
Interventional Cardiologist @lenoxhill / @ZuckerSoM🫀| Interests #CHIP #PERT #CardiacCriticalCare | Previously @nymedcollege @PennMedicine | tweets are my own |
Joined March 2017
- Tweets 1,916
- Following 598
- Followers 1,394
- Likes 7,633
192 Photos and videos










Pinned Tweet

27 Aug 2025
Excited to share our paper, now out in @JACCJournals! Important work led by @MAlvarezVillela:
🔥 Fever in AMI-CS is common and is associated with greater illness severity but seems to be noninfectious in most cases
#CardiogenicShock 🫀
doi.org/10.1016/j.jacadv.202…
3
7
33
6,707
May 3
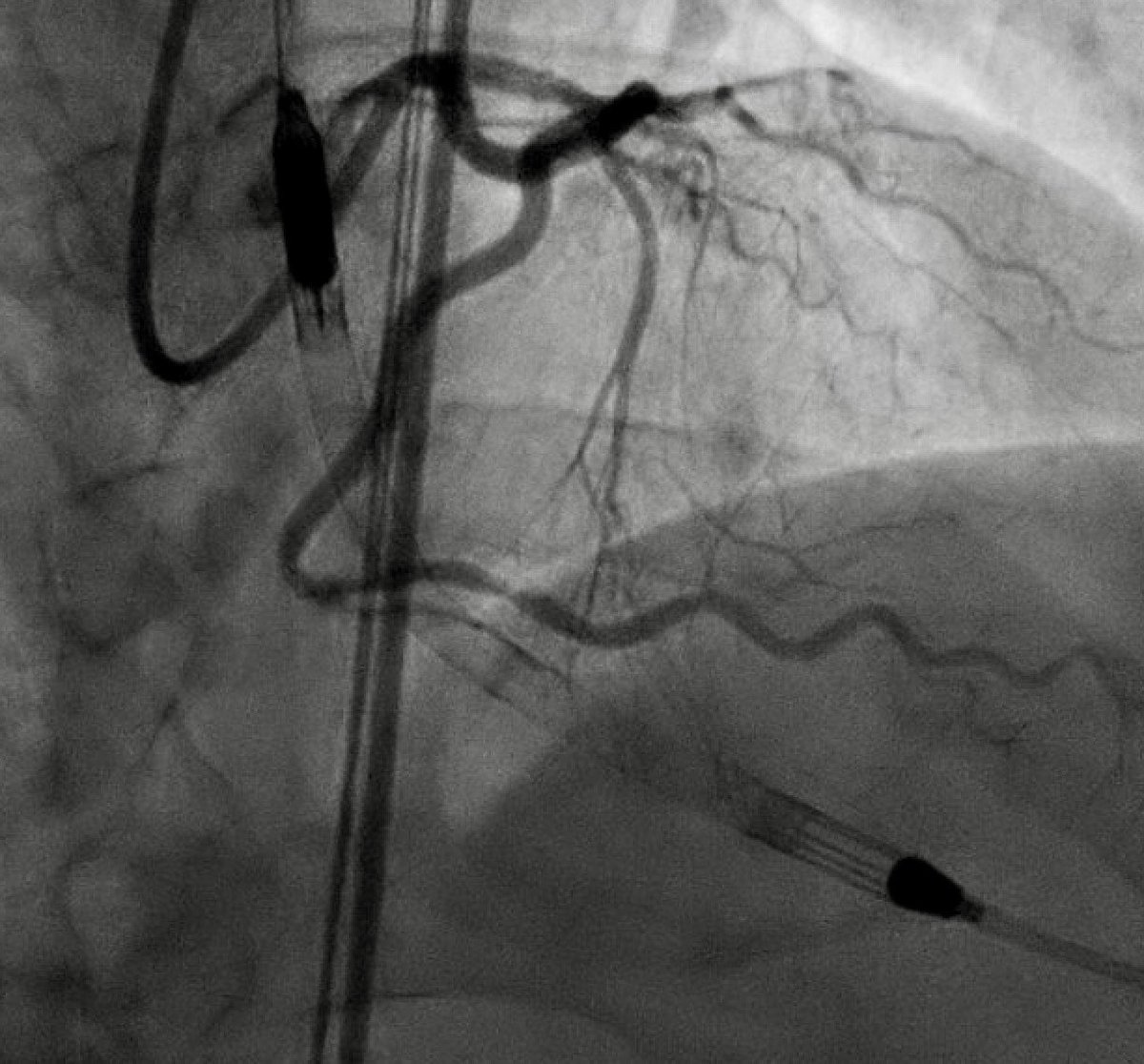
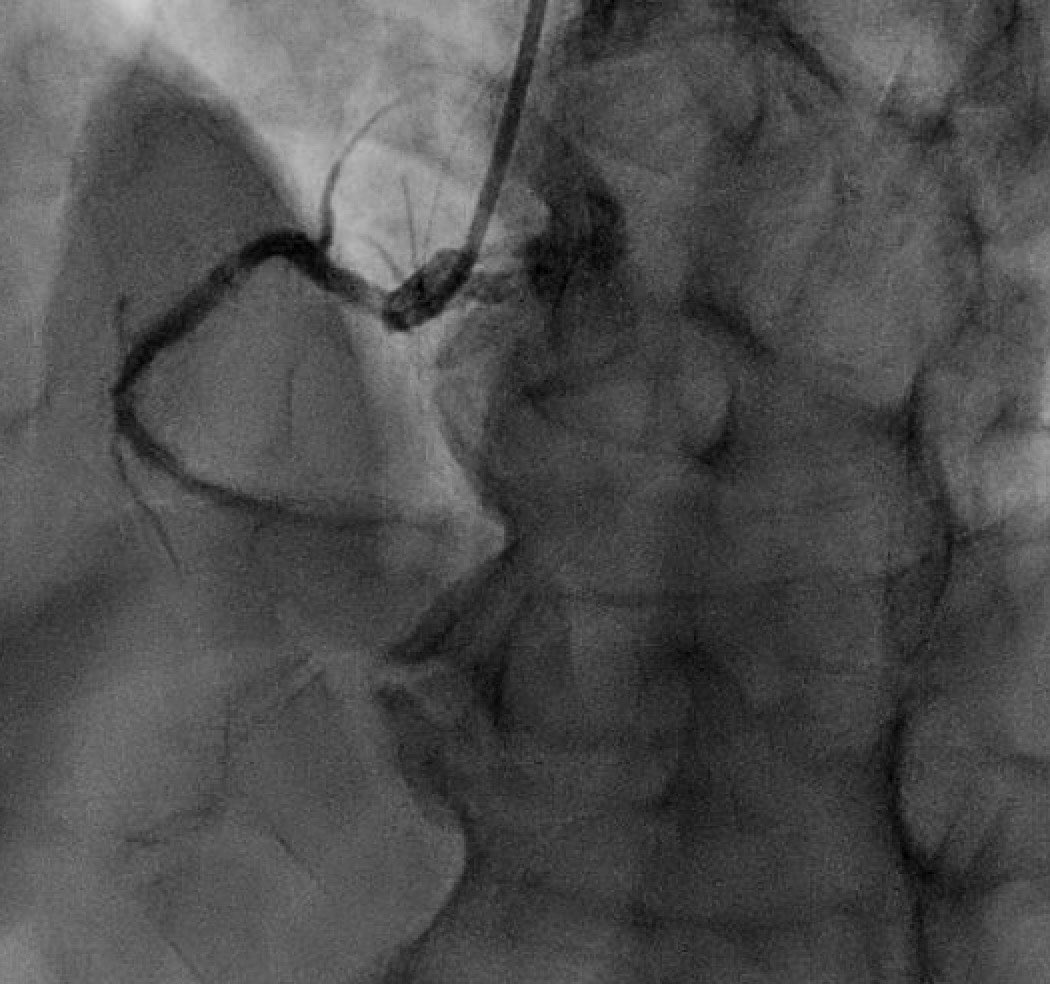
Very interesting from @GreggWStone
Makes sense intuitively - more ischemic time on an already stunned myocardium, elevating EDP, contrast delivery etc...
Non-shock doesn't necessarily mean patient is "stable".

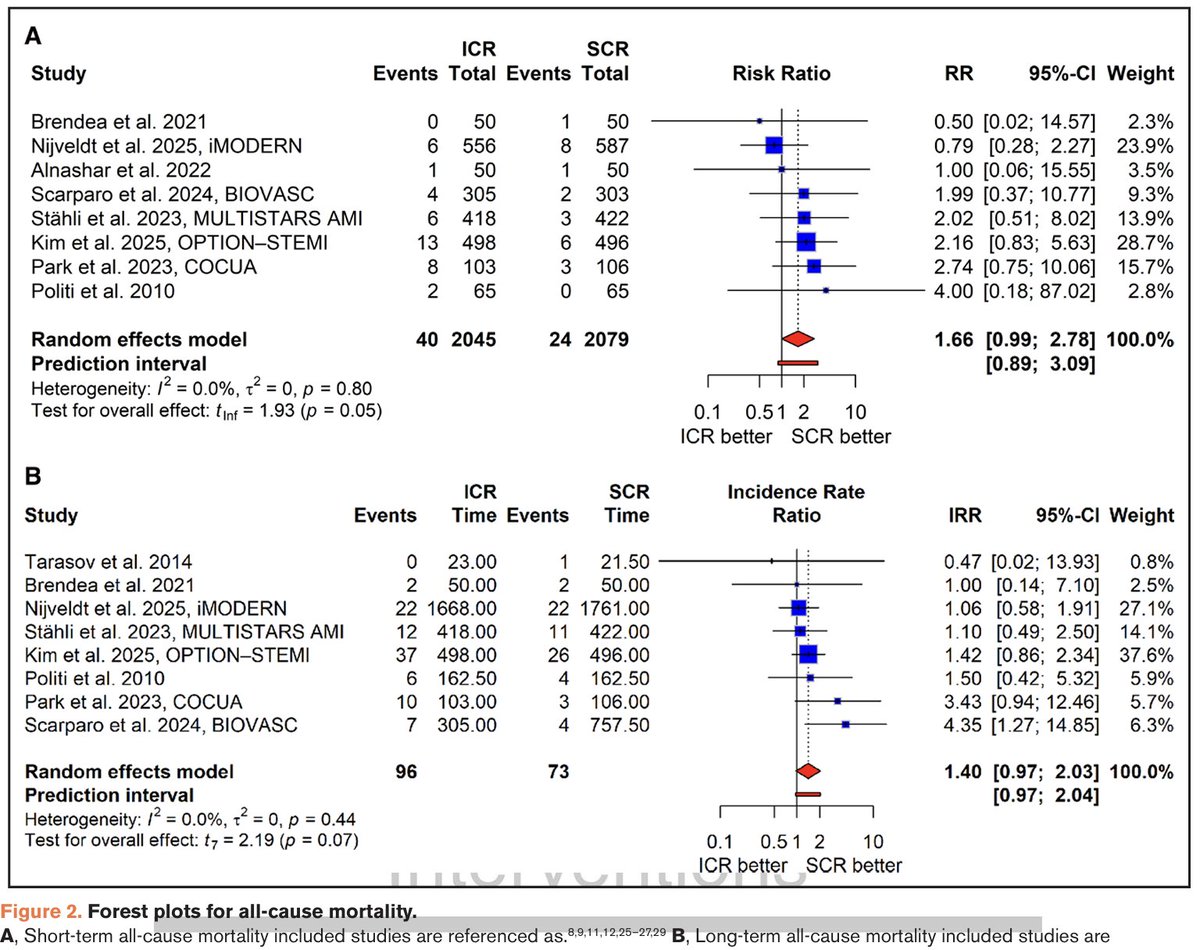
Complete revasc (CR) in pts with non-shock STEMI and multivessel ds. reduces MACE. But is the best timing for non-culprit lsn PCI immediate (during primary PCI) or staged? Our new meta-analysis publ in Circ CV Interv suggests immediate CR may increase mortality, same as in shock.
4
366
Atul D. Bali, MD retweeted

Mar 13
Key updates to this guideline include:
➡️ The use of the American Heart Association PREVENT-ASCVD equations to guide primary-prevention and lipid-lowering therapy decisions.
➡️ Testing Lp(a) at least once in a lifetime and selective apolipoprotein B measurement to improve risk assessment and guide treatment
➡️ The return of LDL-C and non-high-density lipoprotein cholesterol treatment goals (with lower targets for higher-risk groups)
➡️ Expanded use of coronary artery calcium scoring to reclassify risk[ME1.1]
✍🏼 @rblument1 @tygluckman @RonBlankstein @PamelaBMorris @pnatarajanmd @AnnMarieNavar @SethShayMartin @APRN_CNS @nyulangone @DrMichaelShapir @kgradneyrd @eugeniagianos @virani_md @KellieMcLain1 @ijeomaheartdoc @SamiaMoraMD @DrHeatherJohn @dmljmd
9
148
329
115,714
28 Dec 2025
What a Christmas 🎄 call
VT/electrical storm needing #ECMO
Valvular #cardiogenicshock needing salvage BAV
Mid LAD #STEMI w/ critical LM bifurcation disease
Tamponade w/ hemorrhagic effusion
& a CCU that has not let up, all during a snowstorm!
Wouldn’t have it any other way 🙏🏽
7
8
99
14,492
29 Dec 2025
2/
Piling on to finish the call weekend:
Acute stent thrombosis of metal jacket LAD done a few days prior. With double layer in the prox
SCAI D AMI cardiometabolic shock
Multiple aspiration, repeated PTCA, distal vasodilators, MCS, lots of drugs
Very tough thrombus burden
1
342
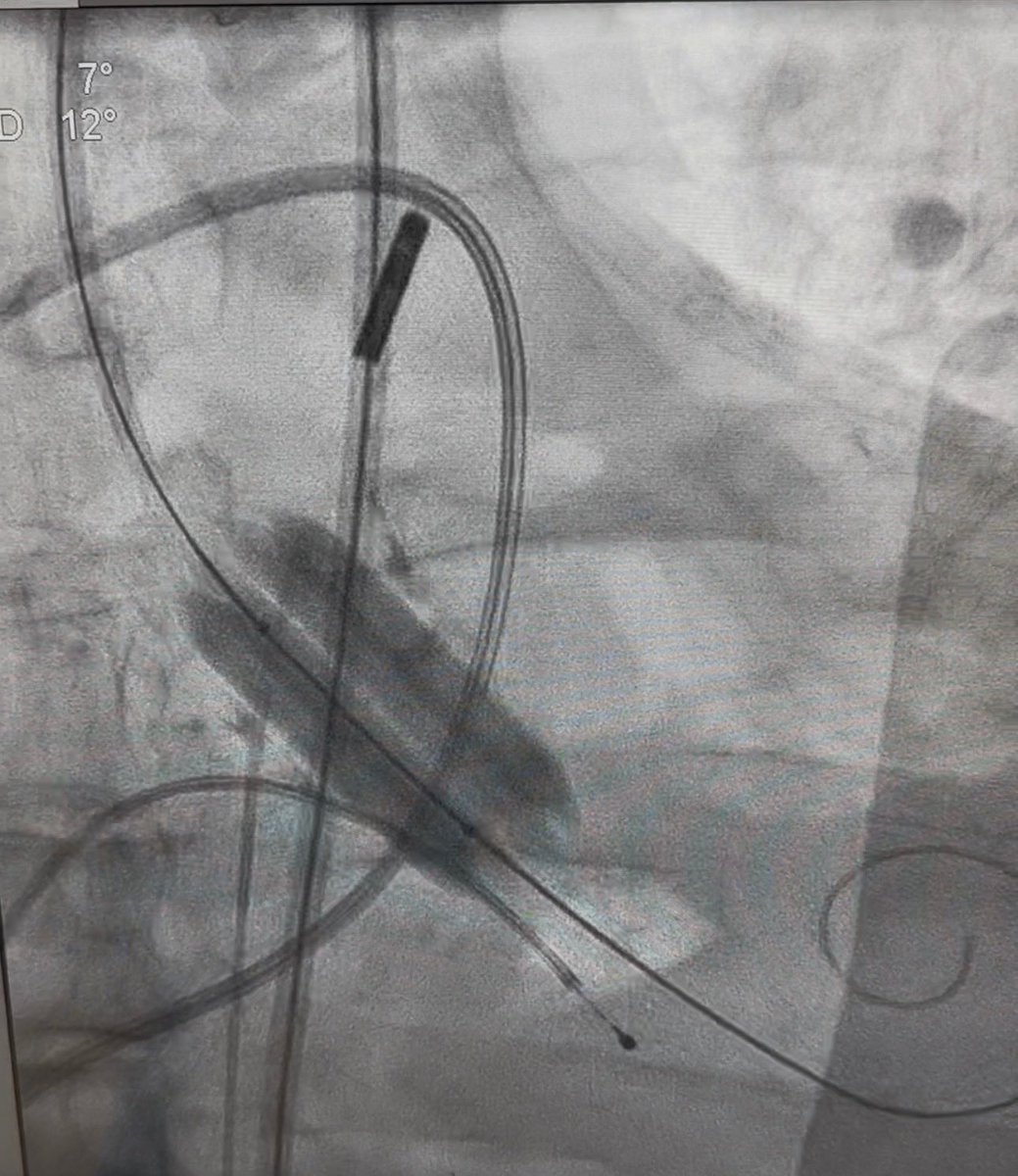
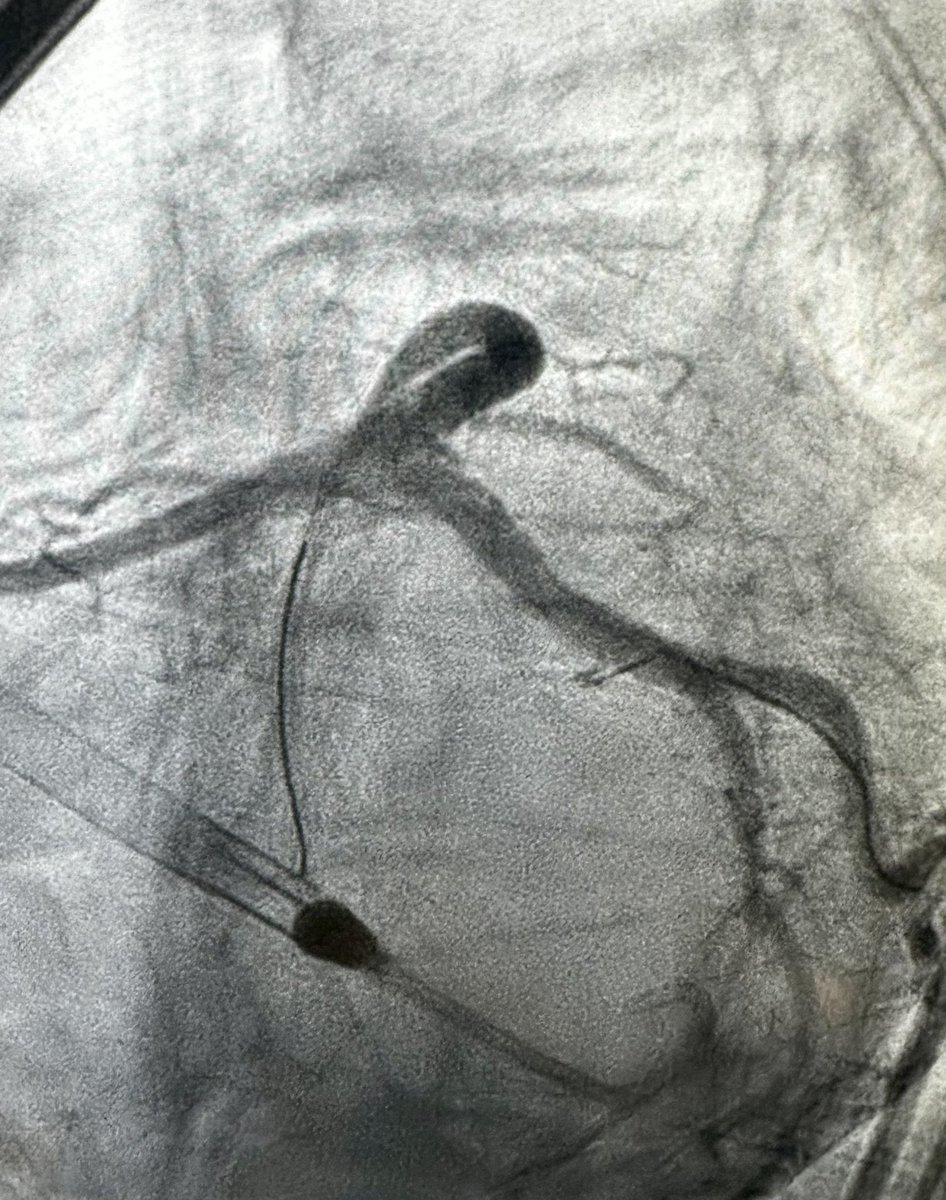
8 Nov 2025
Last weeks complex case:
60s, dilated CDM (LV 6.8cm, EF 20%). P/w refractory angina, limited meds due to low BP on GDMT
Not sick enough for transplant yet (ambulatory, CI 2.5, on oral 💊). Surgical turndown due to risk
🫀team➡️ PCI for QOL/angina
How would you approach? #CHIP

4
2
7
1,021
9 Nov 2025
3/
Ostial LM CSA - 3.2, severe dampening. 7Fr w/ SH, single access w/ tMCS
Wiring was tricky! Took an XTA & was able to wire into a septal off the aneurysm, then direct down to LAD
Up-front Rota 1.5 through LM -> mid LAD,
IVUS sized DESx2 mid LAD to Ostial LM. (Bumper wire)
1
327
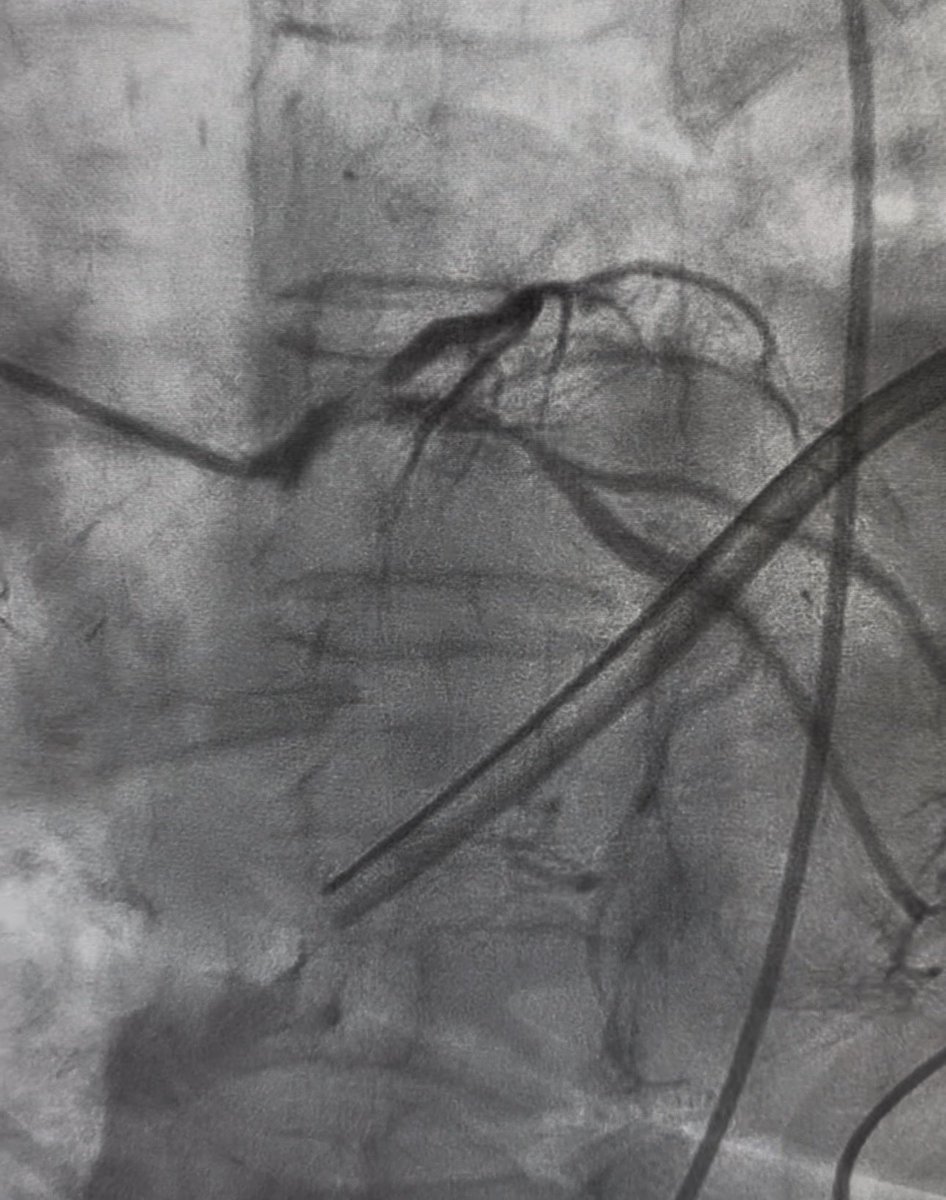
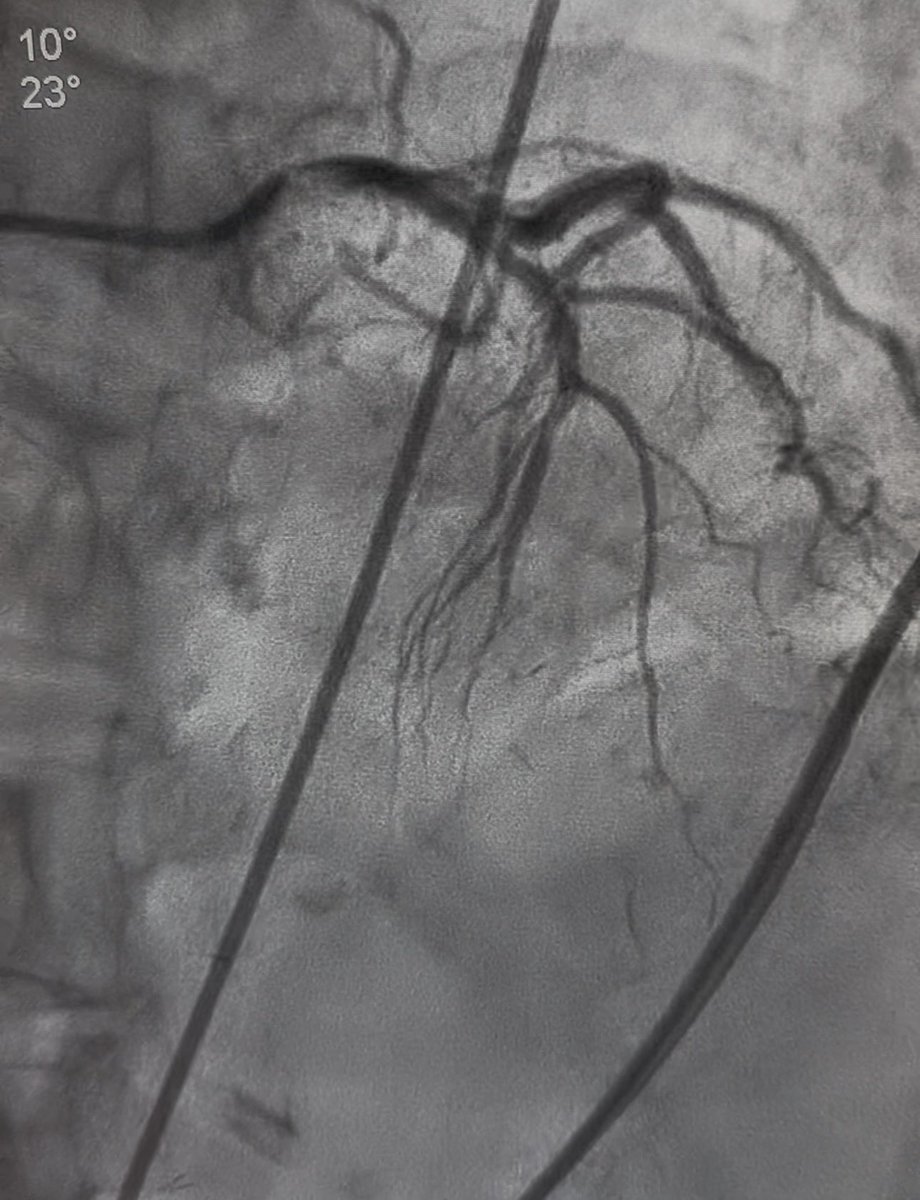
9 Nov 2025
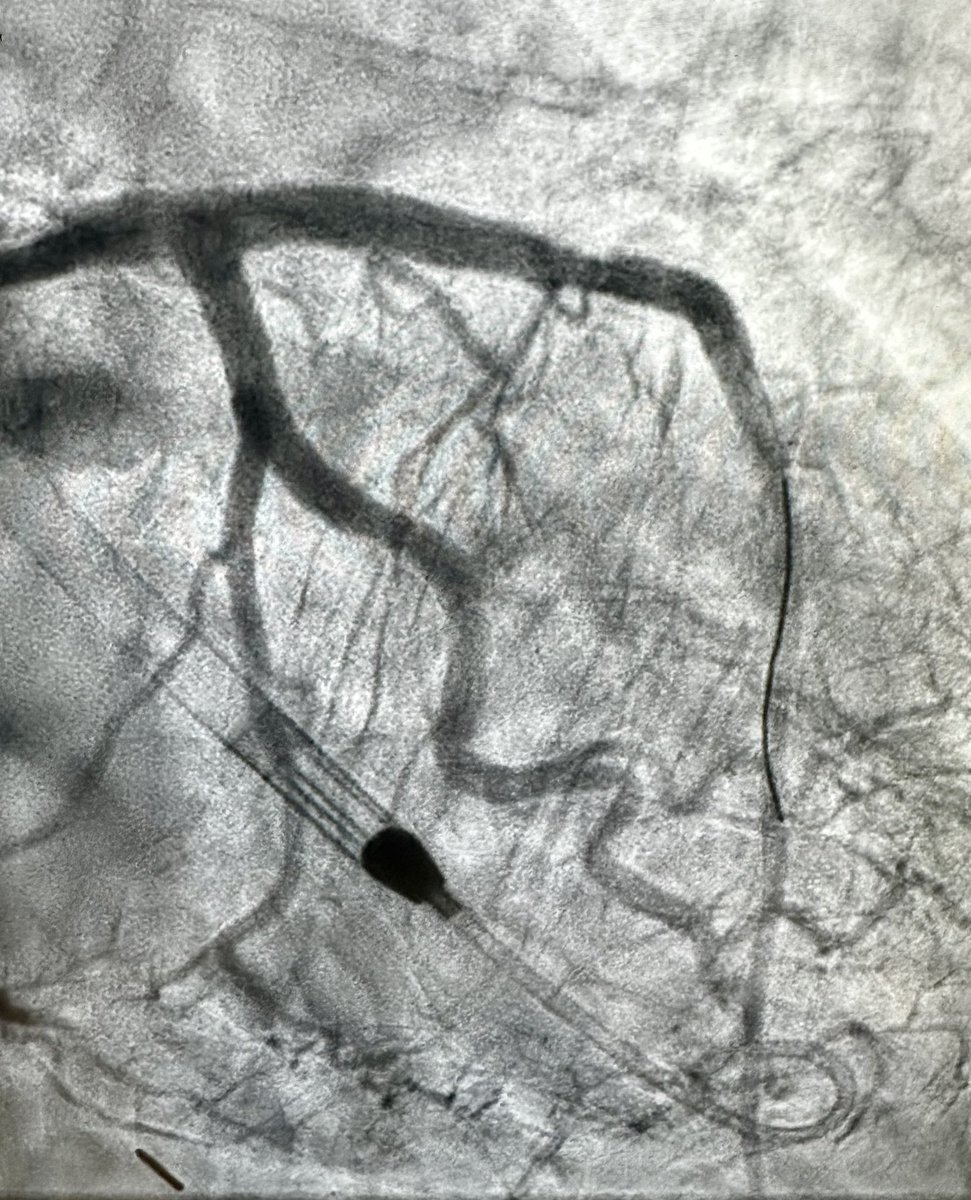
4/
Procedural clips and IVUS post stenting (post dilation performed after)
Will decide on RCA based on symptoms given cardiomyopathy.
1
246
Atul D. Bali, MD retweeted

24 Oct 2025
This week we hosted the first edition of the Northwell Cardiogenic Shock Skills day. Over 50 junior faculty members and fellows from cardiology, IC, CTS & CCM joined a day of hemodynamic simulations, hands-on tMCS and PAC learning and expert discussions of real-life CS cases.

1
1
9
631
24 Oct 2025
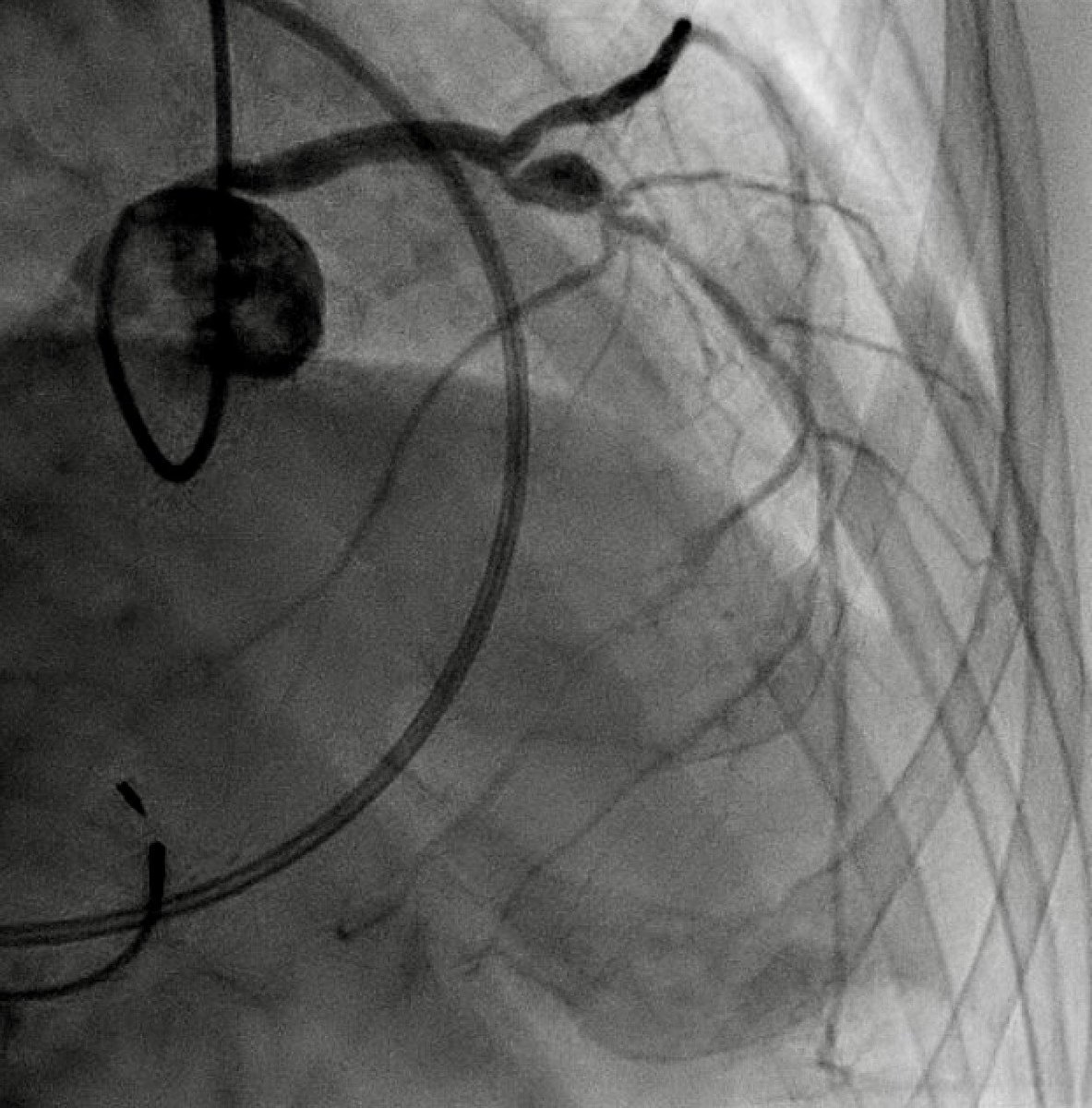
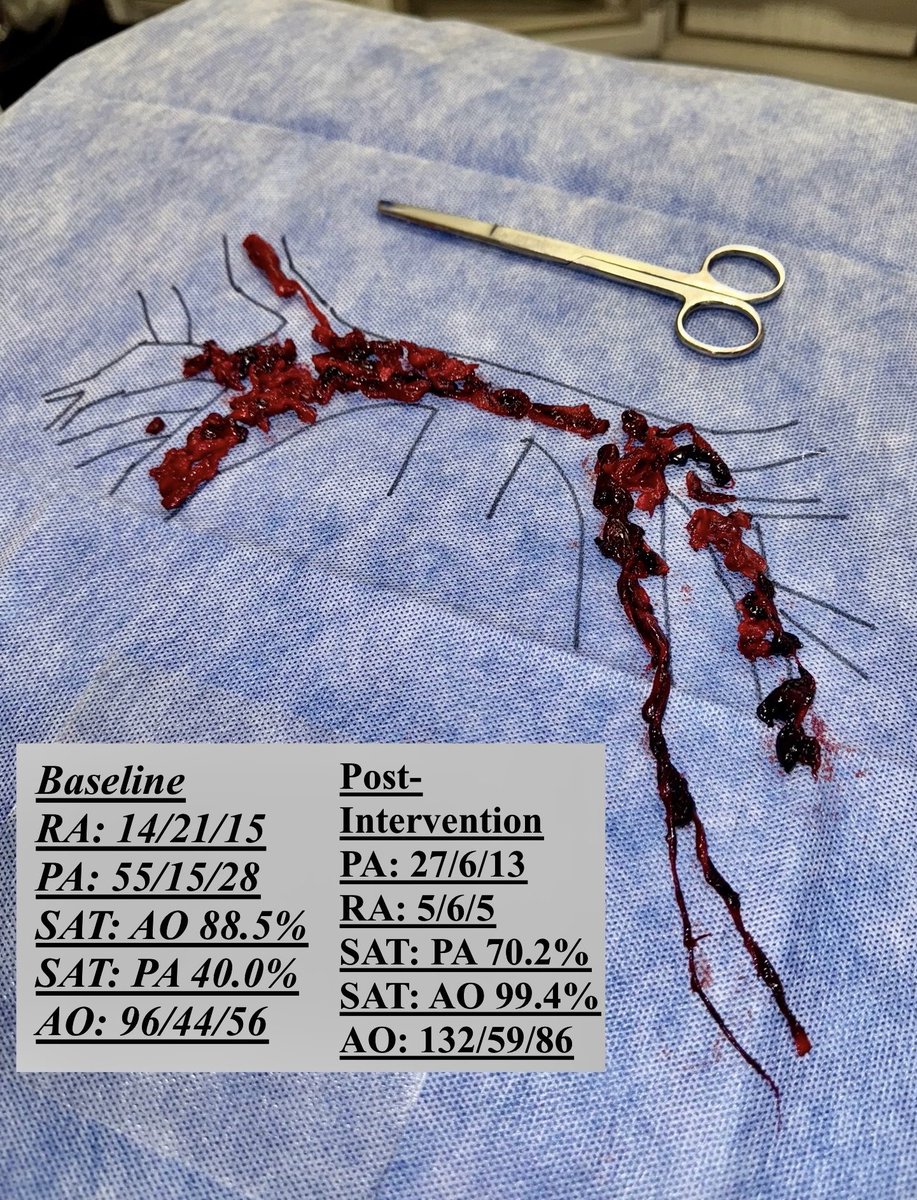
High risk PE on call last night🫀p/w syncope & ⬇️ BP
Heavily impacted bilateral PE w/ saddle, RV/LV 1.6. Opening hemos c/w normotensive shock (on inotropes CI 1.4). MCS on standby.
Immediate response to thrombectomy.
POD1 - walking, normal RV fxn on TTE.
#PERT @PERTConsortium
29
55
525
46,983
Atul D. Bali, MD retweeted

10 Oct 2025
“Every physician carries within himself a small cemetery, where from time to time he goes to pray.” — René Leriche
The guilt is real. Each name finds its place there, quiet and heavy.
What surprises me still are the families who meet loss with gratitude—who somehow thank you through their own heartbreak. That grace stays with you far longer than the failure ever does.
23
147
853
70,013
30 Aug 2025
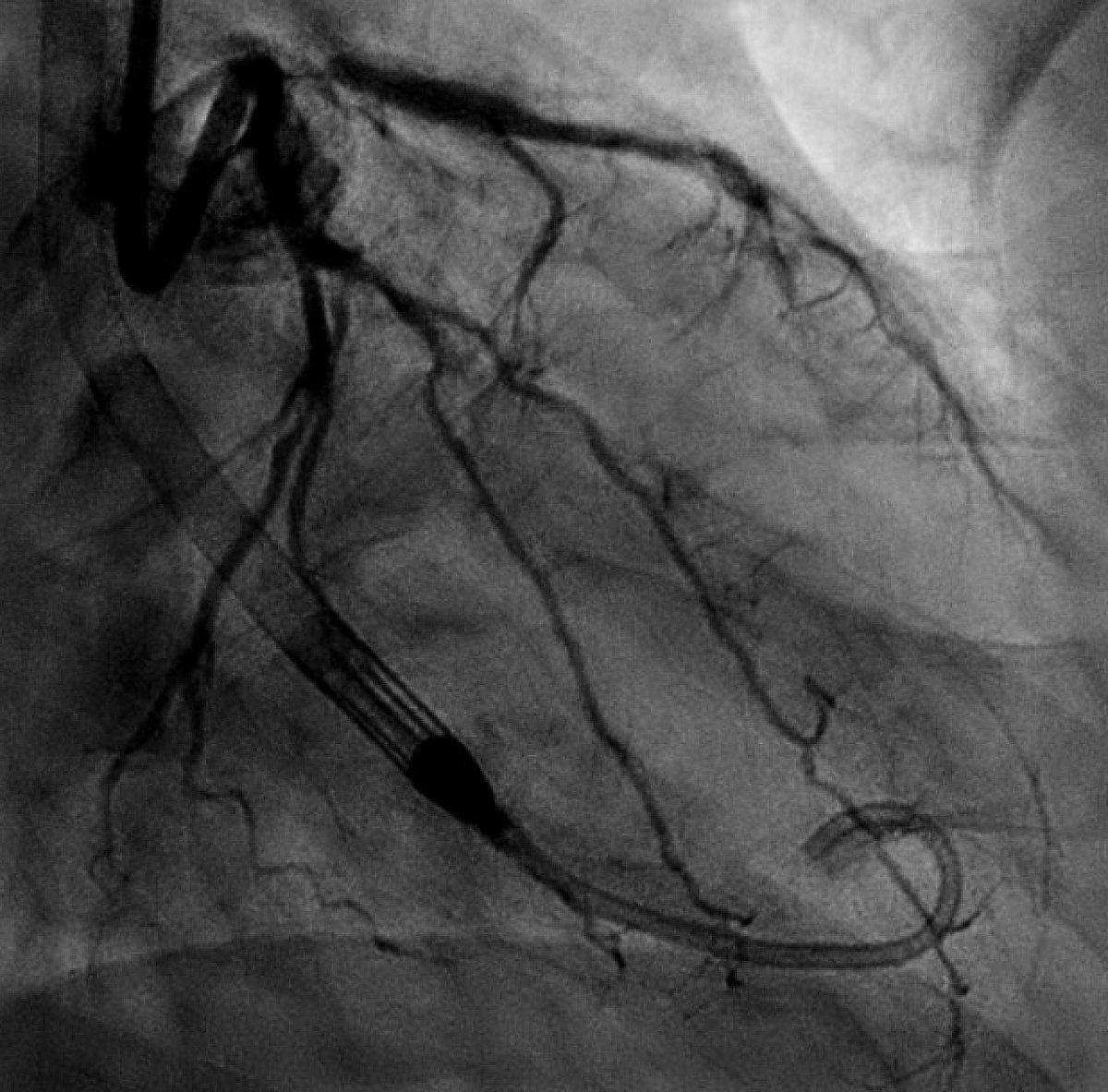
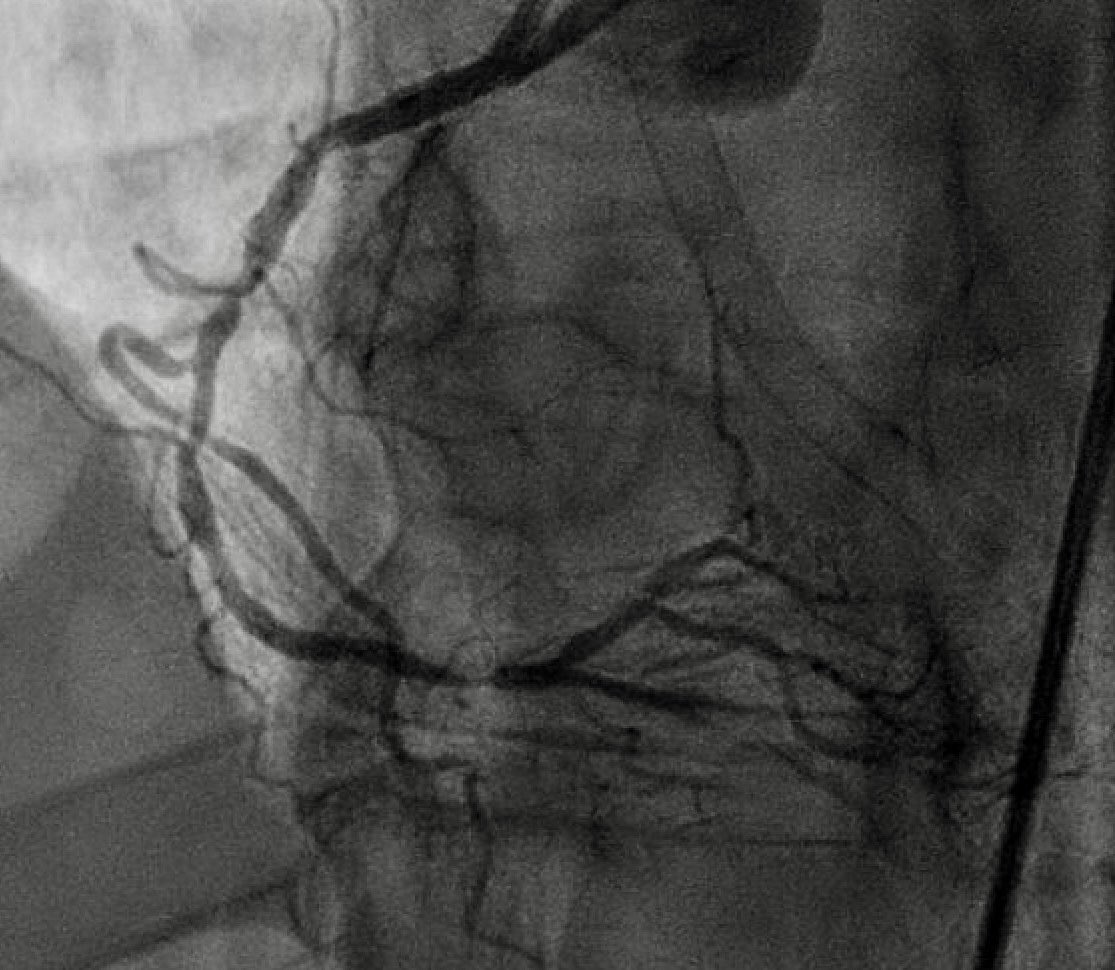
Iatrogenic LM ➡️ LAD dissection sent emergently from an outside hospital.
Operator was attempting IVUS of dLM nodularity, resulted in dissection, wire loss (unable to rewire). Long dissection flap & slow flow noted.
Transferred in for salvage PCI. What is your approach? 🫀

4
1
17
2,988
31 Aug 2025
4/
On IVUS, LM “appeared” free of dissection.
So I did the following:
- Rota 1.5 of LM into LCx calcium
- pt became ischemic -> Impella CP
- supercross 120 w/ mongo allows me to wire
- balloon to re-establish flow
- stent prox LAD, then mini crush to LM bifurcation
1
3
581
31 Aug 2025
5/
More case clips in the video below and final images:
Impella and all pressors off at end of case, discharged day after. 🫀
2
5
617
30 Aug 2025
Landscape changing data for oHCM🫀
Aficamten v Metoprolol monotherapy:
No reduction in LVOT gradients with metoprolol, worsening pVO2, worsening NTproBNP
A trial that challenges decades of practice!
#ESCCongress @NEJM @escardio
30 Aug 2025

Aficamten or Metoprolol Monotherapy for Obstructive Hypertrophic Cardiomyopathy: @NEJM #ESCCongress2025
🥸 Aficamten for HOCM
😱 Summary
👇👇👇
2
7
903
27 Aug 2025
Excited to share our work now out in @JACCJournals, important work led by @MAlvarezVillela:
🔥 Fever in AMI-CS is common and is associated with greater illness severity but seems to be noninfectious in most cases. 🫀
sciencedirect.com/science/ar…
1
1
3
661