
GenitoUrinary Alliance for Research and Development
Joined February 2023
- Tweets 698
- Following 223
- Followers 815
- Likes 458
277 Photos and videos








🔬 GUARD Consortium impulsa 6 ensayos clínicos en oncología genitourinaria a escala europea:
▸ RINGQUEST
▸ Quantum
▸ REGUARD
▸ REINFORCE
▸ STAMPEDE
▸ THUNDER
Ciencia colaborativa. Impacto real en los pacientes.
#GUARDConsortium #ClinicalTrials #GUOncology #Oncología @DrFelixGuerrero @cdanicas @dralvaropinto @drenriquegrande @fcounago @docjavip @BerUrologia @DrJaVallejo @Maroto5Pablo @nachoduranm @RodriguezAntona @AnaPlatabello1
4
7
619
📍Ayer, especialistas de GUARD Consortium estuvieron presentes en el 89.º Congreso Nacional de Urología de @InfoAeu celebrado en Madrid.
Los dres. Teresa Alonso Gordoa, @dralvaropinto, Carmen Gómez del Cañizo, @PelechanoPaula, Ainara Azueta, @abraocantoMD, @Hilario_FH y Javier Molina, participaron en esta cita científica de referencia para seguir compartiendo conocimiento, generando nuevas colaboraciones y avanzando en la investigación de los tumores genitourinarios.
Seguimos comprometidos con una oncología cada vez más innovadora, multidisciplinar y centrada en el paciente.
#GUARDConsortium #AEU2026 #Urología #GUOncology #Oncología #InvestigaciónClínica #CáncerGU
6
9
1,559
Detrás del GUARD International Symposium 2026 hay un equipo científico de primer nivel:
👤 Dr. Daniel Castellano · HU 12 de Octubre, Madrid
👤 Dr. Alfonso Gómez de Liaño · CH Universitario Insular Materno-Infantil, Las Palmas
👤 Dr. Félix Guerrero · HU 12 de Octubre, Madrid
👤 Dr. Fernando López Campos · HU Ramón y Cajal, Madrid
👤 Dra. Ana Plata · HU La Laguna, Tenerife
👤 Dra. Cristina Rodríguez González de Antona · IIB CSIC/UAM, Madrid
👤 Dr. Juan Antonio Vallejo · HU Reina Sofía, Córdoba
Un comité multidisciplinar y de alcance nacional.
TODA LA INFO ➡️ guardconsortium.org/activida…
@DrFelixGuerrero @cdanicas @dralvaropinto @drenriquegrande @fcounago @docjavip @BerUrologia @DrJaVallejo @Maroto5Pablo @nachoduranm @RodriguezAntona @AnaPlatabello1 @Uro_Oncologist
6
11
563
🔹 Esta tarde participamos en el 89.º Congreso Nacional de Urología de la @InfoAeu, que se celebra desde ayer en el Palacio Municipal de Congresos de Madrid.
Desde #GUARDConsortium estaremos presentes en el Simposio GUARD, abordando el papel de los biomarcadores, la toma de decisiones multidisciplinar y las perspectivas de futuro en cáncer renal junto a destacados especialistas.
Nos vemos a las 16:00 h.
#AEU2026 #CáncerRenal #Biomarcadores #GUARDConsortium #Urología #OncologíaRenal @DrFelixGuerrero @cdanicas @dralvaropinto @drenriquegrande @fcounago @docjavip @BerUrologia @DrJaVallejo @Maroto5Pablo @nachoduranm @RodriguezAntona @AnaPlatabello1
3
3
299
Hoy, 11 de junio, es el Día Mundial del #CáncerDePróstata
1 de cada 8 hombres lo padecerá. Si se detecta a tiempo, la tasa de curación supera el 90%.
Hazte la prueba PSA a partir de los 45 años — o antes si tienes antecedentes familiares.
#DiaMundial #SaludMasculina #GuardConsortium @DrFelixGuerrero @cdanicas @dralvaropinto @drenriquegrande @fcounago @docjavip @BerUrologia @DrJaVallejo @Maroto5Pablo @nachoduranm @RodriguezAntona @AnaPlatabello1
4
7
269
El carcinoma de células renales representa aproximadamente el 2-3% de todos los tumores malignos en adultos y su incidencia ha aumentado en las últimas décadas.
El diagnóstico incidental gracias a técnicas de imagen ha cambiado el perfil del paciente que llega a consulta.
Fuente: @_SEOM
#GUARDConsortium #GUOncology #CancerRenal #Oncología @DrFelixGuerrero @cdanicas @dralvaropinto @drenriquegrande @fcounago @docjavip @BerUrologia @DrJaVallejo @Maroto5Pablo @nachoduranm @RodriguezAntona @AnaPlatabello1
1
4
4
461
🧬 El miércoles 16 de septiembre arrancamos #guardsymposium2026 con la mesa de CÁNCER DE PRÓSTATA LOCALIZADA DE ALTO RIESGO.
Radioterapia de rescate vs adyuvante, SBRT y biomarcadores.
¡No te lo pierdas! INSCRÍBETE ➡️ guardconsortium.org/activida…
@DrFelixGuerrero @cdanicas @dralvaropinto @drenriquegrande @fcounago @docjavip @BerUrologia @DrJaVallejo @Maroto5Pablo @nachoduranm @RodriguezAntona @AnaPlatabello1 @Uro_Oncologist
7
11
479
La semana pasada en #ASCO2026 Chicago, la oncología genitourinaria ha sido protagonista.
Inmunoterapia combinada, ADCs, biomarcadores, PSMA PET, calidad de vida del paciente...
¿Cuál es el avance que más te ha llamado la atención?
🔵 Nuevas combinaciones en cáncer renal
🟢 ADCs en cáncer de vejiga
🔴 Hormonoterapia neoadyuvante en próstata
⚪ Biomarcadores y medicina de precisión
👇 Cuéntanos en comentarios
#GUARDConsortium #GUOncology #Oncología #ASCO2026 @DrFelixGuerrero @cdanicas @dralvaropinto @drenriquegrande @fcounago @docjavip @BerUrologia @DrJaVallejo @Maroto5Pablo @nachoduranm @RodriguezAntona @AnaPlatabello1
3
7
467
El Dr. @nachoduranm presentó en #ASCO2026 los datos actualizados del estudio Duravelo-1 B7.
Zelenectide pevedotin pembrolizumab en pacientes con carcinoma urotelial localmente avanzado/metastásico no elegibles para cisplatino — una población con pronóstico históricamente desfavorable:
🔵 50% de tasa de respuesta objetiva confirmada
🟢 Supervivencia libre de progresión: 13 meses
🟣 82% de control de enfermedad
🔵 5 respuestas completas
Perfil de seguridad diferencial respecto a los ADC convencionales. Datos que abren el camino a Duravelo-2 (fase 2/3).
Gracias a los investigadores, centros participantes y a los pacientes.
#ASCO2026 #UrothelialCarcinoma #Oncología #Duravelo #Investigación #GuardConsortium @DrFelixGuerrero @cdanicas @dralvaropinto @drenriquegrande @fcounago @docjavip @BerUrologia @DrJaVallejo @Maroto5Pablo @RodriguezAntona @AnaPlatabello1
4
9
426
🔬 GUARD Consortium lanza una Ayuda de Investigación en Tumores Genitourinarios
💰 Dotación: 40.000 €
📅 Plazo: hasta el 27 de septiembre de 2026
🎯 Dirigida a profesionales que tratan tumores GU en España
Fomenta la investigación clínica y traslacional independiente.
📋 Bases e inscripción 👇
guardconsortium.org/investig…
@DrFelixGuerrero @cdanicas @dralvaropinto @drenriquegrande @fcounago @docjavip @BerUrologia @DrJaVallejo @Maroto5Pablo @nachoduranm @RodriguezAntona @AnaPlatabello1
6
11
762
📖 LECTURA RECOMENDADA
Nuevos avances en imagen molecular y medicina de precisión podrían mejorar el abordaje del cáncer de próstata recurrente.
Las técnicas PET/TC con PSMA continúan ganando protagonismo en la toma de decisiones clínicas.
Recuperamos este artículo vía @larazon_es 👇 larazon.es/salud/logran-espe…
@DrFelixGuerrero @cdanicas @dralvaropinto @drenriquegrande @fcounago @docjavip @BerUrologia @DrJaVallejo @Maroto5Pablo @nachoduranm @RodriguezAntona @AnaPlatabello1
3
6
465
📍 El GUARD Symposium 2026 se celebra en el Espacio Maldonado (Madrid).
Presencial y en streaming 🗓️ 16-18 septiembre
¿Nos vemos allí?
👇 #guardsymposium2026 @DrFelixGuerrero @cdanicas @dralvaropinto @drenriquegrande @fcounago @docjavip @BerUrologia @DrJaVallejo @Maroto5Pablo @nachoduranm @RodriguezAntona @AnaPlatabello1 @Uro_Oncologist @F_lopez_campos
7
10
692
🔬 Clinical Insight
La creciente disponibilidad de opciones terapéuticas en tumores genitourinarios plantea un nuevo desafío: definir la mejor secuencia de tratamiento para cada paciente.
La investigación clínica continúa trabajando para responder cuándo, cómo y para quién.
#ClinicalInsight #GUOncology @DrFelixGuerrero @cdanicas @dralvaropinto @drenriquegrande @fcounago @docjavip @BerUrologia @DrJaVallejo @Maroto5Pablo @nachoduranm @RodriguezAntona @AnaPlatabello1
1
2
4
245
🔬 ¡Ya está aquí! El GUARD International Symposium 2026 se celebra los días 16-18 de septiembre en Madrid. Tres días de ciencia, debate y avances en uro-oncología.
🗓️ ¡Consulta el programa preliminar y reserva tu plaza!👇 guardconsortium.org/activida…
#guardsymposium2026 @DrFelixGuerrero @cdanicas @dralvaropinto @drenriquegrande @fcounago @docjavip @BerUrologia @DrJaVallejo @Maroto5Pablo @nachoduranm @RodriguezAntona @AnaPlatabello1 @Uro_Oncologist @F_lopez_campos
9
11
529
🎯 ¿Estamos ante un cambio de práctica clínica en cáncer de próstata de alto riesgo?
El debate continúa, pero la integración de PET-PSMA basal, biomarcadores y bpMRI apunta hacia una estratificación más precisa de los pacientes y una mejor toma de decisiones terapéuticas.
Seguimos atentos a los avances presentados en #ASCO26
#ProstateCancer #GUOncology #ASCO26 #GUARDConsortium #PrecisionOncology
Jun 1

🎯 Excellent discussion @ASCO @declangmurphy as usual!! @gu_onc !! @ASCOPres It’s practice changing? Yes or no we have a new opportunity for our pts! We need more information to better define a HRPCa➡️ baseline PET-PSMA, biomarkers, bpMRI! @DrChoueiri @GuardConsortium
1
133
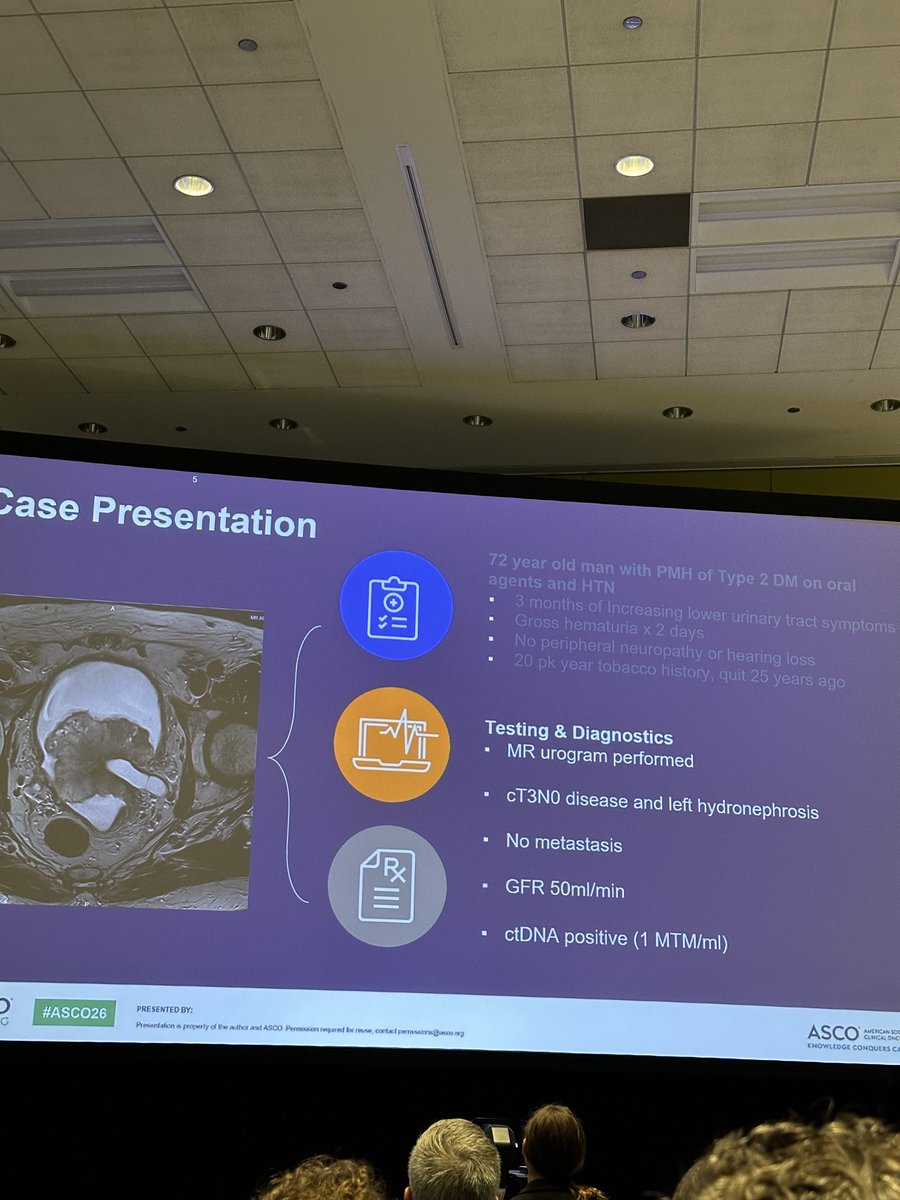
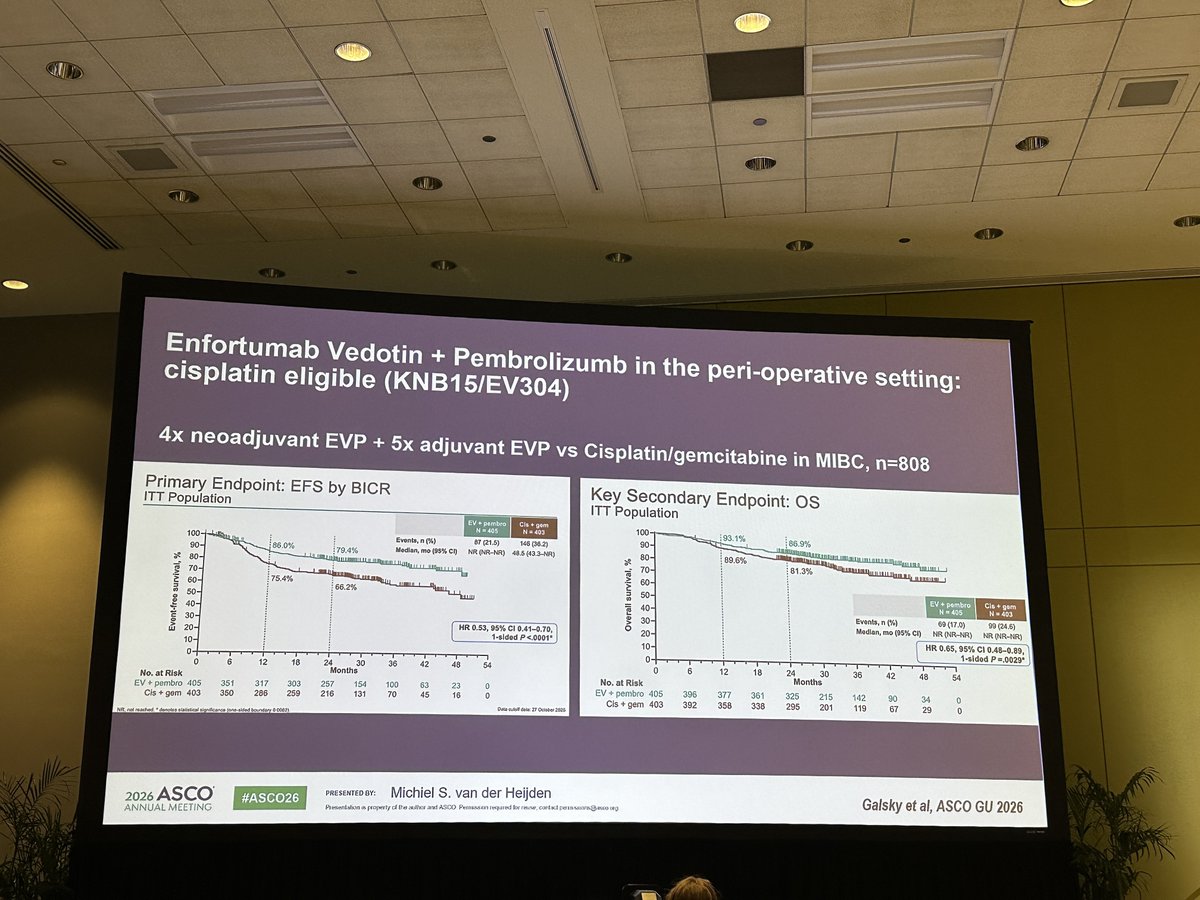
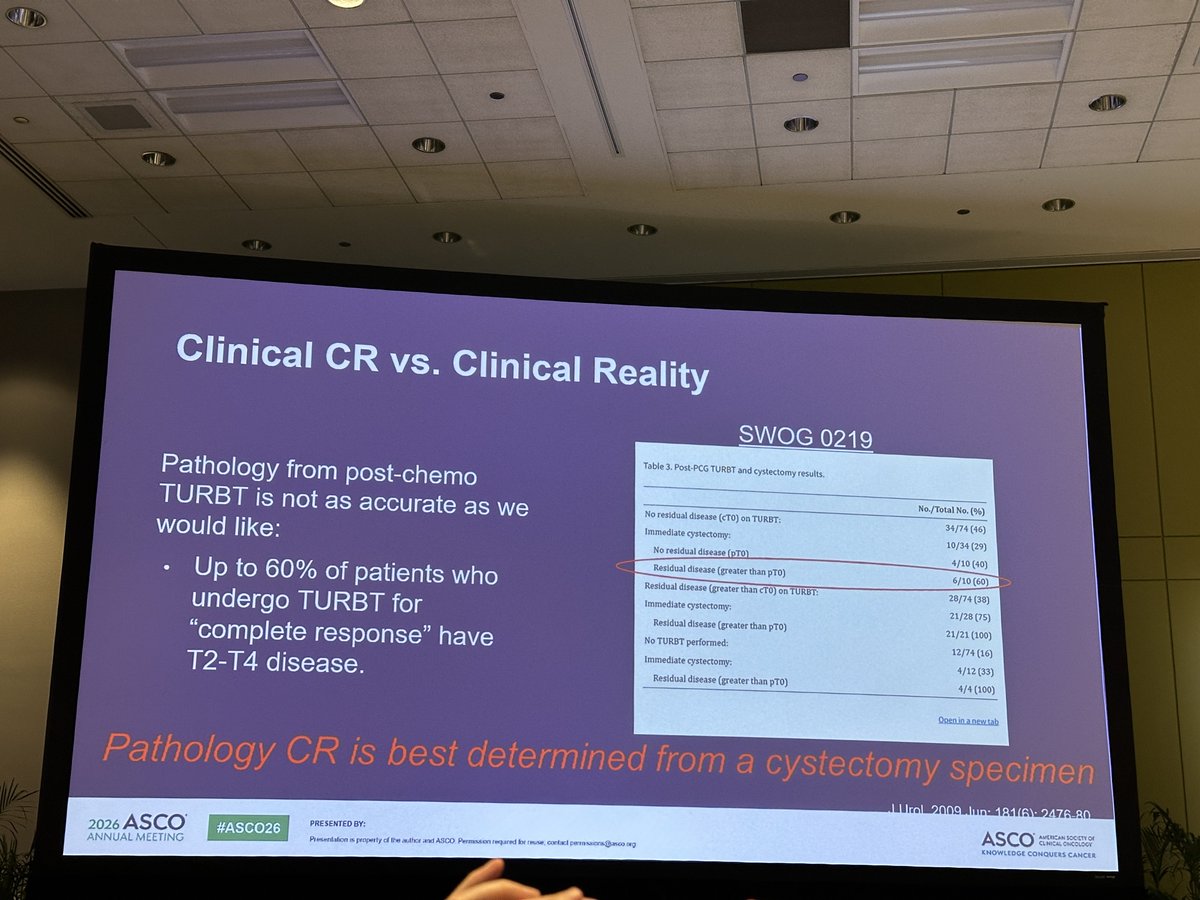
🔬 Interesante debate en #ASCO26 sobre biomarcadores y manejo perioperatorio en cáncer urotelial músculo-invasivo.
#BladderCancer #GUOncology
May 31
🎯🎯 #ASCO26 @ASCO Starting a Day 3 . Please don’t miss a Biomarker and perioperative management of MIUC! ➡️ Now in a S102 room! Excellent Clinical-based discussion!
@OncoAlert @urotoday @ASCOPres @GuardConsortium @UroTarget @DrRosenbergMSK @MichvdHeijden
1
2
256
GUARD Consortium retweeted

May 30
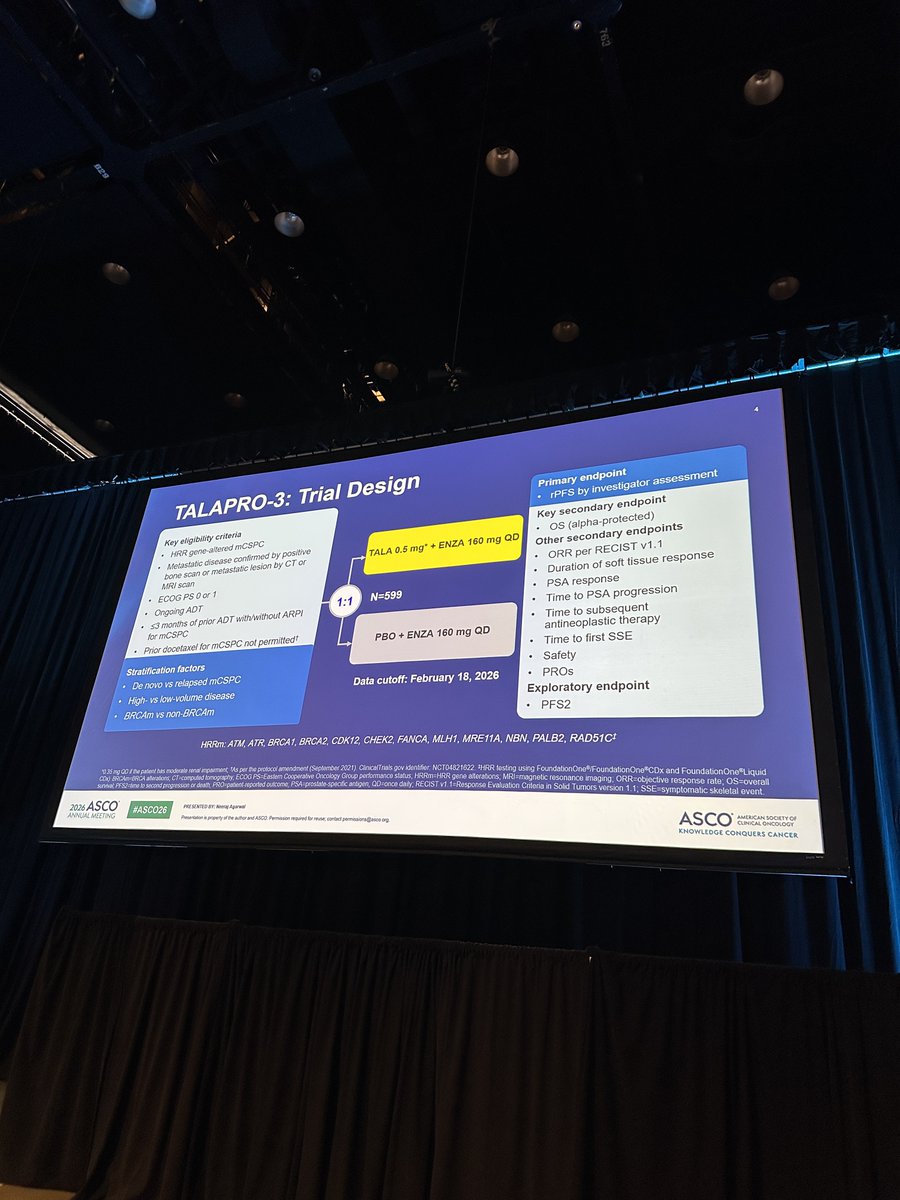
🎯 ##ASCO26 @ASCO TALAPRO-3 ph 3 study of ADT Enza /- talazoparib in mHSPC presented by Dr Neeraj Agarwal!
👉 TALA ENZA led to a clinically meaningful and statistically significant prolongation of rPFS (HR, 0.48) vs the active ENZA control in men with HRR gene-altered mCSPC
@OncoAlert @tompowles1 @DrChoueiri @GuardConsortium @UroTarget @neerajaiims


7
13
1,078
🌍 Desde #ASCO26, un mensaje clave: la investigación colaborativa y global es fundamental para seguir avanzando contra el cáncer.
Gracias al Dr. @cdanicas por compartir las principales reflexiones de la sesión inaugural.
#GUARDConsortium #CancerResearch #GUOncology
May 30
🎯#ASCO26 @ASCO Excellent, deep and meaningful presentation by Dr Eric Small @ASCOPres (President of ASCO) in a Opening session about the value of the war against cancer and expand the research around the world!! @OncoAlert @ESMO_Open @DrChoueiri @urotoday @neerajaiims @NazliDizman @GuardConsortium @aaoncoclinica


2
3
292
🎙️ Desde #ASCO26, la Dra. @Ecastromarcos comparte su visión sobre los cambios en el manejo del cáncer de próstata metastásico hormonosensible.
Un área en constante evolución que sigue incorporando nueva evidencia para optimizar la toma de decisiones clínicas.
Seguimos compartiendo las principales novedades desde Chicago.
@OncoAlert #ProstateCancer #GUOncology #UroOncology
May 30

Dear Colleagues at #ASCO26
@Ecastromarcos of Hospital 12 de Octubre in Madrid🇪🇸talking about the Changes in the Management of Metastatic Hormone Sensitive #ProstateCancer .
A great Educational Capsule by our partners at @GuardConsortium
cc:
@cdanicas
@dralvaropinto
@drenriquegrande
@nachoduranm
@DrJaVallejo
@abraocantoMD
@docjavip
@AlvarezMa89031
@DrFelixGuerrero
@BerUrologia
@AnaPlatabello1
@scocmem
@OncBrothers
@Helena_de_Palma
@F_lopez_campos
@mjuanfi81
@EurUrolOncol
Pinging OncoAlert Faculty
@montypal
@crisbergerot
@DrDanielHeng
@apolo_andrea
@DrChoueiri
@PGrivasMDPhD
@TiansterZhang
@HHammersMD
@ravikanesvaran
@neerajaiims
@amerseburger
@sonpavde
@drenriquegrande
@scserendipity1
@Silke_Gillessen
@EfstathiouEleni
@tompowles1
@BraunMDPhD
@nataliagandur
@cdanicas
@brian_rini
@AOmlin
#OncoAlertAF
@nataliagandur
@realbowtiedoc
@Onco_Cifu88
@scocmem
@AmandaNizamMD
3
4
693
GUARD Consortium retweeted

#ASCO26 GU Oncology Spotlight 🚨
🔬 Precision Oncology: How to Apply New Biomarkers in Clinical Practice
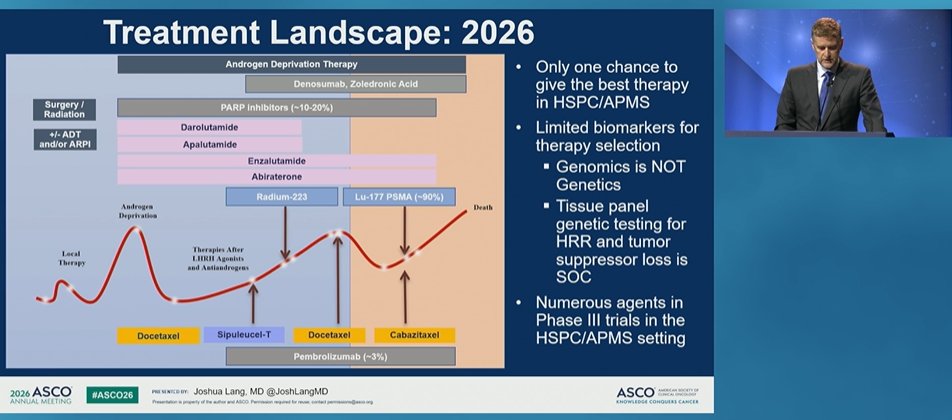
Excellent discussion by Joshua M. Lang, MD, MS
@JoshLangMD
@OncoAlert
@ASCO
This session captured the real challenge of precision oncology in GU cancers:
A biomarker is only useful if it answers a clinical decision.
Not just:
➡️ Is the patient high risk?
➡️ Is the biomarker prognostic?
But:
➡️ What treatment decision changes?
➡️ Who should be intensified?
➡️ Who can safely avoid toxicity?
➡️ Can we reduce imaging, treatment burden, or overtreatment?
🟦 Prostate cancer: intensification is getting crowded
In metastatic hormone-sensitive prostate cancer and high-risk localized disease, we now have multiple active options:
• ADT
• ARPIs
• docetaxel
• abiraterone-based intensification
• PARP inhibitor strategies in selected patients
• radioligand approaches under study
But the clinical problem remains:
➡️ We often have only one chance to choose the best early strategy.
And biomarkers for therapy selection remain limited.
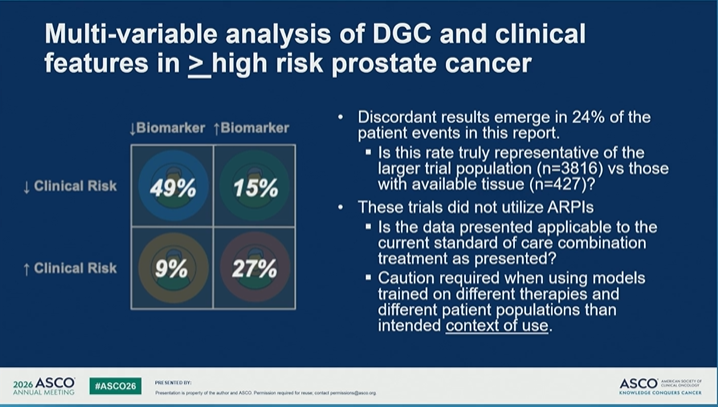
🟩 Abstract 5000: clinical genomic risk for abiraterone intensification
The clinico-transcriptomic model in high-risk localized prostate cancer reinforces an important concept:
Clinical risk alone is imperfect.
Adding genomic classifier information may better define who resembles the STAMPEDE M0 very-high-risk population — the group in whom abiraterone intensification has a strong rationale.
But caution is essential:
⚠️ pooled legacy trials
⚠️ no contemporary PSMA PET staging
⚠️ no abiraterone-treated patients in the NRG/RTOG cohorts
⚠️ model-based inference, not a definitive treatment-selection rule
So this is promising risk refinement — not yet a final decision tool.
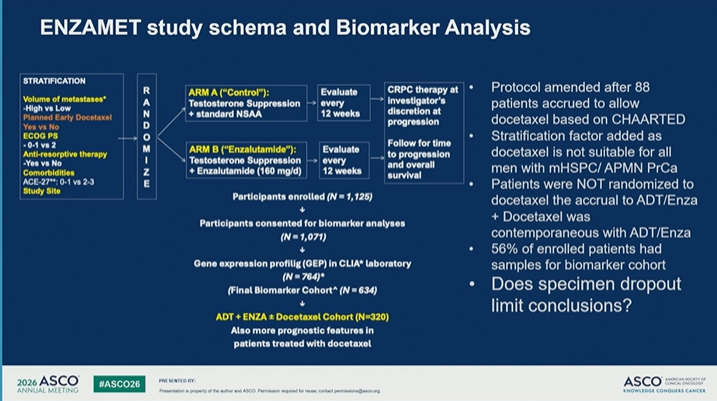
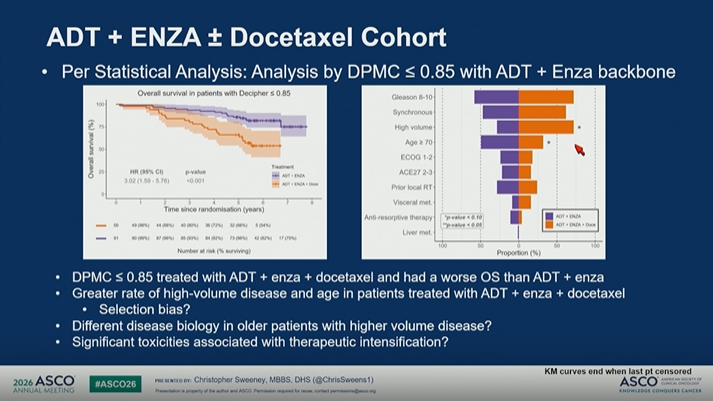
🟨 Abstract 5001: ENZAMET Decipher
ENZAMET offered a unique opportunity to ask whether Decipher can help identify patients who benefit from adding docetaxel to ADT enzalutamide.
Key signal:
• DGC >0.85 was associated with poorer OS
• patients with higher Decipher scores had more adverse clinical features
• the analysis suggested potential enrichment for docetaxel benefit in selected biologically high-risk patients
But again, the key question is clinical utility:
➡️ Does the biomarker predict treatment benefit enough to change practice?
➡️ Or is it mainly identifying worse prognosis?
That distinction matters.
🟧 Abstract 5002: spatial transcriptomics computational pathology
ST-DoxPCa takes the field in another direction:
Can routine H&E images be linked to spatial transcriptomic biology to identify who benefits from docetaxel?
This is exciting because it points toward biomarkers that may be embedded in ordinary pathology workflows.
But implementation questions remain:
• retrospective analysis
• limited sample availability
• need for validation
• ADT docetaxel is no longer the full modern standard backbone
• generalizability to today’s ARPI-containing regimens remains uncertain
🟥 LBA5003 / SWOG S1823: miR371 in early-stage testicular cancer
In testicular germ cell tumors, miR371 showed:
• high specificity
• strong negative predictive value
• modest sensitivity overall
• better sensitivity with more advanced relapse
This may help refine surveillance, but the key question remains:
➡️ Does miR371 change imaging frequency?
➡️ Does it trigger treatment?
➡️ Can it safely reduce CT exposure?
That is the clinical utility test.
💬 My take
This was an excellent discussion because it emphasized the right standard for biomarkers.
A biomarker should not only be statistically impressive.
It should be:
✓ clinically actionable
✓ prospectively validated
✓ interpreted in the right population
✓ aligned with current treatment standards
✓ able to change a decision that matters
For GU oncology, the next era of precision medicine will not be defined by “more biomarkers.”
It will be defined by better biomarker-driven decisions.
#ASCO26 #GUOnc #ProstateCancer #TesticularCancer #PrecisionOncology #Biomarkers #Genomics #Decipher #miR371
1
13
15
807