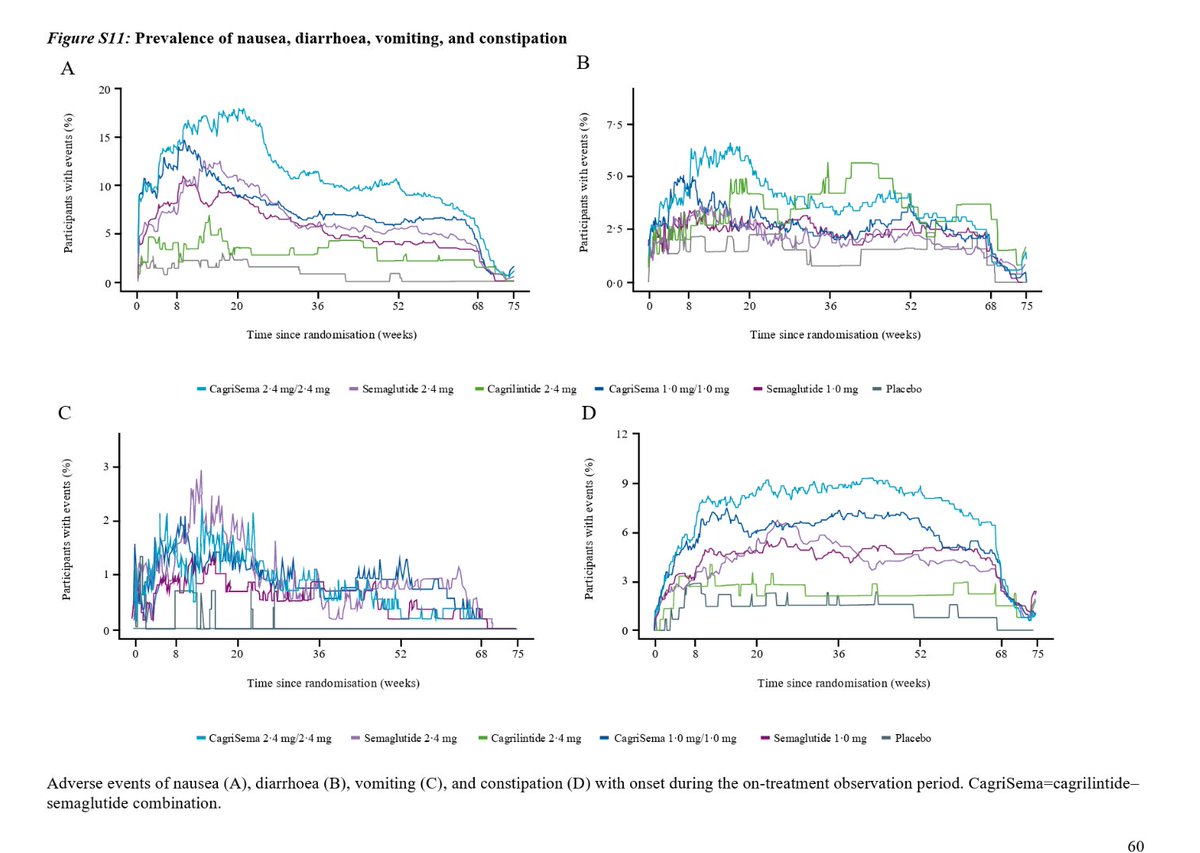


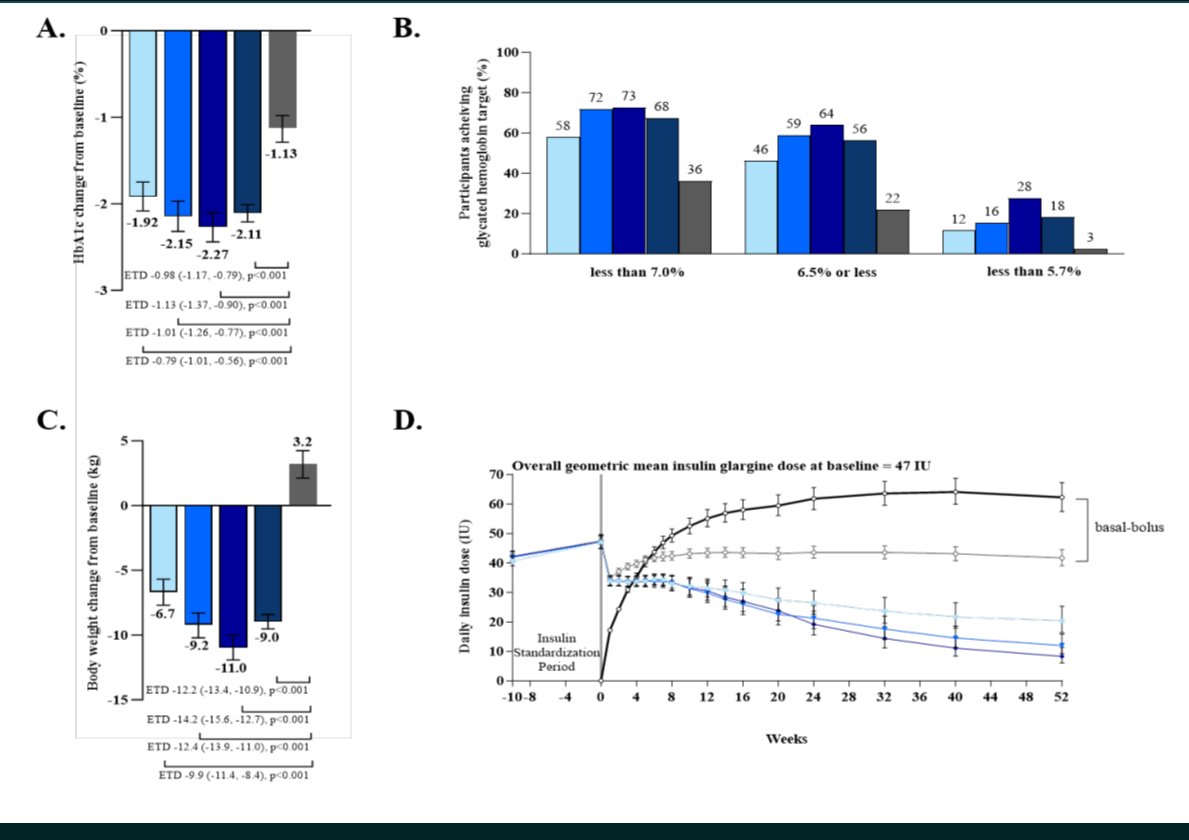




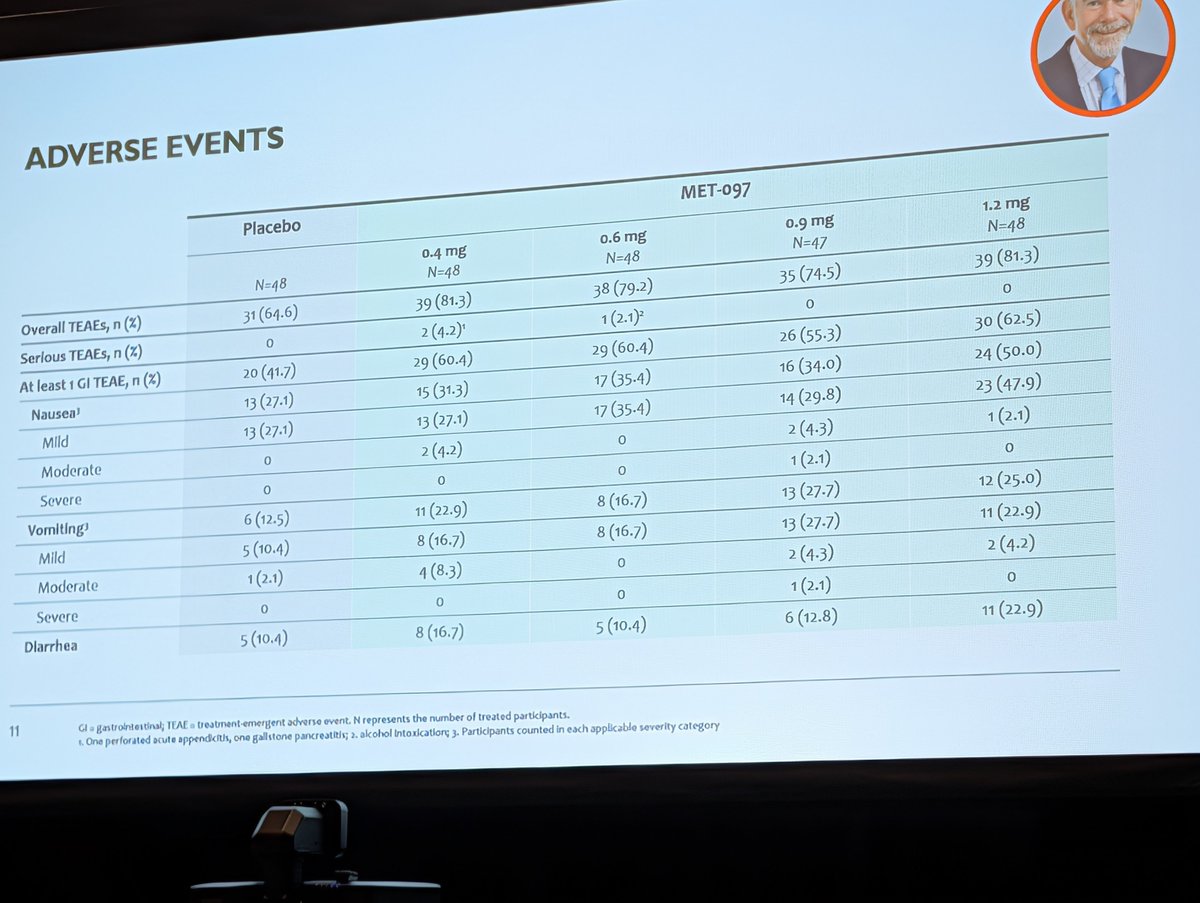
Pay no attention to the man behind the curtain...but I suspect these rates of side effects have something to do with it. It's funny to say but survodutide suffers from rigid titration schedule, and same is true with CagriSema flexible dosing. Both molecule have tolerance issues!
8
665
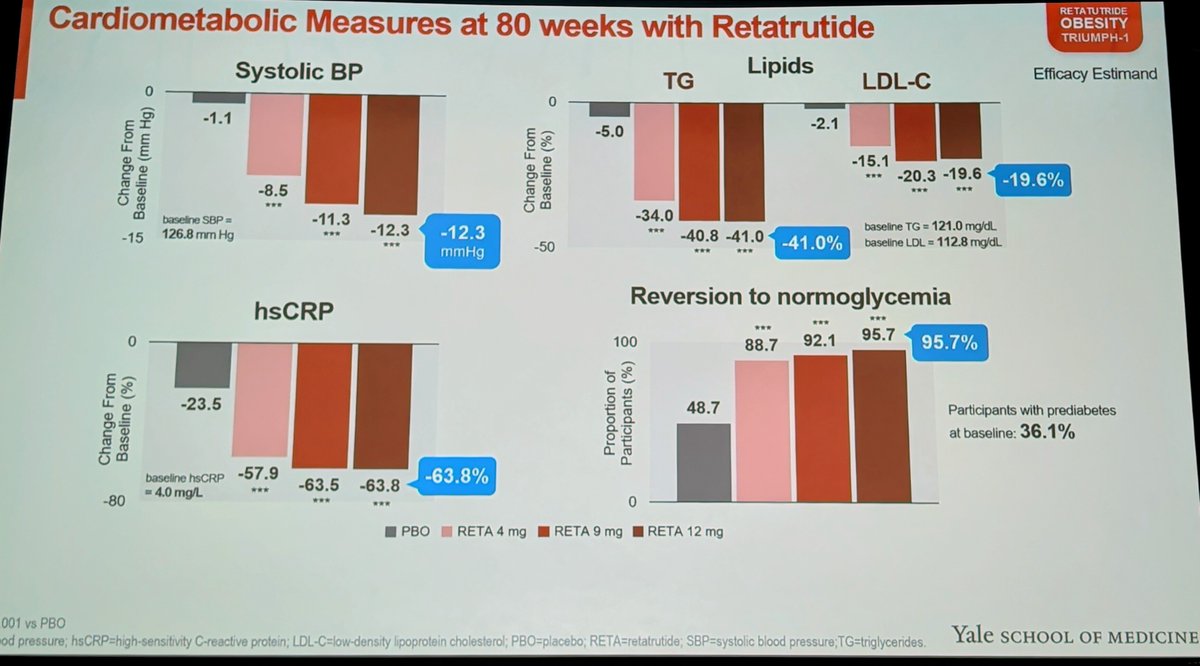
I'll have A LOT of retatrutide thoughts. But these cardiometabolic improvements are stunning. 40% drop in triglycerides, 20% drop in LDL. 63% drop in hsCRP, 12 point reduction in BP. It's not a stretch to imagine this drug massively reducing death from CVD and CKD all on its own.
25
75
750
71,996
Sept 23 2023. That's when I took my first dose of retatrutide. Nearly 1000 days ago.
I had no idea how much it would change my life that day. I'm now 30% lighter. My asthma & fatty liver disease are long gone. My chronic achilles tendonitis disappeared 3 months into the trial.
29
14
494
66,899
I have to take Zetia for my cholesterol because I'm not on high dose Reta anymore Reta decreases my LDL cholesterol by 55% and my triglycerides by almost 80%
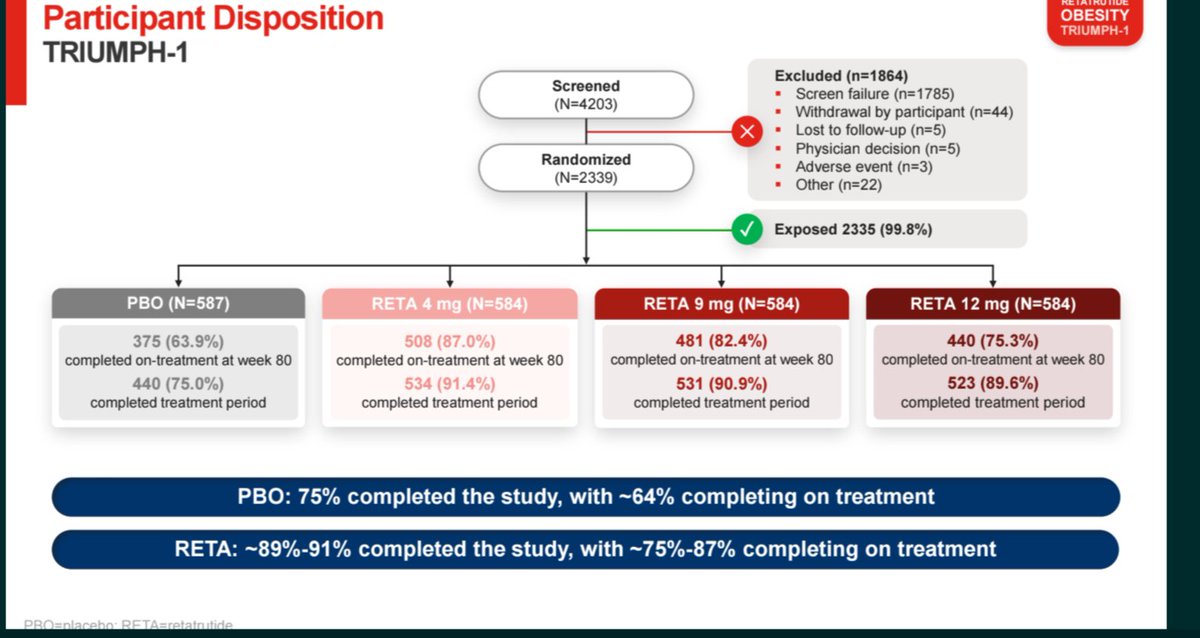
Today in a few hours I get to see my trial data get published for the first time. It's a very full circle moment for me.
4
1
55
5,451
I'm sure there will be debates on side effects, beneficial effects & more for months if not years to come. But regardless, today, we can confidently say we have a drug that can capitulate bariatric surgery outcomes & that is a remarkable & historic triumph of science & medicine.
3
62
5,087
FlexNP retweeted

Jun 4
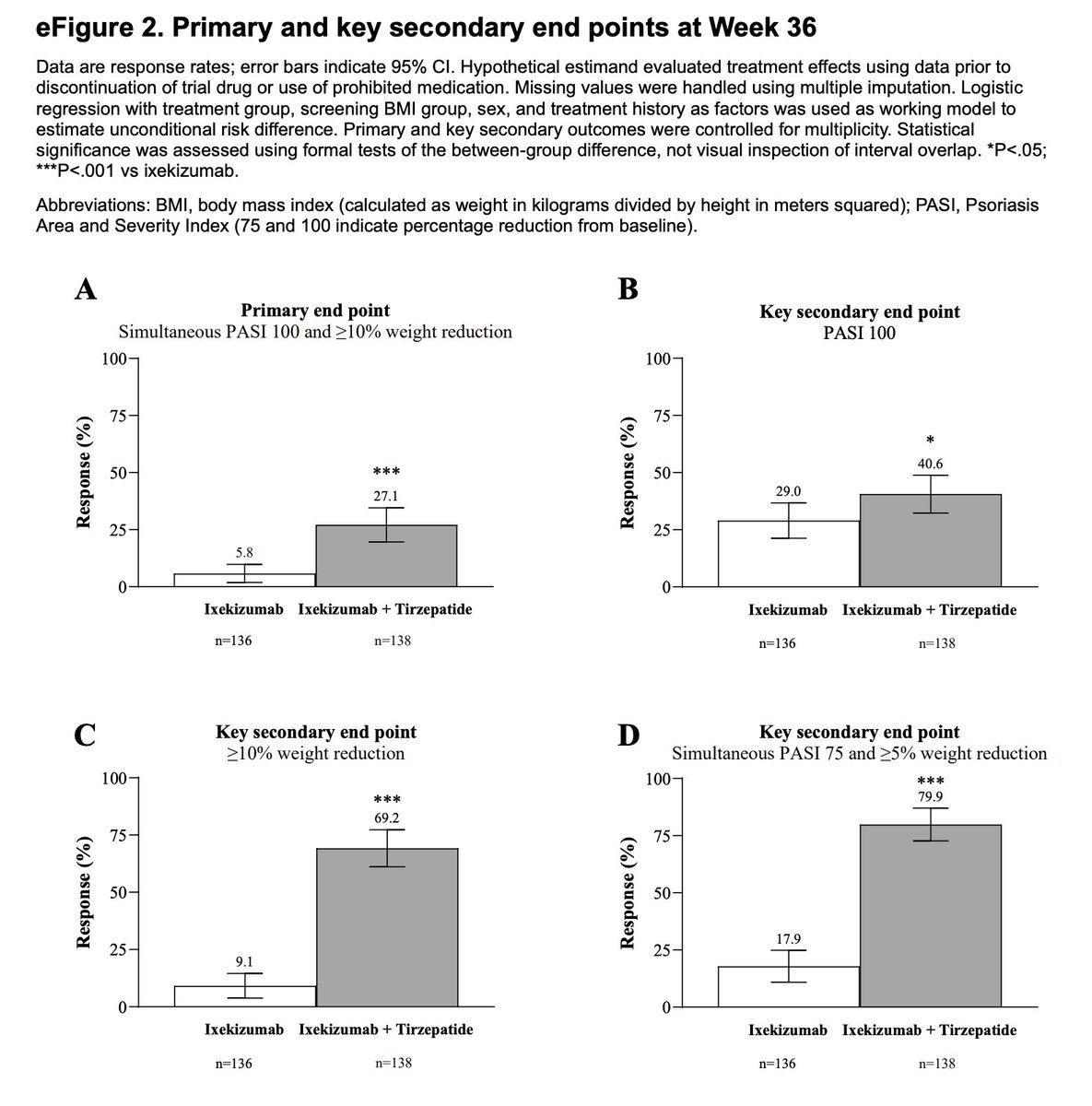
Can GLP-1 drugs improve psoriasis beyond standard therapy alone?
In this RCT of 274 psoriasis patients, those randomized to Tirzepatide Ixekizumab had a higher rate of full skin clearance (PASI 100) compared to Ixekizumab alone (40.6% vs 29.0%).
13
17
100
18,178
So anyways GLP1/GIP/Glucagon agonists are fasting mimicks as glucagon induced ketosis and GIP and glucagon agonism both drive down insulin secretion.
Just saying.
Jun 1

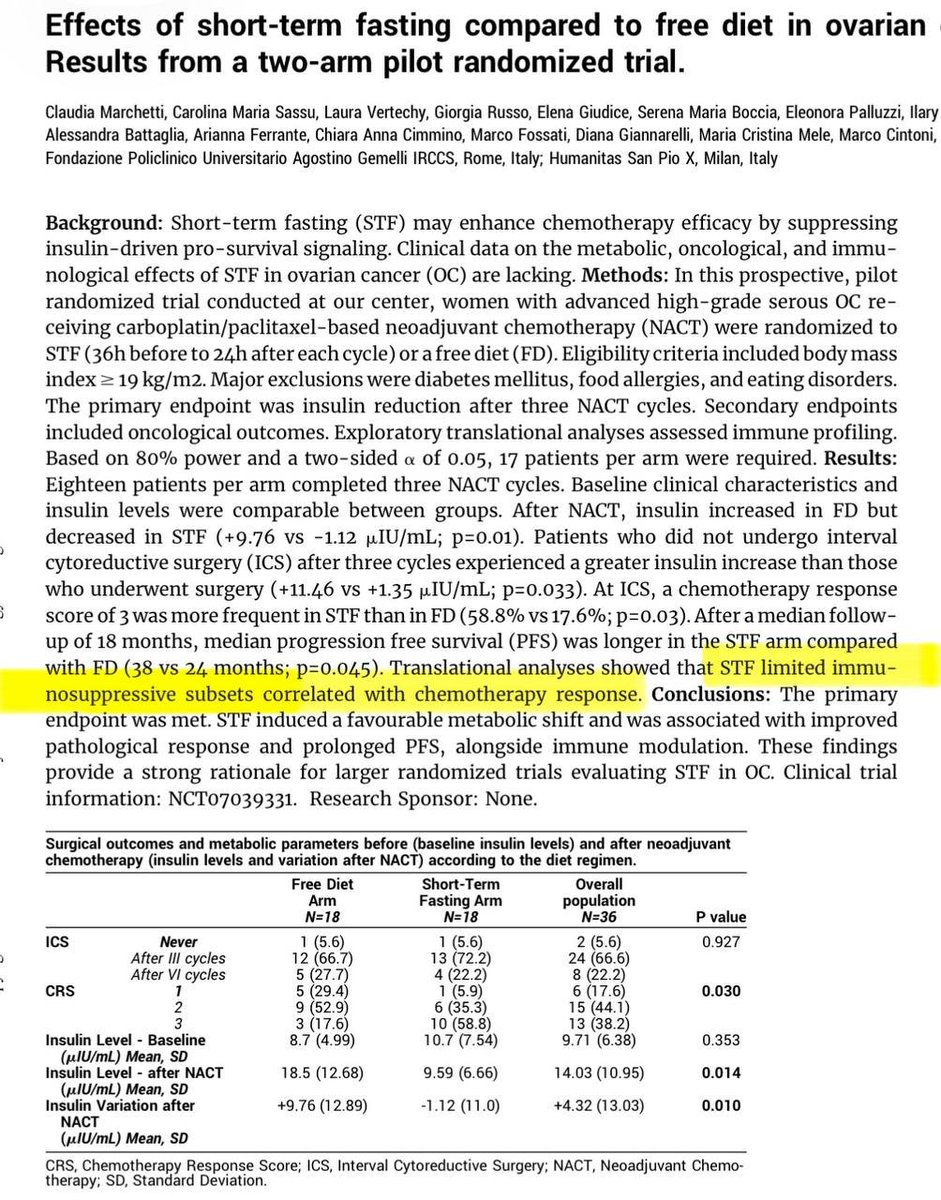
Short-term fasting during neoadjuvant chemotherapy for advanced ovarian cancer is one of the more intriguing non-drug interventions presented at #ASCO2026.
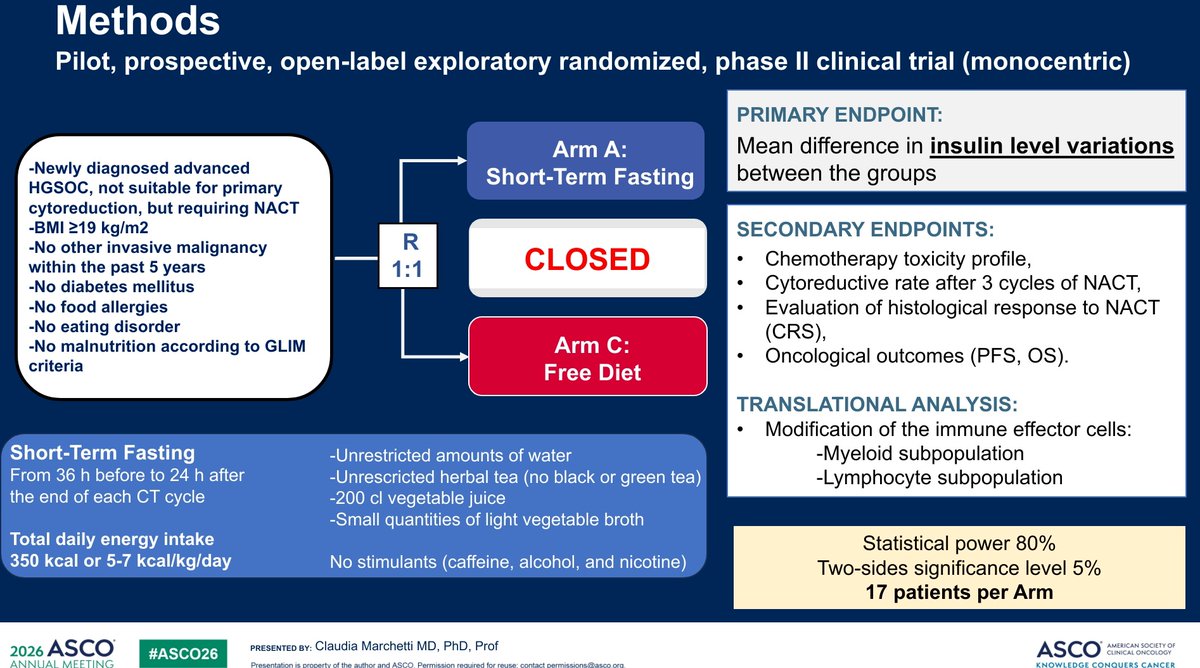
The study met its primary endpoint: fasting prevented the chemotherapy-associated rise in insulin levels and demonstrated a favorable metabolic shift.
The headline result was a PFS signal:
• mPFS 38 months with fasting vs 24 months with free diet •
HR 0.26 • Log-rank p=0.045
Before we get too excited, several important limitations deserve attention:
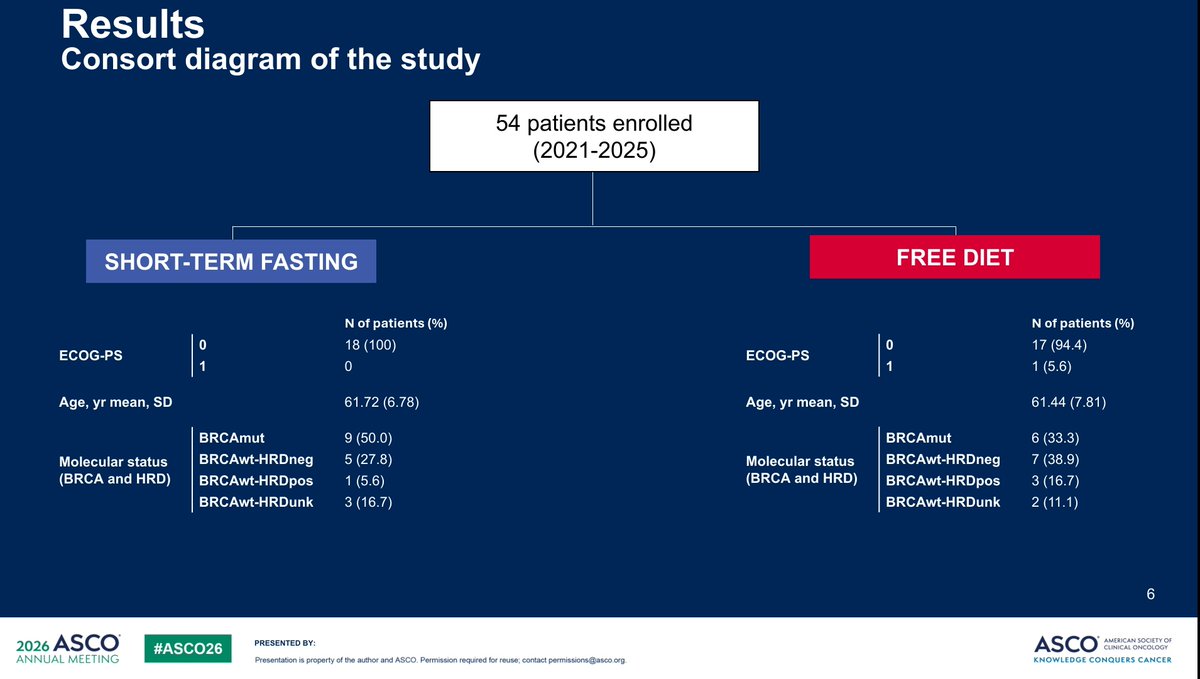
🔹 Only ~18 patients per arm after exclusions
🔹 Trial was powered for insulin changes, not PFS
🔹 Open-label design
🔹 Borderline statistics (95% CI 0.06–1.00; Cox p=0.056)
🔹 Multiple secondary and exploratory analyses increase the risk of false-positive findings
🔹 BRCA-mutated patients were more common in the fasting arm (50% vs 33%), which could influence outcomes
🔹 Median follow-up was only 16 months despite reporting a large difference in mPFS
🔹 Immune findings were hypothesis-generating with p-values around 0.06–0.07
🔹 Analysis appears vulnerable to selection bias from withdrawals and compliance-related exclusions
The most convincing finding is that short-term fasting is feasible and biologically active, affecting insulin and metabolic pathways.
The least convincing finding is a 14-month absolute PFS improvement from a dietary intervention in a 36-patient study.
Interesting study.
But extraordinary efficacy claims require validation in a larger multicenter randomized trial before fasting enters routine ovarian cancer practice.
@OncoAlert
@ASCO #asco26
2
12
4,547

Well there's the next phase 3 Eloralintide trial, @JCanNuSH Sleep apnea trial. Given the length of time of these trials(75 weeks) seems Lilly is anticipating 15-20% weight loss which would be what's needed for OSA improvements
clinicaltrials.gov/study/NCT…

1
8
1,438
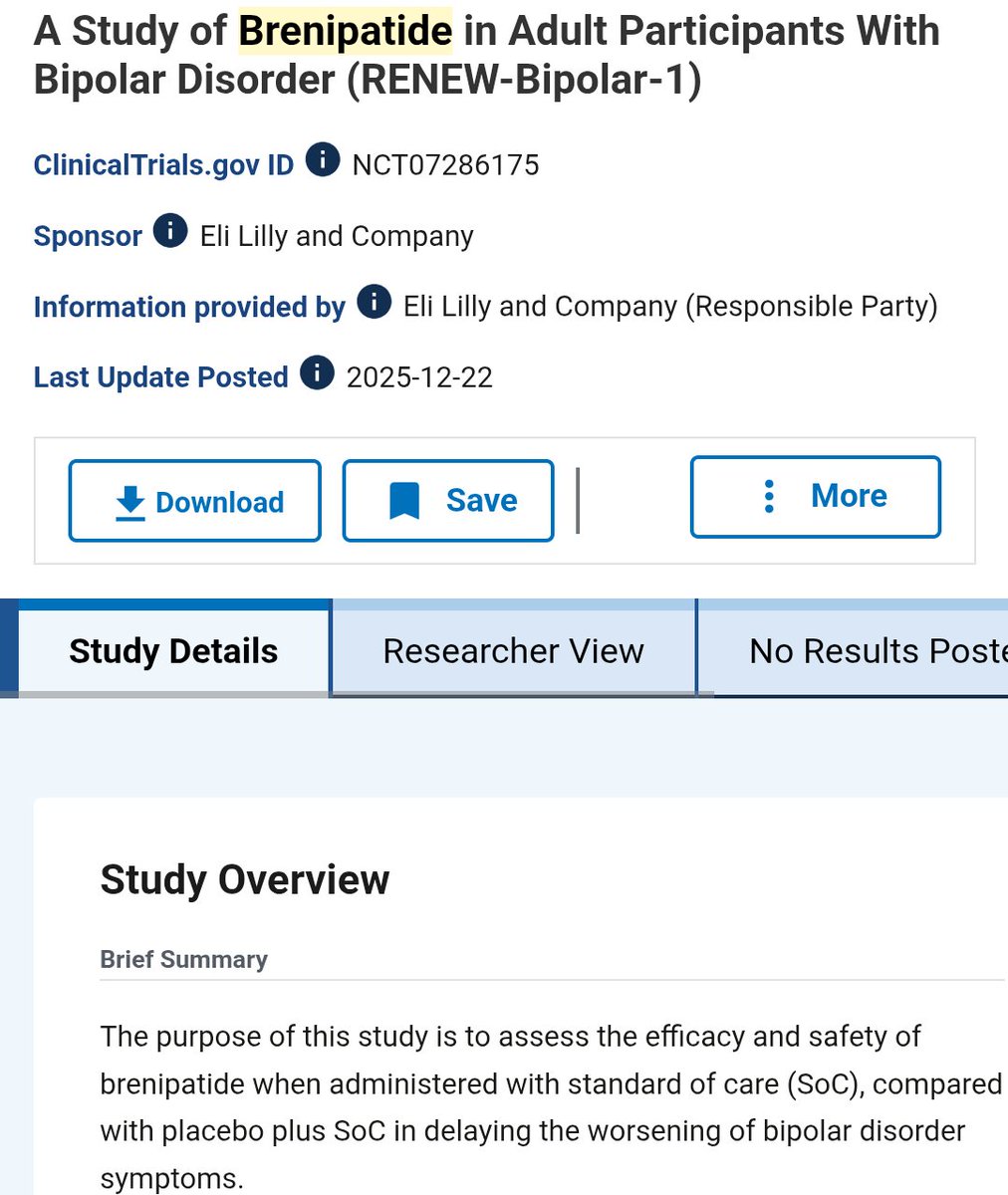
While everyone else plays checkers chasing weight loss indications , Eli Lilly is out here chasing every potential indication. Brenipatide is a dual GIP/GLP1 med, now being tested for bipolar disorder, severe asthma, alcohol use disorder and smoking cessation.
5
1
22
3,347
FlexNP retweeted

16 Dec 2025
1/
It's almost impossible to convince ideological medical conservatives to change their minds. They will always find some reason to discount a RCT result that goes against their **beliefs**.
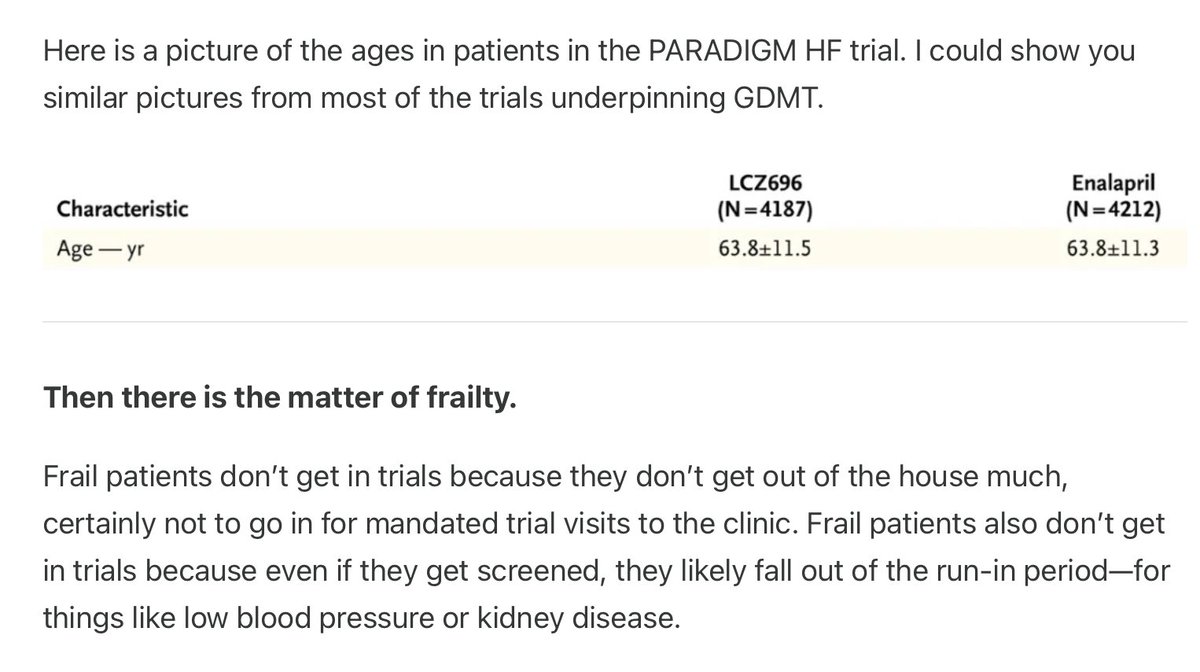
Main criticism here is that these HF RCT trials only enrolled patients who are relatively younger (<70) and not frail.
Therefore, @Drjohnm argues that these benefits don't translate to older more frail patients.
There is no MECHANISTIC argument on why a drug's pharmacology changes once a patient reaches 70 or so.

Heart Failure in Trials vs Heart Failure in the Average Hospital/Clinic: @drjohnm was misunderstood on the Internet. Here is his explanation: it has to do with the (minimally disruptive) treatment of patients with heart failure
open.substack.com/pub/sensib…
Prof @RichardLehman1 said this donkey's yrs ago.
5
3
22
11,345
20-23% weight loss? Did they even look at the phase 2 data for retatrutide?
🤦🤦
Unless this trial is 70% men it's gonna be more like 25-28% weight loss despite being only 68 weeks long
4 Dec 2025

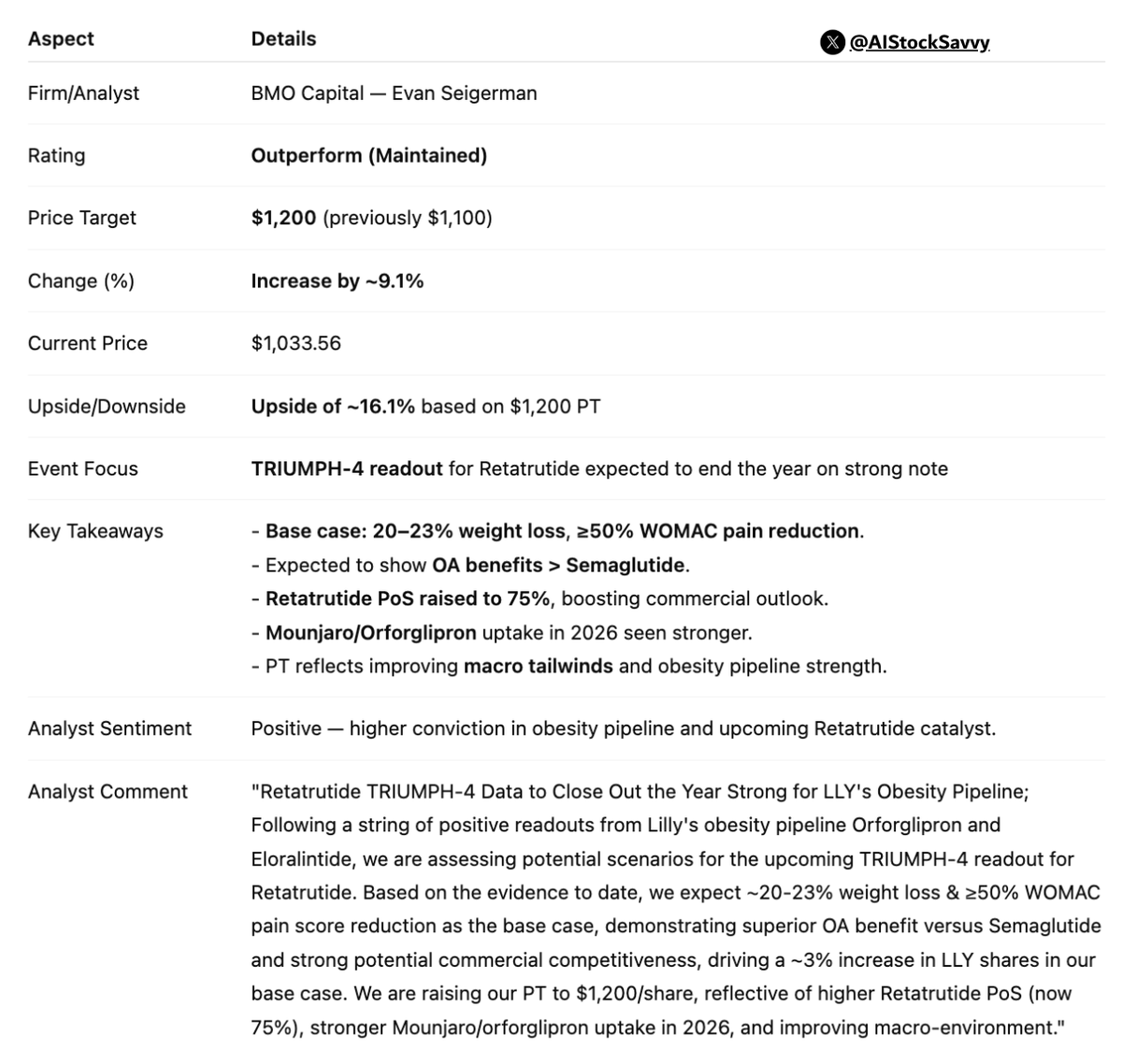
$LLY | 𝐄𝐥𝐢 𝐋𝐢𝐥𝐥𝐲: BMO Capital reiterates Outperform, raises 𝐏𝐓 𝐭𝐨 $𝟏,𝟐𝟎𝟎
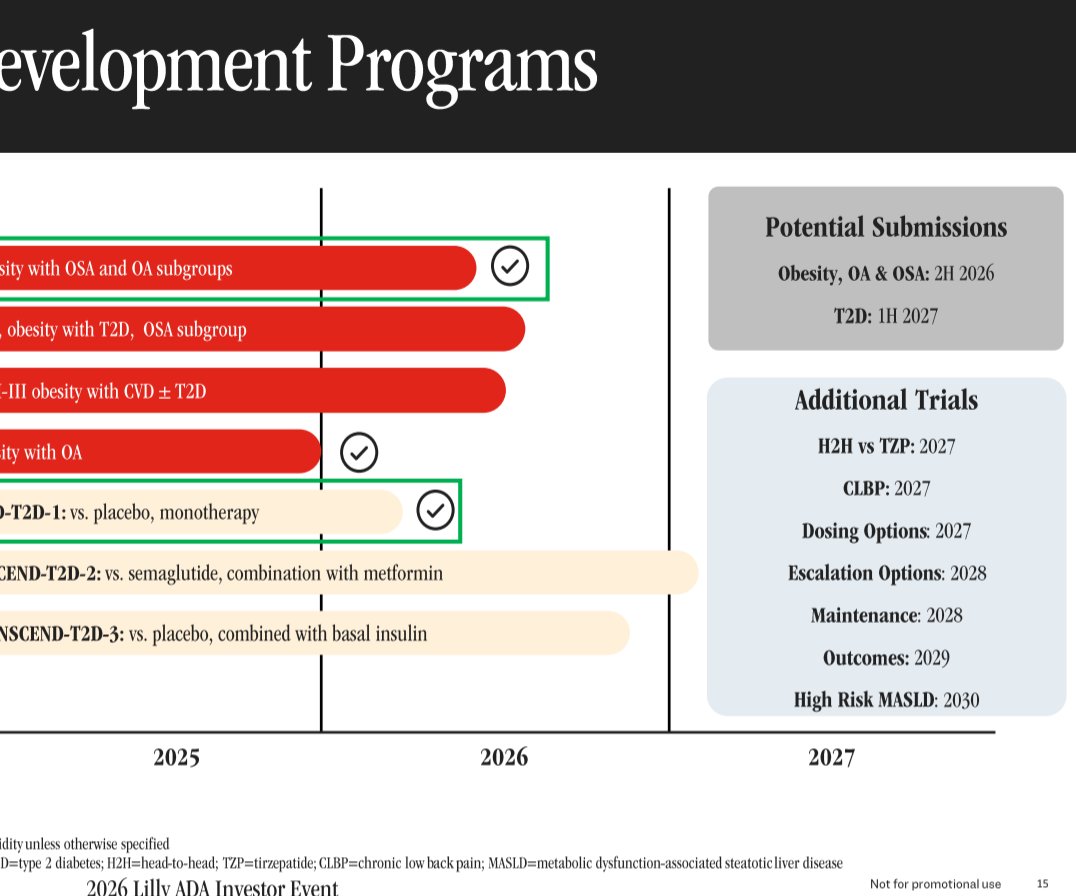
Analyst sees strong close to year with TRIUMPH-4 data; boosts PT on higher Retatrutide confidence and obesity franchise momentum.
4
1
7
1,960
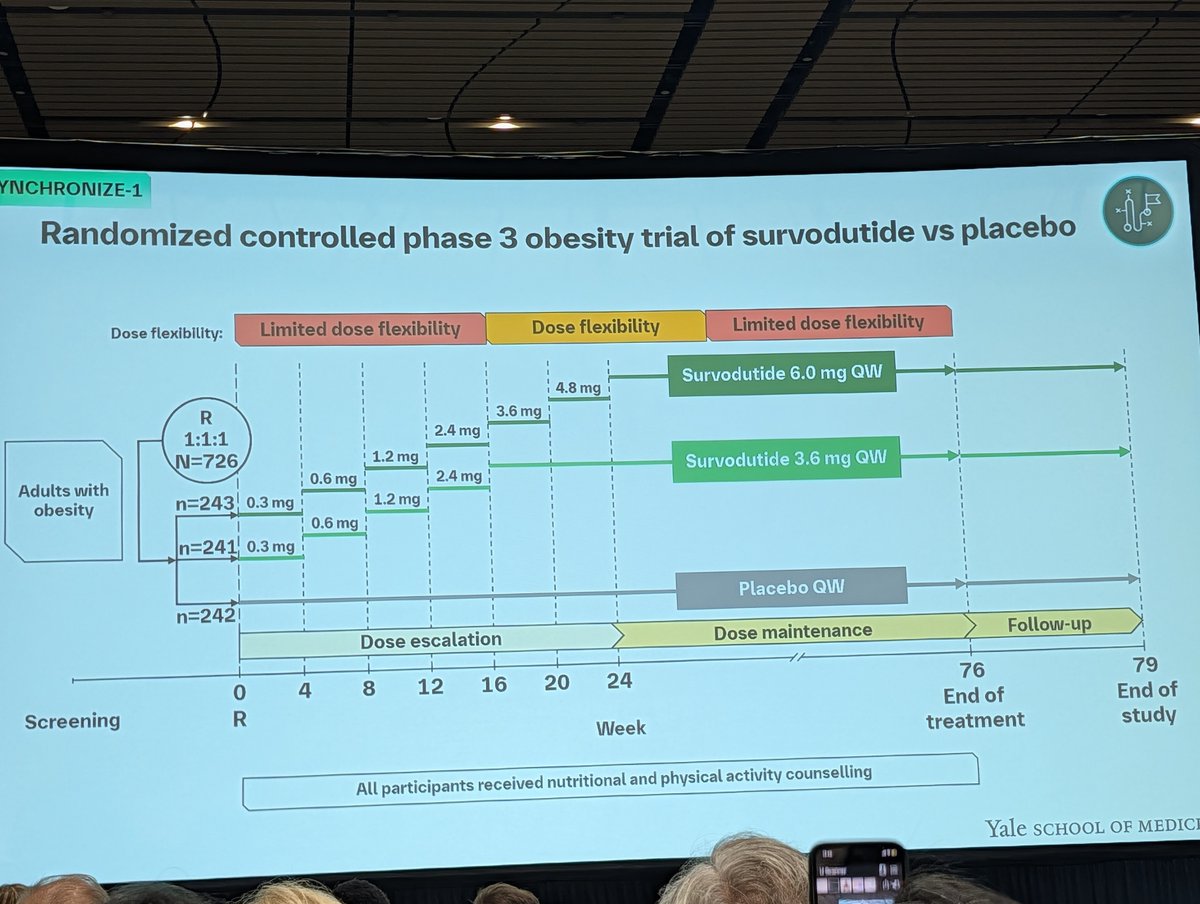
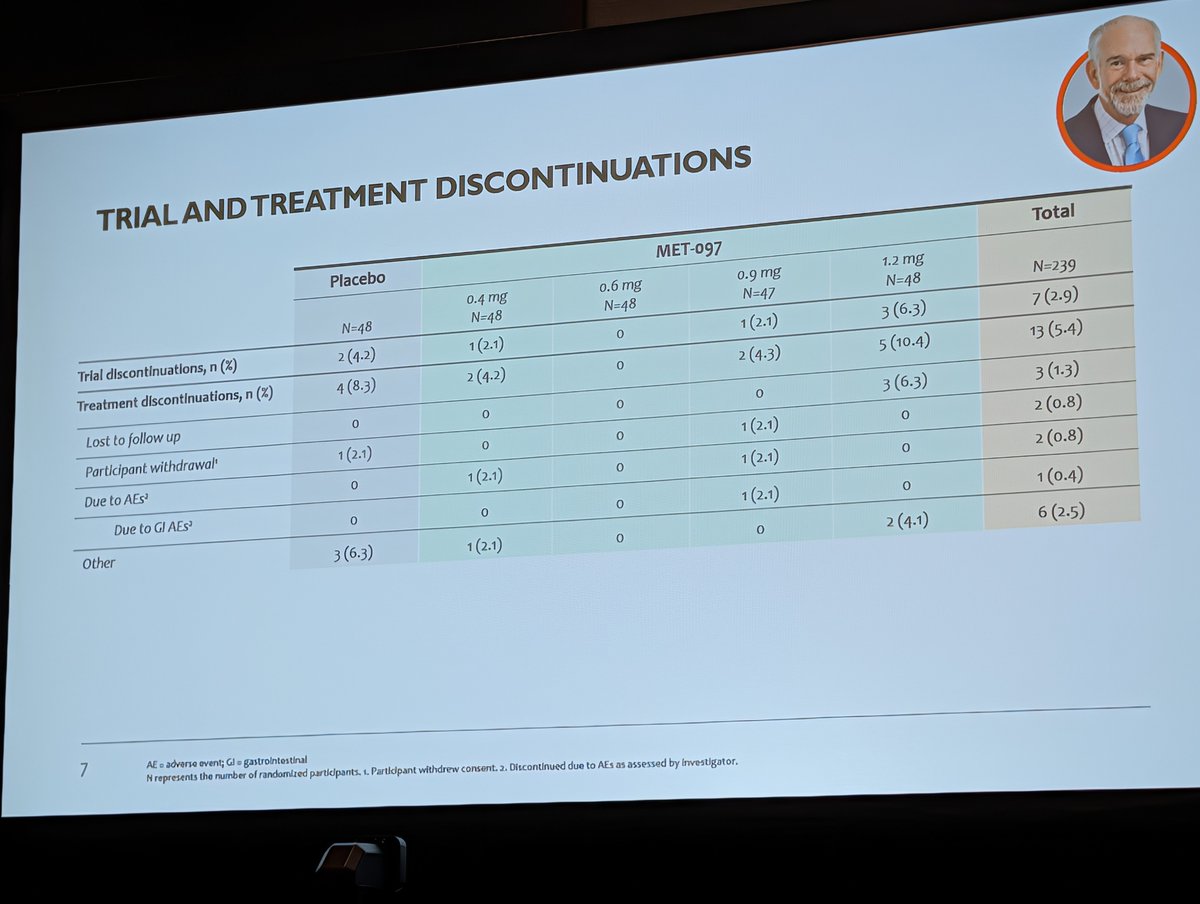
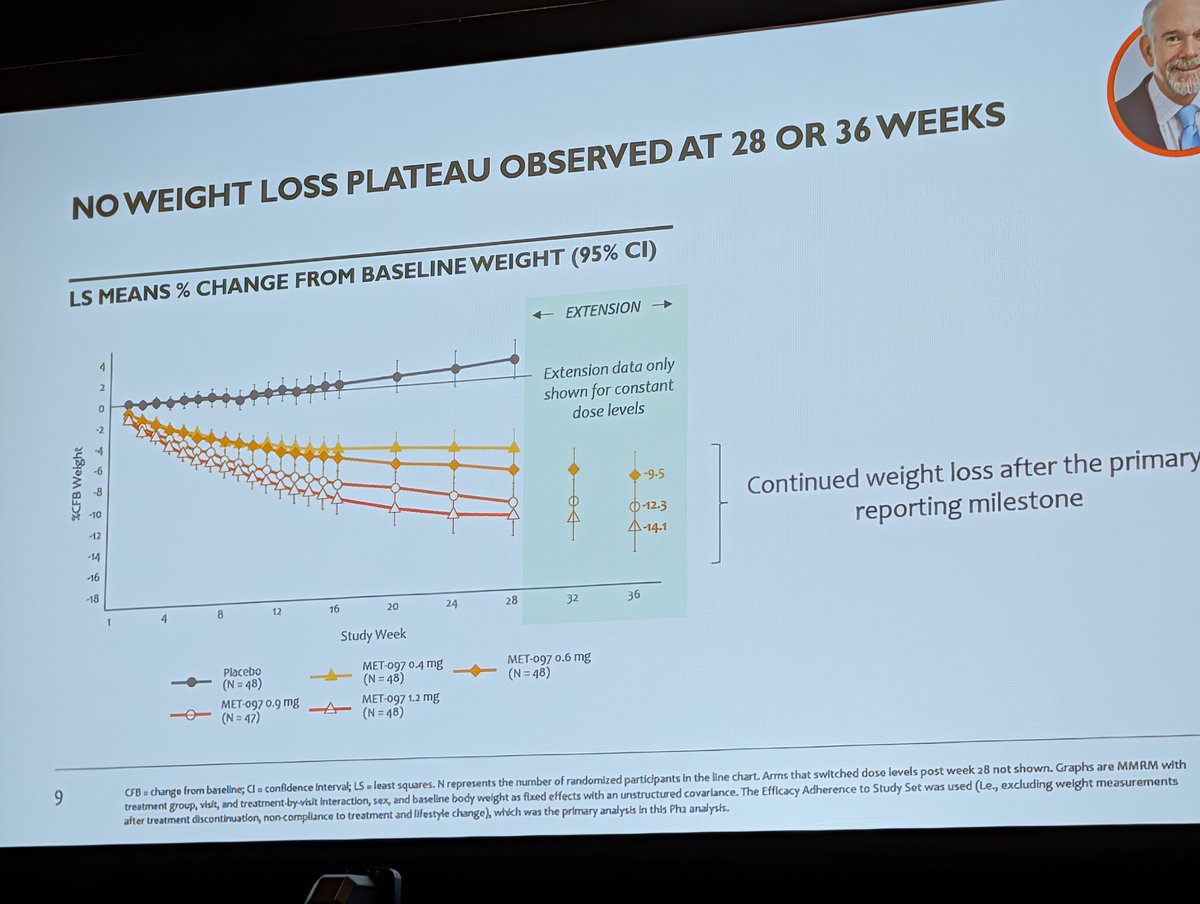
So yeah this was a very hard sell to the Pfizer and Novo reps in the audience. Weight loss is alright/middle of road for mono agonist. Higher rate of N/V that got better with titration. No talk of PK or PD
6 Nov 2025

4
1
19
32,594
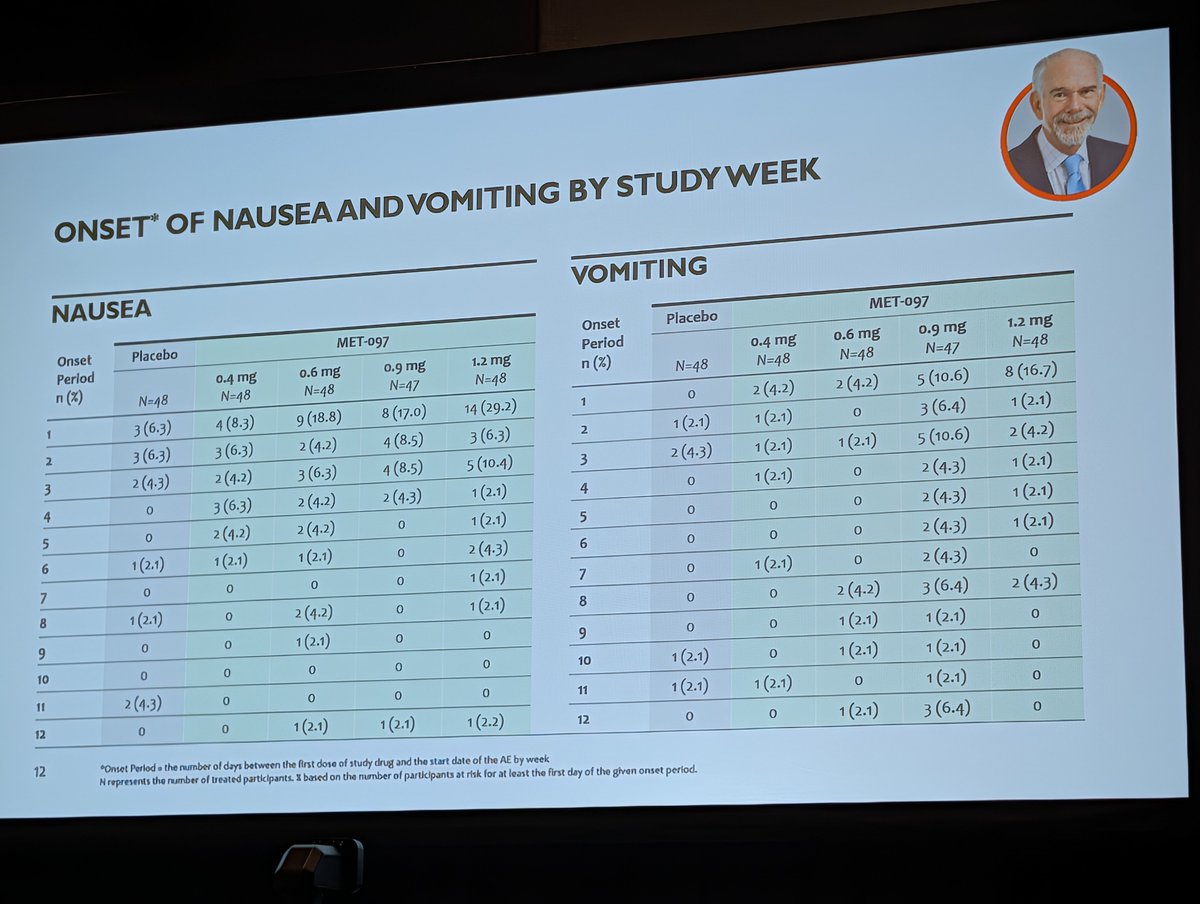
When they titrated, tolerability got a lot better to no surprise? My hot take? Add it to the pile of peptides Perhaps their Amylin and/or dual agonists show more potential, but given Eloralintide results today this is another drug that works but not majorly better


1
7
1,436