
RN , ACCP, USS and POCUS enthusiast. Deluded football player / manager. Ex 90s dance child.
Joined March 2013
- Tweets 3,192
- Following 238
- Followers 290
- Likes 6,416
46 Photos and videos









Lee Berry retweeted
💧 Fluid Management in Sepsis and Septic Shock
Early, but Not Excessive
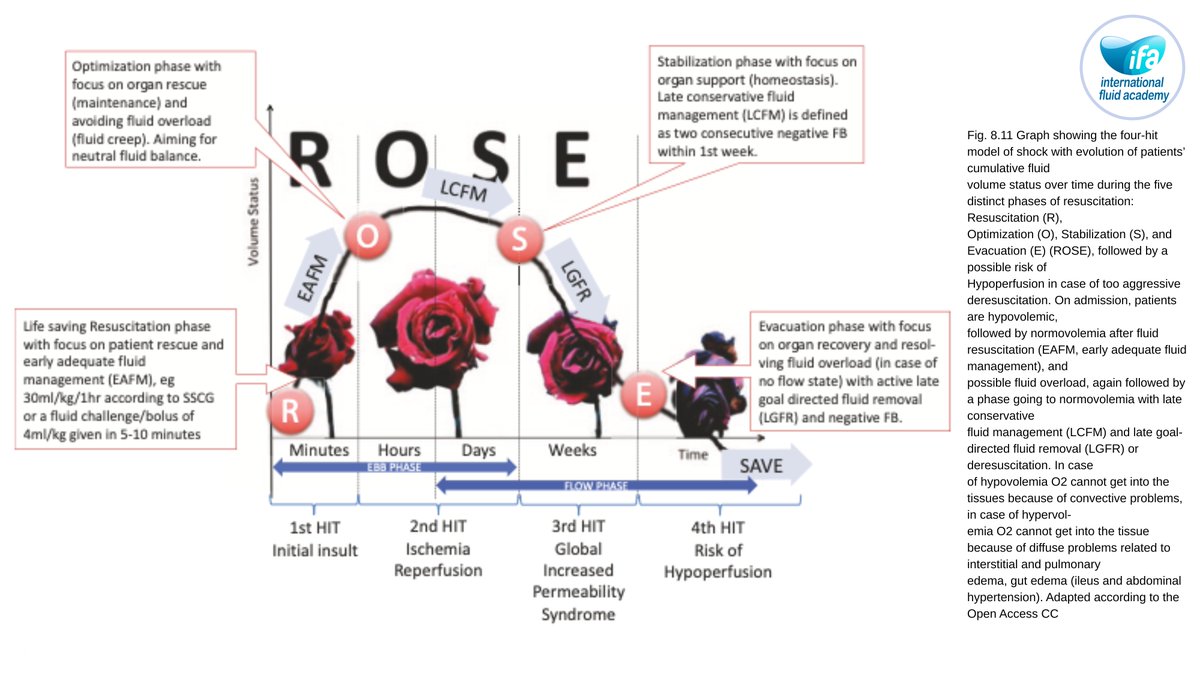
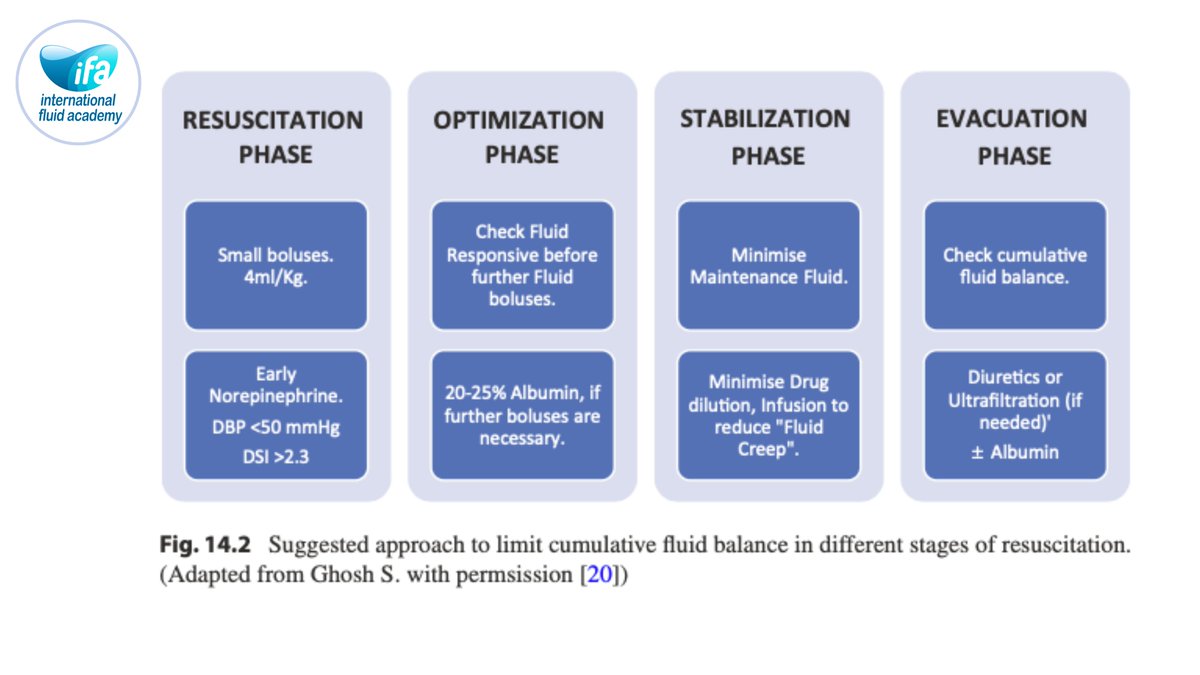
This core chapter revisits sepsis resuscitation in the era of stewardship, showing how initial fluids remain essential to reverse life‑threatening hypoperfusion, but fixed large bolus protocols can lead to harmful volume overload when applied indiscriminately. It integrates the ROSE concept, emphasizing short, targeted resuscitation followed by optimization and, where needed, timely evacuation.
Dynamic Assessment and Early Vasopressors
The authors advocate dynamic tests of fluid responsiveness (passive leg raising, stroke volume variation, echocardiographic indices) and early vasopressor support rather than repeated blind boluses. Evidence linking positive fluid balance with mortality in sepsis is summarized, underlining the need for explicit stop rules and deresuscitation plans once shock has resolved.
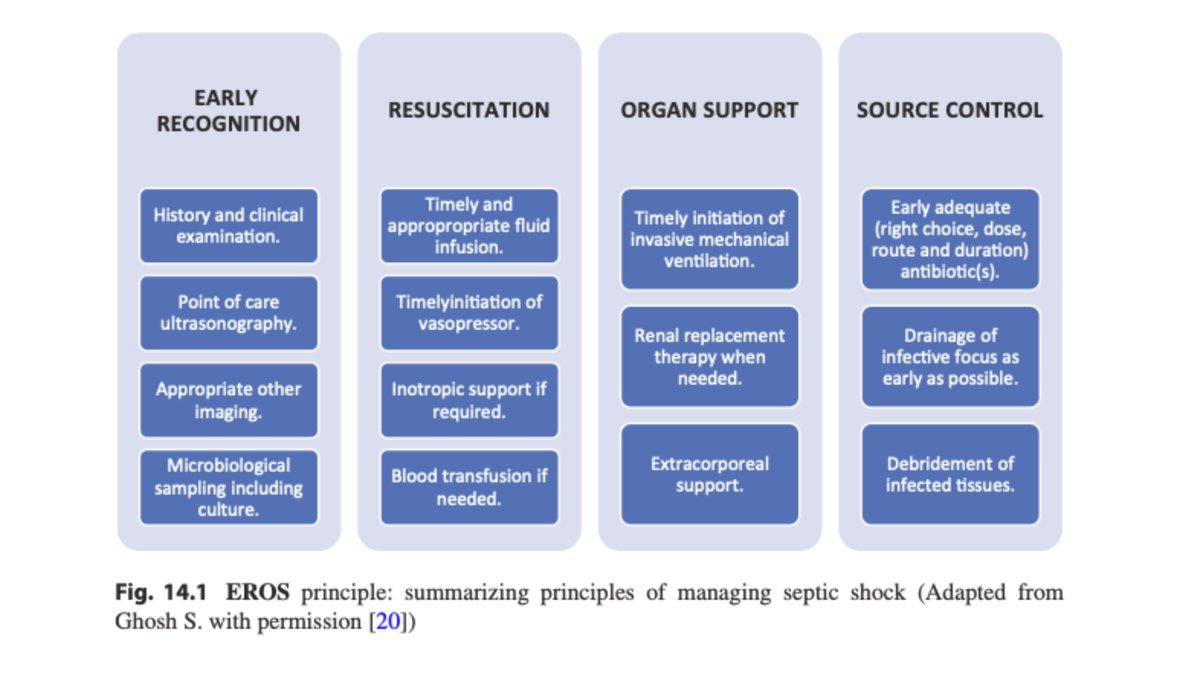
📘 Full sepsis algorithms and case vignettes in Chapter 14.
🔵 IFAD 2026 in Antwerp will devote multiple sessions to sepsis fluid management, including hands‑on hemodynamics and stewardship.
👉Registration: fluidacademy.org/ifad-2026-r…
#Sepsis #SepticShock #FluidResuscitation #ICU #ROSE #FluidStewardship
1
29
66
2,783
Lee Berry retweeted

Today's Paper of the Day is:
Lung fuction impairment following cerebral ischemic stroke: Pathophysiology, mechanisms, and clinical challenges
criticalcarereviews.com/late…
Join us to read 1 paper per day and stay up-to-date as we cover the spectrum of critical care across 2026

33
86
4,064
Lee Berry retweeted

#CCR26 is over!
12 outstanding RCTs presented!
😍Save and share this figure to keep a concise overview of the key information!
🎨 Color coding reflects my personal overall interpretation:
🟢 Benefit
⚪ No difference
🔴 Harm
Few practice-changing results but plenty to discuss!

5
35
74
7,877
Lee Berry retweeted

🫀 The Most Dangerous Moment in the ICU May Last Less Than 60 Seconds
We often think of tracheal intubation as an airway procedure. Physiologically, it is a profound cardiovascular intervention.
Why Do ICU Patients Crash During Intubation?
The problem begins before the laryngoscope enters the mouth.
Many critically ill patients survive on a fragile compensatory state characterized by:
🔹 Endogenous catecholamine surge
🔹 Tachycardia
🔹 Vasoconstriction
🔹 Increased myocardial oxygen demand
What appears to be "stable" hemodynamics may actually represent physiological exhaustion.
The moment induction drugs are administered, this compensatory sympathetic drive disappears.
The result? A sudden reduction in:
• Systemic vascular resistance
• Cardiac output
• Coronary perfusion pressure
• Organ blood flow
This phenomenon has been termed adrenergic collapse.
Intubation Is a Hemodynamic Timeline
The authors propose viewing intubation as a sequence of cumulative threats rather than a single procedure:
1️⃣ Pre-induction adrenergic dependence
2️⃣ Sympatholysis after induction
3️⃣ Apnea, hypoxemia, hypercapnia, and acidosis
4️⃣ Transition to positive-pressure ventilation
5️⃣ Post-intubation ventilator and sedation effects
Each phase adds physiological stress.
Together, they can culminate in cardiovascular collapse.
The Propofol Question
One of the most clinically relevant findings is the growing evidence regarding induction agent selection.
In the INTUBE cohort, propofol was associated with a higher risk of cardiovascular collapse and was the only modifiable risk factor consistently identified.
The review therefore suggests:
✅ Ketamine
✅ Etomidate
as preferred induction agents in patients at risk of hemodynamic instability, while propofol should be used cautiously in shock states.
Positive Pressure Ventilation: The Forgotten Hemodynamic Challenge
Once the tube is secured, many clinicians relax.
The physiology is only beginning.
Positive-pressure ventilation:
🔹 Reduces venous return
🔹 Increases intrathoracic pressure
🔹 Raises right ventricular afterload
🔹 May precipitate right ventricular failure
This is particularly relevant in ARDS, pulmonary hypertension, pulmonary embolism, and severe hypoxemic respiratory failure.
Reference 📚
Kotani Y, Koroki T, Hayashi Y, Russotto V. The hemodynamics of tracheal intubation in critically ill patients: a narrative review. Journal of Intensive Care. 2026;14:42. DOI: 10.1186/s40560-026-00877-4.

ALT
3
100
271
10,989
Lee Berry retweeted

From the first International Consensus Conference on Lung Ultrasound in 2012 to the updated document: 13 years of scientific growth, new evidence, and multidisciplinary collaboration.
#LungUltrasound #PoCUS #CriticalCare #EmergencyMedicine
link.springer.com/10.1007/s0…
15
13
833
Lee Berry retweeted
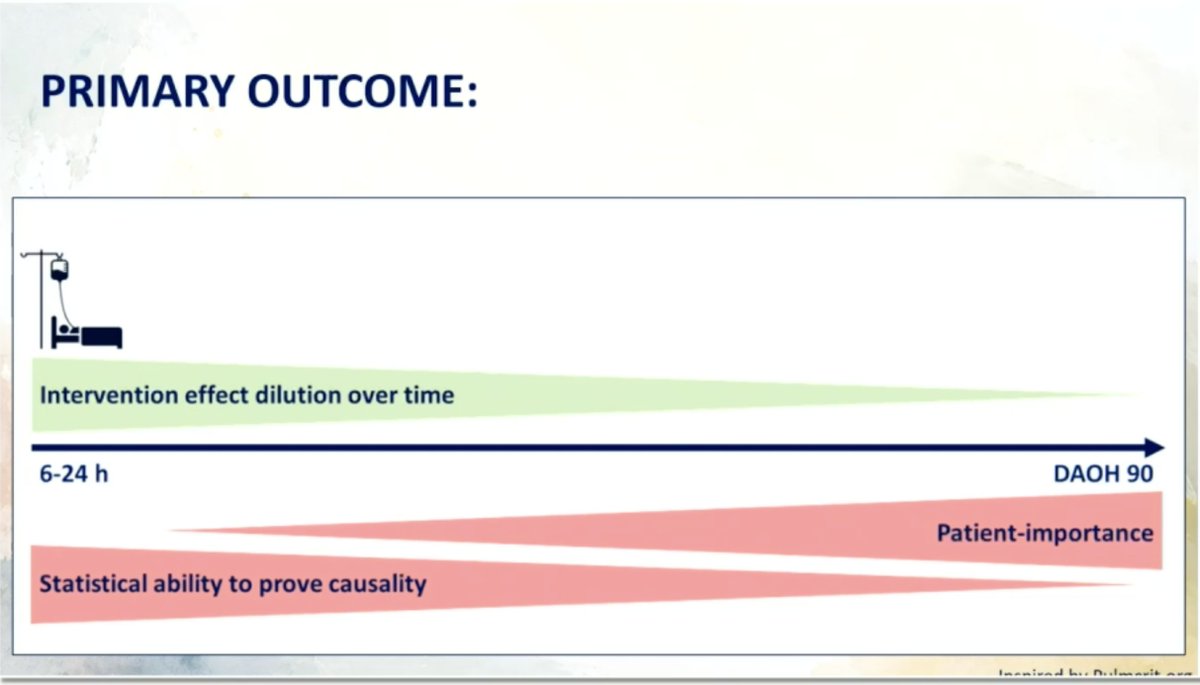
Love this figure from the editorialist at #CCR26
Patient-centered outcomes tell us whether an intervention matters. But intermediate outcomes may tell us why. Good critical care research needs both!
3
11
1,033
Lee Berry retweeted
@sandrapeake01 & @spjmacdonald presented the results of @ARISEFluidsRct at CCR26 this morning
ARISE-FLUIDS was simultaneously published in @NEJM
nejm.org/doi/10.1056/NEJMoa2…
Here is the trialists' brief summary.
4
16
1,861
Lee Berry retweeted

Jun 11
ARISE-FLUIDS has arrived and it's awesome 🥳
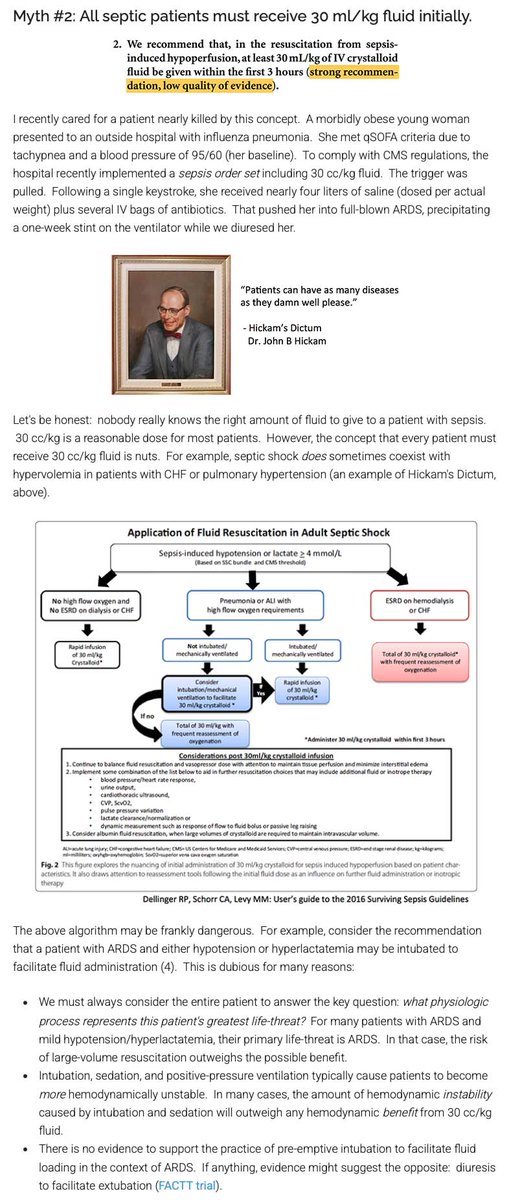
For over a decade, the Surviving Sepsis Guidelines recommended that septic patients get at least 30 cc/kg fluid. In the United States, these guidelines were weaponized into performance metrics, pressuring clinicians to prescribe arbitrary volumes to every patient.
Evidence-based clinicians have LONG known that this guideline lacked evidentiary support. For example, I've attached a picture of a blog I wrote about this back in 2017. Despite the lack of evidentiary support and some evidence of harm, the Surviving Sepsis Guidelines INSISTED on perpetually recommending 30 cc/kg fluid resuscitation.
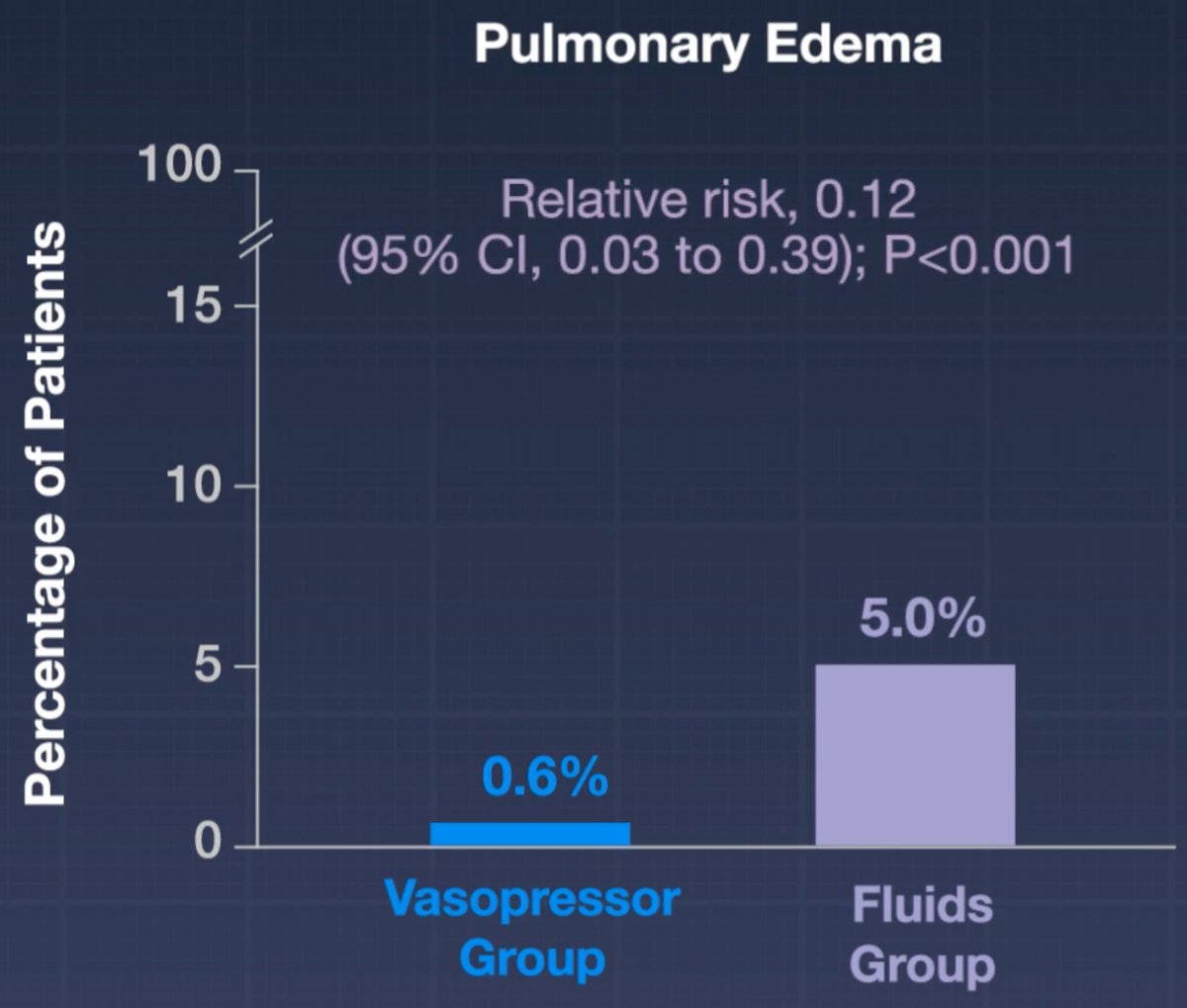
We finally have a prospective RCT demonstrating that mandating early administration of 30 cc/kg fluid (as compared to early vasopressors) doesn't help and may actually cause harm.
It's important to note that all of the hard endpoints in this trial were neutral (e.g., mortality, days free of organ support).
I still think that 30 cc/kg fluid is a pretty reasonable volume of fluid for *most* patients. But the study does suggest that giving too much fluid may promote edema - so we should be *thoughtful* about this intervention rather than mandating it for every septic patient.
Based on the subgroup analysis, the fluid-conservative strategy may have helped the subgroup of pneumonia patients the most. This is statistically nonsignificant but aligns with my expectation. ARDSy patients often don't respond well to fluid. (In contrast, I really doubt that a liter of fluids in either direction matters for most urosepsis patients.)
This is a great example of the over-reach of guidelines and protocoled medicine. People get all upset about practice variation, so sometimes they try to stomp it out using guidelines and protocols. But these guidelines are highly fallible, so what may occur is that you standardize care in a way that harms everyone equally. 🤦♂️


17
146
464
58,841
Lee Berry retweeted

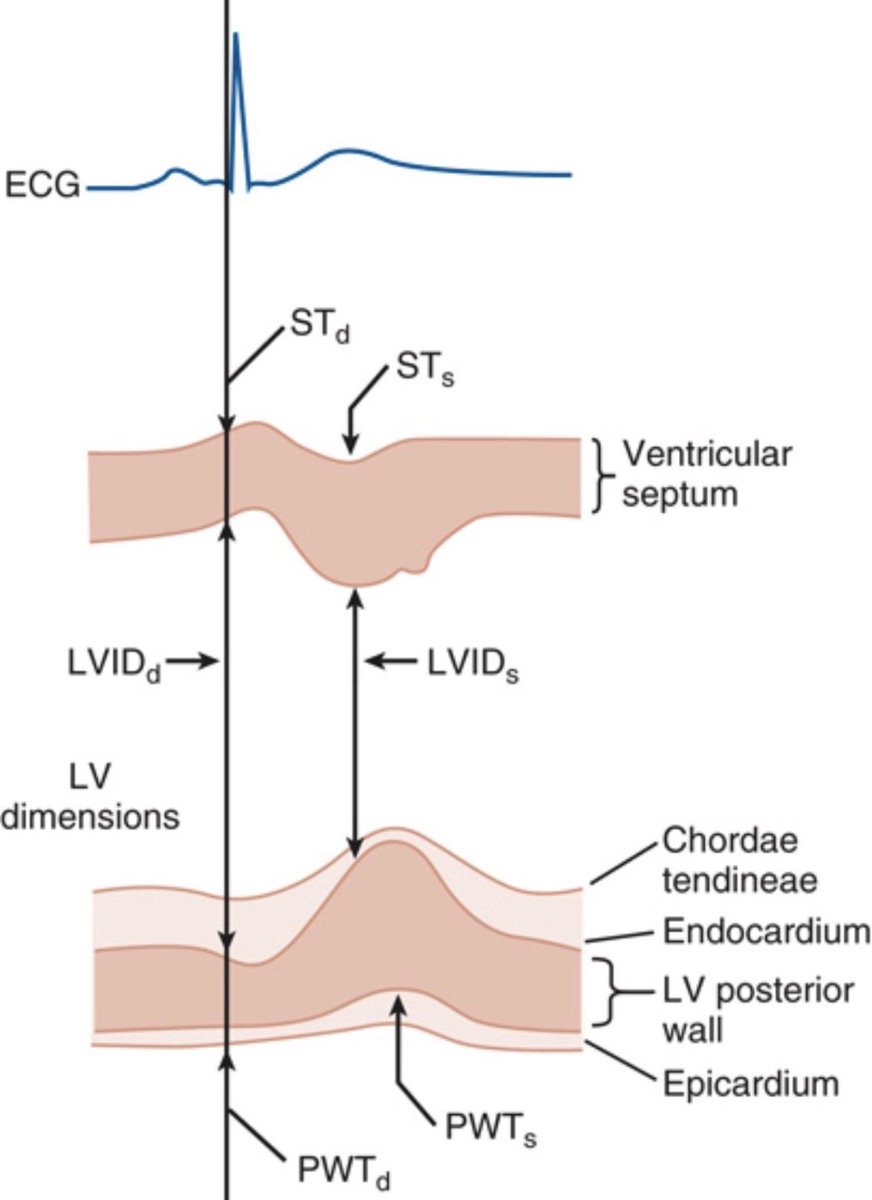
M-mode echocardiography remains a valuable tool for assessing left ventricular size and function.
Measurements such as LV dimensions, wall thickness, and fractional shortening continue to provide important insights into cardiac performance.
@ClevelandClinic
#MedTwitter #Echocardiography #Cardiology #CardiacImaging
2
13
34
1,297
Lee Berry retweeted
🫁 ARDS… or something else?
Every intensivist has faced it.
A patient arrives with acute hypoxemic respiratory failure, bilateral infiltrates, severe oxygenation impairment, and fulfills all clinical criteria for ARDS.
But what if it is not ARDS?
A timely review published in Intensive Care Medicine reminds us that approximately 8% of patients meeting ARDS criteria have no identifiable classical ARDS risk factor, and some of these patients harbor highly treatable diseases that require a completely different therapeutic strategy.
The authors propose a practical diagnostic framework for identifying ARDS mimickers, particularly when the presentation includes:
🔹 No clear ARDS risk factor
🔹 Subacute symptom onset
🔹 Extrapulmonary manifestations
🔹 Diffuse alveolar hemorrhage
🔹 Unexpected radiologic patterns
The major categories include:
✅ Immune-mediated diseases
• ANCA-associated vasculitis
• Anti-GBM disease
• Idiopathic inflammatory myopathies (anti-MDA5, antisynthetase syndrome)
✅ Drug-induced lung injury
• Amiodarone
• Chemotherapy
• mTOR inhibitors
• Immune checkpoint inhibitors
✅ Neoplastic pulmonary infiltration
✅ Idiopathic disorders
• Acute eosinophilic pneumonia
• Organizing pneumonia (OP)
One of the most useful concepts from this review is that diagnosis should not rely solely on the chest CT.
Instead, intensivists should combine:
📌 Detailed history and medication review
📌 Extrapulmonary examination (skin, joints, muscles, kidneys)
📌 Autoimmune testing
📌 Bronchoscopy with BAL
📌 Pattern recognition on CT imaging
The article highlights several time-critical diagnoses not to miss:
⚠️ Anti-MDA5 dermatomyositis and antisynthetase syndrome
ICU mortality approaches 50%, and up to 20% of patients require VV-ECMO. Early aggressive immunosuppression is essential.
⚠️ ANCA-associated vasculitis and anti-GBM disease
Prompt recognition of diffuse alveolar hemorrhage and initiation of immunosuppression can be life-saving and kidney-saving.
⚠️ Immune checkpoint inhibitor pneumonitis
A rapidly growing cause of severe respiratory failure in oncology patients that often responds to corticosteroid therapy if recognized early.
The key message is simple:
Not every patient fulfilling ARDS criteria has diffuse alveolar damage.
When classical risk factors are absent, the diagnosis should trigger curiosity rather than closure.
Because sometimes the difference between survival and mortality lies in recognizing the mimicker.
Question for the ICU community:
What is the most memorable ARDS mimicker you have encountered in your practice?
Reference 📚
Bay P, Gibelin A, de Prost N. Acute respiratory distress mimickers: a practical approach for intensivists. Intensive Care Medicine. 2026. DOI: 10.1007/s00134-026-08496-1.
ALT
2
42
135
4,316
Lee Berry retweeted

Chiumello et al explore why females are less likely to receive lung protective ventilation in #ARDS leading to higher mortality compared to males in this BJA #Editorial.
bjanaesthesia.org/article/S0…
7
16
1,366
Lee Berry retweeted

Jun 10
How should we resuscitate patients with septic shock when there are competing priorities (e.g. fluid responsiveness and fluid tolerance).
Come find out! @katiewiskar @john_basmaji @edu_kattan and I are going to discuss this live.
When: June 10th, 2026 3pm EST (12pm PST)
Free Webinar Link: hubs.ly/Q04hyRNf0
See you there!
5
12
55
4,766
Lee Berry retweeted

Jun 10
Check out the latest episode of Critical Care Trials, all popped together so you can update quickly!
👇👇
criticalcarenorthampton.com/…
#CriticalCare #ICU #IntensiveCare #Anaesthesia #Anesthesia #Anesthesiology #CritCare #ICUnurse #ICUMedicine #FOAMcc #FOAMed #Medicine #Medical #MedEd #EmergencyMedicine #Resuscitation
2
13
21
1,685
Lee Berry retweeted

A gift from us to you
Try this Ventilator Simulator, calculate total System and Trans-Pulmonary work/energy, its components
societymechanicalventilation…


8
14
1,313
Lee Berry retweeted
In ICU, the wrong drug can make a bad situation worse
➡️ Join AOP Health at CCR26 for @Whitehouse_ICU
➡️ Practical choices in drug treatment for ICU tachyarrhythmias
➡️ Thursday June 11, 15:05–15:25
➡️ Full, free livestream
criticalcarereviews.com
#CCR26

5
17
2,153
Lee Berry retweeted
APRV has always divided opinion
➡️ Join Dräger at CCR26 for Prof Luigi Camporota on the RELEASE Trial
➡️ Revisiting APRV from physiology to clinical implications
➡️ Wednesday June 10, 12:40–13:20
➡️ Full, free livestream
criticalcarereviews.com
#CCR26

1
6
32
2,231
Lee Berry retweeted
Today's Paper of the Day is:
Bedside ventilatory settings guided by respiratory mechanics in acute respiratory distress syndrome
criticalcarereviews.com/late…
Join us to read 1 paper per day and stay up-to-date as we cover the spectrum of critical care across 2026

35
123
5,047

Lee Berry retweeted

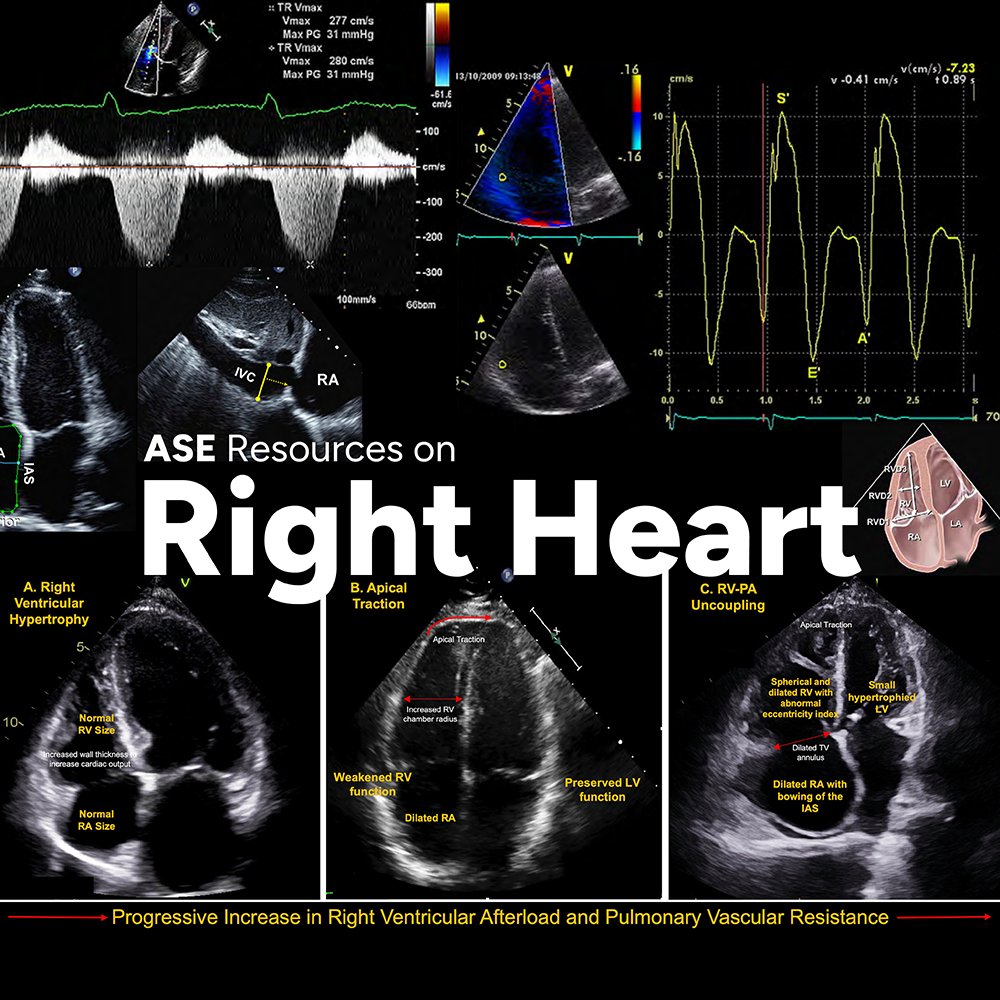
ASE and @accpchest recently partnered on a project to develop two educational webinars to improve the understanding of cardiovascular ultrasound's application in pulmonary hypertension (PH). @chest
You can find them on our Right Heart Resources web page! bit.ly/4nQ5E7p
54
150
6,252
Lee Berry retweeted

Jun 8
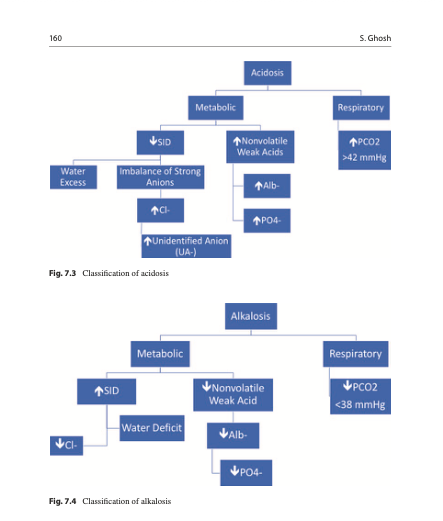
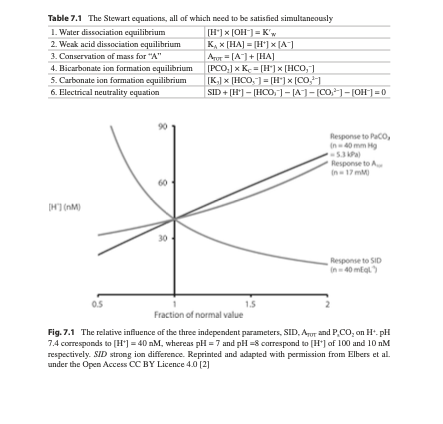
💧 Acid–Base Effects of IV Fluids – Stewart Approach
Beyond bicarbonate: Strong Ion Difference
This chapter introduces the Stewart approach, where pH is determined by strong ion difference, PaCO₂ and weak acids rather than bicarbonate alone. It shows how chloride‑rich fluids reduce the strong ion difference and drive hyperchloremic metabolic acidosis, whereas balanced solutions better preserve acid–base equilibrium.
Clinical Application at the Bedside
Through worked examples, the authors demonstrate how to interpret ABGs after large volumes of saline vs balanced crystalloids. Recognizing fluid‑induced acid–base changes helps clinicians adjust both fluid choice and ventilatory strategy, especially in patients with sepsis, kidney injury or major surgery.
📘 Detailed figures and case discussions in the acid–base chapter: link.springer.com/book/10.10…
🔵 At IFAD 2026, a dedicated session will apply the Stewart approach to real ICU blood gases and fluid decisions.
👉Registration: fluidacademy.org/ifad-2026-r…
#AcidBase #StewartApproach #Chloride #ICU


46
131
6,417