
Internista - Intensivista, Magister Gerencia Hospitalaria y Salud Pública 🇪🇨🇦🇷🇺🇾🇮🇹
Joined March 2012
- Tweets 9,633
- Following 743
- Followers 4,799
- Likes 6,921
1,406 Photos and videos






Pinned Tweet

28 Mar 2020
Mi papi. Nino Antonio Cassanello Layana. Mi ídolo, mi vida, mi todo. El era la medicina. Por el soy médico. El arte de la semiología médica. Internista. Sin temor a nada, ni nadie. Sembró en todos aquellos que lo rodearon. Hoy recibo esos afectos.

237
373
3,515
Jerónimo Xavier Cassanello retweeted

22h
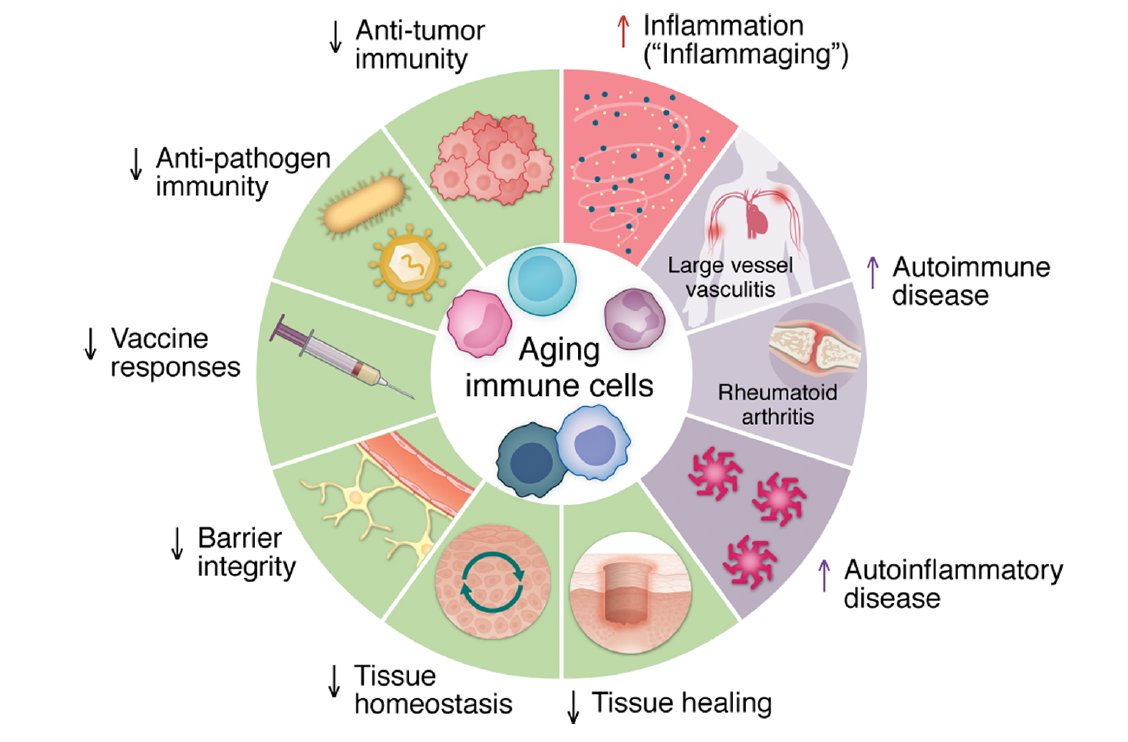
Our immune response loses its integrity and protection as we age. If we're going to promote healthspan, we'll need to counter that loss of function and, at the same time, avoid inducing autoimmune diseases
A new @jclinicalinvest review, open-access jci.org/articles/view/206227
16
124
461
27,537
Ha llegado a mis manos después de varias semanas. La vida de Eugene Braunwald.
1
2
97
Jerónimo Xavier Cassanello retweeted

Jun 13
1929: Alexander Fleming calmly discovers penicillin

5
11
82
5,479
Jerónimo Xavier Cassanello retweeted

Jun 11
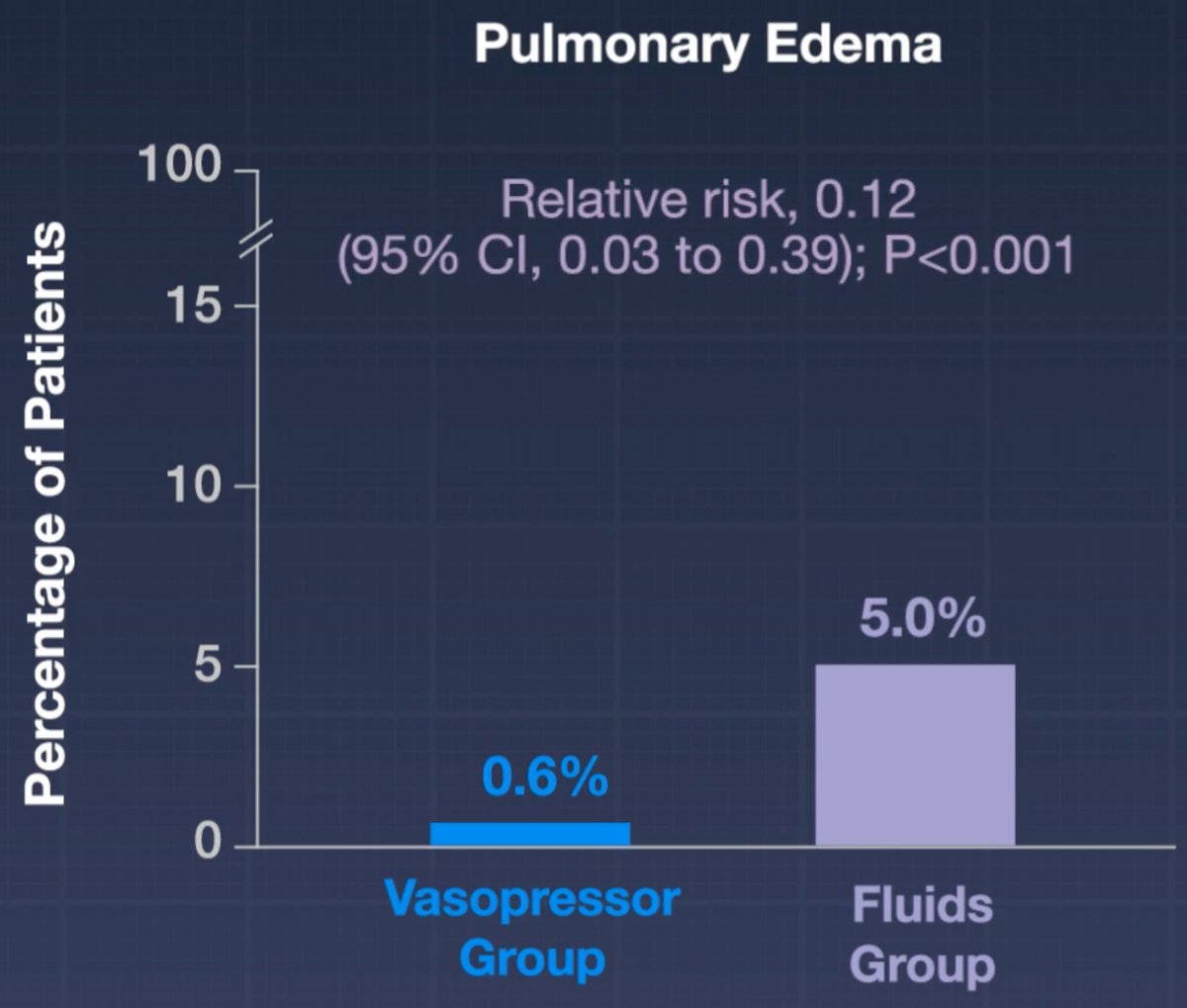
ARISE-FLUIDS has arrived and it's awesome 🥳
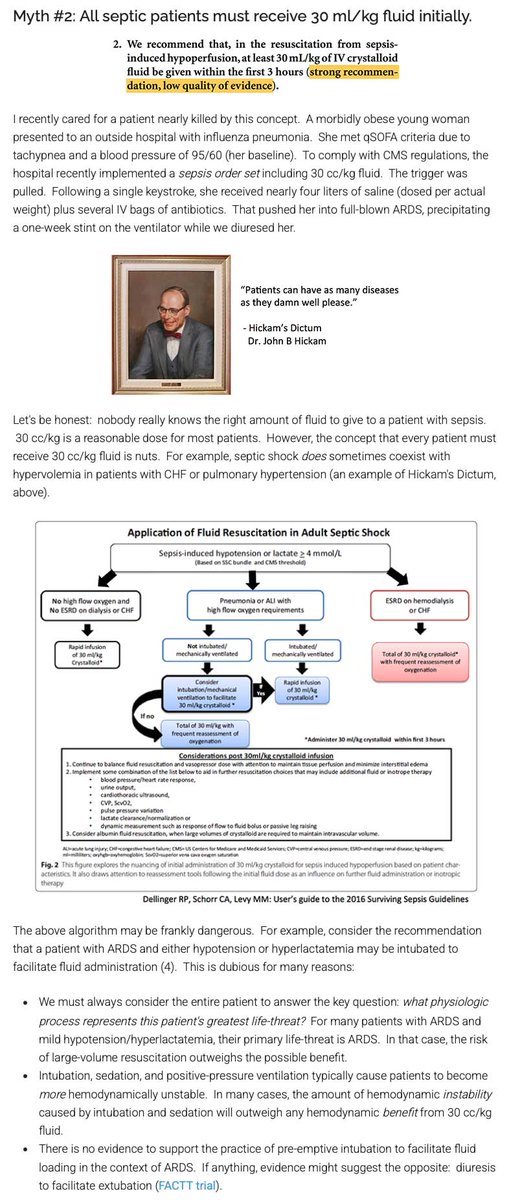
For over a decade, the Surviving Sepsis Guidelines recommended that septic patients get at least 30 cc/kg fluid. In the United States, these guidelines were weaponized into performance metrics, pressuring clinicians to prescribe arbitrary volumes to every patient.
Evidence-based clinicians have LONG known that this guideline lacked evidentiary support. For example, I've attached a picture of a blog I wrote about this back in 2017. Despite the lack of evidentiary support and some evidence of harm, the Surviving Sepsis Guidelines INSISTED on perpetually recommending 30 cc/kg fluid resuscitation.
We finally have a prospective RCT demonstrating that mandating early administration of 30 cc/kg fluid (as compared to early vasopressors) doesn't help and may actually cause harm.
It's important to note that all of the hard endpoints in this trial were neutral (e.g., mortality, days free of organ support).
I still think that 30 cc/kg fluid is a pretty reasonable volume of fluid for *most* patients. But the study does suggest that giving too much fluid may promote edema - so we should be *thoughtful* about this intervention rather than mandating it for every septic patient.
Based on the subgroup analysis, the fluid-conservative strategy may have helped the subgroup of pneumonia patients the most. This is statistically nonsignificant but aligns with my expectation. ARDSy patients often don't respond well to fluid. (In contrast, I really doubt that a liter of fluids in either direction matters for most urosepsis patients.)
This is a great example of the over-reach of guidelines and protocoled medicine. People get all upset about practice variation, so sometimes they try to stomp it out using guidelines and protocols. But these guidelines are highly fallible, so what may occur is that you standardize care in a way that harms everyone equally. 🤦♂️


17
146
465
59,193
Jerónimo Xavier Cassanello retweeted

Hoy en Sr. Miércoles, les presento: “Entre Pokémon y fondos de pensiones”
1
10
15
397
Jerónimo Xavier Cassanello retweeted

En el 1er día de actividades del festival "Historias de Hermandad" organizado por la Universidad UTE con el apoyo de la Embajada de Italia y la CBEI como homenaje a los 80 años de la República Italiana 🇮🇹 se realizó el concierto de la Orquesta Coral Italia: dal Opera alla Canzone
Espectacular montaje de los alumnos de la universidad
@UTEoficial @ItalyinEcuador @guidoflavio @aramondi2 @CeEcuatoriano @FECABE_Ecuador @JCCassinelli @Gabrielacartage @sebascampana



1
4
115
Jerónimo Xavier Cassanello retweeted

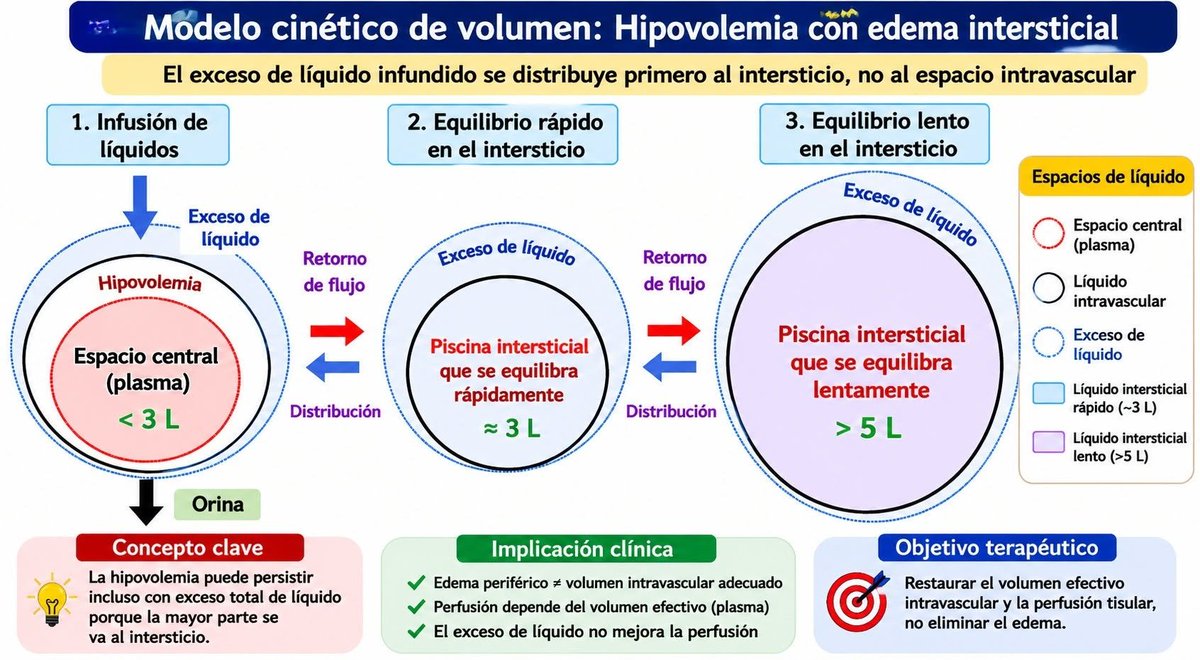
🔰Hipovolemia con edema periférico: ¿qué está fallando?❓️❓️
☝🏻🤓Comprendiendo la paradoja hemodinámica entre la congestión y la hipoperfusión🔎
🚿💧La coexistencia de hipovolemia intravascular y edema5 periférico representa una de las paradojas fisiopatológicas más frecuentes y mal interpretadas en terapia intensiva. Tradicionalmente, la presencia de edema se ha asociado con sobrecarga de volumen; sin embargo, numerosos pacientes presentan edema☝🏻🤓 generalizado mientras mantienen una reducción crítica del volumen circulante efectivo, comprometiendo la perfusión tisular y la entrega de oxígeno.🔎
🎯El concepto central radica en diferenciar el volumen total corporal del volumen intravascular efectivo. El edema refleja expansión del compartimento intersticial, mientras que la perfusión depende del volumen sanguíneo funcional dentro del sistema vascular.
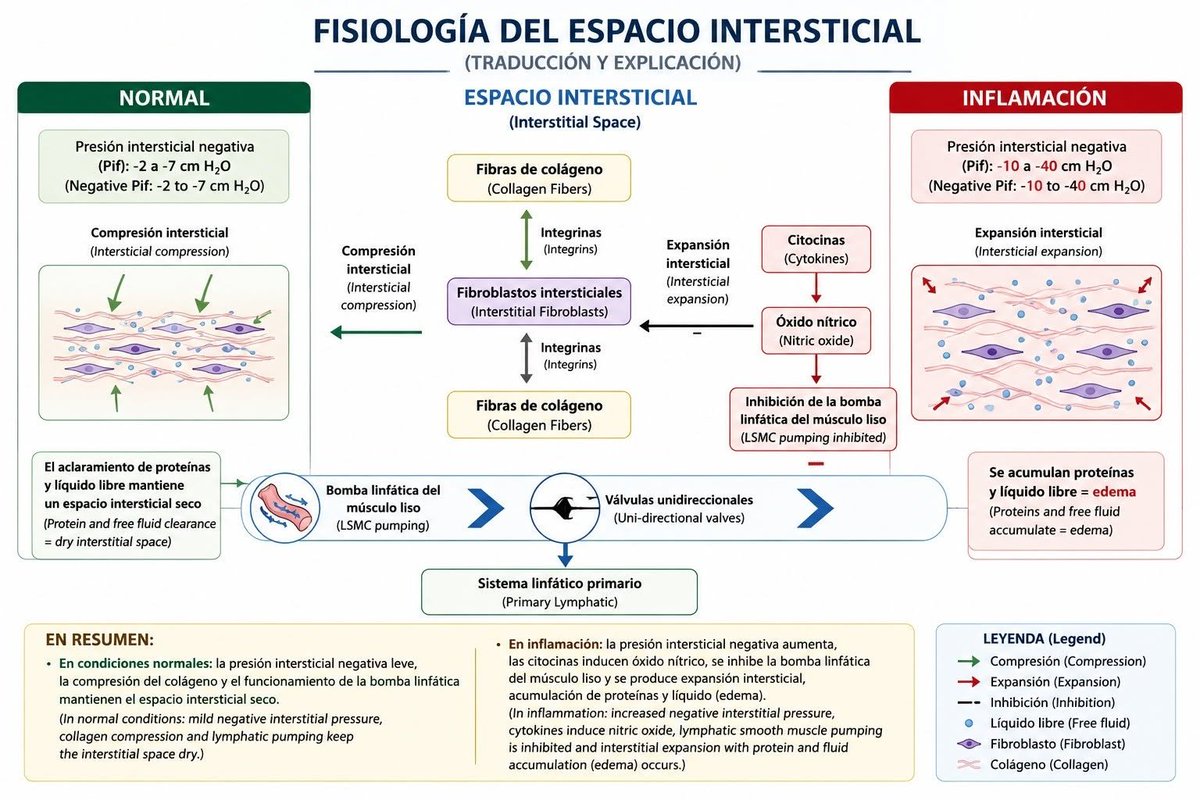
🔰Fisiopatología: ¿por qué puede existir edema con hipovolemia?
1️⃣. Alteración de las fuerzas de Starling y del glicocálix endotelial
La visión moderna reconoce que el glicocálix endotelial regula el intercambio de fluidos mucho más que las fuerzas clásicas de Starling.
Cuando ocurre:Sepsis,Trauma, Quemaduras, Cirugía mayor,Inflamación sistémica.
➡️se produce lesión del glicocálix, aumentando la permeabilidad capilar y permitiendo la fuga de líquidos hacia el intersticio.
📚Resultado:
▪️↓ Volumen intravascular efectivo
▪️↑ Edema tisular
▪️↓ Retorno venoso efectivo
▪️↓ Perfusión microcirculatoria
2️⃣. Hipoalbuminemia
➡️La disminución de la presión oncótica favorece la salida de líquido desde el espacio vascular hacia el intersticial.
💧Frecuente en:Cirrosis,Síndrome nefrótico,Sepsis,Desnutrición,Pacientes críticos crónicos.
🔎Hallazgos:-Edema masivo,-Ascitis
-Derrames pleurales,pero simultáneamente: ■Hipotensión
■Disminución de la precarga efectiva
■Hipoperfusión renal
3️⃣ Congestión venosa con bajo volumen arterial efectivo.
Principalmente en insuficiencia cardiaca avanzada y cirrosis:
💧El volumen total corporal está aumentado, pero la circulación arterial percibe hipovolemia.
📚Se activan:Sistema renina-angiotensina-aldosterona,Sistema simpático, Vasopresina
☝🏻🤓Lo que genera:▪️Retención de sodio y agua,▪️Más edema, ▪️Mayor congestión sin corregir la perfusión sistémica.
4️⃣Hipertensión venosa y disfunción linfática.
💧El edema también puede desarrollarse por:▪️Congestión venosa sistémica, ■Elevación de PVC
■Insuficiencia ventricular derecha■ Hipertensión intraabdominal.
☝🏻🤓La presión venosa elevada reduce el gradiente de perfusión capilar y favorece la acumulación de líquido intersticial.🚿
📚Implicaciones hemodinámicas
🚿El edema periférico no predice respuesta a los LÍQUIDOS 💧💧
🔰Muchos pacientes edematizados presentan:▪️Vena cava inferior colapsable▪️Bajo volumen sistólico
▪️Bajo gasto cardíaco,▪️Hipoperfusión periférica
☝🏻🤓Por ello, la exploración clínica aislada tiene baja precisión para definir el estado de volumen.
☝🏻🤓 Siempre!! Valorar la
Microcirculación‼️: ▪️Tiempo de ▪️llenado capilar, ▪️Mottling score
▪️Temperatura periférica
▪️Lactato,▪️ΔPCO₂ venoso-arterial
☝🏻🤓La presencia de edema no excluye hipoperfusión.
🔺️Rol del ultrasonido en esta paradoja.
🔺️Ecografía pulmonar.
▪️Puede mostrar:Líneas B. ▪️Congestión pulmonar
☢️Mientras el paciente mantiene:
▪️Hipotensión
▪️Bajo volumen sistólico
▪️VExUS permite identificar congestión venosa sistémica y diferenciar:🚿Sobrecarga venosa verdadera, Hipoperfusión por bajo gasto,Congestión asociada a lesión renal.
🫀Ecocardiografía crítica.
Es fundamental para determinar:
▪️Función ventricular izquierda
▪️Función ventricular derecha
▪️Acoplamiento ventrículo-arterial
▪️Estado real de precarga
🎯El objetivo no es tratar el edema, sino restaurar la perfusión efectiva.
Dependiendo del mecanismo:
▪️Fuga capilar
▪️Reanimación guiada por objetivos
🚿Evitar sobrecarga hídrica
➡️Uso racional de albúmina en casos seleccionados: 💧Congestión venosa
👇🏽👇🏽👇🏽

1
74
153
5,664
Jerónimo Xavier Cassanello retweeted

Jun 7
The core of the discussion about physicians today is less about money and more about the loss of autonomy. Laws have shifted the balance of control of medicine toward insurers, administrators, and government, and completely away from doctors. Physician “Burn Out” occurs from a loss of control and all the new demands that must be met while lacking the ability to protest or change. The doctor no longer has control or leverage and that is first frustrating and ultimately infuriating.
13
9
55
7,160
Jerónimo Xavier Cassanello retweeted

Lo trágico del tiempo no es tanto como afecta tus recuerdos, sino lo lejos que te lleva de ellos.
1
1
90
Jerónimo Xavier Cassanello retweeted

28 Jul 2022
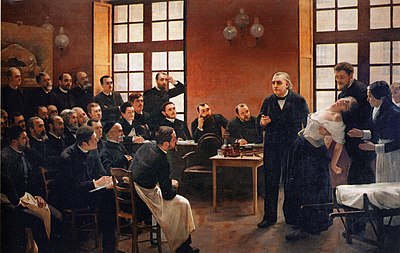
Let's talk about Jean-Martin Charcot, the "Father of Neurology"! He casts a shadow too wide to cover in one #tweetorial. First, let's talk about his training and legacy as a teacher (and stay tuned for more about him later).
#neurotwitter #neurology #medicalhistory
1/10

9
76
242
Jerónimo Xavier Cassanello retweeted
28 Jul 2022
Which brings me to this amazing painting, A Clinical Lesson at the Salpêtrière, depicting Wittman, Babinski (holding her), and many other famous neurologists including Marie, Tourette, Parinaud, and Vigouroux.
9/10
1
4
39
Jerónimo Xavier Cassanello retweeted
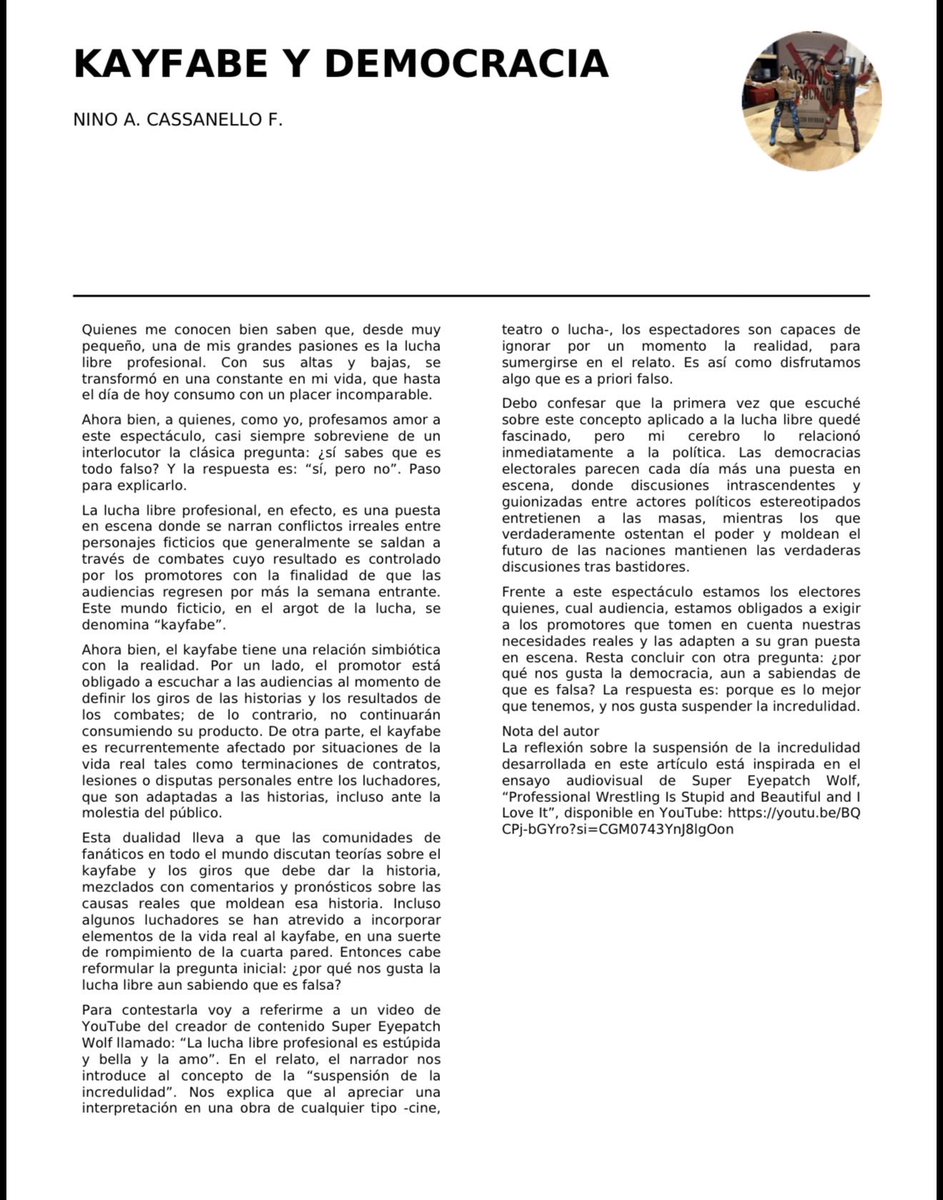
Hoy en Señor Miércoles les presento: “Kayfabe y democracia”. Una aproximación a la política desde la lucha libre:
11
14
497
Jerónimo Xavier Cassanello retweeted

Vas por la perimetral y ahí estoy.
Que podamos disfrutar de este bosque a futuro, depende de todos los Guayaquileños.
Defendamos a Cerro Azul
5
204
314
4,956
Jerónimo Xavier Cassanello retweeted

May 31
🇬🇧 | El King's College Hospital en Londres ha inaugurado un jardín en la azotea para pacientes de cuidados críticos. Su primera paciente dijo que el espacio al aire libre le dio «un verdadero impulso para seguir adelante».
28
769
15,086
888,721
Jerónimo Xavier Cassanello retweeted

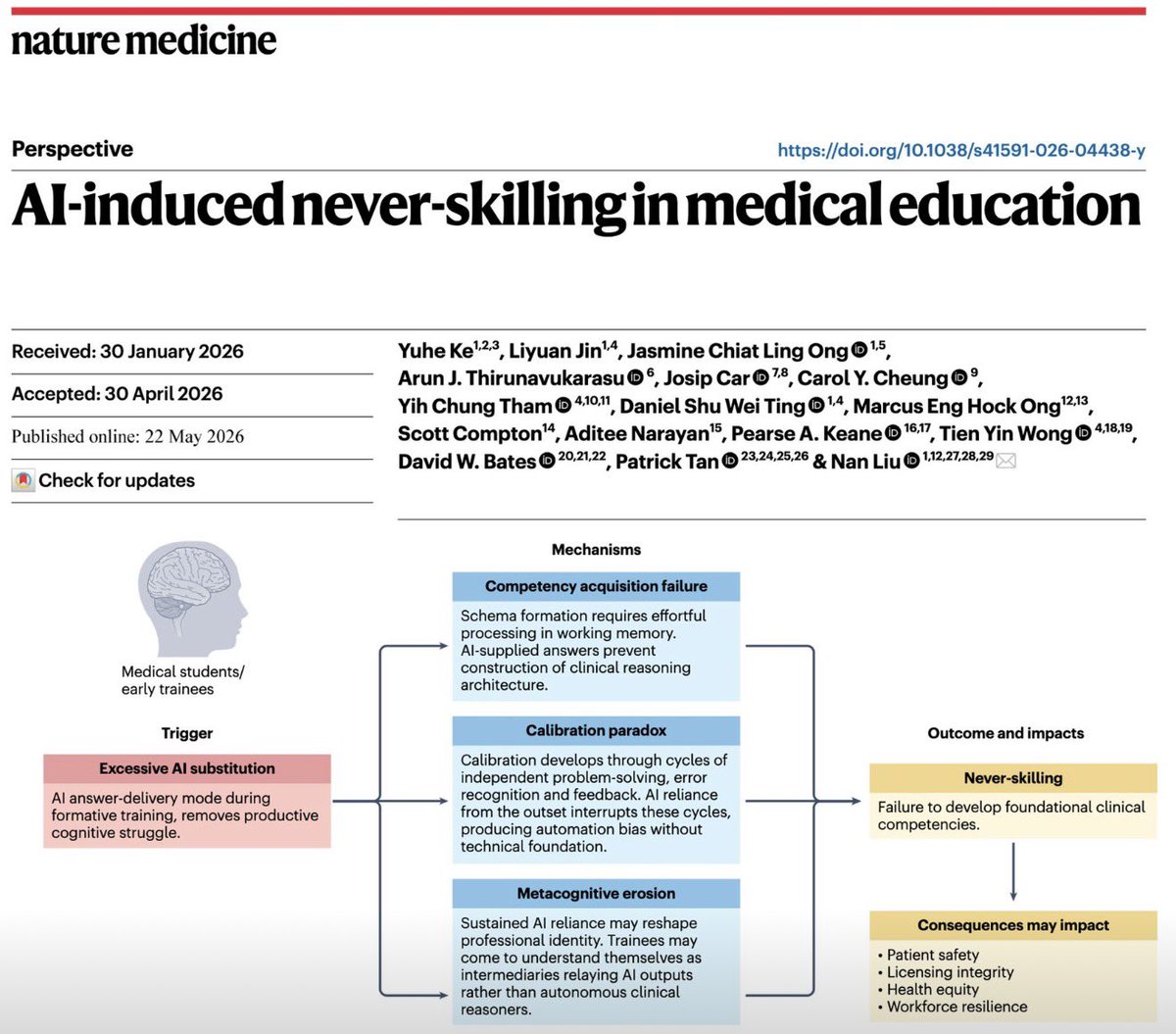
AI in medicine warning! The never skilling effect in medical education! @TomVargheseJr @pferrada1 @SWexner @AmCollSurgeons
15
117
410
62,769
Jerónimo Xavier Cassanello retweeted

May 24
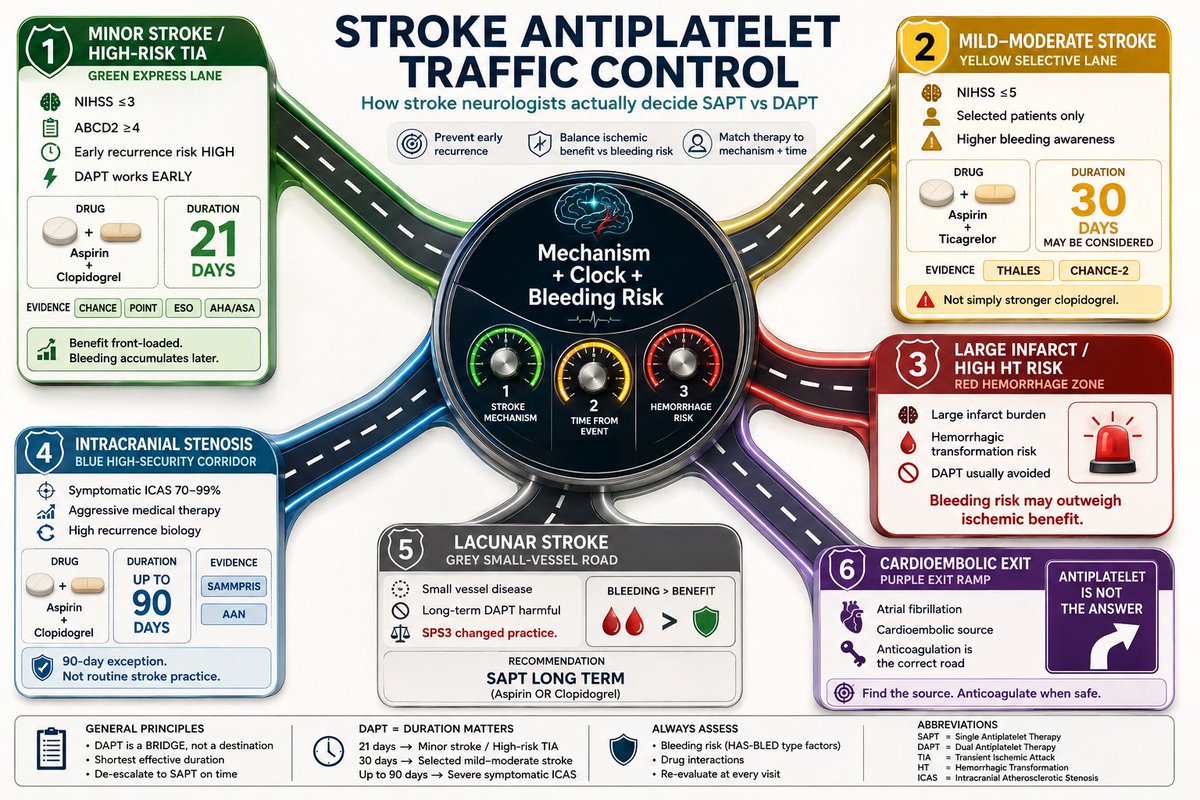
Antiplatelet therapy after stroke is not:
Aspirin for everyone.
DAPT for everyone.
Or clopidogrel because the patient had a stroke on aspirin.
It is a 3-question decision.
What is the mechanism?
What is the clock?
What is the bleeding risk?
That is the whole game.
Minor non-cardioembolic stroke or high-risk TIA, early presentation, low bleeding risk?
Think short DAPT.
Aspirin plus clopidogrel.
Usually 21 days.
Then single antiplatelet.
Not 3 months by habit.
Not lifelong because the first prescription was never reviewed.
Mild to moderate stroke or high-risk TIA with selected high-risk features?
Ticagrelor plus aspirin may enter the discussion.
But it is not simply stronger clopidogrel.
It is a selected-patient decision, with bleeding and dyspnoea on the other side of the scale.
Severe symptomatic intracranial stenosis?
This is the 90-day exception.
Aspirin plus clopidogrel may be justified, but only as part of aggressive medical therapy:
statin, BP, diabetes, smoking, lifestyle.
DAPT alone is not a treatment plan.
Lacunar stroke?
Respect SPS3.
Long-term aspirin plus clopidogrel is not wisdom.
It is bleeding dressed as prevention.
ESUS?
Do not guess with anticoagulation.
Start antiplatelet, investigate properly, and reclassify the mechanism when evidence appears.
AF-related stroke?
Antiplatelet therapy is not enough.
The patient needs an anticoagulation strategy when safe.
Stroke on aspirin?
First ask:
Was it really aspirin failure?
Or was it:
missed AF,
intracranial stenosis,
carotid plaque,
non-adherence,
wrong dose,
cancer-associated stroke,
or uncontrolled risk factors?
Never escalate before you re-diagnose.
The clean bedside rule:
DAPT is a bridge.
SAPT is the destination.
Anticoagulation is a different road.
Mechanism decides the map.
In stroke prevention, the most dangerous antiplatelet error is not choosing the wrong tablet.
It is forgetting to write the stop date.
#Neurotwitter #MedX #Stroke #Aspirin
6
142
427
17,786
Jerónimo Xavier Cassanello retweeted

What are the differences between an animal ICU and human one?
8
4
59
10,225